Hall V. Actinomyces--gathering evidence of human colonization and infection. Anaerobe. 2008 Feb. 14(1):1-7. [QxMD MEDLINE Link].
Ruggiero SL, Mehrotra B, Rosenberg TJ, Engroff SL. Osteonecrosis of the jaws associated with the use of bisphosphonates: a review of 63 cases. J Oral Maxillofac Surg. 2004 May. 62(5):527-34. [QxMD MEDLINE Link].
Markiewicz MR, Margarone JE 3rd, Campbell JH, Aguirre A. Bisphosphonate-associated osteonecrosis of the jaws: a review of current knowledge. J Am Dent Assoc. 2005 Dec. 136(12):1669-74. [QxMD MEDLINE Link].
Hansen T, Kunkel M, Weber A, James Kirkpatrick C. Osteonecrosis of the jaws in patients treated with bisphosphonates - histomorphologic analysis in comparison with infected osteoradionecrosis. J Oral Pathol Med. 2006 Mar. 35(3):155-60. [QxMD MEDLINE Link].
Urbán E, Gajdács M. Microbiological and Clinical Aspects of Actinomyces Infections: What Have We Learned?. Antibiotics (Basel). 2021 Feb 3. 10 (2):[QxMD MEDLINE Link].
Könönen E, Wade WG. Actinomyces and related organisms in human infections. Clin Microbiol Rev. 2015 Apr. 28 (2):419-42. [QxMD MEDLINE Link].
Tuck N, Leatherman J, Assi M, Kallail KJ. A Case of Actinomycosis Presenting as Purulent Pericarditis with Cardiac Tamponade. Kans J Med. 2021. 14:227-228. [QxMD MEDLINE Link].
Shimoda M, Tanaka Y, Kokutou H, Furuuchi K, Osawa T, Morimoto K, et al. Actinomyces meyeri pleural infection that was difficult to treat due to delayed culture: A case report and literature review of 28 cases. Respir Med Case Rep. 2021. 34:101530. [QxMD MEDLINE Link].
Westhoff C. IUDs and colonization or infection with Actinomyces. Contraception. 2007 Jun. 75(6 Suppl):S48-50. [QxMD MEDLINE Link].
Sung HY, Lee IS, Kim SI, Jung SE, Kim SW, Kim SY. Clinical Features of Abdominal Actinomycosis: A 15-year Experience of A Single Institute. J Korean Med Sci. 2011 Jul. 26(7):932-7. [QxMD MEDLINE Link].
Sudhakar SS, Ross JJ. Short-term treatment of actinomycosis: two cases and a review. Clin Infect Dis. 2004 Feb 1. 38(3):444-7. [QxMD MEDLINE Link].
Wolff A, Rodloff AC, Vielkind P, Borgmann T, Stingu CS. Antimicrobial Susceptibility of Clinical Oral Isolates of Actinomyces spp. Microorganisms. 2022 Jan 7. 10 (1):[QxMD MEDLINE Link].
Macfarlane DJ, Tucker LG, Kemp RJ. Treatment of recalcitrant actinomycosis with ciprofloxacin. J Infect. 1993 Sep. 27(2):177-80. [QxMD MEDLINE Link].
Ferreira Dde F, Amado J, Neves S, Taveira N, Carvalho A, Nogueira R. Treatment of pulmonary actinomycosis with levofloxacin. J Bras Pneumol. 2008 Apr. 34(4):245-8. [QxMD MEDLINE Link].
Apotheloz C, Regamey C. Disseminated infection due to Actinomyces meyeri: case report and review. Clin Infect Dis. 1996 Apr. 22(4):621-5. [QxMD MEDLINE Link].
Arend SM, Oosterhof H, van Dissel JT. Actinomyces and the intrauterine device. Arch Intern Med. 1998 Jun 8. 158(11):1270. [QxMD MEDLINE Link].
Belmont MJ, Behar PM, Wax MK. Atypical presentations of actinomycosis. Head Neck. 1999 May. 21(3):264-8. [QxMD MEDLINE Link].
Brown JR. Human actinomycosis. A study of 181 subjects. Hum Pathol. 1973 Sep. 4(3):319-30. [QxMD MEDLINE Link].
Cayley J, Fotherby K, Guillebaud J, et al. Recommendations for clinical practice: actinomyces like organisms and intrauterine contraceptives. The Clinical and Scientific Committee. Br J Fam Plann. 1998 Jan. 23(4):137-8. [QxMD MEDLINE Link].
Chaudhry SI, Greenspan JS. Actinomycosis in HIV infection: a review of a rare complication. Int J STD AIDS. 2000 Jun. 11(6):349-55. [QxMD MEDLINE Link].
Choi J, Koh WJ, Kim TS, et al. Optimal duration of IV and oral antibiotics in the treatment of thoracic actinomycosis. Chest. 2005 Oct. 128(4):2211-7. [QxMD MEDLINE Link].
Chouabe S, Perdu D, Deslee G, et al. Endobronchial actinomycosis associated with foreign body: four cases and a review of the literature. Chest. 2002 Jun. 121(6):2069-72. [QxMD MEDLINE Link].
Cintron JR, Del Pino A, Duarte B, Wood D. Abdominal actinomycosis. Dis Colon Rectum. 1996 Jan. 39(1):105-8. [QxMD MEDLINE Link].
Clarridge JE, Zhang Q. Genotypic diversity of clinical Actinomyces species: phenotype, source, and disease correlation among genospecies. J Clin Microbiol. 2002 Sep. 40(9):3442-8. [QxMD MEDLINE Link].
Colmegna I, Rodriguez-Barradas M, Rauch R, Clarridge J, Young EJ. Disseminated Actinomyces meyeri infection resembling lung cancer with brain metastases. Am J Med Sci. 2003 Sep. 326(3):152-5. [QxMD MEDLINE Link].
Curi MM, Dib LL, Kowalski LP, et al. Opportunistic actinomycosis in osteoradionecrosis of the jaws in patients affected by head and neck cancer: incidence and clinical significance. Oral Oncol. 2000 May. 36(3):294-9. [QxMD MEDLINE Link].
de Montpreville VT, Nashashibi N, Dulmet EM. Actinomycosis and other bronchopulmonary infections with bacterial granules. Ann Diagn Pathol. 1999 Apr. 3(2):67-74. [QxMD MEDLINE Link].
Endo S, Murayama F, Yamaguchi T, et al. Surgical considerations for pulmonary actinomycosis. Ann Thorac Surg. 2002 Jul. 74(1):185-90. [QxMD MEDLINE Link].
Felekouras E, Menenakos C, Griniatsos J, et al. Liver resection in cases of isolated hepatic actinomycosis: case report and review of the literature. Scand J Infect Dis. 2004. 36(6-7):535-8. [QxMD MEDLINE Link].
Fife TD, Finegold SM, Grennan T. Pericardial actinomycosis: case report and review. Rev Infect Dis. 1991 Jan-Feb. 13(1):120-6. [QxMD MEDLINE Link].
Göçmen G, Varol A, Göker K, Basa S. Actinomycosis: report of a case with a persistent extraoral sinus tract. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011 Dec. 112(6):e121-3. [QxMD MEDLINE Link].
Hamid D, Baldauf JJ, Cuenin C, Ritter J. Treatment strategy for pelvic actinomycosis: case report and review of the literature. Eur J Obstet Gynecol Reprod Biol. 2000 Apr. 89(2):197-200. [QxMD MEDLINE Link].
Hansen T, Kunkel M, Kirkpatrick CJ, Weber A. Actinomyces in infected osteoradionecrosis--underestimated?. Hum Pathol. 2006 Jan. 37(1):61-7. [QxMD MEDLINE Link].
Hsieh MJ, Liu HP, Chang JP, Chang CH. Thoracic actinomycosis. Chest. 1993 Aug. 104(2):366-70. [QxMD MEDLINE Link].
Huang KL, Beutler SM, Wang C. Endocarditis due to Actinomyces meyeri. Clin Infect Dis. 1998 Oct. 27(4):909-10. [QxMD MEDLINE Link].
Kim JC, Ahn BY, Kim HC, et al. Efficiency of combined colonoscopy and computed tomography for diagnosis of colonic actinomycosis: a retrospective evaluation of eight consecutive patients. Int J Colorectal Dis. 2000 Aug. 15(4):236-42. [QxMD MEDLINE Link].
Kim TS, Han J, Koh WJ, et al. Thoracic Actinomycosis: CT Features with Histopathologic Correlation. AJR Am J Roentgenol. 2006 Jan. 186(1):225-31. [QxMD MEDLINE Link].
Kuijper EJ, Wiggerts HO, Jonker GJ, et al. Disseminated actinomycosis due to Actinomyces meyeri and Actinobacillus actinomycetemcomitans. Scand J Infect Dis. 1992. 24(5):667-72. [QxMD MEDLINE Link].
Lequerre T, Nouvellon M, Kraznowska K, et al. Septic arthritis due to Actinomyces naeslundii: report of a case. Joint Bone Spine. 2002 Oct. 69(5):499-501. [QxMD MEDLINE Link].
Lippes J. Pelvic actinomycosis: a review and preliminary look at prevalence. Am J Obstet Gynecol. 1999 Feb. 180(2 Pt 1):265-9. [QxMD MEDLINE Link].
Litwin KA, Jadbabaie F, Villanueva M. Case of pleuropericardial disease caused by Actinomyces odontolyticus that resulted in cardiac tamponade. Clin Infect Dis. 1999 Jul. 29(1):219-20. [QxMD MEDLINE Link].
Mabeza GF, Macfarlane J. Pulmonary actinomycosis. Eur Respir J. 2003 Mar. 21(3):545-51. [QxMD MEDLINE Link].
Macfarlane DJ, Tucker LG, Kemp RJ. Treatment of recalcitrant actinomycosis with ciprofloxacin. J Infect. 1993 Sep. 27(2):177-80. [QxMD MEDLINE Link].
Oostman O, Smego RA. Cervicofacial Actinomycosis: Diagnosis and Management. Curr Infect Dis Rep. 2005 May. 7(3):170-174. [QxMD MEDLINE Link].
Pulverer G, Schutt-Gerowitt H, Schaal KP. Human cervicofacial actinomycoses: microbiological data for 1997 cases. Clin Infect Dis. 2003 Aug 15. 37(4):490-7. [QxMD MEDLINE Link].
Reddy I, Ferguson DA Jr, Sarubbi FA. Endocarditis due to Actinomyces pyogenes. Clin Infect Dis. 1997 Dec. 25(6):1476-7. [QxMD MEDLINE Link].
Rothschild B, Naples V, Barbian L. Bone manifestations of actinomycosis. Ann Diagn Pathol. 2006 Feb. 10(1):24-27. [QxMD MEDLINE Link].
Sabbe LJ, Van De Merwe D, Schouls L, et al. Clinical spectrum of infections due to the newly described Actinomyces species A. turicensis, A. radingae, and A. europaeus. J Clin Microbiol. 1999 Jan. 37(1):8-13. [QxMD MEDLINE Link].
Scarano FJ, Ruddat MS, Robinson A. Actinomyces viscosus postoperative endophthalmitis. Diagn Microbiol Infect Dis. 1999 Jun. 34(2):115-7. [QxMD MEDLINE Link].
Schaal KP, Lee HJ. Actinomycete infections in humans--a review. Gene. 1992 Jun 15. 115(1-2):201-11. [QxMD MEDLINE Link].
Schaal KP, Pape W. Special methodological problems in antibiotic susceptibility testing of fermentative actinomycetes. Infection. 1980. 8 Suppl 2:S176-82. [QxMD MEDLINE Link].
Sharma M, Briski LE, Khatib R. Hepatic actinomycosis: an overview of salient features and outcome of therapy. Scand J Infect Dis. 2002. 34(5):386-91. [QxMD MEDLINE Link].
Smego RA Jr, Foglia G. Actinomycosis. Clin Infect Dis. 1998 Jun. 26(6):1255-61; quiz 1262-3. [QxMD MEDLINE Link].
Smith AJ, Hall V, Thakker B, Gemmell CG. Antimicrobial susceptibility testing of Actinomyces species with 12 antimicrobial agents. J Antimicrob Chemother. 2005 Aug. 56(2):407-9. [QxMD MEDLINE Link].
Soria-Aledo V, Flores-Pastor B, Carrasco-Prats M, et al. Abdominopelvic actinomycosis: a serious complication in intrauterine device users. Acta Obstet Gynecol Scand. 2004 Sep. 83(9):863-5. [QxMD MEDLINE Link].
Wagenlehner FM, Mohren B, Naber KG, Mannl HF. Abdominal actinomycosis. Clin Microbiol Infect. 2003 Aug. 9(8):881-5. [QxMD MEDLINE Link].
Warren NG. Actinomycosis, nocardiosis, and actinomycetoma. Dermatol Clin. 1996 Jan. 14(1):85-95. [QxMD MEDLINE Link].
Weese WC, Smith IM. A study of 57 cases of actinomycosis over a 36-year period. A diagnostic 'failure' with good prognosis after treatment. Arch Intern Med. 1975 Dec. 135(12):1562-8. [QxMD MEDLINE Link].
Wust J, Steiger U, Vuong H, Zbinden R. Infection of a hip prosthesis by Actinomyces naeslundii. J Clin Microbiol. 2000 Feb. 38(2):929-30. [QxMD MEDLINE Link].
Xia T, Baumgartner JC. Occurrence of Actinomyces in infections of endodontic origin. J Endod. 2003 Sep. 29(9):549-52. [QxMD MEDLINE Link].
Yung BC, Cheng JC, Chan TT, et al. Aggressive thoracic actinomycosis complicated by vertebral osteomyelitis and epidural abscess leading to spinal cord compression. Spine. 2000 Mar 15. 25(6):745-8. [QxMD MEDLINE Link].
Stájer A, Ibrahim B, Gajdács M, Urbán E, Baráth Z. Diagnosis and Management of Cervicofacial Actinomycosis: Lessons from Two Distinct Clinical Cases. Antibiotics (Basel). 2020 Mar 25. 9 (4):[QxMD MEDLINE Link].
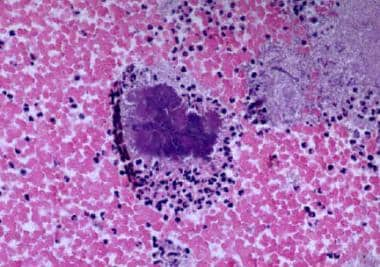 Actinomycosis in the endometrial tissue, low-power view. Image courtesy of Paul Gibbs, MD.
Actinomycosis in the endometrial tissue, low-power view. Image courtesy of Paul Gibbs, MD.
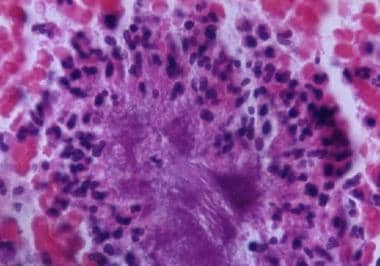 Actinomycosis in the endometrial tissue, high-power view. Image courtesy of Paul Gibbs, MD.
Actinomycosis in the endometrial tissue, high-power view. Image courtesy of Paul Gibbs, MD.








