Approach Considerations
Bacillus anthracis is present in high numbers in the ulcer/eschar of cutaneous anthrax, in bloody pleural fluid in inhalational anthrax, in the cerebrospinal fluid (CSF) in anthrax meningitis, and in the blood in septicemic anthrax. Specimens may be stained or cultured to demonstrate the organism. Culture is performed on sheep blood or peptone agar. In persons exposed to antibiotics, immunohistochemical examination of the suspected fluid (eg pleural fluid, CSF, cutaneous biopsy) is performed using antibodies to B anthracis cell wall and capsule.
The diagnosis of cutaneous anthrax is usually suggested by the characteristic appearance of skin lesions. As spore germination occurs within macrophages at the site of inoculation, anthrax bacilli are isolated easily from the vesicular lesions and can be observed on Gram stain. If prior treatment with antibiotics has occurred, the best way to determine infection is to perform serologic testing and punch biopsy at the edge of the lesion and examine by silver staining and immunohistochemical testing.
In patients with inhalational anthrax, a chest radiograph typically shows widening of the mediastinum and pleural effusions, whereas the parenchyma may appear normal. In a review of the 11 patients infected by anthrax in October 2001, chest radiographs from the initial examination showed mediastinal widening, paratracheal and hilar fullness, and pleural effusions or infiltrates. In some patients, the initial findings were subtle and not detected immediately.
Gram Stain and Blood Culture
The preferred diagnostic procedure for cutaneous anthrax is staining the ulcer exudate with methylene blue or Giemsa stain. B anthracis readily grows on blood agar, and staining microbiologically differentiates the organism from non– B anthracis bacilli. Warn laboratory personnel that contracting anthrax from specimens is possible and that they must take appropriate biohazard (level II) precautions.
 Polychrome methylene blue stain of Bacillus anthracis. Image courtesy of Anthrax Vaccine Immunization Program Agency, Office of the Army Surgeon General, United States.
Polychrome methylene blue stain of Bacillus anthracis. Image courtesy of Anthrax Vaccine Immunization Program Agency, Office of the Army Surgeon General, United States.
In patients with cutaneous anthrax who have fever and systemic symptoms that suggest extracutaneous spread, blood culture may be indicated. Treat blood cultures as biohazard II specimens. Blood culture and Gram stain are high-yield tests in infected persons who have not taken antibiotics. Sputum from patients seldom yields positive smears or cultures. A Gram stain is the easiest means of initially identifying suggested cases. Anthrax appears as a large, gram-positive rod.
In October 2001, blood cultures were positive for anthrax in all 8 patients who did not receive antibiotics. Serologic diagnosis of anthrax can be made using a microhemagglutination test specific for the protective antigen (PA) component of the toxin. Any Gram stain results suggestive of anthrax should be reported to the CDC.
Several biochemical tests aid in differentiating B anthracis from other members of the species (chief among them is Bacillus cereus, which has been associated with outbreaks of human food poisoning). B anthracis is characterized by the absence of hemolysis on sheep blood agar, lack of motility, absence of salicin fermentation, gelatin hydrolysis, and lack of growth on phenylethyl alcohol medium.
Enzyme-Linked Immunosorbent Assay
Enzyme-linked immunosorbent assay (ELISA) serologic diagnosis is also available. The ELISA for edema and lethal toxins is positive if a single acute-phase titer is highly elevated or if a fourfold greater rise in the titer is observed between acute and convalescent specimens.
ELISA to detect immunoglobulin G (IgG) response to B anthracis protective antigen (PA) is 98.6% sensitive and 80% specific. Protective antigen–competitive inhibition ELISA is used as a second confirmatory step to improve specificity. Specific IgG anti-PA antibody can be detected as early as 10 days after onset of symptoms, but peak IgG levels may not be observed until 40 days of symptom onset.
Chest Radiography and Computed Tomography
If inhalational anthrax is suspected, obtain a chest radiograph or computed tomography (CT) scan. The appearance on chest radiograph or CT scan may suggest the diagnosis, especially if other predisposing disorders that might result in a widening mediastinum (eg, dissecting aortic aneurysm, bacterial mediastinitis) are absent.
 Inhalation anthrax. Chest radiograph with widened mediastinum 22 hours before death. Image courtesy of P.S. Brachman, MD, Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
Inhalation anthrax. Chest radiograph with widened mediastinum 22 hours before death. Image courtesy of P.S. Brachman, MD, Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
Inhalational anthrax often does not appear on chest radiographs as a typical pneumonia; pulmonary densities often are absent. A prominent mediastinum with pleural effusions may be present. The prominent mediastinum is caused by hilar lymphadenopathy. In the 11 cases of inhalational anthrax, initial examination was often subtle but showed mediastinal widening, paratracheal and hilar fullness, and pleural effusions and/or infiltrates.
CT of the chest detects hemorrhagic mediastinal and hilar lymph nodes and edema, peribronchial thickening, and pleural effusions. It also may help differentiate inhalational anthrax from histoplasmosis, sarcoidosis, tuberculosis, and lymphoma.
Lumbar Puncture
If anthrax meningitis is suspected, perform a lumbar puncture to obtain CSF for stain and culture. The CSF in patients with anthrax meningitis is grossly hemorrhagic with few polymorphonuclear neutrophils (PMNs) and numerous gram-positive bacilli. As with other specimens from patients with possible anthrax, advise laboratory personnel to handle specimens with biohazard level II precautions.
Histologic Findings
The characteristic finding in anthrax is the presence of the organisms in the capillaries at the infection site; therefore, if a patient is infected, expect B anthracis in the capillaries of the skin, intestines, liver, spleen, lungs, or leptomeninges. Pathological findings are not in proportion to the numbers of bacilli present, which is best explained by the effects of one or more of the toxins associated with B anthracis. Hemorrhage may be evident.
 Histopathology of mediastinal lymph node showing a microcolony of Bacillus anthracis on Giemsa stain. Image courtesy of Marshall Fox, MD, Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
Histopathology of mediastinal lymph node showing a microcolony of Bacillus anthracis on Giemsa stain. Image courtesy of Marshall Fox, MD, Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
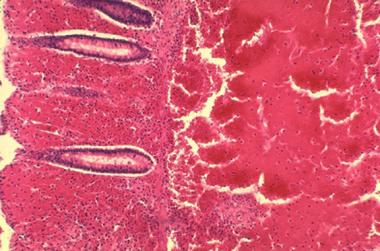 Histopathology of large intestine showing marked hemorrhage in the mucosa and submucosa. Image courtesy of Marshall Fox, MD, Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
Histopathology of large intestine showing marked hemorrhage in the mucosa and submucosa. Image courtesy of Marshall Fox, MD, Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
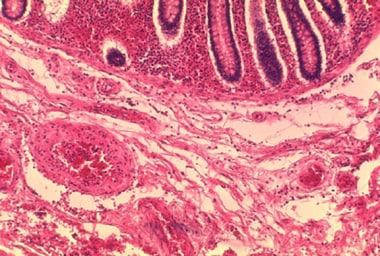 Histopathology of the large intestine showing submucosal thrombosis and edema. Image courtesy of Marshall Fox, MD, Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
Histopathology of the large intestine showing submucosal thrombosis and edema. Image courtesy of Marshall Fox, MD, Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
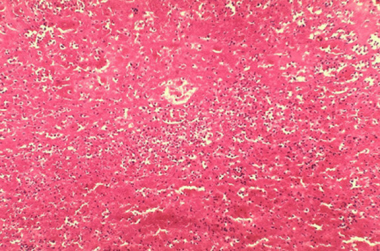 Histopathology of mediastinal lymph node showing mediastinal necrosis. Image courtesy of Marshall Fox, MD, Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
Histopathology of mediastinal lymph node showing mediastinal necrosis. Image courtesy of Marshall Fox, MD, Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
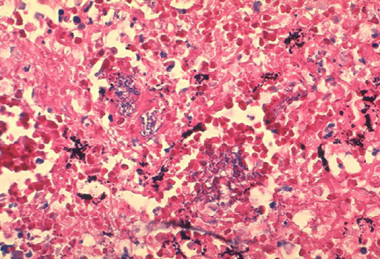
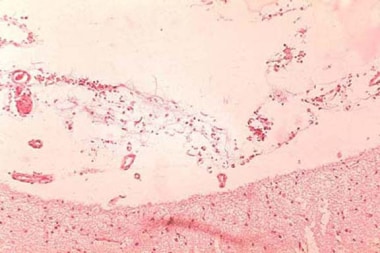 Anthrax infection. Histopathology of hemorrhagic meningitis in anthrax. Image courtesy of Marshall Fox, MD, Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
Anthrax infection. Histopathology of hemorrhagic meningitis in anthrax. Image courtesy of Marshall Fox, MD, Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
-
Polychrome methylene blue stain of Bacillus anthracis. Image courtesy of Anthrax Vaccine Immunization Program Agency, Office of the Army Surgeon General, United States.
-
Histopathology of mediastinal lymph node showing a microcolony of Bacillus anthracis on Giemsa stain. Image courtesy of Marshall Fox, MD, Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
-
Cutaneous anthrax. Image courtesy of Anthrax Vaccine Immunization Program Agency, Office of the Army Surgeon General, United States.
-
Skin lesion of anthrax on face. Image courtesy of the Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
-
Skin lesions of anthrax on neck. Cutaneous anthrax showing the typical black eschar. Image courtesy of the Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
-
Histopathology of large intestine showing marked hemorrhage in the mucosa and submucosa. Image courtesy of Marshall Fox, MD, Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
-
Histopathology of the large intestine showing submucosal thrombosis and edema. Image courtesy of Marshall Fox, MD, Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
-
Inhalation anthrax. Chest radiograph with widened mediastinum 22 hours before death. Image courtesy of P.S. Brachman, MD, Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
-
Histopathology of mediastinal lymph node showing mediastinal necrosis. Image courtesy of Marshall Fox, MD, Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
-
Hemorrhagic meningitis resulting from inhalation anthrax. Image courtesy of the Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
-
Anthrax infection. Histopathology of hemorrhagic meningitis in anthrax. Image courtesy of Marshall Fox, MD, Public Health Image Library, US Centers for Disease Control and Prevention, Atlanta, Georgia.
-
Microscopic picture of anthrax showing gram-positive rods. Image courtesy of Ramon E. Moncada, MD.
-
Seven-month-old infant with anthrax. In this infant, the infection progressed rapidly with significant edema developing the day after exposure. This large hemorrhagic lesion developed within 3 more days. The infant was febrile and was admitted to the hospital on the second day after the symptoms appeared.On September 28, 2001, the infant had visited the mother's workplace. On September 29, nontender massive edema and a weeping erosion developed. On September 30, a 2-cm sore developed over the edematous area. (Note that edema preceded the primary lesion.) On October 2, an ulcer or eschar formed, and the lesion was diagnosed as a spider bite. Hemolytic anemia and thrombocytopenia developed, and the patient was hospitalized. Serum was drawn on October 2; the polymerase chain reaction results were positive for Bacillus anthracis. On October 13, skin biopsy results were positive with immunohistochemical testing for the cell wall antigen.Note that the initial working diagnosis was a Loxosceles reclusa spider bite with superimposed cellulitis. Courtesy of American Academy of Dermatology with permission of NEJM.
-
Fourth patient with cutaneous anthrax in New York City, October 2001. This dry ulcer was present. Photo used with permission of the patient. Courtesy of American Academy of Dermatology. Courtesy of Sharon Balter of the New York City Department of Health.
-
Note the hemorrhage that is associated with cutaneous anthrax lesions. The early ulcer has a moist base. Courtesy of American Academy of Dermatology.
-
Note the central ulcer and eschar. Courtesy of American Academy of Dermatology.
-
An example of a central ulcer and eschar with surrounding edema. Courtesy of American Academy of Dermatology with permission from Boni Elewski, MD.
-
Note the black eschar. Courtesy of American Academy of Dermatology. Courtesy of Gorgas Course in Clinical Tropical Medicine.
-
Anthrax with facial edema. Courtesy of American Academy of Dermatology.
Tables
- Table 1. Microbiological Differences Between B anthracis and Non– B anthracis Bacilli
- Table 2. Toxins and Protein Toxins of Bacillus anthracis
- Table 3. CDC Expert Panel Recommendations for Treatment of Cutaneous Anthrax
- Table 4. CDC Expert Panel Recommendations for Treatment of Systemic Anthrax Without Meningitis [15]
- Table 5. CDC Expert Panel Recommendations for Treatment of Anthrax Meningitis [15]
B anthracis |
Non–B anthracis bacilli (pseudoanthrax bacilli) |
Nonmotile long chains |
Generally motile short chains |
Capsule formation on bicarbonate agar |
No capsule formation in bicarbonate |
No growth on penicillin agar (10 mcg/mL) |
Usually good growth on penicillin agar |
Growth in gelatin resembles inverted fir tree |
Growth in gelatin absent or resembles atypical fir tree |
Gelatin liquefaction slow |
Gelatin liquefaction usually rapid |
No hemolysis of sheep RBCs |
Hemolysis of sheep RBCs |
Ferments salicin slowly or not at all |
Usually ferments salicin rapidly |
Pathogenic to laboratory animals |
Nonpathogenic to laboratory animals |
Adapted from Cunha CB. Anthrax: Ancient Plague, Persistent Problem. Infect Dis Pract. 1999;23(4):35-9. |
|
Edema factor (EF) + lethal factor (LF) = Host cell penetration by B anthracis |
EF + protective antigen (PA) = Edema toxin |
LF + PA = Lethal toxin (primary virulence factor of B anthracis) |
Edema toxin + lethal toxin = Inhibited PMN function and phagocytosis |
Nonpregnant adults |
Pregnant/lactating women |
Children |
|---|---|---|
Recommended therapy [15] : Treatment duration, 7-10 days |
||
Ciprofloxacin 500 mg every 12 hours |
Ciprofloxacin 500 mg every 12 hours |
Ciprofloxacin 30 mg/kg/day divided every 12 hours (max dose, 500 mg/dose) |
Doxycycline 100 mg every 12 hours |
Amoxicillin 75 mg/kg/day divided every 8 hours (max dose, 1 g/dose) |
|
Levofloxacin 750 mg every 12 hours |
||
Moxifloxacin 400 mg every 24 hours |
||
Alternative therapy |
||
Clindamycin 600 mg every 8 hours |
Levofloxacin 750 mg every 12 hours |
Doxycycline < 45 kg: 4.4 mg/kg/day divided every 12 hours (max dose, 100 mg/dose) >45 kg: 100 mg every 12 hours |
Amoxicillin 1 g every 8 hours (susceptible strain only) |
Amoxicillin 1 g every 8 hours (susceptible strain only) |
Clindamycin 30 mg/kg/day divided every 8 hours (max dose, 600 mg/dose) |
Levofloxacin < 50 kg: 16 mg/kg/day divided every 12 hours (max dose, 250 mg/dose) >50 kg: 500 mg every 24 hours |
||
Adults |
Children |
|---|---|
1. Bactericidal agent |
|
Ciprofloxacin 400 mg every 8 hours |
Ciprofloxacin 30 mg/kg/day divided every 8 hours (max dose, 400 mg/dose) |
Alternative |
|
Levofloxacin 750 mg every 24 hours -OR- |
Meropenem 60 mg/kg/day divided every 8 hours (max dose, 2 g/dose) -OR- |
Moxifloxacin 400 mg every 24 hours -OR- |
Levofloxacin < 50 kg: 20 mg/kg/day divided every 12 hours (max dose, 250 mg/dose) >50 kg: 500 mg every 24 hours -OR- |
Meropenem 2 g every 8 hours -OR- |
Imipenem 100 mg/kg/day divided every 6 hours (max dose, 1 g/dose) -OR- |
Imipenem 1 g every 6 hours -OR- |
Vancomycin 60 mg/kg/day divided every 8 hours (max dose, 2 g/dose); trough target, 15-20 mcg/mL |
Doripenem 500 mg every 8 hours -OR- |
|
Vancomycin 60 mg/kg/day divided every 8 hours (max dose, 2 g/dose); trough target, 15-20 mcg/mL |
|
PLUS |
|
2. Protein synthesis inhibitor |
|
Clindamycin 900 mg every 8 hours -OR- |
Clindamycin 40 mg/kg/day divided every 8 hours (max dose, 900 mg/dose) |
Linezolid 600 mg every 12 hours |
|
Alternative |
|
Doxycycline 200-mg loading dose followed by 100 mg every 12 hours -OR- |
Linezolid < 12 years: 30 mg/kg/day divided every 8 hours >12 years: 30 mg/kg/day divided every 12 hours (max dose, 600 mg/dose) -OR- |
Rifampin 600 mg every 12 hours |
Doxycycline < 45 kg: 4.4 mg/kg loading dose (max 200 mg) followed by 4.4 mg/kg/day divided every 12 hours (max 100 mg/dose) >45 kg: 200 mg loading dose followed by 100 mg every 12 hours -OR- |
Rifampin 20 mg/kg/day divided every 12 hours (max dose, 300 mg/dose) |
|
Adults |
Children |
|---|---|
1. Bactericidal agent |
|
Ciprofloxacin 400 mg every 8 hours |
Ciprofloxacin 30 mg/kg/day divided every 8 hours (max 400 mg/dose) |
Alternative |
|
Levofloxacin 750 mg every 24 hours -OR- |
Levofloxacin < 50 kg: 16 mg/kg/day divided every 12 hours (max 250 mg/dose) ≥50 kg: 500 mg every 24 hours -OR- |
Moxifloxacin 400 mg every 24 hours |
Moxifloxacin Age 3 months to < 2 years: 12 mg/kg/day divided every 12 hours Age 2-5 years: 10 mg/kg/day divided every 12 hours Age 6-11 years: 8 mg/kg/day divided every 12 hours Age 12-17 years, < 45 kg: 8 mg/kg/day divided every 12 hours (Max 200 mg/dose) Age 12-17 years, ≥45 kg: 400 mg every 24 hours |
PLUS |
|
2. Second bactericidal agent |
|
Meropenem 2 g every 8 hours |
Meropenem 120 mg/kg/dose divided every 8 hours (max 2 g/dose) |
Alternative |
|
Imipenem 1 g every 6 hours -OR- |
Imipenem 100 mg/kg/day divided every 6 hours (max 1 g/dose) -OR- |
Doripenem 500 mg every 8 hours -OR- |
Doripenem 120 mg/kg/day divided every 8 hours (max 1 g/dose) -OR- |
Ampicillin 3 g every 6 hours -OR- |
Vancomycin 60 mg/kg/day divided every 8 hours (max 2 g/dose); target trough, 15-20 mcg/mL -OR- |
Ampicillin 400 mg/kg/day divided every 6 hours (max 3 g/dose) |
|
PLUS |
|
3. Protein synthesis inhibitor |
|
Linezolid 600 mg every 12 hours |
Linezolid < 12 years old: 30 mg/kg/day divided every 8 hours ≥12 years old: 30 mg/kg/day divided every 12 hours (Max 600 mg/dose) |
Alternative |
|
Clindamycin 900 mg every 8 hours -OR- |
Clindamycin 40 mg/kg/day divided every 8 hours (max 900 mg/dose) -OR- |
Rifampin 600 mg every 12 hours -OR- |
Rifampin 20 mg/kg per day divided every 12 hours (max 300 mg/dose) -OR- |
Chloramphenicol 1 g every 6-8 hours |
Chloramphenicol 100 mg/kg per day divided every 6 hours (max 1 g/dose) |








