Approach Considerations
Generally, no workup is required in uncomplicated cases of cellulitis that meet the following criteria [1] :
-
Limited area of involvement
-
Minimal pain
-
No systemic signs of illness (eg, fever, chills, dehydration, altered mental status, tachypnea, tachycardia, hypotension)
-
No risk factors for serious illness (eg, extremes of age, general debility, immunocompromised status)
Because the bacterial etiology of cellulitis in typical cases is expected to represent streptococcal and, less commonly, staphylococcal infection, additional procedures are also usually unnecessary. However, in more severe disease or unique clinical scenarios, additional procedures may be indicated. [1]
For serious infections, perform a blood culture, Gram stain, and culture of needle aspiration or punch biopsy specimens to pinpoint the etiology. [4] Blood cultures are only positive in 5%-15% of patients with cellulitis. Aspiration of the leading edge of cellulitis margins rarely yields positive results but may be performed if clinicians are facing difficult situations.
The IDSA recommends bloodwork for patients with skin or soft tissue infection (SSTI) who have signs and symptoms of systemic toxicity; such tests include blood cultures, complete blood cell (CBC) with differential, and levels of creatinine, bicarbonate, creatine phosphokinase, and C-reactive protein (CRP). [4]
Considerations for hospitalization
The IDSA also recommends considering inpatient admission in the presence of hypotension and/or the following laboratory findings: an elevated creatinine level; an elevated creatine phosphokinase level (2-3 times the upper limit of normal [ULN]); a CRP level >13 mg/L (123.8 mmol/L); a low serum bicarbonate level; or a marked left shift on the CBC with differential. [4]
If a complicated or deep infection is suspected, imaging studies and/or surgical consultations should be done promptly. [4]
Jenkins et al also developed guidelines for the management of patients who require hospitalization for cellulitis or cutaneous abscess. The guidelines were shown to decrease the use of resources without an adverse effect on clinical outcomes. [69]
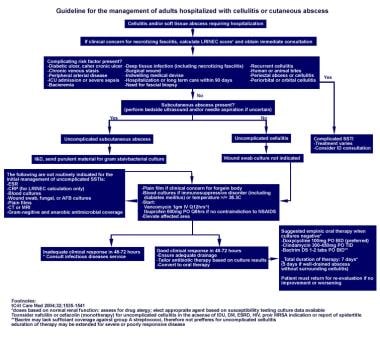 Guidelines for the management of patients who require hospitalization for cellulitis or cutaneous abscess. AFB = acid-fast bacilli; BID = twice daily; CRP = C reactive protein; CT = computed tomography scanning; DS = double strength; DM = diabetes mellitus; ESR = erythrocyte sedimentation rate; ESRD = end-stage renal disease; HIV = human immunodeficiency virus; ICU = intensive care unit; I&D = incision and drainage; ID = infectious disease; IDU = injection drug user; IV = intravenous; LRINEC = Laboratory Risk Indicator for Necrotizing Fasciitis; MRI = magnetic resonance imaging; MSRA = methicillin-resistant Staphylococcus aureus; NSAIDS = nonsteroidal anti-inflammatory drugs; PO = by mouth; SSTI = skin and soft-tissue infections; TID = 3 times daily. Adapted from Jenkins TC, Knepper BC, Sabel AL, et al. Decreased antibiotic utilization after implementation of a guideline for inpatient cellulitis and cutaneous abscess. Arch Intern Med. 2011;171(12):1072-9.
Guidelines for the management of patients who require hospitalization for cellulitis or cutaneous abscess. AFB = acid-fast bacilli; BID = twice daily; CRP = C reactive protein; CT = computed tomography scanning; DS = double strength; DM = diabetes mellitus; ESR = erythrocyte sedimentation rate; ESRD = end-stage renal disease; HIV = human immunodeficiency virus; ICU = intensive care unit; I&D = incision and drainage; ID = infectious disease; IDU = injection drug user; IV = intravenous; LRINEC = Laboratory Risk Indicator for Necrotizing Fasciitis; MRI = magnetic resonance imaging; MSRA = methicillin-resistant Staphylococcus aureus; NSAIDS = nonsteroidal anti-inflammatory drugs; PO = by mouth; SSTI = skin and soft-tissue infections; TID = 3 times daily. Adapted from Jenkins TC, Knepper BC, Sabel AL, et al. Decreased antibiotic utilization after implementation of a guideline for inpatient cellulitis and cutaneous abscess. Arch Intern Med. 2011;171(12):1072-9.
Moderate to Severe Cases and Systemic Symptoms
The following laboratory tests may be considered in patients who present with moderate to severe cellulitis and/or systemic symptoms [1] :
A complete blood cell (CBC) count often shows leukocytosis in the setting of severe disease; leukopenia may also be present in severe disease, especially in cases of toxin-mediated cellulitis.
The erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level are also frequently elevated, especially in patients with severe disease requiring prolonged hospitalization. [65]
In most cases of cellulitis, blood cultures are neither necessary nor cost-effective, [12, 70] but they should be performed in patients with moderate to severe disease, [4] such as patients with cellulitis complicating lymphedema, [6] because the prevalence of bacteremia is higher in these individuals. Blood cultures are also recommended for cellulitis of specific anatomic sites, such as facial and especially ocular areas; in patients with a history of contact with potentially contaminated water; in patients with malignancy on chemotherapy, neutropenia, or severe cell-mediated immunodeficiency; and in patients with animal bites.
Gram stain, whether obtained via biopsy or aspiration of the infected area, has a low yield and is unnecessary in most cases, unless purulent material is draining or bullae or abscess is present.
If recurrent episodes of cellulitis are suspected to be secondary to tinea pedis or onychomycosis, mycologic investigations are advisable.
Creatinine levels may be helpful to assess baseline renal function in order to correctly prescribe antimicrobial agents.
Ultrasonography, CT Scanning, and MRI
Current data suggest that ultrasonography may play a role in the detection of occult abscess and direction of care, especially in an emergency department setting. [8] Ultrasonographic-guided aspiration of pus has been shown to shorten hospital stay and fever duration in children with cellulitis. [9]
If necrotizing fasciitis is a concern, computed tomographic (CT) imaging is typically used to help rule out this condition in stable patients; magnetic resonance imaging (MRI) can be performed, [10] but MRI typically takes much longer than CT scanning. However, strong clinical suspicion of necrotizing fasciitis should prompt surgical consultation without delay for imaging. [1]
Aspiration, Dissection, and Biopsy
Needle aspiration should be performed only in selected patients and/or in unusual cases, such as in cases of cellulitis with bullae or in patients who have diabetes, are immunocompromised, are neutropenic, are not responding to empiric therapy, or have a history of animal bites or immersion injury. [1, 11, 12, 13]
Aspiration or punch biopsy of the inflamed area may have a culture yield of 2-40% and is of limited clinical value in most cases. [14] By contrast, Gram stain and culture following incision and drainage of an abscess yields positive results in more than 90% of cases. [4]
Dissection of the underlying fascia to assess for necrotizing fasciitis may be determined by surgical consultation or indicated following initial evaluation and imaging studies. [1, 15]
Skin biopsy is not routine but may be performed in an attempt to rule out a noninfectious entity. Tissue stains and microscopy reveal findings of soft tissue inflammation. Leukocyte infiltration, capillary dilatation, and bacterial invasion of tissue are observed. [1]
Histologic Findings
In cases in which cellulitis is extensive and tissue is no longer viable, debridement may be performed. In such cases, the normally bright-yellow fat becomes hemorrhagic and necrotic. Microscopic evaluation shows clusters of neutrophils (acute inflammation) invading adipose tissue, which can produce fat necrosis if it is extensive enough. An abscess forms when neutrophils aggregate into large clusters. Rarely, organisms can be seen on routine histologic stains. [1]
 Gross photograph of complicated cellulitis. Instead of the presence of yellow fat, the tissue is hemorrhagic and necrotic.
Gross photograph of complicated cellulitis. Instead of the presence of yellow fat, the tissue is hemorrhagic and necrotic.
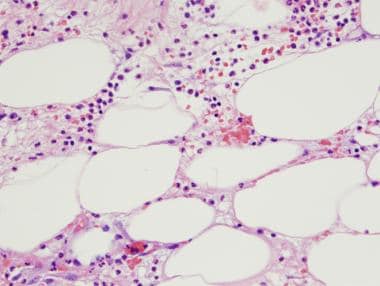 Hematoxylin and eosin (H&E) stain, high power. This image shows deeper subcutaneous tissue involved in a case of cellulitis, with acute inflammatory cells and fat necrosis.
Hematoxylin and eosin (H&E) stain, high power. This image shows deeper subcutaneous tissue involved in a case of cellulitis, with acute inflammatory cells and fat necrosis.
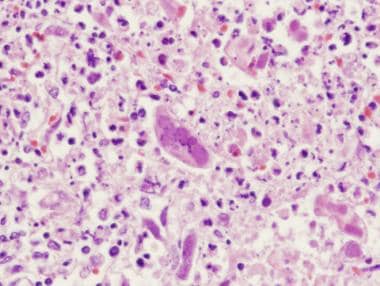 Hematoxylin and eosin (H&E) stain, high power. This image shows cellulitis caused by herpes simplex virus, with the multinucleated organism in the center of the picture.
Hematoxylin and eosin (H&E) stain, high power. This image shows cellulitis caused by herpes simplex virus, with the multinucleated organism in the center of the picture.
-
Mild cellulitis with a fine lacelike pattern of erythema. This lesion was only slightly warm and caused minimal pain, which is typical for the initial presentation of mild cellulitis.
-
Swelling seen in cellulitis involving the hand. In a situation with hand cellulitis, always rule out deep infection by imaging studies or by obtaining surgical consultation.
-
Severe cellulitis of the leg in a woman aged 80 years. The cellulitis developed beneath a cast and was painful and warm to the touch. Significant erythema is evident. The margins are irregular but not raised. An ulcerated area is visible in the center of the photograph.
-
Burns complicated by cellulitis. The larger lesion is a second-degree burn (left), and the smaller lesion is a first-degree burn (right), each with an expanding zone of erythema consistent with cellulitis.
-
Cellulitis due to documented Vibrio vulnificus infection. (Image courtesy of Kepler Davis.)
-
A case of cellulitis without associated purulence in an infant. Note the presence of lymphedema, a risk factor for cellulitis.(Photo courtesy of Amy Williams.)
-
Patient with cellulitis of the left ankle. This cellulitis was caused by community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA). (Photo courtesy of Texas Dept. of Public Health.)
-
Abscess and associated cellulitis caused by community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA). (Photo courtesy of Texas Dept. of Public Health.)
-
Guidelines for the management of patients who require hospitalization for cellulitis or cutaneous abscess. AFB = acid-fast bacilli; BID = twice daily; CRP = C reactive protein; CT = computed tomography scanning; DS = double strength; DM = diabetes mellitus; ESR = erythrocyte sedimentation rate; ESRD = end-stage renal disease; HIV = human immunodeficiency virus; ICU = intensive care unit; I&D = incision and drainage; ID = infectious disease; IDU = injection drug user; IV = intravenous; LRINEC = Laboratory Risk Indicator for Necrotizing Fasciitis; MRI = magnetic resonance imaging; MSRA = methicillin-resistant Staphylococcus aureus; NSAIDS = nonsteroidal anti-inflammatory drugs; PO = by mouth; SSTI = skin and soft-tissue infections; TID = 3 times daily. Adapted from Jenkins TC, Knepper BC, Sabel AL, et al. Decreased antibiotic utilization after implementation of a guideline for inpatient cellulitis and cutaneous abscess. Arch Intern Med. 2011;171(12):1072-9.
-
A male patient with orbital cellulitis with proptosis, ophthalmoplegia, and edema and erythema of the eyelids. The patient also exhibited pain on eye movement, fever, headache, and malaise.
-
A male patient with orbital cellulitis with proptosis, ophthalmoplegia, and edema and erythema of the eyelids. The patient also exhibited chemosis and resistance to retropulsion of the globe.
-
Gross photograph of complicated cellulitis. Instead of the presence of yellow fat, the tissue is hemorrhagic and necrotic.
-
Hematoxylin and eosin (H&E) stain, high power. This image shows deeper subcutaneous tissue involved in a case of cellulitis, with acute inflammatory cells and fat necrosis.
-
Hematoxylin and eosin (H&E) stain, high power. This image shows cellulitis caused by herpes simplex virus, with the multinucleated organism in the center of the picture.
Tables
Location |
Likely Organisms |
Other Organisms |
Complication/ Discussion |
Antibiotic Regimen -- Oral/ Outpatient |
Indication for Hospitalization |
Antibiotic Regimen -- Parenteral/ Hospitalized |
Uncomplicated cellulitis |
Group A streptococci much more likely than Staphylococcus aureus |
|
|
Cephalexin or dicloxacillin or clindamycin |
|
Cefazolin or oxacillin or nafcillin |
Cellulitis, concern for methicillin-resistant S aureus is a concern |
Group A streptococci and S aureus |
|
|
[(Cephalexin or dicloxacillin or clindamycin) plus trimethoprim/ sulfamethoxazole] or Clindamycin |
|
Vancomycin Daptomycin Ceftaroline |
Dog bite |
Pasteurella species (50% of wounds) S aureus Streptococcus pyogenes |
Staphylococci, streptococci Aerobes --Moraxella and Neisseria Anaerobes --Fusobacterium, Bacteroides, Porphyromonas, and Prevotella |
Capnocytophaga canimorsus may cause sepsis in patients with asplenia/hepatic disease. Avoid first-generation cephalosporins/ erythromycin/ dicloxacillin. High likelihood of infection – Prophylactic antibiotics indicated for the following wounds: deep puncture, hands, requiring surgical repair, immunocompromised host, venous or lymphatic compromise, crush injury. Requires close follow-up care within 24-48 h. |
Amoxicillin/ clavulanate Penicillin allergic: Moxifloxacin |
Deep wounds or severe wounds; infections not responding to oral antibiotics |
Third-generation cephalosporin (ceftriaxone [Rocephin]) plus metronidazole or beta-lactam/beta-lactamase inhibitor (eg, ampicillin/sulbactam) or fluoroquinolone plus metronidazole or carbapenem (ertapenem) |
Human bite |
Eikenella corrodens (gram-negative facultative anaerobe, 29% of wounds) Aerobic gram-positive cocci, anaerobes |
|
Clenched fist lacerations over metacarpophalangeal joints should be considered human bites; anesthetize wounds and irrigate; reevaluate within 24-48 h. Intercanine distance >3 cm is likely bite from adult; if wound to child, consider abuse. |
Amoxicillin/ clavulanate Penicillin allergic: Moxifloxacin or (Clindamycin or metronidazole) plus (doxycycline or cefuroxime or trimethoprim/ sulfamethoxazole) |
|
Third-generation cephalosporin (Rocephin) plus metronidazole or beta-lactam/beta-lactamase inhibitor (eg, ampicillin/sulbactam) or fluoroquinolone plus metronidazole or carbapenem (ertapenem) |
Cat bite |
Pasteurella multocida and P septica (75% of wounds) |
Staphylococci, streptococci, Bacteroides, Peptostreptococcus, Actinomyces, Fusobacterium, Porphyromonas, and Veillonella parvula |
Avoid first-generation cephalosporins/ erythromycin/ dicloxacillin High likelihood of infection -- Prophylactic antibiotics indicated for the following wounds: deep puncture, hands, requiring surgical repair, immunocompromised host, venous or lymphatic compromise. Requires close follow-up care within 24-48 h. |
Amoxicillin/ clavulanate Penicillin allergic -- Moxifloxacin or (Clindamycin or metronidazole) plus (doxycycline or cefuroxime or trimethoprim/ sulfamethoxazole) |
Deep wounds or severe wounds; infections not responding to oral antibiotics |
Third-generation cephalosporin (Rocephin) plus metronidazole or beta-lactam/beta-lactamase inhibitor (eg, ampicillin/sulbactam) or fluoroquinolone plus metronidazole or carbapenem (ertapenem) |
Preseptal (periorbital) cellulitis |
Haemophilus influenzae type b, Streptococcus pneumoniae, S aureus, other streptococcal species, and anaerobes |
Nocardia brasiliensis, Bacillus anthracis, Pseudomonas aeruginosa, Neisseria gonorrhoeae, Proteus species, Pasteurella multocida, Mycobacterium tuberculosis |
Largest study indicates that H influenzae type b and S pneumoniae not diminished in facial cellulitis as a result of immunizations [29] |
Amoxicillin-clavulanate, cefpodoxime, cefdinir |
Age < 1 y/ more severe disease require intravenous antibiotic |
Third-generation cephalosporin (Rocephin) |
Lower extremity -- Complicating saphenous venectomy site after coronary bypass grafting |
No pathogen identifiable in most infections, but it is likely to be streptococcal (> staphylococcal) Non-group A beta-hemolytic streptococci most likely organism; S aureus less common |
|
Recurrent episodes common; may be associated with rigors, extreme fatigue, myalgias, and hypotension; some associated with tinea pedis (toe web cultures may be useful in establishing probable pathogen) |
Dicloxacillin or cephalexin. Add trimethoprim/ sulfamethoxazole or tetracycline or clindamycin if concern for methicillin-resistant S aureus |
|
First-generation cephalosporin (cefazolin); clindamycin; vancomycin |
Breast/arm - - (not mastitis) Complicating breast cancer surgery/lymph node dissection |
No pathogen identifiable in most infections Group A or Non-group A beta-hemolytic streptococci most likely organisms |
|
|
Dicloxacillin, cephalexin. Add trimethoprim/ sulfamethoxazole or tetracycline or clindamycin if concern for methicillin-resistant S aureus |
Fever, recent chemotherapy, neutropenia |
Multiple regimens, none clearly superior –Piperacillin/tazobactam or ceftazidime plus aminoglycoside; or ciprofloxacin plus beta-lactam or monotherapy with piperacillin/tazobactam or cefepime |
Aquatic environment -- Fresh water/ salt water/ brackish water/ swimming pools/ aquarium Puncture/ laceration |
Aeromonas hydrophila, Pseudomonas and Plesiomonas species, Vibrio species, Erysipelothrix rhusiopathiae, Mycobacterium marinum, and others |
|
A hydrophila and Vibrio vulnificus may produce rapidly progressive soft tissue infection and sepsis |
Fluoroquinolone (eg, ciprofloxacin or levofloxacin) Note: For M marinum infection, use clarithromycin plus either ethambutol or rifampin |
|
Third- or fourth-generation cephalosporin (eg, ceftazidime or cefepime) or fluoroquinolone (eg, ciprofloxacin or levofloxacin) |
Clenched-fist injury |
E corrodens (gram-negative anaerobe, 29 % of wounds); aerobic gram-positive cocci, anaerobes |
|
Lacerations over metacarpophalangeal joints should be considered human bites; anesthetize wounds and irrigate; reevaluate within 24-48 h Lacerations of extensor tendon |
Amoxicillin/ clavulanate; penicillin allergic: Moxifloxacin or (clindamycin or metronidazole) plus (doxycycline or cefuroxime or trimethoprim/ sulfamethoxazole) |
Failure to respond to oral therapy marked by increasing pain and swelling or purulent drainage |
Beta-lactam/beta-lactamase inhibitor (eg, ampicillin/sulbactam) |
Odontogenic facial cellulitis |
Aerobic and facultative organisms: group A beta-hemolytic streptococci, Neisseria and Eikenella species Anaerobes: Prevotella and Peptostreptococcus species |
|
Require extraction or root canal |
Amoxicillin-clavulanate or clindamycin |
|
Beta-lactam/beta-lactamase inhibitor (eg, ampicillin/sulbactam) or clindamycin |






