Overview
Immunoblastic lymphoma (IBL), also known as diffuse histiocytic lymphoma, is a malignant disorder of the B cell (see the image below). Although this condition was initially considered a more aggressive variety of lymphoma with a poor prognosis when compared with diffuse large-cell non-Hodgkin lymphoma (DLCL), newer combination chemotherapeutic approaches yield an overall survival rate in immunoblastic lymphoma that is similar to the rate in DLCL.
 Immunoblastic lymphoma. Lymph node biopsy (hematoxylin and eosin stain) showing diffuse involvement with loss of architecture in a patient with immunoblastic non-Hodgkin lymphoma (NHL).
Immunoblastic lymphoma. Lymph node biopsy (hematoxylin and eosin stain) showing diffuse involvement with loss of architecture in a patient with immunoblastic non-Hodgkin lymphoma (NHL).
Immunoblastic lymphoma is a fatal disease if untreated and is potentially curable with intensive chemotherapy. The success of treatment depends on the extent of disease at the time of presentation, associated B symptoms, initial therapeutic choice, and response to therapy.
The frequency rate in the United States is approximately 9% of all non-Hodgkin lymphomas. Of these, 70% are of B-cell origin and 25% are of T-cell origin.
No difference exists among races or between the sexes. However, although immunoblastic lymphoma can appear in persons of any age, it presents most commonly in persons who are middle-aged or older, and it is commonly observed in patients of any age who are immunocompromised.
Go to Non-Hodgkin Lymphoma for a complete discussion of this topic.
Classification
The World Health Organization (WHO) consensus classification should replace all existing classifications. The WHO classification of hematologic malignancies uses an updated version of the Revised European-American Lymphoma (REAL) classification for lymphoid neoplasms. [1, 2, 3]
Earlier classifications subdivided diffuse large B-cell lymphomas (DLBCLs) either by morphology or by the biologic behavior. Kiel's classification subdivides large B-cell lymphoma into immunoblastic and centroblastic lymphomas. In the Working Formulation, immunoblastic lymphoma is classified with lymphoblastic lymphoma and small noncleaved-cell lymphoma as a high-grade non-Hodgkin lymphoma (NHL). The International Lymphoma Study group uses all available information, morphology, immunophenotype, genetic features, and clinical features, to define a disease entity.
Etiology and Pathophysiology
Causes of immunoblastic lymphoma include the following:
-
Environmental – Previous radiation exposure or exposure to pesticides and herbicides
-
Infectious – Human immunodeficiency virus (HIV) infection. Patients with acquired immunodeficiency syndrome (AIDS) have a higher incidence of immunoblastic lymphoma. [4]
-
Autoimmune – Sjögren syndrome (associated with immunoblastic lymphoma); solid organ transplantation or bone marrow transplantation (associated with a higher risk of developing immunoblastic lymphoma)
Immunoblastic lymphoma can originally derive from B or T cells. The Working Formulation differentiates subtypes of immunoblastic lymphoma by cell of origin. [5] The subtypes include plasmacytoid, clear cell, polymorphous, and epithelial cell component. From a clinical point of view, this subclassification has little value; B- or T-cell origin cannot be predicted based on morphology. [6]
In the Revised European-American Lymphoma (REAL) classification, except in morphologic descriptions, the schema includes immunologic, cytogenetic, and molecular information in order to define distinct lymphoma entities. [7] The diffuse large B-cell lymphomas (DLBCLs) are considered in the REAL classification as the classic diffuse large-cell non-Hodgkin lymphoma (DLCL) of B-cell origin defined by the Working Formulation.
Clinical Evaluation
Most patients with immunoblastic lymphoma present with advanced disease; only as few as 30% present with limited-stage disease (I or II). Symptoms vary and depend on the site of involvement.
Painless lymphadenopathy is the most common presenting feature of immunoblastic lymphoma. Occasionally, pain might be associated with aggressive tumor growth. Adenopathy is usually marked and may involve any site; often, it is generalized.
B symptoms may be present. Patients report profuse night sweats, fever is usually low grade (range 100-101°F), and patients may report unintentional weight loss of more than 10% in 6 months. Other symptoms may include fatigue (anemia) and neurologic deficit (central nervous system [CNS] involvement).
Physical examination findings may include the following:
-
Lymphadenopathy
-
Pallor (anemia)
-
Hemorrhage: Petechiae, ecchymoses, epistaxis, and bleeding gums may be present.
-
Hepatosplenomegaly: This may be present as a result of organ involvement.
-
Common sites of extranodal immunoblastic lymphoma include the gastrointestinal tract, bone, testis, and CNS.
-
Unilateral or bilateral tonsillar enlargement: This may be present and typically is refractory to antibiotic treatment.
-
Skin lesions: Rarely, patients may present with skin lesions.
Staging
The Ann Arbor Staging Classification designed for Hodgkin disease is now used (with certain limitations) for non-Hodgkin lymphoma (NHL) classification. This classification, outlined below, does not recognize disease of bulk, which has prognostic and therapeutic importance.
-
Stage I – Single lymph node involvement
-
Stage IE– Single extranodal site or organ involvement
-
Stage II – Two or more lymph nodes involved on the same side of the diaphragm
-
Stage IIE– Localized involvement of an extranodal site or organ and involvement of one or more lymph node regions on the same side of the diaphragm
-
Stage III – Involvement of lymph node regions on both sides of diaphragm, which might be accompanied by localized involvement of an extranodal organ or site (stage IIIE), the spleen (stage IIIS), or both (stage IIISE)
-
Stage IV – Diffuse or disseminated involvement of one or more distant extranodal organs, with or without associated lymph node involvement
Differential Diagnosis
The following conditions are considered a part of the differential diagnosis of high-grade immunoblastic lymphoma:
Laboratory Evaluation
Obtain a complete blood cell (CBC) count and peripheral blood smear, as well as serum chemistry levels, including lactate dehydrogenase (LDH) and serum electrolytes. Other laboratory studies should include liver and renal function tests.
Elevated beta-2 microglobulin levels are associated with a poor prognosis.
Obtain a coagulation profile before any surgical intervention (eg, tissue biopsy, placement of a venous access port).
Serum protein electrophoresis is rarely performed; however, this may show the presence of monoclonal proteins or an increase in immunoglobulins.
Cytogenetic Studies
Cytogenic studies are generally used to help exclude other types of non-Hodgkin lymphoma (NHL). Chromosomal aberrations, such as del(6q),+X, are associated with immunoblastic lymphoma, but they are not exclusive for this type. Mutations or allelic losses of the p53 tumor suppressor gene are common in the immunoblastic type.
Yunis et al observed that rearrangement of BCL2 in patients with immunoblastic lymphoma correlates with poor response to therapy. [8]
Immunoblastic lymphoma morphology is characterized by MUM1 expression and infrequent bcl6 expression.
Radiography, CT Scanning, and MRI
Chest radiographs are used for staging purposes.
Computed tomography (CT) scanning of the chest, abdomen, and pelvis to evaluate nodal and extranodal involvement is also usually part of the staging workup. CT scanning of the head is performed only if neurologic symptoms are present.
Magnetic resonance imaging (MRI) of the spine and brain may be performed for patients with a paraspinal mass to assess for epidural involvement and cord compression. Patients with signs or symptoms suggestive of intracranial disease may also require an MRI.
Nuclear Imaging
Most of the studies evaluating positron emission tomography (PET) scanning results were performed mainly in cases of diffuse large-cell non-Hodgkin lymphoma (DLCL). PET scans may be more sensitive compared with other imaging modalities, including gallium, when used for lymphoma staging.
Although a nonspecific test, a gallium scan is often useful in follow-up evaluations for patients with initial gallium-avid disease. Therefore, gallium scanning is performed as part of the initial staging workup. Clinical correlation with computed tomography (CT) scan results is always recommended in patients with abnormal gallium scan results.
Bone scanning should be performed only if the patient has unexplained bone pain and a high alkaline phosphatase level.
Multigated angiogram (MUGA) scanning is usually performed to assess the cardiac ejection fraction before starting potentially cardiotoxic chemotherapy.
Biopsy
Bilateral iliac crest bone marrow biopsy and aspiration is performed as part of the staging evaluation. Excisional lymph node biopsy is preferred over fine-needle aspiration in patients with suspected lymphoma. Adequate tissue should be obtained for histopathologic and flow cytometric examination.
Skin biopsy may be indicated, although rarely, if lesions suggestive of cutaneous involvement are present.
Lumbar Puncture
Lumbar puncture and cerebrospinal fluid (CSF) examination are warranted in patients with THE following:
-
A paraspinal or paranasal mass
-
Concurrent human immunodeficiency virus (HIV) infection
-
Involvement of the Waldeyer ring
-
Testicular involvement
-
Bone marrow involvement
Histology
Preferably, an experienced hematopathologist should review pathology findings.
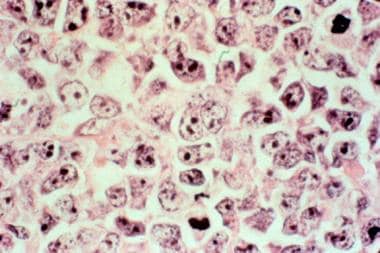
Immunoblastic lymphomas have varying morphologic characteristics, ranging from plasmacytoid features to more pleomorphic characteristics. Generally, they comprise immunoblasts (>90%), with centrally located nucleoli, and centroblasts (must be < 10%) (see the following image).
Immunoblastic lymphoma. Lymph node biopsy (hematoxylin and eosin stain) showing diffuse involvement with loss of architecture in a patient with immunoblastic non-Hodgkin lymphoma (NHL).
Treatment Overview
As discussed earlier, immunoblastic lymphoma is classified as an intermediate-grade non-Hodgkin lymphoma (NHL) and is treated using therapeutic guidelines similar to those used for diffuse large-cell non-Hodgkin lymphoma (DLCL).
Non-Hodgkin lymphoma is treated with chemotherapy, with or without radiation.
The current standard of treatment for immunoblastic lymphoma is combined-modality treatment in the limited stage and chemotherapy only in the advanced stage. CHOP+R regimen (cyclophosphamide, hydroxydaunomycin [doxorubicin], Oncovin [vincristine], prednisone, and rituximab) is the therapy of choice. [9, 10] All other chemotherapeutic regimens are used as salvage treatment.
Patients can be further subclassified as having bulky or nonbulky disease and low, intermediate, or high risk based on the International Prognostic Index (see Prognosis and Prognostic Factors).
Surgical procedures are limited to diagnostic or palliative purposes or for placement of an indwelling central venous catheter.
Admission and transfer
Admit patients for chemotherapy-related toxicity or febrile neutropenia. In addition, those patients who may require high-dose chemotherapy (HDC) and autologous bone marrow transplant (ABMT) require inpatient care until their counts recover, and engraftment is achieved posttransplantation.
Patients may require transfers in following situations:
-
Patients may be transferred to tertiary care centers if HDC and ABMT are being considered for therapy.
-
Patients who have refractory or relapsed disease and who have poor performance status—thus, they’re not candidates for further therapy—may need to be transferred to a terminal care facility.
-
Transfer to a rehabilitation center may be required posttherapy.
-
Home-based nursing care may be required.
Pharmacotherapy
Antibiotics may be needed in episodes of fever postchemotherapy. The choice of antibiotics is usually based on the clinical presentation and clinical findings upon presentation. In cases in which no identifying source is found, broad-spectrum coverage should be started empirically. Most patients require hospitalization and intravenous administration of antibiotics.
Antiemetic agents are usually prescribed for both acute and delayed onset of nausea and vomiting.
In the hospital, intravenous hydration may be warranted in patients with a high tumor burden who are at high risk for tumor lysis syndrome. Allopurinol is usually started in patients with a high tumor burden to prevent tumor lysis syndrome.
Consultations
The following consultations may be needed during the course of treatment:
-
Surgeon - To obtain a tissue biopsy sample or an excisional lymph node biopsy sample for initial diagnosis
-
Interventional radiologist - For placement of an indwelling venous catheter or subcutaneous port for venous access
-
Radiation oncologist - For patients who have limited disease or those with bulky disease who do not require radiotherapy
-
Dietary specialist
-
Social services counselor
Limited Stage I and II Disease
In patients with nonbulky disease and no adverse risk factors, use the cyclophosphamide, hydroxydaunomycin, Oncovin (vincristine), prednisone, and rituximab (CHOP+R) chemotherapy regimen for 3-4 cycles and involved-field radiation therapy (IFRT). [11]
In patients with bulky disease (tumor >10 cm in the greatest dimension) and the presence of an adverse risk factor, use the CHOP+R chemotherapy regimen for 6-8 cycles and involved-field radiation therapy.
In a randomized study by Ennishi et al, CHOP+R therapy (rituximab administered on day 1 of CHOP) emerged to become the standard initial treatment for diffuse large B-cell lymphoma (DLBCL) in the United States. [12]
The benefit of irradiation is still controversial. Chemotherapy followed by consolidation radiotherapy has a 5-year overall survival rate and progression-free survival rates of up to 80%. Rituximab-based chemotherapy and the observation that radiation does not improve overall survival incline for chemotherapy alone. [13]
Advanced Stage III and IV Disease
In patients with low-intermediate risk, use 6-8 cycles of the cyclophosphamide, hydroxydaunomycin, Oncovin (vincristine), prednisone, and rituximab (CHOP+R) chemotherapy regimen.
In individuals with high-intermediate or high risk, use 6-8 cycles of the CHOP+R chemotherapy regimen or offer enrollment in a clinical trial.
High-Dose Chemotherapy and ASCT
Patients with primary resistant or relapsed disease who show some chemosensitivity with second-line salvage therapy should be considered for high-dose chemotherapy (HDC) and autologous stem cell transplantation (ASCT). [14, 15]
Current recommendations are to carefully consider HDC and ASCT for patients in their first relapse, after chemoresponsiveness is established with a second-line salvage therapy. However, the role of HDC plus ASCT in first complete remission for patients who have a slow initial response to front-line chemotherapy, those with poor initial prognostic factors, or as up-front therapy has not been clearly defined and remains controversial.
Salvage Regimens
For primary resistant or refractory cases, the dexamethasone, cisplatin, and cytarabine (DHAP) regimen may be used. Alternatively, consider using the etoposide, methylprednisolone, cisplatin, and cytarabine (ESHAP) regimen. Finally, consider using the methotrexate, [16] bleomycin, Adriamycin (doxorubicin), cyclophosphamide, Oncovin, and dexamethasone (M-BACOD) regimen every 3 weeks.
Follow-Up Monitoring
While on chemotherapy, patients should be monitored very carefully, including complete blood cell (CBC) counts and serum chemistry evaluations. Elderly patients may require home health services, because chemotherapy may compromise their performance status.
Follow up periodically with patients whose condition responds to chemotherapy and who achieve a complete response. Those who have a partial remission should either be treated with a new non–cross-resistant chemotherapy regimen or be considered for the best supportive care.
Patients with indwelling catheters may require daily heparin flushes to prevent clotting.
Growth factors may be required in patients with neutropenia or anemia, such as granulocyte-macrophage colony-stimulating factor (GM-CSF), granulocyte colony-stimulating factor (G-CSF), or recombinant erythropoietin. These are administered subcutaneously and can usually be administered by the patients themselves in an outpatient setting.
For patients who develop severe anemia or thrombocytopenia as a result of chemotherapy, outpatient transfusions may be required.
For patients with concomitant diabetes mellitus, home monitoring of blood glucose may be required while they undergoing chemotherapy, because these patients often develop electrolyte imbalances from nausea/vomiting or hyperglycemia from steroids, which are administered as part of the chemotherapy regimen (eg, cyclophosphamide, hydroxydaunomycin, Oncovin [vincristine], prednisone, and rituximab [CHOP+R]).
Posttreatment periodic follow-up evaluation is essential in these patients, because a substantial number of patients may relapse, especially those categorized as intermediate-high risk or high risk. A complete physical examination, CBC count, and computed tomography (CT) scans are initially performed every 3 months for the first year; the frequency can then be decreased to every 4-6 months depending on the initial risk category of the lymphoma.
Complications
Neutropenic fever, opportunistic infections, and tumor lysis syndrome (ie, hyperuricemia, hyperkalemia, hyperphosphatemia) are all possible complications of immunoblastic lymphoma.
In many cases, even if treated properly, neutropenic fever can be fatal. Shortening the neutropenic phase with cytokines and early induction of prophylactic antibiotics is helpful.
Recognizing the patients who are at risk of tumor lysis syndrome (high uric acid level, high tumor burden) is important. Before chemotherapy, allopurinol, intravenous hydration, and urine alkalization should be started. Renal function should be monitored carefully.
Neutropenia and/or anemia may result from the disease or its treatment. Growth factors (eg, recombinant erythropoietin, interleukin 11 [IL-11], granulocyte-macrophage-colony-stimulating factor [GM-CSF], granulocyte-colony-stimulating factor [G-CSF]) may be indicated in some patients to promote bone marrow proliferation and blood cell production.
Prognosis and Prognostic Factors
Patients undergoing combination chemotherapy may experience long-term morbidity primarily associated with the chemotherapeutic agents.
International Prognostic Index
The International Prognostic Index (IPI) is commonly used to assess the prognosis of aggressive non-Hodgkin lymphoma (NHL). [17, 18] This was established by the International Non-Hodgkin's Lymphoma Prognostic Factors Project as a predictive model for patients with NHL based on 5 adverse pretreatment characteristics, as follows [18] :
-
Age - Older than 60 years
-
Tumor stage - Stages III and IV
-
Number of extranodal sites involved by NHL - More than one
-
Patient performance status - Two or more
-
Lactate dehydrogenase (LDH) level - Elevation above normal values
From the evaluation of the 5 characteristics, patients are classified into 4 categories, as follows:
-
High-risk patients - Four or 5 adverse factors
-
High-intermediate–risk patients - Three adverse factors
-
Low-intermediate–risk patients - Two adverse factors
-
Low-risk patients – No or one adverse factor
Based on these pretreatment risk factors, the complete remission (CR) rate is 87% and the 5-year overall survival rate is 73% for patients who are at low risk compared to 44% and 26%, respectively, in the high-risk group.
Skp2 and p27 as prognostic markers
Seki et al reported there is a significant correlation between poor overall survival and the presence of either high Skp2 expression or low p27 expression; the worst survival rate occurred in their patients with a combination of high Skp2 expression and low p27 expression. [13] The investigators examined the efficacy of CHOP+R therapy in patients with high expression of S-phase kinase-associated protein 2, or Skp2, and/or low expression of cyclin-dependent kinase inhibitor p27(kip1). (Previous evidence has pointed to a role for Skp2 not only in carcinogenesis but also in lymphomagenesis.) Of 671 patients, 425 were treated with CHOP patients and 246 received CHOP+R (246 patients). Due to the correlation of Skp2 and p27 in both treatment groups, Seki et al suggested that, with regard to rituximab treatment, Skp2 and p27 may be useful as prognostic markers. [13]
Patient Education
Patients should receive information about the following:
-
Potential short- and long-term adverse effects of chemotherapy
-
Neutropenic fever
-
Chemotherapy-associated thrombocytopenia and risk of bleeding
-
Avoidance of pregnancy and use of adequate birth control methods in reproductive-aged men or women
-
Sperm banking and other methods to ensure future fertility
-
Possible alteration in menstrual cycles during and after chemotherapy
-
Chemotherapy-induced fatigue
Sterile technique should be emphasized in patients who are prescribed growth factors postchemotherapy at home.
Patients with indwelling catheters should be instructed about daily heparin flushes under aseptic conditions to prevent clotting. Also discuss possible catheter-related complications.
In most instances, no special activity restrictions are required. Special circumstances may require some intervention.
Patients with neutropenia
Patients with neutropenia should follow a neutropenic diet; that is, avoid undercooked meat, and fruits and vegetables should be either cooked or peeled.
All personnel and visitors of neutropenic patients should wash their hands. Neutropenic individuals should avoid contact with persons known to have ongoing viral or bacterial infections, as well as avoid potted plants and flowers, because these may be a source of fungal spores.
Adequately educate patients regarding neutropenic fevers, and emphasize seeking early medical attention in case of fever that may develop postchemotherapy.
Patients with thrombocytopenia
Thrombocytopenic patients should pay special attention to oral hygiene, including frequent rinsing and brushing of teeth only with a toothette sponge. These individuals should also take precautions to avoid falls and to avoid strenuous physical activity.
For patient education information, see Blood and Lymphatic System Center, as well as Lymphoma.
Special Considerations
Potential medicolegal pitfalls include the following:
-
Failure to properly diagnose and stage the lymphoma
-
Failure to clearly explain the short- and long-term adverse effects of chemotherapy agents
-
Failure to clearly explain and discuss issues related to chemotherapy-associated infertility
-
Failure to discuss procedure-related adverse effects and failure to obtain informed consent
-
Adequate pathologic diagnosis
-
History of allergic reaction to medications
-
Risk and hazards associated with blood product transfusions
-
Cases in which a high-dose chemotherapy (HDC) and autologous bone marrow transplantation (ABMT) are required: Discussion of the risk of mortality and morbidity associated with regimen-related toxicity and the long-term follow-up is essential.
-
Immunoblastic lymphoma. Lymph node biopsy (hematoxylin and eosin stain) showing diffuse involvement with loss of architecture in a patient with immunoblastic non-Hodgkin lymphoma (NHL).
Tables

What would you like to print?
- Overview
- Etiology and Pathophysiology
- Clinical Evaluation
- Staging
- Differential Diagnosis
- Laboratory Evaluation
- Cytogenetic Studies
- Radiography, CT Scanning, and MRI
- Nuclear Imaging
- Biopsy
- Lumbar Puncture
- Histology
- Treatment Overview
- Limited Stage I and II Disease
- Advanced Stage III and IV Disease
- High-Dose Chemotherapy and ASCT
- Salvage Regimens
- Follow-Up Monitoring
- Complications
- Prognosis and Prognostic Factors
- Patient Education
- Special Considerations
- Show All
- References








