
|
Important Dates & Deadlines
Important Information
|
You are here >
Due to unforeseen circumstances, the symposium has been cancelled The story of my first NORA case ages ago.Supervisor: Yvon, tomorrow you have the gyn list in the morning and the PE case in the afternoon ...Me: ... sorry the PE case ... ? Supervisor: ... pneumoencephalography ... just do a GA and intubate the patient, but take care of the tubing ...
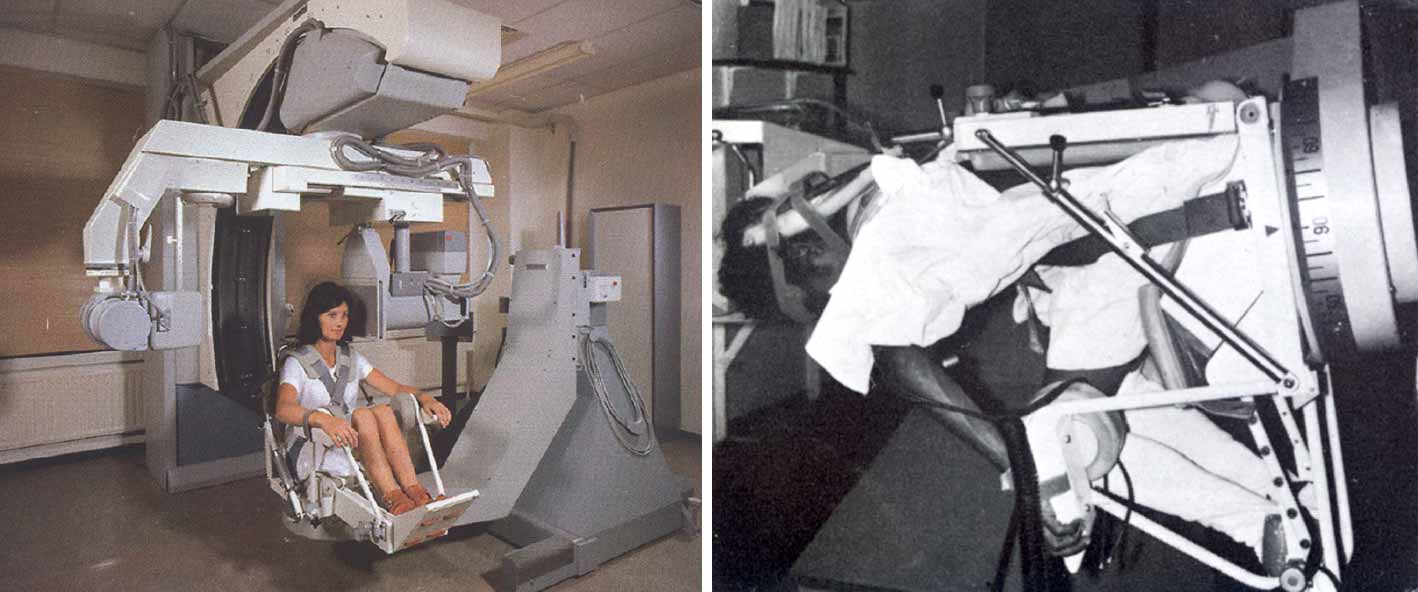
... and then the line was switched off. Dear All, So that was a conversation ages ago with one of my supervisors. I was a few weeks in training, and I could barely intubate a patient … and the next day I had to put somebody asleep for a pneumoencephalogram in a distant location far away from the operating rooms, without a supervisor in the vicinity … but again: WHAT’s a pneumoencephalogram …. ? I dare to guess that most nowadays physicians don’t know what a PE is … In short, just to avoid you switch to Google, PE was X-ray imaging modality used to visualize brain tumors. One injected air in the cerebrospinal liquid and the patient sitting in a chair was rotated in 3 dimensions, head down for instance (that ‘s why I had to take care of the tubing).
With courtesy of The Belgian Museum of Radiology (R. Van Tiggelen, MD)
Moreover the only monitoring device at that time was a “HP oscilloscope” (for the EKG), blood pressure was measured by the Riva Rocci method … no capnography, no pulse oxymetry … and just a lot of stress for the anesthesiologist.
Over the following years, fortunately PE disappeared from the diagnostic armamentarium in favor for more confortable diagnostic tools (CT and MRI), and a number of non-invasive monitors became available for the anaesthesiologist.
This is the story of my first NORA case ages ago.
In the beginning of my career I considered these out of operating room cases as rather exceptional activities for an anaesthesiologist whose core business was in the OR.
However, over the years, the demand for anaesthesia services outside the operating room increased. In the past, surgeons were the driving forces behind the anesthesiologists for pushing patient’s physiological capacities to further limits . Nowadays it is clear, because technological advances, the “medical interventionalists” toke over the dynamics for pushing the anesthesiologists to elaborate innovating strategies in order to provide anesthesia for extremely sick patients.
In the first part of my career, as cardiothoracic anaesthesiologist, these were in first instance the paediatric and interventional cardiologists, followed by cardiac electrophysiologists.
Anaesthesia for these cardiac interventions was still in close relation with my primary scientific interest, namely cardiorespiratory physiology and hemodynamics.
I considered anaesthesia for interventions beyond the cardiac arena as duly necessary but from the physiological point of view not very interesting. This was a complete misconception of myself (and in fact not a really scientific attitude).
The return to my hometown, Brussels, and the appointment at the “Hors Quartier” at the Erasme University Hospital of the U.L.B., was a real game changer.
My appointment at the “Hors Quartier” was the start of a serendipitous journey to NORA.
The idea of organizing a NORIA symposium had a dual purpose:
Moreover, it’s my conviction that in the future a substantial commitment from the anaesthesiology departments for NORA will be essential for the overall quality medical care provided by the hospital. By consequence, the non-operating room anaesthesiologist will be key player in the organization of the delivery of medical care in his or her institution.
I look forward welcoming you in Brussels,
|

| Copyright © 2018 Semico nv | Powered by Mintyfresh Software Architects |
|---|