Medical Therapy
Nephroptosis should be treated only in the rare patients who present with a full array of symptoms and confirmation of the diagnosis with one of the imaging studies described above (see Imaging Studies).
Owing to hypochondriac behaviors that often accompany symptomatic nephroptosis, nonsurgical treatments are recommended as a first-line intervention. Some such treatments include weight gain, therapy with gastrointestinal medications, abdominal wall–strengthening exercises, abdominal wall binders (eg, corsets), and frequent rests in the supine position. Extracorporeal support of the ptotic kidney appears to be the most effective nonsurgical treatment, and abdominal binders and corsets were in common use throughout the 1900s. [3] Similar to a truss for treating a hernia, these approaches are all temporizing maneuvers.
Surgical Therapy
All surgical therapies for nephroptosis are based on the principle that the ptotic kidney must be irreversibly fixed into its normal position by securing the kidney or perinephric tissue (renal capsule, perirenal fat, Gerota fascia) to the body wall high in the retroperitoneum via either suture or subsequent adhesion formation. A few of the prominent surgical procedures are discussed below.
Nephropexy
This procedure is used to affix the kidney to the retroperitoneal tissues via open or laparoscopic surgery. The renal capsule is attached to the psoas or quadratus lumborum muscle with nonabsorbable sutures, fascial or muscle bands, and/or polyglactin mesh. [1] This procedure was pioneered by Bassini and is currently the most commonly used open surgical nephropexy technique. Using the 12th rib as a sling or skewer has generally fallen out of favor.
Endourological procedures
In the last 20 years, the endourological procedures laparoscopic nephropexy and circle (U) nephrostomy tube insertion have gained favor as surgical treatments for nephroptosis. [3]
Laparoscopic nephropexy
This is a laparoscopic procedure that closely duplicates the open nephropexy described above but that results in significantly lower morbidity. Laparoscopic nephropexy confers a significant and durable improvement in quality of life in approximately 70%-90% of patients who undergo the procedure. [20, 8, 21, 22] The technique is practiced at many centers with extensive laparoscopic experience.
In 1997, Fornara and colleagues compared open with laparoscopic nephropexy. The mean operative time was 49 minutes and 61 minutes, respectively. Postoperative analgesic control was measured to be an average of 15 mg morphine equivalents in the laparoscopic group and 38 mg in the open group. In the laparoscopic group, the average hospital stay was 3.7 days, versus 16 days in the open surgery group. In addition, split renal function improved from 38% to 47% postoperatively in the laparoscopic group. [20]
Multiple laparoscopic procedural techniques exist, including the use of absorbable mesh, fixation staples, and/or sutures placed through Gerota fascia and sutures through the renal capsule. Many studies have shown that tissue adhesives (eg, butyl cyanoacrylate) and medical devices (eg, tension-free vaginal tape) can also be used to secure the kidney high in the retroperitoneum. [23, 24, 25] Successful kidney fixation has been reported with the sliding cup technique utilizing suture and nonabsorbable polymer clips. [26]
Multiple long-term outcome studies have proven the efficacy of laparoscopic nephropexy. [8, 9, 21, 27] These reports, with follow-up times ranging from 3.3-8.2 years, showed that, postprocedure, 71% of patients reported an improvement in quality of life and showed an 80%-91% reduction in pain.
The original laparoscopic procedure, known as the Washington University technique (transperitoneal laparoscopic retroperitoneal nephropexy), is described in detail in Intraoperative Details.
Circle (U) nephrostomy tube insertion
Note the image below.
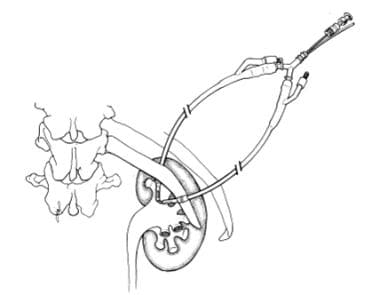 Circle (U) nephrostomy tube treatment. The nephrostomy tube enters above the 12th rib, passes through the kidney through an upper pole, and exits through a middle calyx and below the 12th rib, suspending the kidney. (Reprinted from Hoenig DM, Hemal AK, Shalhav AL, Clayman RV. Nephroptosis: a "disparaged" condition revisited. Urology. Oct 1999;54(4):590-6, with permission from Elsevier.)
Circle (U) nephrostomy tube treatment. The nephrostomy tube enters above the 12th rib, passes through the kidney through an upper pole, and exits through a middle calyx and below the 12th rib, suspending the kidney. (Reprinted from Hoenig DM, Hemal AK, Shalhav AL, Clayman RV. Nephroptosis: a "disparaged" condition revisited. Urology. Oct 1999;54(4):590-6, with permission from Elsevier.)
In this procedure, first described by Szekely and colleagues in 1997, a 14F-16F nephrostomy tube is placed through two points in the middle and upper calices, with the tube entering above the 12th rib and exiting below the 12th rib, forming a sling used to suspend the kidney to the 12th rib. The tube is then sutured to the skin with moderate tension and left in place for 2-3 weeks to allow sufficient scar formation for kidney fixation. [28]
In a long-term outcome study of 90 patients over 12 years, Szekely and colleagues were able to show a 79% long-term success rate with nephrostomy tube insertion based on pain intensity. They reported a mean operative time of 18 minutes and an average hospital stay of 3 days for the procedure. This method, although lacking in widespread application, is considered a low-morbidity, easy-to-perform, cost- and time-effective alternative to laparoscopic nephropexy by those adept in its use. [29] However, because this technique is not widespread in application, corroborating data from other institutions as to its success are absent.
Preoperative Details
Preoperative consultation includes the following:
-
Thorough medical history
-
Verification of symptoms (in the awake patient via imaging studies in both supine and upright positions) [21]
-
Perioperative antibiotics
-
Possible preoperative mechanical bowel preparation of low-sediment diet and glycerin enema for bowel decompression to facilitate laparoscopy
Intraoperative Details
Transperitoneal laparoscopic retroperitoneal nephropexy
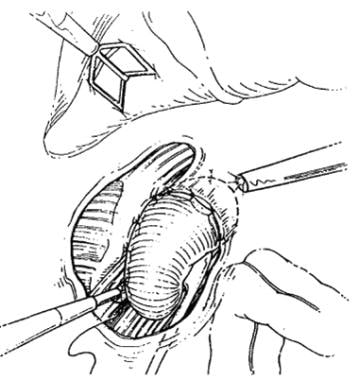 Transperitoneal laparoscopic nephropexy. The lateral border of the renal capsule has been sutured to quadratus lumborum fascia. In addition, the superior flap of the hepatic triangular ligament has been sutured to the anterior renal capsule. (Reprinted from Elashry OM, Nakada SY, McDougall EM, Clayman RV. Laparoscopic nephropexy: Washington University experience. J Urol. Nov 1995;154(5):1655-9, with permission from Elsevier.)
Transperitoneal laparoscopic nephropexy. The lateral border of the renal capsule has been sutured to quadratus lumborum fascia. In addition, the superior flap of the hepatic triangular ligament has been sutured to the anterior renal capsule. (Reprinted from Elashry OM, Nakada SY, McDougall EM, Clayman RV. Laparoscopic nephropexy: Washington University experience. J Urol. Nov 1995;154(5):1655-9, with permission from Elsevier.)
This procedure was first successfully conducted by Urban and colleagues in 1993 at Washington University in St. Louis, Missouri. [30]
A transperitoneal approach is preferred over a retroperitoneal approach because it allows for horizontal and vertical fixation of the kidney while eliminating the need for conversion from retroperitoneal to transperitoneal approach in the rare situation when the kidney is both ptotic and markedly displaced anteriorly. [16] However, more recent studies have shown success and symptom resolution in retroperitoneal approach laparoscopic nephropexy using nonabsorbable sutures placed horizontally rather than in the classic vertical distribution. [31]
Retroperitoneal laparoscopic nephropexy may be particularly indicated in patients who have undergone prior abdominal surgery. [6] Furthermore, tissue adhesives such as butyl cyanoacrylate have shown initial success in affixing the kidney to the retroperitoneum. [24, 23] In 2002, Gyftopoulos et al showed that, with a mean follow-up of 25 months, 9 patients who had undergone adhesive nephropexy had significant improvement on pain scales, as well as proper kidney fixation on follow-up radiographic studies. [32] Nonetheless, further long-term outcome studies are still needed.
The procedure described below has been used in multiple long-term outcome series of laparoscopic nephropexy and has proven to be a safe treatment associated with low morbidity that resolves symptoms due to nephroptosis. [8, 9, 21]
The patient is placed in the lateral decubitus position. A Veress needle is passed into the peritoneum, and the abdomen is subsequently insufflated to 25 mm Hg. A 12-mm umbilical port is placed, followed by insertion of a 30° 10-mm laparoscope. Three additional ports are also placed, as follows:
-
A 12-mm port subcostally at the midclavicular line (Note that a 5-mm port can be substituted, if preferred; in this case, all sutures are then passed via the 12-mm umbilical port.)
-
A 5-mm port in the anterior axillary line at the level of the umbilicus
-
A 5-mm port subcostally in the anterior axillary line
An incision is made at the line of Toldt. The right colon is mobilized and the retroperitoneum exposed. The Gerota fascia is incised, and the kidney is dissected and mobilized on the anterior, posterior, superior, inferior and lateral aspects using electrosurgical scissors and a hook electrode. The medial portion of the kidney can be left undisturbed. The posterior wall of the retroperitoneum is bluntly dissected to expose fascia overlying the psoas major and quadratus lumborum muscles.
The patient is then repositioned in a steep head-down position, allowing for cephalad displacement of the kidney. The kidney is affixed using simple or horizontal mattress sutures of 1-0, nonabsorbable, intracorporeal sutures along the lateral border of the renal capsule from the upper to lower pole of the kidney. The sutures are then placed through the fascia of the quadratus lumborum. Intracorporeal knot tying or Lapra-Ty clips can be used for suture fixation. In addition, newer technologies such as polyglactin mesh, fibrin glue, or nonabsorbable polymer clips can be used to secure the kidney in place high in the retroperitoneum or to add to the security of other types of repairs. [21, 33] A horizontal line of fixation can also be created by anastomosing the superior aspect of the incised posterior coronary hepatic ligament to the anterior renal capsule with nonabsorbable sutures.
Finally, check for hemostasis at the 5-mm port.
Postoperative Details
Patients usually resume oral intake the night of surgery and begin ambulating on the first or second postoperative day, with discharge on the second or third day. Usually, patients receive oral analgesics for pain control and return for follow-up imaging studies 2-6 months following the procedure. [16]
Complications
Potential complications of nephroptosis include the following [1] :
-
Pyelonephritis
-
Renal calculi
-
Hematuria
-
Hypertension
-
Kidney ischemia
-
Flank pain
Potential complications of nephropexy include the following [20] :
-
Urinary tract infection
-
Uncorrected ptotic kidney
-
Retroperitoneal hematoma
-
Bowel injury or puncture during trocar placement
-
Conversion to open nephropexy
-
Muscle paresthesia
-
Genitofemoral nerve injury or entrapment
Outcome and Prognosis
Laparoscopic nephropexy and circle U nephrostomy tube treatment for nephroptosis yield excellent results, with effective pain control in properly selected patients. [19, 34] Multiple long-term outcome studies have shown that patients undergoing laparoscopic nephropexy have significantly reduced morbidity, decreased postoperative discomfort, and a faster recovery time than patients undergoing open nephropexy.
A study by Hubner and colleagues (1994) showed that laparoscopic nephropexy had a mean operative time of 2.7 hours, with 10 mg of morphine required for adequate pain control following the procedure. Follow-up showed anecdotal resolution of symptoms and no significant kidney descent upon repeat intravenous pyelography. [35] However, the follow-up period in this study was only 10.5 months.
In 2000, McDougall and colleagues showed that, with an average follow-up of 3.3 years, analogue pain scales improved by 80%, with 21% of patients considered cured and 71% of patients improved. The procedure failed in only 7% (one patient). Radiographic studies showed that ptosis resolved in all patients, and renal function was unchanged as evaluated by serum creatinine levels. [8]
In 2001, Plas and colleagues published a study validating laparoscopic nephropexy with data garnered from patients with an average of 5.9 years of follow-up. [9] Patient follow-up included standing and supine intravenous pyelography to confirm permanent fixation of the kidney. Ptosis recurred in 20% of patients, while all patients reported anecdotal improvement in symptoms.
Most recently, Gozen and colleagues have shown laparoscopic nephropexy to be a suitable, established, and safe treatment for nephroptosis, with an improvement of symptoms, increased patient satisfaction, and 71% of patients reporting an improvement in quality of life over an average follow-up of 8.2 years. Pain relief was on an anecdotal basis only; 85% of patients were pain-free postprocedure. [21]
Future and Controversies
The existence of pathological nephroptosis and the necessity of its surgical treatment have been debated by urologists for more than a century. However, current knowledge suggests that, in the rare symptomatic patient, laparoscopic nephropexy can prove to be a safe and effective treatment for symptomatic nephroptosis as documented by appropriate radiographic studies.
Many other possible therapies could improve on transperitoneal or retroperitoneal laparoscopic nephropexy, such as the following:
-
Using tissue adhesives (these require further study)
-
Percutaneous suture suspension placement [36]
-
Intravenous urogram. (A) Supine intravenous urogram showing the kidney in proper position with the renal pelvis opposite vertebral body L3 and no hydronephrosis. (B) Upright intravenous urogram showing descent of the kidney and malrotation, with subsequent hydronephrosis development. (Reprinted from Hoenig DM, Hemal AK, Shalhav AL, Clayman RV. Nephroptosis: a "disparaged" condition revisited. Urology. Oct 1999;54(4):590-6, with permission from Elsevier.)
-
Circle (U) nephrostomy tube treatment. The nephrostomy tube enters above the 12th rib, passes through the kidney through an upper pole, and exits through a middle calyx and below the 12th rib, suspending the kidney. (Reprinted from Hoenig DM, Hemal AK, Shalhav AL, Clayman RV. Nephroptosis: a "disparaged" condition revisited. Urology. Oct 1999;54(4):590-6, with permission from Elsevier.)
-
Transperitoneal laparoscopic nephropexy. The lateral border of the renal capsule has been sutured to quadratus lumborum fascia. In addition, the superior flap of the hepatic triangular ligament has been sutured to the anterior renal capsule. (Reprinted from Elashry OM, Nakada SY, McDougall EM, Clayman RV. Laparoscopic nephropexy: Washington University experience. J Urol. Nov 1995;154(5):1655-9, with permission from Elsevier.)

