Background
Although pacemakers provide relief from life-threatening arrhythmias and can improve quality of life significantly, they also can function in a nonphysiologic manner, which is accompanied by nontrivial morbidity. Ventricular pacing has been noted to sacrifice the atrial contribution to ventricular output; in some instances, atrial contraction occurs against closed atrioventricular (AV) valves, producing reverse blood flow and nonphysiologic pressure waves.
McWilliam described a reduction in blood pressure in response to electrical stimulation of a cat's ventricle in 1889. [1] Since the first pacemaker was implanted in 1958, investigators have reported decreased cardiac output in humans as a response to ventricular pacing (see the Cardiac Output calculator). In response to decreased cardiac output, the majority of patients demonstrate aortic and carotid baroreceptor reflex activity, which increases total peripheral resistance (TPR) to maintain constant blood pressure. In some patients, TPR does not increase in response to decreased cardiac output, which results in decreased blood pressure. [2, 3, 4] The combination of decreased cardiac output, loss of atrial contribution to ventricular filling, loss of TPR response, and nonphysiologic pressure waves contributes to symptoms collectively known as pacemaker syndrome.
The definition of pacemaker syndrome has evolved and been the subject of discussion since 1969, when Mitsui and colleagues first reported a constellation of symptoms they thought to be rate-related in patients with ventricular pacemakers. [5, 6] Successive definitions have sought to include data from later investigations into the pathophysiology of the symptoms produced. Furman redefined pacemaker syndrome in a 1994 editorial in which he included the following elements [7] :
-
Loss of AV synchrony
-
Retrograde ventriculoatrial (VA) conduction
-
Absence of rate response to physiologic need
Ellenbogen and colleagues focused on clinical utility and proposed that "pacemaker syndrome represents the clinical consequences of AV dyssynchrony or suboptimal AV synchrony, regardless of the pacing mode." [8]
Recently, most authors have recognized that pacemaker syndrome, which initially was described in patients with ventricular pacemakers, is related to nonphysiologic timing of atrial and ventricular contractions, which may occur in a variety of pacing modes. Some have proposed renaming the syndrome "AV dyssynchrony syndrome," which more specifically reflects the mechanism responsible for symptom production.
AV dyssynchrony may occur outside the setting of pacemakers, however, as noted by Furman, who described the following nonpacing conditions [7] :
-
Extremely prolonged first-degree AV block
-
Nodal rhythm more rapid than the atrial rate, as might occur in children with sinus node dysfunction after congenital defect repair
Such examples have been termed "pseudo pacemaker syndrome," in an effort to reserve the term pacemaker syndrome only for cases involving pacemakers. Other examples of pseudo pacemaker syndrome have been described, including hypertrophic cardiomyopathy with complete AV block. [9]
Pseudo pacemaker syndrome may occur in the setting of an implanted pacemaker when the pacemaker does not participate significantly in creation of AV dyssynchrony. One example is demonstrated in the figure below, which is an example of atrial tachycardia with Wenckebach-type, second degree AV block that results in significant AV dyssynchrony. The patient exhibited symptoms of pacemaker syndrome, including fatigue, lightheadedness, and exertional dyspnea.
 Pacemaker Syndrome. Pacemaker syndrome without pacemaker participation. Displayed are stored data from a dual-chamber pacemaker. The intracardiac tracings reveal atrial tachycardia with second-degree AV block that together created continuous atrioventricular (AV) dyssynchrony, leading to symptoms of pacemaker syndrome, including fatigue, lightheadedness, and exertional dyspnea. Notice that the pacemaker does not participate in creation of AV dyssynchrony. There are no paced events. Top tracing: atrial electrogram. Middle tracing: ventricular electrogram. Bottom tracing: channel markers. Ab = atrial sensed event in postventricular blanking period, AR = atrial sensed event in postventricular refractory period; VS – Ventricular sensed event.
Pacemaker Syndrome. Pacemaker syndrome without pacemaker participation. Displayed are stored data from a dual-chamber pacemaker. The intracardiac tracings reveal atrial tachycardia with second-degree AV block that together created continuous atrioventricular (AV) dyssynchrony, leading to symptoms of pacemaker syndrome, including fatigue, lightheadedness, and exertional dyspnea. Notice that the pacemaker does not participate in creation of AV dyssynchrony. There are no paced events. Top tracing: atrial electrogram. Middle tracing: ventricular electrogram. Bottom tracing: channel markers. Ab = atrial sensed event in postventricular blanking period, AR = atrial sensed event in postventricular refractory period; VS – Ventricular sensed event.
The working definition of pacemaker syndrome currently includes the following:
-
A constellation of specific symptoms occurs.
-
Symptoms occur in the setting of a pacemaker, temporary or permanent.
-
Symptoms result from loss of physiologic timing of atrial and ventricular contractions.
The last condition may be unnecessary, and it helps blur the distinction between definition of syndrome and elucidation of cause. It also excludes at least one mechanism known to contribute to production of the constellation of symptoms, specifically, ventricular activation pattern.
Pathophysiology
Loss of physiologic timing of atrial and ventricular contractions, or AV dyssynchrony, leads to multiple mechanisms of symptom production. Several large trials have focused on pacing mode in the setting of sinus node dysfunction as a mechanism of symptom production. [10, 11, 12, 13] Physiologic pacing is associated with fewer symptoms in the setting of complete heart block. [14, 15] An altered ventricular activation pattern contributes to decreased cardiac output and, consequently, to symptom production. See the Cardiac Output calculator.
Loss of atrial kick
Estimates of atrial contribution to cardiac output vary from 15-25% in healthy hearts at rest. However, in cases of decreased ventricular compliance, atrial "kick" may contribute as much as 50% to cardiac output. Causes of decreased ventricular compliance include diseases such as hypertensive cardiomyopathy, hypertrophic cardiomyopathy, and restrictive cardiomyopathies, and it also occurs in some elderly patients. Inappropriate pacing in these patients can result in loss of atrial kick and can significantly reduce cardiac output.
Cannon a waves
Atrial contraction against a closed AV valve can cause pronounced symptoms of pulsation in the neck and abdomen, headache, cough, and jaw pain.
Increased atrial pressure
Ventricular pacing is associated with elevated right and left atrial pressures, as well as elevated pulmonary venous [16] and pulmonary arterial pressures, which can lead to symptomatic pulmonary and hepatic congestion.
Increased production of atrial natriuretic peptide
Ventricular pacing leads to decreased cardiac output, with resultant increase in left atrial pressure and left ventricular filling pressure. These pressure increases result in increased production of atrial natriuretic peptide (ANP) and B-type natriuretic peptide (BNP). [17, 18] ANP and BNP are potent arterial and venous vasodilators that can override carotid and aortic baroreceptor reflexes attempting to compensate for decreased blood pressure. Patients with pacemaker syndrome exhibit increased plasma levels of ANP, and patients with cannon a waves have higher plasma levels of ANP than those without cannon a waves.
VA conduction
A major cause of AV dyssynchrony is VA conduction. Retrograde conduction leads to delayed, nonphysiologic timing of atrial contraction in relation to ventricular contraction. Nishimura and colleagues showed that patients with intact VA conduction have a greater decrease in blood pressure in response to ventricular pacing than patients with AV dissociation. [19] As is discussed in Etiology, many conditions other than VA conduction promote AV dyssynchrony.
Ventricular activation pattern
The nonphysiologic depolarization pattern produced by pacemakers may be responsible for lower cardiac output with ventricular paced rhythms. Placement of pacemaker leads in the apex of the right ventricle results in initiation of ventricular depolarization in the right ventricular apex, causing an altered pattern of ventricular depolarization and contraction. In a small sample of patients, Rosenqvist and colleagues demonstrated a 10% greater cardiac output during atrial inhibited (AAI) pacing, with physiologic ventricular depolarization, compared with AV sequential, or dual-mode, dual-pacing, dual-sensing (DDD) pacing, with retrograde ventricular depolarization initiated in the right ventricular apex. [20]
The importance of ventricular activation pattern has been more recently highlighted with the advent of biventricular pacing. Bordachar and colleagues showed an increase in cardiac output from 2.2 L/min at baseline to 3.8 L/min with institution of biventricular pacing in patients with heart failure. [21]
A study by Mollazadeh et al, however, suggested that with regard to non-DDD pacing, the biventricular and left ventricular modes provide no significantly greater benefit for systolic blood pressure than does right ventricular pacing; the report also indicated that DDD-biventricular pacing does provide such benefits. The study involved 40 patients with a biventricular pacing device, with patients switched between different pacing modes. The investigators found that the mean systolic blood pressure did not differ between ventricular-only pacing modes but that it was significantly higher in patients undergoing DDD biventricular pacing. The study also determined that palpitations and dyspnea occurred in 22.5% of patients when they were switched from DDD-biventricular mode to right or left ventricular-only pacing and in 12.5% of patients when switched from DDD-biventricular mode to non-DDD – biventricular pacing. [22]
Suboptimal AV timing
Cardiac output can be diminished, leading to symptoms of pacemaker syndrome, when the programmed AV delays in a dual-chamber pacemaker are suboptimal. [23] This seems to occur more frequently in the setting of atrial-synchronous ventricular pacing in patients with intact sinus node function and high degree AV block. Pacemaker programmed AV delay intervals may be too long or too short. Echocardiographic optimization, although rarely used in general practice, can been employed to optimize AV delays.
Etiology
Risk factors
In the MOST trial, low baseline sinus rate and higher programmed lower rate limit were the only preimplantation variables that predicted development of pacemaker syndrome. [24] Postimplantation, an increased percentage of ventricular paced beats was the only variable in the multivariate analysis that significantly predicted development of pacemaker syndrome.
Patients with intact VA conduction are at greater risk for developing pacemaker syndrome. As many as 90% of patients with preserved AV conduction have intact VA conduction, and 30-40% of patients with complete AV block have preserved VA conduction. Patients may have intact VA conduction not apparent at the time of pacemaker implantation or may develop VA conduction at any time after implantation.
Patients with noncompliant ventricles and diastolic dysfunction are particularly sensitive to loss of atrial contribution to ventricular filling. This includes patients with cardiomyopathy (hypertensive, hypertrophic, restrictive) and elderly individuals.
Other factors correlated with development of pacemaker syndrome include decreased stroke volume, decreased cardiac output (see the Cardiac Output calculator), and decreased left atrial total emptying fraction associated with ventricular pacing.
Situations in which AV dyssynchrony may arise
Classically, pacemaker syndrome has been observed in the setting of VVI pacing. Since the advent of dual-chamber pacing, however, examples of pacemaker syndrome have been reported in the setting of many additional pacing modes. [25]
Ventricular inhibited, with and without rate modulation (VVI[R]) pacing
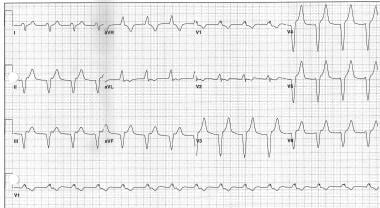
The ventricle is paced independent of atrial activity, yielding AV dissociation, or VA conduction results in AV dyssynchrony. An example of 1:1 retrograde VA conduction during VVI pacing is shown in the image below.
 Pacemaker Syndrome. Retrogradely conducted P waves are visible directly following each ventricular-paced complex.
Pacemaker Syndrome. Retrogradely conducted P waves are visible directly following each ventricular-paced complex.
Atrial inhibited, rate-modulated (AAIR) pacing
Exercise induces pacemaker-mediated rate increase. The paced-A to sensed-R (AR) interval increases when a steep rate-response curve precipitates an increased pacing rate prior to expected catecholamine surge, or progression of AV nodal disease leads to increased AR interval. Interatrial and intra-atrial conduction delays may also lead to an increased AR interval. These conditions may arise outside the setting of an implanted pacemaker.
Single-lead, atrial synchronous, ventricular triggered and inhibited, with and without rate modulation (VDD[R]) pacing
Native atrial rate falls below programmed lower rate limit and VVI(R) pacing supervenes. See the figure above.
Dual-mode, ventricular inhibited, with and without rate modulation (DDI[R]) pacing
Dual-mode, ventricular inhibited, with and without rate modulation (DDI[R]) pacing may cause AV dyssynchrony.
In complete AV block, when sinus rate exceeds the programmed lower rate, ventricular stimulation does not track atrial activation because ventricular triggered mode is absent. AV dissociation occurs, with atrial contraction driven by sinus node activity and ventricular contraction driven by the pacemaker.
In high-grade AV block, either fixed or transient, a ventricular premature contraction (VPC) creates retrograde atrial depolarization, which occurs after the postventricular atrial refractory period (PVARP), inhibiting the atrial channel. The subsequent ventricular stimulation occurs at the lower rate limit, creating the next retrograde atrial depolarization. This process results in functional VVI pacing because all pacemaker-mediated atrial stimuli are inhibited. Also, any sensed atrial activity, including an atrial premature contraction (APC) or extracardiac myopotential, may initiate the cycle.
In the absence of complete AV block, spontaneous atrial depolarization occurs just at the end of atrial refractoriness, resulting in long AR interval.
In the setting of atrial tachyarrhythmias, many DDD mode pacemakers exhibit mode switching to DDI pacing when the native atrial rate exceeds the programmed mode switching rate, thus avoiding pacemaker-mediated ventricular tracking of the atrial tachycardia. This type of mode switching, however, by definition creates AV dyssynchrony. In the specific case of crosstalk, in which ventricular depolarizations are sensed in the atrial channel as atrial activity, the apparent sensed atrial rate becomes twice the actual atrial rate, and inappropriate mode switching to DDI pacing occurs. In such cases, the programmed atrial sensing threshold may be increased to avoid crosstalk sensing.
DVI pacing
DVI pacing may cause AV dyssynchrony. [26] Spontaneous atrial escape occurs earlier than programmed atrial stimulation, and no corresponding ventricular stimulation is triggered. The result is loss of AV synchrony.
When the spontaneous atrial rate exceeds the programmed upper rate limit, the pacemaker responds in various ways: pseudo-Wenckebach AV block, which yields a ventricular rate slower than the atrial rate; higher degree pacemaker AV block; or Fallback, in which ventricular rate decreases independent of atrial rate. All of these pacer responses result in ventricular dissociation from atrial activity, and the physiologic AV relationship is lost.
In complete heart block, an atrial depolarization occurs within the PVARP, creating atrial myocardial refractoriness. The next pacemaker atrial stimulus does not result in atrial depolarization, but the associated ventricular stimulus leads to retrograde VA conduction. This conduction causes subsequent atrial depolarization, again occurring within the PVARP, such that it does not initiate an AV interval but does create an atrial myocardial refractory period. Functional VVI pacing results even though the pacemaker continues producing atrial stimuli, because these are muted by atrial refractoriness. Schuller and Brandt labeled this phenomenon pseudoatrial exit block. [25]
Jais and colleagues reported a case of pacemaker syndrome in the DDD mode in the absence of any pacing stimuli. [27] The setting was sinus tachycardia with excessive PR prolongation, both of which contributed to a shortened RP interval. In this example, the native P wave occurred so soon after the previous QRS that the P wave fell within the PVARP period. No pacemaker AV interval was initiated, but the P wave was eventually conducted, producing a native ventricular depolarization. [28]
This process may have been initiated by a VPC that resulted in pacemaker mode reversion to a longer PVARP period, effectively masking subsequent P waves. Hemodynamic compromise may have precipitated a further increase in heart rate, moving the P wave further back in the PVARP period. During normal DDD mode operation, this type of excessive PR prolongation is prevented and AV synchrony maintained by ventricular stimulation after the programmed AV delay. In the example by Jais and colleagues, AV dyssynchrony was facilitated by failure of P wave sensing secondary to a relatively long PVARP period. The elements leading to this scenario included prolonged PR interval, sinus tachycardia, and relatively long PVARP period.
Degenerate mode reversion
Pacemaker resets from DDD[R] to VVI or ventricular paced (VOO) mode under the following circumstances: interference of noise or dying battery, detection of inappropriate mode switching during automated pacemaker memory review, or detection of irregularities in memory data bits during automated pacemaker memory review. [27] Pacemaker and defibrillator programmed parameter reset leading to symptoms of pacemaker syndrome has been observed as a consequence of radiotherapy. [28]
An example of mode reversion is demonstrated in the first image below, which depicts a patient who had bipolar leads in both chambers and was paced in the DDD mode. Atrial and ventricular stimuli are noted as low-voltage spikes on surface ECG. During routine automated pacemaker memory review, a data bit fault was detected and the pacemaker reverted to VVI mode with unipolar ventricular stimulation, as seen in the second image below. The patient developed symptoms of pacemaker syndrome that resolved upon reprogramming of the pacemaker. AV dissociation can be seen in the second image below, as evidenced by successively shorter PR intervals between native atrial depolarizations and ventricular pacemaker-stimuli.
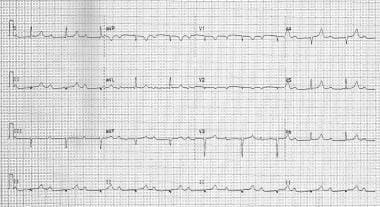 Pacemaker Syndrome. Pronounced PR interval prolongation. The effect of this PR interval prolongation on AV dyssynchrony is demonstrated in this ECG image.
Pacemaker Syndrome. Pronounced PR interval prolongation. The effect of this PR interval prolongation on AV dyssynchrony is demonstrated in this ECG image.
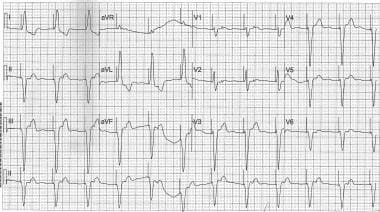
 Pacemaker Syndrome. AV dyssynchrony resulting from severe PR interval prolongation in the setting of sinus rhythm. In this ECG, the PR interval is prolonged to the point that the P wave occurs coincident with the peak of the T wave. Compare to the prior image of the same patient with a slower sinus rate.
Pacemaker Syndrome. AV dyssynchrony resulting from severe PR interval prolongation in the setting of sinus rhythm. In this ECG, the PR interval is prolonged to the point that the P wave occurs coincident with the peak of the T wave. Compare to the prior image of the same patient with a slower sinus rate.
Accelerated junctional rhythm
Accelerated junctional rhythm, sometimes occurring after AV junctional ablation, with or without VA conduction or accelerated ventricular rhythm can precipitate pacemaker syndrome. An example of a junctional rhythm with retrogradely conducted P waves is shown in the image below.
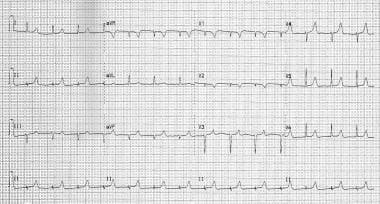
 Pacemaker Syndrome. Junctional rhythm with retrogradely conducted P waves. If symptoms of pacemaker syndrome develop, increasing the lower rate limit for pacing may help to restore AV synchrony.
Pacemaker Syndrome. Junctional rhythm with retrogradely conducted P waves. If symptoms of pacemaker syndrome develop, increasing the lower rate limit for pacing may help to restore AV synchrony.
Idioventricular rhythm
An example of an idioventricular rhythm with retrogradely conducted P waves is shown in the image below. In such cases, the lower rate limit can be programmed to be greater than the junctional or ventricular rate causing symptoms, thus restoring pacemaker-mediated AV synchrony. Alternatively, beta-blocker therapy can be instituted to slow the native junctional or ventricular rhythm to less than the lower rate limit already programmed.
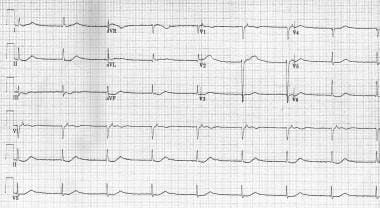
 Pacemaker Syndrome. Accelerated idioventricular rhythm with retrogradely conducted P waves. This ECG demonstrates a mechanism of AV dyssynchrony that might lead to pseudopacemaker syndrome.
Pacemaker Syndrome. Accelerated idioventricular rhythm with retrogradely conducted P waves. This ECG demonstrates a mechanism of AV dyssynchrony that might lead to pseudopacemaker syndrome.
Pacemaker lead malfunction
Pacemaker lead malfunction can result in loss of atrial capture. In such cases, pacemaker ventricular stimulation may become dissociated from atrial depolarization, leading to AV dyssynchrony. One approach in such cases is to increase the voltage or duration of atrial stimulation to restore atrial capture. Ultimately, atrial lead repositioning or replacement may become necessary.
Managed ventricular pacing (MVP) mode
During managed ventricular pacing (MVP) mode, in which AAI(R) pacing predominates, functional undersensing of native P waves can occur during intermittent AV block. [29] This occurs when a native P wave falls in the atrial refractory period (ARP) and is functionally ignored by the logic of the MVP pacing mode. In MVP mode, the ARP is dependent on the R-R interval and not the P-P interval; the ARP is set to 75% of the R-R interval for rates 75 beats per minute or faster, and 600 ms for rates slower than 75 beats per minute. Therefore, when 2:1 AV block occurs, the ARP may be long enough to mask the succeeding native P wave, leading to AV dyssynchrony. During managed ventricular pacing, first-degree atrioventricular block that is induced by hyperkalemia may induce pacemaker syndrome. [30]
Epidemiology
United States data
Several factors complicate efforts to study the incidence of pacemaker syndrome. Symptoms of pacemaker syndrome are nonspecific, occur in settings other than cardiac pacing, and often have been ascribed to the aging process. In addition, memory deficits in elderly patients complicate reporting of symptoms.
Ausubel and Furman estimated the incidence of pacemaker syndrome to range from 7% (symptoms severe enough to warrant pacemaker revision) to 20% (mild to moderately severe symptoms). [31]
The overall incidence of pacemaker syndrome, as prospectively defined in the Mode Selection Trial (MOST), was 18%, with an incidence of 16% at 1 year after pacemaker implantation. [24]
Heldman and colleagues suggested the possibility of a subclinical pacemaker syndrome by comparing dual-chamber pacing to ventricular pacing in the same patients. While their study was small and subject to bias and methodological shortfalls, they nonetheless detected a recognizable syndrome in 83% of patients paced in the ventricular inhibited (VVI) mode, with 65% of patients having moderately severe to severe symptoms. [32]
In a small study, Sulke and associates found that up to 75% of patients who were satisfied with VVI pacing nonetheless benefited from upgrade to DDD mode pacing, which suggests the existence of a subclinical pacemaker syndrome. [33]
Pacemaker syndrome occurs with equal frequency in both sexes, and it can occur at any age.
Prognosis
Morbidity/mortality
The prognosis is excellent with correction of pacing mode.
No direct data are available regarding morbidity and mortality rates associated with pacemaker syndrome.
Investigators have estimated frequency and severity of pacemaker syndrome sequelae by examining patients with AV dyssynchrony and assuming similar statistics; for the purpose of establishing incidence statistics, patients with pacemaker syndrome may be considered a subset of patients with AV dyssynchrony. Estimates of frequency and severity of pacemaker syndrome sequelae largely come from studies examining morbidity and mortality rates associated with different pacing modalities in the sick sinus syndrome. [10] VVI pacing creates AV dyssynchrony, which is used as a surrogate for the pacemaker syndrome; VVI statistics are compared to either AAI or DDD statistics, which are presumed to represent physiologic pacing.
AV dyssynchrony is associated with atrial fibrillation and, therefore, thromboembolic complications, and also is associated with chronic heart failure. By extension, investigators have assumed the same complications for pacemaker syndrome. Following is a discussion of the incidence of these complications, as revealed by studies investigating different pacing modalities, mostly in the setting of sick sinus syndrome, a frequent indication for pacemaker implantation.
Complications
Complications of AV dyssynchrony include atrial fibrillation, thromboembolic events, and heart failure.
Pacemaker syndrome also can be complicated by syncope or near syncope. Individuals may develop a subjectively worse quality of life with ventricular pacing than they had prior to pacemaker implantation, or they may endure a persistently degraded quality of life, as suggested by Sulke's study of subclinical pacemaker syndrome.
Complications of treatment may include the same complications of pacemaker implantation if reimplantation, additional lead placement, or explantation is involved. These complications include infection (4%), pneumothorax (1%), cardiac perforation and tamponade, bleeding, and pain.
Atrial fibrillation
In patients with sick sinus syndrome, VVI pacing leads to a higher rate of atrial fibrillation than does physiologic (ie, AAI or DDD) pacing. Estimates of chronic atrial fibrillation incidence are summarized in the table. The data presented in the following table reveal an annual incidence of chronic atrial fibrillation of 5-13% for VVI versus 0.7-1.7% for AAI pacing. Studies with combined data for AAI and DDD pacing show an annual incidence of 0-4.5%.
Table. Incidence of Atrial Fibrillation in Patients with Pacemakers (Open Table in a new window)
Study |
Patients (number) |
Total Incidence (%) |
Follow-up (years) |
Annual Incidence (%) |
||||
|
|
VVI |
AAI |
DDD |
|
VVI |
AAI |
DDD |
Frielingsdorf [34] |
1838 |
18-47 |
0-17* |
3.75 |
4.8-12.5 |
0-4.5* |
||
Sutton and Kenny [35] |
1061 |
22 |
3.9 |
|
AAI: 2.75 VVI: 3.25 |
6.77 |
1.42 |
|
Hesselson [36] |
8827 |
14-57 |
0-23 |
|
AAI: 1-8 VVI: 3-8 |
Cannot be determined |
||
Hesselson [36] |
950 |
38 |
7 |
|
7 |
5.43 |
1.00 |
|
Santini [37] |
339 |
48 |
3.7 |
13 |
5 |
9.6 |
0.74 |
2.6 |
Sasaki [38] |
75 |
41 |
2* |
AAI: 3.25 VVI: 5.17 |
7.9 |
0.62* |
||
Rosenqvist [39] |
168 |
47 |
6.7 |
|
4 |
11.8 |
1.68 |
|
*Combined AAI and DDD |
||||||||
Thromboembolic events
The relative risk for thromboembolic events parallels the risk for development of chronic atrial fibrillation. In patients with sinus node disease, thromboembolic events occur more frequently in patients who are paced in the ventricular mode than in patients with atrial pacing. Data from studies by Sutton and Kenny [35] , Sasaki and colleagues [38] , and Andersen and colleagues [40] have revealed an annual incidence of thromboembolic events of 4-8% for VVI and 0.6-2% for AAI pacing.
Heart failure
Fewer studies have analyzed incidence and severity of heart failure as a sequela of AV dyssynchrony than have analyzed occurrences of atrial fibrillation and thromboembolic events. Rosenqvist and colleagues showed the incidence of new heart failure to be 9% with VVI versus 4% with AAI pacing. [39] Andersen et al showed significantly less severe heart failure by NYHA (New York Heart Association) class with AAI pacing than with VVI pacing. [40] Sasaki and associates found a trend toward increased incidence of heart failure with VVI pacing than with AAI or DDD pacing. [38]
Mortality
Mortality rates for various pacing modalities in sick sinus syndrome have been well studied, and most studies show that VVI pacing is associated with a higher annual mortality rate than AAI or DDD pacing. Rosenqvist and colleagues [39] and Santini and colleagues [37] studied mortality rates in sick sinus syndrome, comparing VVI with AAI pacing. They obtained data remarkably similar in annual incidence to that provided in the survey of 11 studies by Frielingsdorf and colleagues [34] . Pooling data from the three studies yields an annual all-cause mortality rate of 5.9-7.5% for VVI and 2.2-3.2% for AAI pacing.
Sasaki et al found similar rates of 6.8% with VVI pacing and 3.8% for combined AAI and DDD pacing modalities in sick sinus syndrome. [38, 36]
In one of the few prospective randomized trials, Andersen and colleagues reported an annual mortality rate of 9.4% for VVI and 6.2% for AAI pacing, but this difference lost statistical significance in the multivariate analysis. [40] Zanini et al found that pacing mode had a greater effect on mortality than did the indication for pacing, sinus node dysfunction versus atrioventricular block. [41]
Other studies of note include that of Alpert and associates, which demonstrated no significant difference in mortality rates between VVI and combined DDD and dual-mode, ventricular inhibited (DVI) pacing modalities in patients without preexistent heart failure. [42] In patients with preexistent heart failure, the difference in annual mortality rates—8.6% for VVI and 5.0% for combined DDD and DVI pacing—reached significance. In their survey of six relevant studies, Sutton and Kenny found no survival advantage in patients with sick sinus syndrome of VVI pacing over no pacing. [35] These studies perhaps demonstrate the significant disadvantage of any ventricular stimulation in the setting of sinus node dysfunction.
Patient Education
Educate patients with pacemaker syndrome as in cases of pacemaker implantation in general. Patients should be aware of the following:
-
Avoid strong electric and magnetic fields. Specifically, avoid welding, magnetic resonance imaging (MRI) studies, and proximity to large motors or generators.
-
Use cell phones in the ear contralateral to the side of the device implantation.
-
Pacemaker Syndrome. Pacemaker syndrome without pacemaker participation. Displayed are stored data from a dual-chamber pacemaker. The intracardiac tracings reveal atrial tachycardia with second-degree AV block that together created continuous atrioventricular (AV) dyssynchrony, leading to symptoms of pacemaker syndrome, including fatigue, lightheadedness, and exertional dyspnea. Notice that the pacemaker does not participate in creation of AV dyssynchrony. There are no paced events. Top tracing: atrial electrogram. Middle tracing: ventricular electrogram. Bottom tracing: channel markers. Ab = atrial sensed event in postventricular blanking period, AR = atrial sensed event in postventricular refractory period; VS – Ventricular sensed event.
-
Pacemaker Syndrome. Pronounced PR interval prolongation. The effect of this PR interval prolongation on AV dyssynchrony is demonstrated in this ECG image.
-
Pacemaker Syndrome. AV dyssynchrony resulting from severe PR interval prolongation in the setting of sinus rhythm. In this ECG, the PR interval is prolonged to the point that the P wave occurs coincident with the peak of the T wave. Compare to the prior image of the same patient with a slower sinus rate.
-
Pacemaker Syndrome. Accelerated idioventricular rhythm with retrogradely conducted P waves. This ECG demonstrates a mechanism of AV dyssynchrony that might lead to pseudopacemaker syndrome.
-
Pacemaker Syndrome. Junctional rhythm with retrogradely conducted P waves. If symptoms of pacemaker syndrome develop, increasing the lower rate limit for pacing may help to restore AV synchrony.
-
Pacemaker Syndrome. Retrogradely conducted P waves are visible directly following each ventricular-paced complex.
-
Pacemaker Syndrome. This is an ECG tracing of a patient with continuous atrioventricular synchronous (DDD) pacing prior to development of symptoms. Atrial stimulation (open arrows) is followed by visible P waves. Wide QRS complexes follow ventricular stimulation (solid arrows).
-
Pacemaker Syndrome. This is an ECG tracing of a patient with atrioventricular (AV) dissociation and resultant pacemaker syndrome. Native atrial depolarizations (arrows) move progressively closer to pacemaker-stimulated ventricular depolarizations. Ventricular pacemaker stimuli (arrowheads) are greater in amplitude than those visible in the previous image, consistent with mode reversion from AV synchronous (DDD) to ventricular inhibited (VVI), which includes a switch from bipolar pacing (low amplitude) to unipolar pacing (higher amplitude).
Tables
Study |
Patients (number) |
Total Incidence (%) |
Follow-up (years) |
Annual Incidence (%) |
||||
|
|
VVI |
AAI |
DDD |
|
VVI |
AAI |
DDD |
Frielingsdorf [34] |
1838 |
18-47 |
0-17* |
3.75 |
4.8-12.5 |
0-4.5* |
||
Sutton and Kenny [35] |
1061 |
22 |
3.9 |
|
AAI: 2.75 VVI: 3.25 |
6.77 |
1.42 |
|
Hesselson [36] |
8827 |
14-57 |
0-23 |
|
AAI: 1-8 VVI: 3-8 |
Cannot be determined |
||
Hesselson [36] |
950 |
38 |
7 |
|
7 |
5.43 |
1.00 |
|
Santini [37] |
339 |
48 |
3.7 |
13 |
5 |
9.6 |
0.74 |
2.6 |
Sasaki [38] |
75 |
41 |
2* |
AAI: 3.25 VVI: 5.17 |
7.9 |
0.62* |
||
Rosenqvist [39] |
168 |
47 |
6.7 |
|
4 |
11.8 |
1.68 |
|
*Combined AAI and DDD |
||||||||





