Cyanosis, or blue spells, is when a reduced amount of blood flows into the lungs. Since blood carries oxygen, less oxygen is delivered to the body. As a result, a child may appear blue or bluish. The colour is caused by high levels of reduced (deoxygenated) hemoglobin in the blood near the surface of the skin.
Cyanosis is a blue discoloration of the skin and mucus membranes caused by an increased concentration of reduced hemoglobin (>1.9–3.1 mmol/L) in the blood.
Peripheral and central forms of cyanosis are well recognized. Peripheral or acrocyanosis in newborns is regarded as a benign transient discoloration of the hands and feet. Central cyanosis is a serious pathological sign and involves discoloration of lips and tongue.
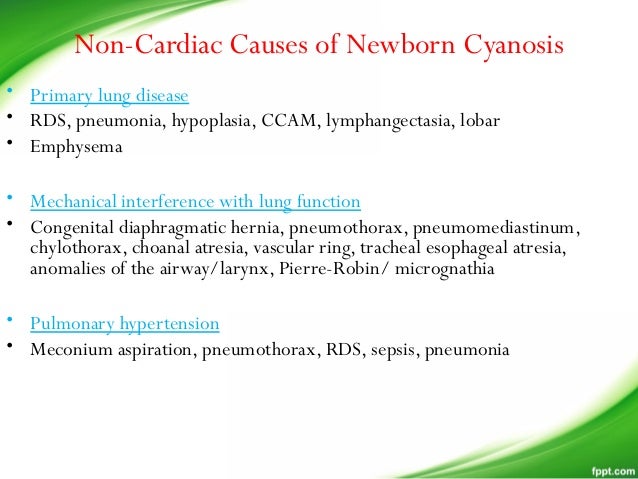
The list of the pathophysiological causes and the most common disorders summarized in Figure 1. Clearly, it can be a formidable task to reach the right diagnosis in a neonate with central cyanosis. The case presented below illustrates diagnostic and management challenges.

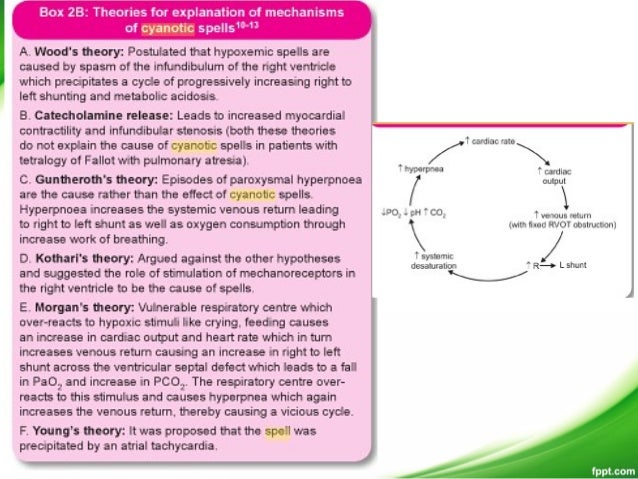
Cyanotic spells occur in children with cyanotic congenital heart disease, in particular tetralogy of Fallot and pulmonary atresia.
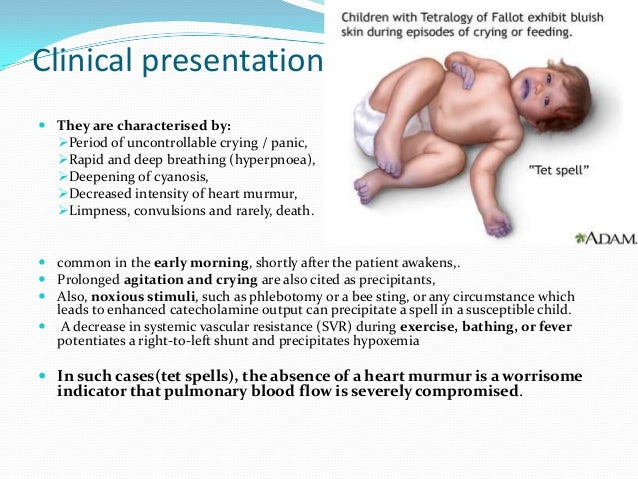
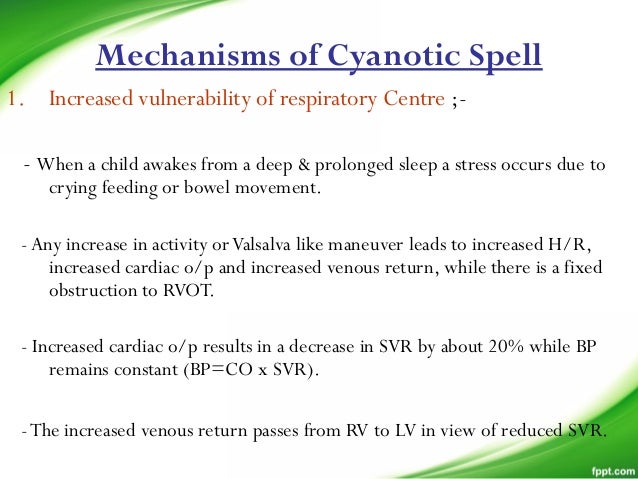
They usually occur early in the morning, or in the context of stress or dehydration ie. periods of increased oxygen demand/ultilisation.
The pathophysiology is not fully understood, but relates to decreased pulmonary blood flow.
Most episodes are self limiting.
Assessment
- Severe cyanosis/pallor (more than usual).
- Distress/hyperpnoea (not tachypnoea).
- Signs of dehydration.
- Lethargy/depressed conscious state.
- Known or evidence suggesting structural heart disease.
- Lessening or absence of previously heard heart murmur.
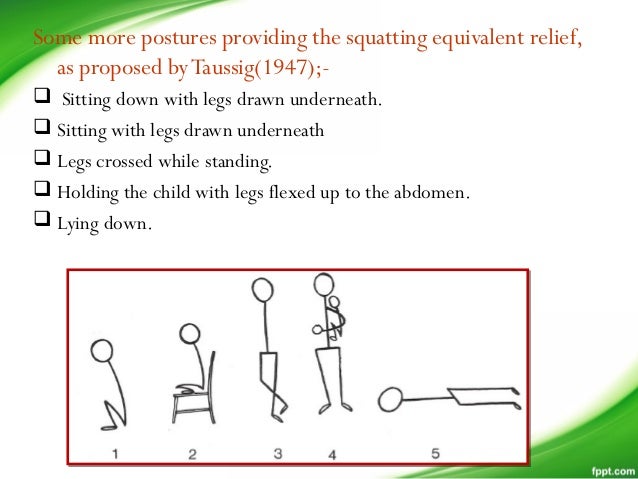
- Previous history of squatting.
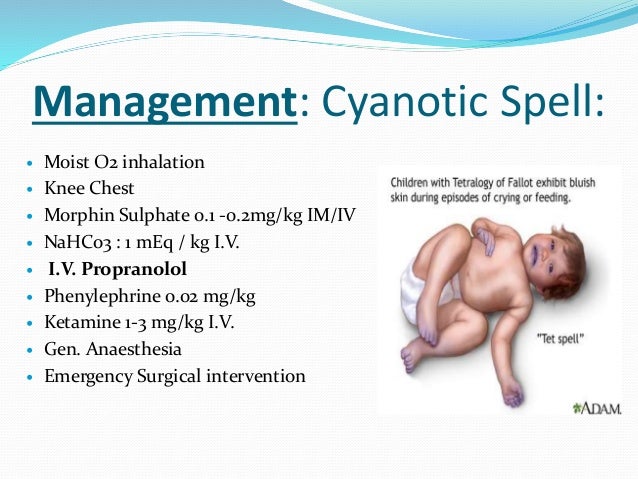
Management
Initial
- Knee to chest position.
- High flow oxygen via mask or headbox.
- Avoid exacerbating distress.
- Morphine 0.2 mg/kg i.m.
- Continuous ECG and oxygen saturation monitoring, frequent BP.
- Correct any underlying cause/secondary problems, which may exacerbate episode, eg. cardiac arrhythmia, hypothermia, hypoglycaemia.
If prolonged
- Consult paediatrician or cardiologist.
- Intravenous fluids – 10 ml/kg bolus followed by maintenance fluids.
- Sodium bicarbonate 2-3 mmol/kg i.v. (ensure adequate ventilation).
- Consider admission.