Approach Considerations
The two main concerns with regard to an adrenal incidentaloma (AI) are (1) whether it is hormonally active (functional) and (2) whether it is malignant. Correlation with the clinical presentation and, if necessary, serum chemical and urinalysis results should be used to determine whether an adrenal cortical adenoma is functional. [49] Benign adrenal cortical adenomas are commonly smaller than 6 cm in diameter on initial presentation, but they may be larger. [50]
No specific medical therapy is required except treating the underlying disease.
Nonsurgical treatment
Conditions that do not warrant surgery include bilateral adrenal diseases such as corticotropin-dependent Cushing disease or bilateral hyperaldosteronism. Nonfunctional (hormonally silent) adrenal cortical adenomas are not premalignant, and surgical excision is not indicated.
The AACE/AAES 2009 guidelines add that patients with bilateral idiopathic hyperaldosteronism (IHA) who cannot or choose not to receive surgical treatment should be managed with selective and nonselective mineralocorticoid receptor blockers. [19]
Surgical treatment
The treatment for a hormonally active adrenal tumor is surgery. The treatment for a malignancy depends on the cell type, spread, and location of the primary tumor. [2]
No randomized trials have compared laparotomy versus laparoscopic adrenalectomy; however, abdominal laparotomy is preferred for bilateral disease, large masses (>10 cm), possible malignant disease, and pheochromocytoma. Fiberoptic laparoscopy is used for visualization, biopsy, and removal. A transthoracic approach is faster than fiberoptic laparoscopy but has a longer postoperative recovery period.
Other experimental approaches, including a laparoscopic robot and augmented-reality visualization of the surgical field, have been described.
Treatment of metastatic disease
Metastatic disease is managed according to the type of primary cancer. Adrenal disease should be removed if the diameter is greater than 6 cm. Otherwise, follow up with repeat computed tomography (CT) scans at periodic intervals.
Complications
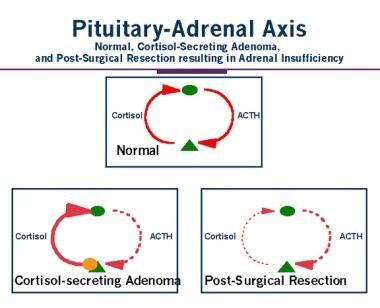
Patients are prone to adrenal insufficiency once the cortisol-secreting tumor is removed. This postoperative adrenal insufficiency is caused by corticotropin suppression and adrenal cortical atrophy of the contralateral adrenal gland, described in the image below.
Consultations
An endocrinologist should be consulted to review the results of endocrine testing.
Long-Term Monitoring
For patients who do not have an adrenalectomy, follow-up is designed to detect interval changes in tumor size or the development of hormonal overproduction. Most adrenal lesions remain unchanged or decrease in size, whereas 5-25% enlarge. Repeat CT scanning at 6-12 months is recommended, and for lesions that do not increase in size, further testing is generally not warranted. [51, 14]
Annual biochemical evaluation of most patients with adrenal incidentalomas (AIs) for as long as 5 years may be reasonable, especially if the tumor is larger than 3 cm in size. [52] Patients with adrenal masses smaller than 4 cm who have a noncontrast attenuation value of more than 10 Hounsfield units should have repeat CT scanning in 3-6 months and again annually for 2 years. Any tumors with indeterminate features on radiology that grow to at least 0.8 cm over 3-12 months may be considered for surgical resection.
Overnight 1-mg dexamethasone suppression testing, a renin-to-aldosterone ratio, and urinary catecholamine and metabolite measurements can be performed yearly or more frequently if clinically indicated. After several years, this testing can probably be discontinued.
Hypercortisolism (especially subclinical) is the most likely hormonal disorder to develop in the follow-up period and is subclinical in most cases.
The AACE/AAES 2009 guidelines state that a patient who has undergone a resection due to a pheochromocytoma should receive long-term follow-up because the recurrence rate is 10-15%. [19]
A study by Leboulleux et al found that 18-fluorodeoxyglucose (FDG) uptake occurred in 14-29% of patients within 24 months after adrenalectomy in patients with adrenocortical carcinoma. [53] The uptake is considered transient and is not suspicious for malignancy.
Primary hyperaldosteronism or catecholamine excess is rarely observed during follow up.
Adrenal insufficiency may occur with bilateral adrenal disease such as lymphoma or hemorrhage.
Hypocortisolism may also occur as a result of corticotropin deficiency from a cortisol-secreting adenoma that is causing contralateral adrenal atrophy. The postoperative course for these patients is prolonged physiologic cortisol replacement.
-
Characteristics of adrenal masses and their malignant potential.
-
Differential diagnosis of adrenal mass
-
Pituitary-adrenal axis and cortisol-secreting adrenal mass.
-
Adrenal incidentaloma and disease type.
-
Left adrenal mass discovered incidentally.
-
Close-up of the left adrenal incidentaloma from the above image.
-
Homogeneous, well-defined, 7-HU ovoid mass is seen in the right adrenal gland; this finding is diagnostic of a benign adrenal incidentaloma.
-
Homogeneously enhancing ovoid mass is seen in the left adrenal gland.
Tables
Author |
Method |
Sample Size |
Prevalence, % |
Russl (1941) |
Autopsy (>1 cm) |
131/9000 |
1.5 |
Kokko (1967) [4] |
Autopsy (>5 mm) |
21/1495 |
1.5 |
Hedeland (1967) |
Autopsy (>2 mm) |
64/739 |
8.7 |
Glazer (1982) [5] |
CT scan |
16/2200 |
0.7 |
Abecassis (1985) [6] |
CT scan |
19/1459 |
1.3 |
Belldegrun (1986) [7] |
CT scan |
88/12000 |
0.7 |
Herrera (1991) [8] |
CT scan |
259/61054 |
0.4 |
Diagnosis |
Features |
Biochemical Tests |
Pheochromocytoma |
High blood pressure, catechol symptoms |
Urine and plasma free metanephrines |
Primary aldosteronism |
High blood pressure, low K+, low PRA* |
Plasma aldosterone-to-renin ratio |
Adrenocortical carcinoma |
Virilization or feminization |
Urine 17-ketosteroids |
Cushing or "silent" Cushing syndrome |
Cushing symptoms or normal examination results |
Overnight 1-mg dexamethasone test |
*Plasma renin activity |
||






