Introduction
Soon after the invention of the direct ophthalmoscope by Hermann von Hemholtz in 1851, clinicians began to identify small, white/gray, elevated lesions in the posterior pole.1 These lesions were first named “soft exudates” in order to differentiate from “hard exudates,” seen as yellow, crystalline granules. Later, these gray-white lesions were renamed “cotton wool spots.” Cotton wool spots are common retinal manifestations of many systemic diseases including vascular and immunological entities.2
SARS-CoV-2 is a novel virus that causes COVID-19, which has affected over 519 million people and killed over 6 million.3 Though COVID-19 has caused significant respiratory illnesses, it has also induced substantial systemic inflammatory, hypercoagulable, and thrombotic states.2 The ocular effects of COVID-19 have not been well identified at this time; however, there have been established associations of COVID-19 related retinopathy with systemic comorbidities, including yet not limited to: hypertension, diabetes, and cardiovascular conditions.
Case Presentation
A 75-year-old Caucasian male presented to clinic for a routine eye exam. The chief complaint was longstanding symptoms of dry eye, which improved with use of artificial tears as needed. His last eye exam was one year ago. The patient’s ocular history included: cataract extraction OU with monocular diplopia status post cataract extraction OS and YAG laser capsulotomy OS. The patient’s medical history included: sciatica, diverticulosis, schizophrenia, anxiety, and benign prostate hyperplasia. Active medications included: acetaminophen, celecoxib, duloxetine, dutasteride, pravastatin, and sildenafil. The patient’s systemic history and family systemic history were negative for microvascular conditions, including hypertension, diabetes, and cardiovascular disease. There were no known allergies.
The patient had developed symptoms consistent with COVID-19 including coughing, constant vomiting, body aches, fatigue, nausea, and headaches 20 days before his visit to the eye clinic. He had received a Pfizer-BioNTech (BNT162bv2) initial vaccination one year prior, with a subsequent vaccination four weeks later. He presented to the emergency department nine days prior to his eye clinic visit requesting a COVID test; at that time, he denied feeling short of breath or difficulties with breathing. He tested positive with a rapid polymerase chain reaction (PCR) test. A request for nirmatrelvir/ritonavir was denied by the pharmacy. The patient reported losing 10 pounds over the course of the infection.
On examination, the patient’s best corrected visual acuity was 20/20 OD and 20/25 OS, with no improvement with pinhole. Extraocular muscles demonstrated a full range of motion and he was orthophoric at both distance and near. The patient’s fields were full in each eye as determined by the Humphreys Frequency Doubling Technique (FDT) perimeter. Pachymetry with the Oculus PARK1 measured 587 microns OD, 605 microns OS. The pupils were equal, round, and reactive to light with no relative afferent pupillary defect. Intraocular pressures were 11 mmHg OD and OS by iCare tonometry. Anterior segment findings were within normal limits, including posterior chamber intraocular implants in both eyes and no posterior capsular opacification OU.
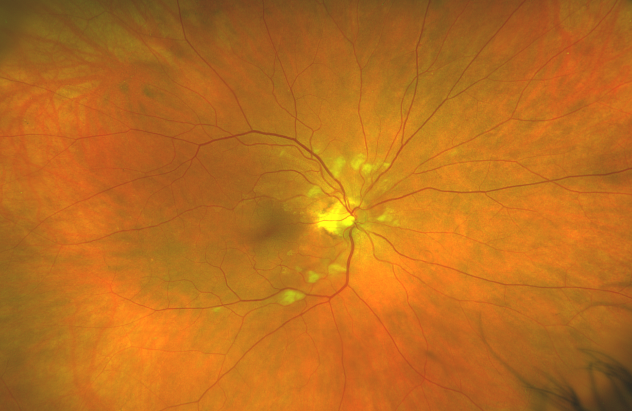
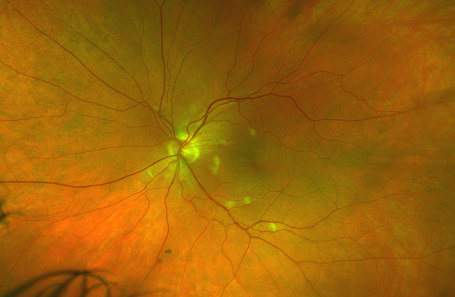
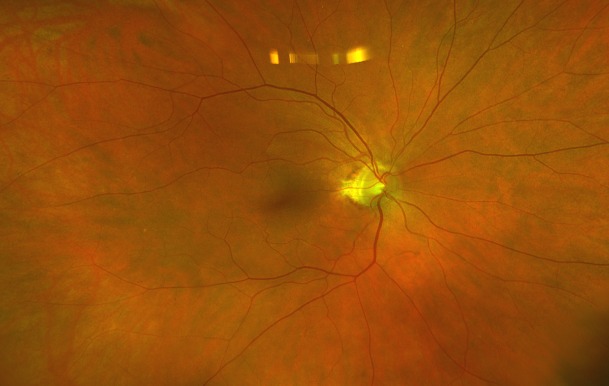
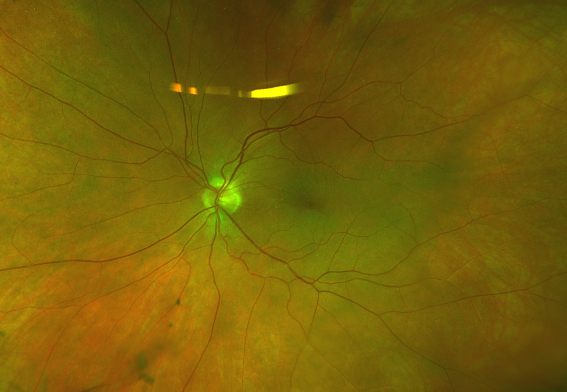
On posterior segment evaluation, the optic nerve head appeared well perfused, with normal cupping in both eyes; the maculas appeared flat and avascular. Several cotton wool spots were evident in the posterior pole, concentrated near the optic nerve head, greater in OD than OS, as seen in fundus photographs of the posterior pole (Fig. 1 & Fig. 2). There was no evidence of diabetic or hypertensive retinopathy. No other signs of pathology were found in posterior pole and periphery of either eye.
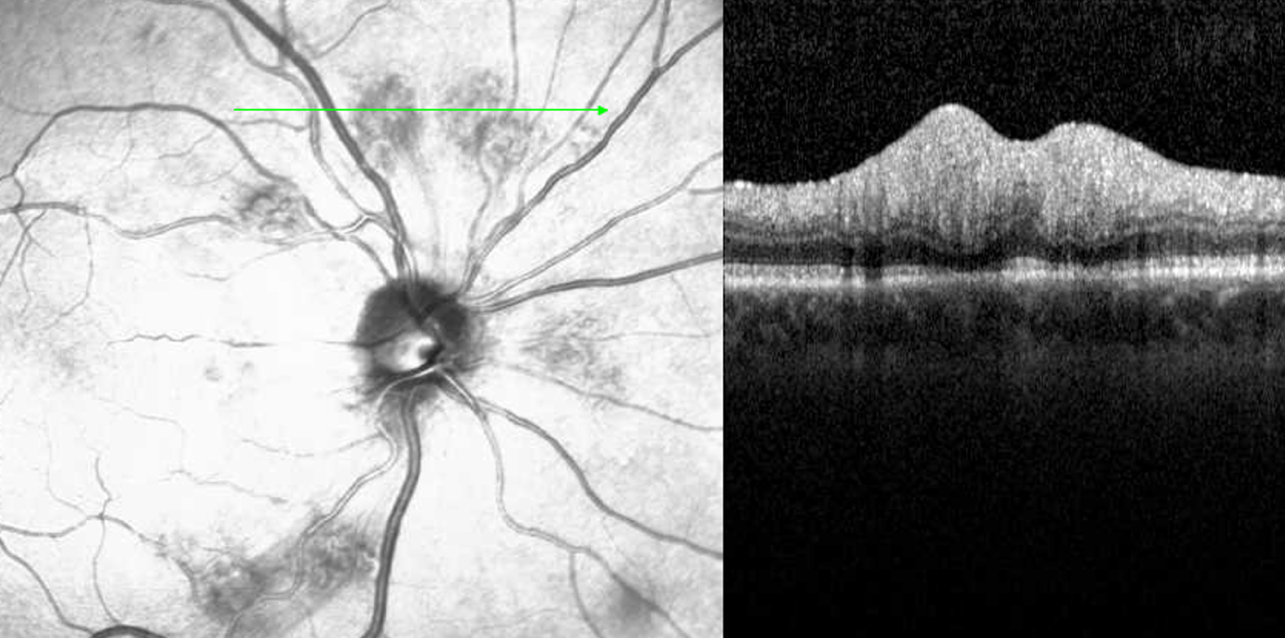
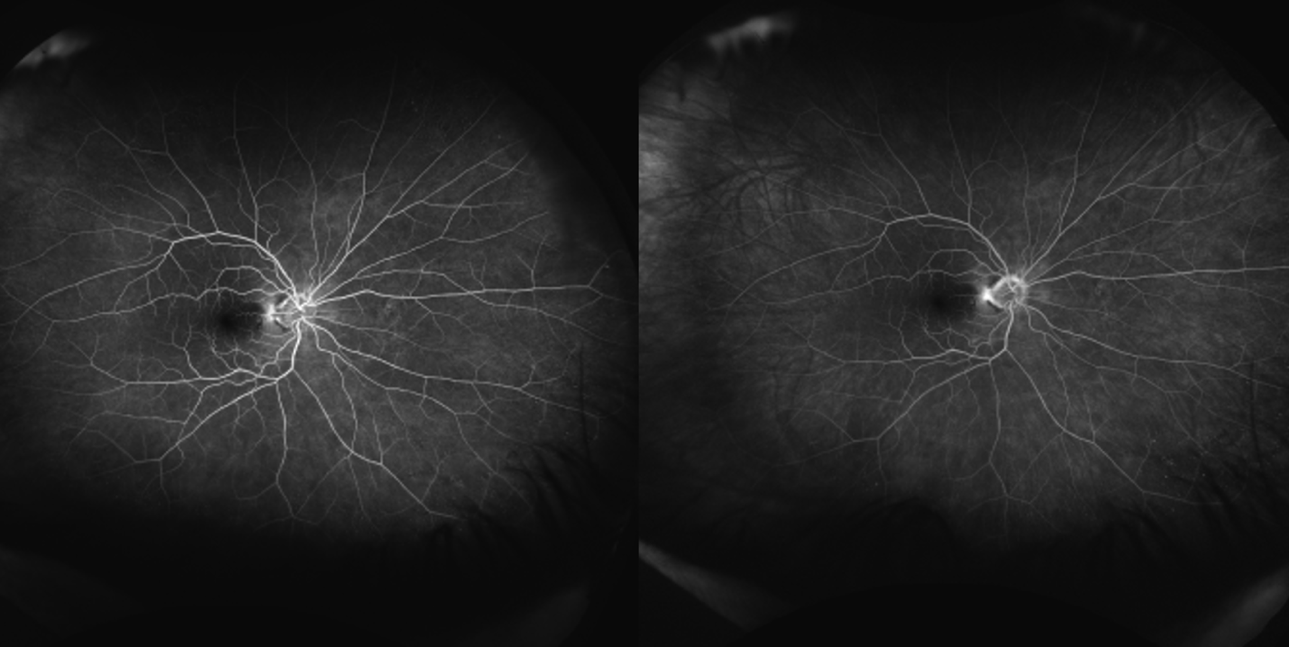
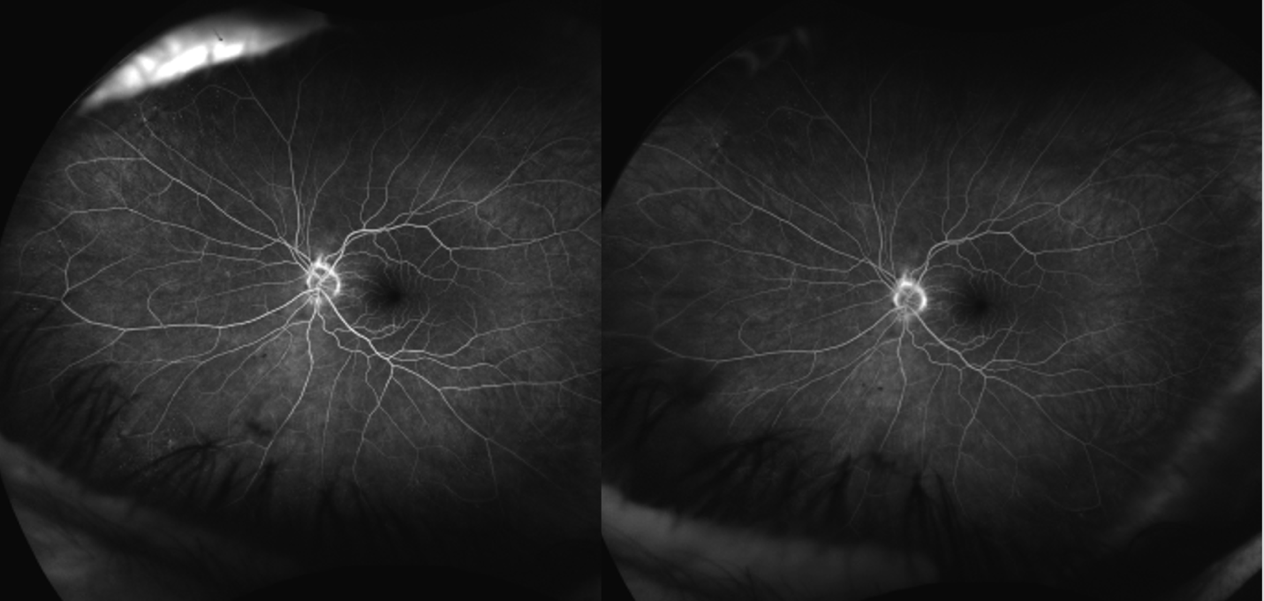
Spectralis optical coherence tomography of the macula demonstrated no evidence of macular edema in either eye. However, a line scan through the cotton wool spots showed focal thickening of the retinal nerve fiber layer (Fig. 3). Optos fluorescein angiography was normal and demonstrated no evidence of non-perfusion or leakage within posterior pole and peripheral retina (Fig. 4 & 5).







The patient’s laboratory testing and medical record was further reviewed to assess for systemic involvement and possible causes of the bilateral cotton wool spots. An evaluation of the patient’s most recent blood pressure readings showed overall low systolic and diastolic pressures without major fluctuations (see Table 1).
After consulting with a retinal specialist, the patient was confirmed to have bilateral cotton wool spots that were likely due to a recent COVID-19 infection based on the ability of the virus to infect the vascular endothelium or produce the release inflammatory cytokines.4 The plan was for the patient to return for a follow-up examination in three months including a dilated fundus exam. At the follow-up visit three months later, the cotton wool spots were fully resolved, and the patient was instructed to return for an annual eye examination unless new concerns developed. (Fig. 6 & Fig. 7)
Discussion
A cotton wool spot is comprised of a nucleus within a cystoid body in a swollen nerve fiber layer. The nucleus is an accumulation of intracytoplasmic organelles which are interrupted in their slow and fast anterograde and retrograde transport between ganglion cell bodies.5 An interruption in axoplasmic flow can be a result of focal ischemia which leads to pre-capillary arterial flow.6
Upon funduscopic exam the following signs will be evident: small, yellow-white, slightly elevated lesions in superficial retina.6 They are normally <1/3 disc diameters in size, most commonly in posterior pole, with indistinct margins and overlying vessels.6 Performing an OCT scan over the white lesions is useful in identifying a swollen nerve fiber layer in the area of the cotton wool spot, which is diagnostic of the finding.6 Generally, patients are asymptomatic unless there is foveal involvement which can lead to a reduction in vision. Cotton wool spots may resolve in 6-12 weeks.7 Treatment is directed towards the underlying etiology. Prior to initiating treatment, a systemic work-up is indicated to determine the etiology of the retinopathy.
Cotton wool spots are a result of multiple different systemic conditions: ischemic, hyperviscosity, inflammatory, infectious, embolic, neoplastic, medication induced, and idiopathic.8 Ischemic causes include: hypertension, diabetes and anemia.9 Hypercoagulable and hyperviscosity states may result from abnormal protein C + S activity or factor V Leiden. Inflammatory causes include: lupus, giant cell arteritis, polyarteritis nodosa, dermatomyositis, and scleroderma.8,9 Infectious causes include: HIV, bacteremia, endocarditis, cat-scratch disease, and fungal infection.8,9 Embolic causes include: cardiac and carotid emboli, deep venous emboli, and Purtscher-like retinopathy.9 Neoplastic causes include: metastasis, leukemia, and lymphoma.9 Medications would include interferon.
The highest differential diagnosis of our case was Purtscher’s-like retinopathy, which can be caused by pancreatitis, renal failure, preeclampsia, connective-tissue disorder, long bone fracture, and Valsalva maneuver.10 In this case, the Valsalva maneuver was considered as a possible etiology due to the patient’s coughing and constant vomiting from the COVID-19 infection. Based on the retinal specialist’s findings, cotton wool spots were not observed to be arrayed in a “rosette” pattern around the optic nerve that would have been characteristic of Purtscher’s-like retinopathy. Moreover, the cotton wool spots could have been misidentified as Purtscher flecken, which is pathognomonic for the condition and may be found in many cases. However, the appearance of the flecken is quite different than cotton wool spots. They are polygonal in shape, variable in size, have sharper borders, and do not obstruct vessels, known as paravascular clearing.11 Other causes of Purtscher’s-like/Purtscher retinopathy such as pancreatitis, lupus, autoimmune disease, and trauma were absent; thus, Purtscher’s-like retinopathy was ruled out in this patient.
The proposed pathophysiology of COVID-19 includes systemic vascular leakage, hypercoagulation, and inflammation: The virus binds to ACE2 receptors on the cell surface increasing vascular permeability, activated neutrophils produce reactive oxygen species.4 Immune cells, inflammatory cytokines, and vasoactive molecules lead to endothelial cell contractility and loosening inter-cell junctions, which upregulates hyaluronic acid and promotes fluid retention all leading up to vascular permeability and leakage.12 Disruption of vascular integrity and endothelial cell death leads to exposure of basement membrane of cells and activates coagulation cascade, which includes platelets releasing VEGF upregulating the coagulation cascade.4 High levels of cytokines destruct endothelial cells further leading to inflammation by expressing leukocyte adhesion molecules.13 Since our patient lacked comorbidities, including diabetes, hypertension, cardiovascular disease, or immunological conditions, it is most likely that the bilateral parapapillary cotton wool spots were caused by the patient’s recent COVID-19 infection. The patient did have elevated ESR and CRP values, which may be associated with a recent COVID-19 infection and are commonly elevated regardless of severity of infection.4
Conclusion
Much continues to remain unknown regarding the ocular side effects of the evolving coronavirus infection. The impacts of COVID-19 on ocular health should not be undermined as the virus continues to evolve; inclusion of COVID-19 as a differential in a patient with retinopathy and a recent history of COVID infection is essential for eyecare professionals.