Practice Essentials
Meningitis is a clinical syndrome characterized by inflammation of the meninges. The most common cause of meningeal inflammation is bacterial or viral infection. Most cases of bacterial meningitis are localized over the dorsum of the brain; however, under certain conditions, meningitis may be concentrated at the base of the brain, as with fungal diseases and tuberculosis. Bacterial meningitis must be the first and foremost consideration in the differential diagnosis of patients with headache, neck stiffness, fever, and altered mental status. Acute bacterial meningitis is a medical emergency, and delays in instituting effective antimicrobial therapy result in increased morbidity and mortality. The decision to obtain a brain CT scan before LP should not delay the institution of antibiotic therapy; such delay can increase mortality. [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11]
Neuroimaging can identify conditions that may predispose to bacterial meningitis; thus, it is indicated in patients who have evidence of head trauma, sinus or mastoid infection, skull fracture, and congenital anomalies. In addition, neuroimaging studies are typically used to identify and monitor complications of meningitis, such as hydrocephalus, subdural effusion, empyema, and infarction and to exclude parenchymal abscess and ventriculitis. Identifying cerebral complications early is important, as some complications, such as symptomatic hydrocephalus, subdural empyema, and cerebral abscess, require prompt neurosurgical intervention. [12, 1] [3, 4, 6, 11]
(See the images below.)
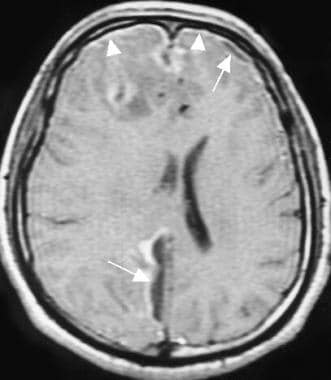 Frontal sinusitis, empyema, and abscess formation in a patient with bacterial meningitis. This contrast-enhanced, axial T1-weighted magnetic resonance image shows a right frontal parenchymal low intensity (edema), leptomeningitis (arrowheads), and a lentiform-shaped subdural empyema (arrows).
Frontal sinusitis, empyema, and abscess formation in a patient with bacterial meningitis. This contrast-enhanced, axial T1-weighted magnetic resonance image shows a right frontal parenchymal low intensity (edema), leptomeningitis (arrowheads), and a lentiform-shaped subdural empyema (arrows).
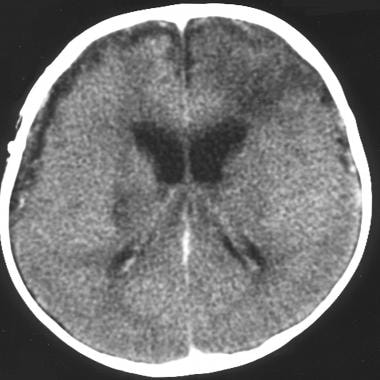 Watershed and lacunar infarcts in a patient with bacterial meningitis. This axial computed tomography scan shows a left frontoparietal watershed infarct, a right basal ganglia lacunar infarct, and a bilateral subdural effusion.
Watershed and lacunar infarcts in a patient with bacterial meningitis. This axial computed tomography scan shows a left frontoparietal watershed infarct, a right basal ganglia lacunar infarct, and a bilateral subdural effusion.
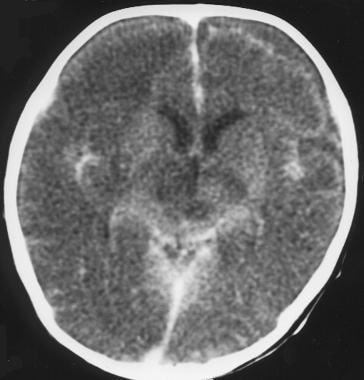
 Ventriculitis in a patient with bacterial meningitis. This contrast-enhanced computed tomography scan shows ependymal enhancement.
Ventriculitis in a patient with bacterial meningitis. This contrast-enhanced computed tomography scan shows ependymal enhancement.
Preferred Radiologic Examination
Computed tomography (CT) scanning is often performed first to exclude contraindications for lumbar puncture. [12, 2] Unfortunately, while increased intracranial pressure is considered a contraindication to lumbar puncture, normal CT scan findings may not be sufficient evidence of normal intracranial pressure in patients with bacterial meningitis. Nonenhanced CT scans and magnetic resonance images (MRIs) of patients with uncomplicated acute bacterial meningitis may be unremarkable. [13, 5, 9, 14, 10]
MRI is the most sensitive imaging modality, because the presence and extent of inflammatory changes in the meninges, as well as complications, can be detected. MRI is superior to CT scanning in the evaluation of patients with suspected meningitis, as well as in demonstrating leptomeningeal enhancement and distention of the subarachnoid space with widening of the interhemispheric fissure, which is reported to be an early finding in severe meningitis. [15, 16, 17, 18] (See the image below.)
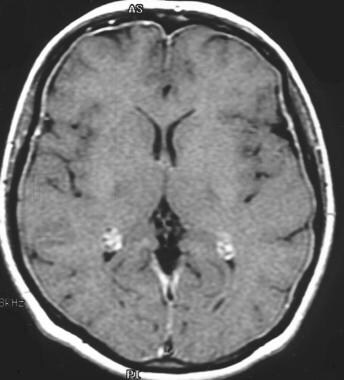
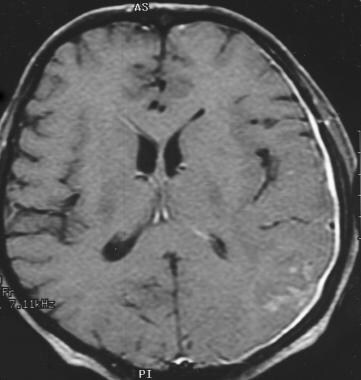
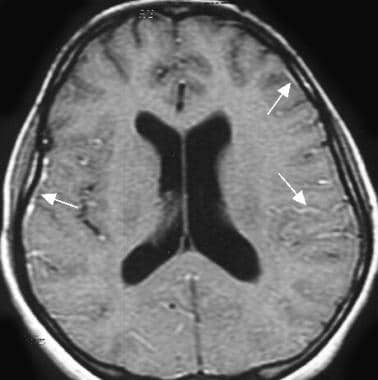 Acute bacterial meningitis. This contrast-enhanced, axial T1-weighted magnetic resonance image shows leptomeningeal enhancement (arrows).
Acute bacterial meningitis. This contrast-enhanced, axial T1-weighted magnetic resonance image shows leptomeningeal enhancement (arrows).
Effusion, hydrocephalus, cerebritis, and abscess can be evaluated well with CT scanning and ultrasonography (US) in infants; however, MRI is the most effective modality for localizing the level of the pathology. Chest radiographs may be obtained to look for signs of pneumonia or fluid in the lungs, especially in children.
In uncomplicated cases of purulent meningitis, early CT scans and MRIs usually demonstrate normal findings or small ventricles and effacement of sulci. The value of CT scanning in the early diagnosis of subdural empyema is limited because of the presence of bone artifact.
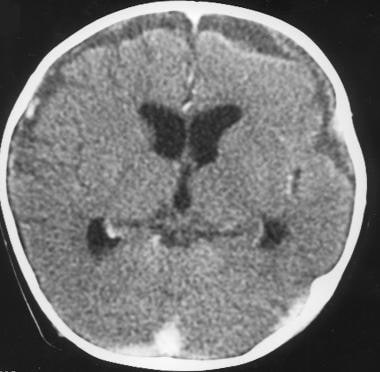
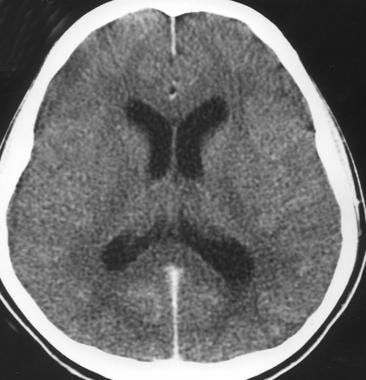 Acute bacterial meningitis. This axial nonenhanced computed tomography scan shows mild ventriculomegaly and sulcal effacement.
Acute bacterial meningitis. This axial nonenhanced computed tomography scan shows mild ventriculomegaly and sulcal effacement.
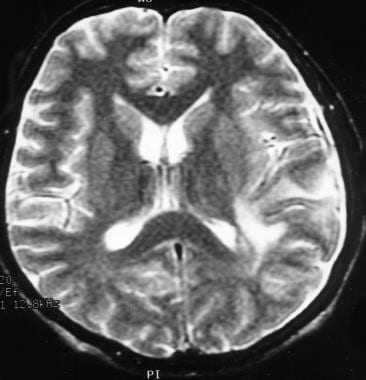
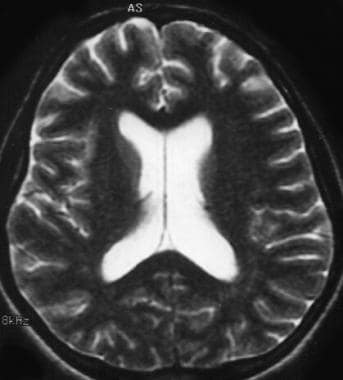 Acute bacterial meningitis. This axial T2-weighted magnetic resonance image shows only mild ventriculomegaly.
Acute bacterial meningitis. This contrast-enhanced, axial T1-weighted magnetic resonance image shows leptomeningeal enhancement (arrows).
Acute bacterial meningitis. This axial T2-weighted magnetic resonance image shows only mild ventriculomegaly.
Acute bacterial meningitis. This contrast-enhanced, axial T1-weighted magnetic resonance image shows leptomeningeal enhancement (arrows).
Enhancement of the meninges is seen on contrast-enhanced CT scans and MRIs in cases of bacterial meningitis. However, meningeal enhancement is nonspecific and may also be caused by the following 5 different etiologic subgroups:
-
Infectious
-
Carcinomatous meningitis
-
Reactive (eg, surgery, shunt, trauma)
-
Chemical (eg, ruptured dermoid and cysticercoid cysts, intrathecal chemotherapy)
-
Inflammatory (eg, sarcoidosis, collagen vascular disease
Arterial angiography may demonstrate arterial spasm or may show focal areas of inflammation that have manifested by hypervascularity. If magnetic resonance venography is not available, a reliable and cost-effective method for detecting venous sinus thrombosis is intravenous digital-subtraction angiography.
Plain radiographs do not have diagnostic importance in bacterial meningitis. Chest radiography may be obtained to look for signs of pneumonia or fluid in the lungs. As many as 50% of patients with pneumococcal meningitis also have evidence of pneumonia on initial chest images.
Guidelines
The European Society for Clinical Microbiology and Infectious Diseases (ESCMID) guidelines for diagnosis and management of acute bacterial meningitis strongly recommended cranial imaging before lumbar puncture in patients with focal neurologic deficits (excluding cranial nerve palsies); new-onset seizures; severely altered mental status (Glasgow Coma Scale score < 10), and severely immunocompromised state. However, cranial imaging before lumbar puncture is not recommended in patients who do not have these characteristics. [3]
The United Kingdom joint specialists societies guidelines on the diagnosis and management of acute meningitis recommend against neuroimaging before lumbar puncture unless one of the following indications of brain shift is present [4] : focal neurologic signs, papilledema, continuous or uncontrolled seizures, or Glasgow Coma Scale score ≤12
The Infectious Diseases Society of America (IDSA) guidelines recommend neuroimaging in patients sith suspected acute bacterial infection with a GCS < 15, arm or leg drift, abnormal ocular motility, visual field defect, dilated pupil, new-onset seizures, immunocompromise, suspected mass lesion, stroke, focal infection, or increased intracranial pressure with papilledema. [5] The IDSA also issued clinical practice guidelines for healthcare-associated ventriculitis and meningitis, including the following [6] :
-
Neuroimaging is recommended in patients with suspected healthcare-associated ventriculitis and meningitis.
-
MRI with gadolinium enhancement and diffusion-weighted imaging is recommended for detecting abnormalities.
-
In patients with infected ventriculoperitoneal shunts and abdominal symptoms (eg, pain or tenderness), an ultrasound or CT of the abdomen should be performed to detect CSF loculations at the shunt terminus.
For excellent patient education resources, visit eMedicineHealth's Brain and Nervous System Center. Also, see eMedicineHealth's patient education articles Meningitis in Adults, Meningitis in Children, and Brain Infection.
Computed Tomography
The most important role of CT scanning in imaging patients with meningitis is to identify contraindications to lumbar puncture and complications that require prompt neurosurgical intervention, such as symptomatic hydrocephalus, subdural empyema, and cerebral abscess. Contrast-enhanced CT scans may also help detect complications such as venous thrombosis, infarction, and ventriculitis. Ventriculitis is a complication of bacterial meningitis that is commonly seen in neonates. Ependymal enhancement can be seen on contrast-enhanced CT scans. [3, 4, 6, 9, 14, 10]
The value of CT scanning in the early diagnosis of subdural empyema and effusion has been controversial, as this modality may not detect meningitis, especially nonenhanced CT scans in the early stage of the disease. Normal results on CT imaging do not exclude the presence of acute meningitis.
CT scans may reveal the cause of meningeal infection. Obstructive hydrocephalus can occur with chronic inflammatory changes in the subarachnoid space or in cases of ventricular obstruction. Otorhinologic structures and congenital and posttraumatic calvarial defects can be evaluated (see the image below).
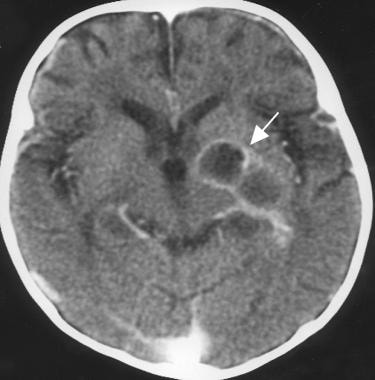
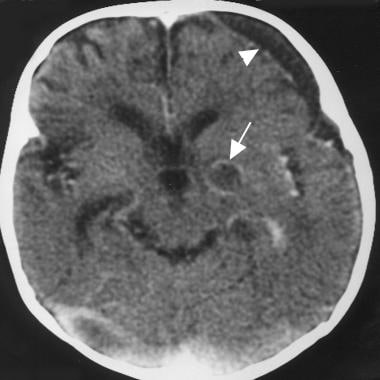 Cerebritis and developing abscess formation in a patient with bacterial meningitis. This contrast-enhanced, axial computed tomography scan was obtained 1 month after surgery and shows a small, ring-enhanced, hypoattenuating mass (recurrence of abscess) in the left basal ganglia and a left lentiform-shaped subdural fluid collection with enhanced meninges (arrowhead).
Cerebritis and developing abscess formation in a patient with bacterial meningitis. This contrast-enhanced, axial computed tomography scan was obtained 1 month after surgery and shows a small, ring-enhanced, hypoattenuating mass (recurrence of abscess) in the left basal ganglia and a left lentiform-shaped subdural fluid collection with enhanced meninges (arrowhead).
Coronal thin-section CT scanning is useful for evaluating patients with recurrent bacterial meningitis; CT cisternography may depict CSF leaks, which may be the source of infection in cases of recurrent meningitis.
Sequelae from meningitis may be depicted on CT scans as periventricular and meningeal calcifications, localized areas of encephalomalacia, porencephaly, and ventricular dilatation secondary to brain atrophy.
Nonenhanced CT scan findings may be normal (>50% of patients), or the studies may demonstrate mildventricular dilatation and effacement of sulci, cerebral edema, and focal low-attenuating lesions. (See the image below.)
Acute bacterial meningitis. This axial nonenhanced computed tomography scan shows mild ventriculomegaly and sulcal effacement.
Obliteration of the basal cisterns may result from increased attenuation, perhaps because of the presence of exudate in the subarachnoid space or leptomeningeal hyperemia. Increased attenuation in the CSF spaces due to meningitis may simulate acute subarachnoid hemorrhage on CT scans.
CT scans for patients with suggested meningitis must be performed with iodinated contrast material. Diffuse enhancement of the subarachnoid space is characteristic. (See the image below.)
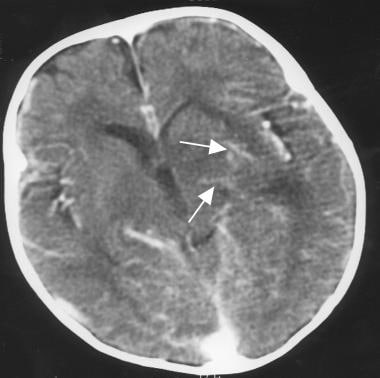 Cerebritis and developing abscess formation in a patient with bacterial meningitis. This contrast-enhanced axial computed tomography scan shows leptomeningitis and parenchymal enhancement (cerebritis) with a low-attenuating area (edema) in the left basal ganglia.
Cerebritis and developing abscess formation in a patient with bacterial meningitis. This contrast-enhanced axial computed tomography scan shows leptomeningitis and parenchymal enhancement (cerebritis) with a low-attenuating area (edema) in the left basal ganglia.
Curvilinear meningeal enhancement over convexities, interhemispheric and sylvian fissures, and obliteration of basal cisterns are usually seen on contrast-enhanced CT scans. Dural enhancement also may occur. However, meningeal enhancement is nonspecific and may be caused not only by bacterial meningitis but also by neoplasm, hemorrhage, sarcoidosis, and other noninfectious inflammatory disorders.
Subdural Effusion
Subdural effusion is a common complication of meningitis, especially in young children. CT scans have shown that as many as 25-40% of children develop this complication during or after treatment for meningitis. Some subdural effusions resolve spontaneously, whereas others may require aspiration or drainage. Important diagnostic features on CT scans are high-attenuating effusions from the CSF and prominent enhancement of the margin of an empyema. The marked degree of enhancement of an empyema that is seen on CT scan rarely occurs in cases of a subdural hematoma, although a thin rim of enhancement is not uncommon in imaging of a chronic subdural hematoma.
(See the images below.)
Cerebritis and developing abscess formation in a patient with bacterial meningitis. This contrast-enhanced, axial computed tomography scan was obtained 1 month after surgery and shows a small, ring-enhanced, hypoattenuating mass (recurrence of abscess) in the left basal ganglia and a left lentiform-shaped subdural fluid collection with enhanced meninges (arrowhead).
 Subdural empyema and arterial infarct in a patient with bacterial meningitis. This contrast-enhanced axial computed tomography scan shows left-sided parenchymal hypoattenuation in the middle cerebral artery territory, with marked herniation and a prominent subdural empyema.
Subdural empyema and arterial infarct in a patient with bacterial meningitis. This contrast-enhanced axial computed tomography scan shows left-sided parenchymal hypoattenuation in the middle cerebral artery territory, with marked herniation and a prominent subdural empyema.
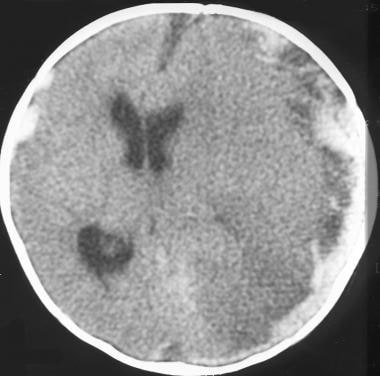
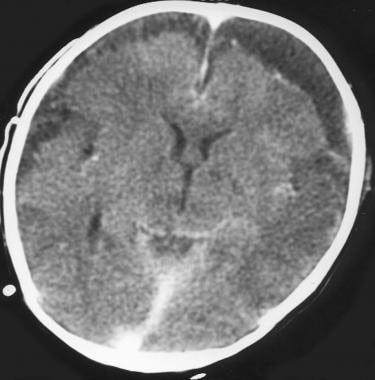 Subdural empyema and diffuse cerebral edema in a patient with bacterial meningitis. This axial computed tomography scan shows bilateral subdural effusion (empyema) and parenchymal low-attenuating areas.
Subdural empyema and diffuse cerebral edema in a patient with bacterial meningitis. This axial computed tomography scan shows bilateral subdural effusion (empyema) and parenchymal low-attenuating areas.
 Subdural empyema with strand in a patient with bacterial meningitis. This contrast-enhanced, axial computed tomography scan shows a bilateral subdural effusion with cortical surface enhancement (empyema). Note that the attenuation of the effusion is higher than that of the cerebrospinal fluid.
Subdural empyema with strand in a patient with bacterial meningitis. This contrast-enhanced, axial computed tomography scan shows a bilateral subdural effusion with cortical surface enhancement (empyema). Note that the attenuation of the effusion is higher than that of the cerebrospinal fluid.
Sinus Thrombosis
Sinus thrombosis can be demonstrated on CT scans. In the acute phase (when the clot is dense), a hyperattenuating thrombus can be seen in the sagittal sinus on a nonenhanced scan. The so-called empty delta sign, which is a triangle of decreased attenuation in the posterior portion of the affected sinus, can be seen on contrast-enhanced CT scans and is visible only after the clot becomes less dense than the contrast-enhanced blood that flows around it.
Infarcts
Infarcts can be reliably diagnosed with CT scanning. Infarcts tend to be sharply marginated and confined to a specific arterial vascular territory. Commonly, multiple lacunar infarcts are seen in the distribution of perforating vessels in the brainstem, basal ganglia, and white matter.
(See the images below.)
Subdural empyema and arterial infarct in a patient with bacterial meningitis. This contrast-enhanced axial computed tomography scan shows left-sided parenchymal hypoattenuation in the middle cerebral artery territory, with marked herniation and a prominent subdural empyema.
Watershed and lacunar infarcts in a patient with bacterial meningitis. This axial computed tomography scan shows a left frontoparietal watershed infarct, a right basal ganglia lacunar infarct, and a bilateral subdural effusion.
 Subdural empyema and diffuse cerebral edema in a patient with bacterial meningitis. This contrast-enhanced computed tomography scan shows diffuse cerebral edema and lacunar infarcts in the thalamus.
Subdural empyema and diffuse cerebral edema in a patient with bacterial meningitis. This contrast-enhanced computed tomography scan shows diffuse cerebral edema and lacunar infarcts in the thalamus.
Cerebritis
In cerebritis, CT scans can show ill-defined areas of low attenuation, which are evidence of edema in the affected brain. On nonenhanced CT scans, abscesses, which are most commonly located near the gray matter–white matter junction, can appear as areas of low attenuation with a thin wall of slightly increased attenuation. After the administration of contrast material, the abscess wall and surrounding inflammatory tissue enhancement are ring shaped.
(See the images below.)
Cerebritis and developing abscess formation in a patient with bacterial meningitis. This contrast-enhanced, axial computed tomography scan was obtained 1 month after surgery and shows a small, ring-enhanced, hypoattenuating mass (recurrence of abscess) in the left basal ganglia and a left lentiform-shaped subdural fluid collection with enhanced meninges (arrowhead).
 Cerebritis and developing abscess formation in a patient with bacterial meningitis. This contrast-enhanced axial computed tomography scan shows a ring-enhancing, lobulated, hypoattenuating mass (abscess) in the left basal ganglia.
Cerebritis and developing abscess formation in a patient with bacterial meningitis. This contrast-enhanced axial computed tomography scan shows a ring-enhancing, lobulated, hypoattenuating mass (abscess) in the left basal ganglia.
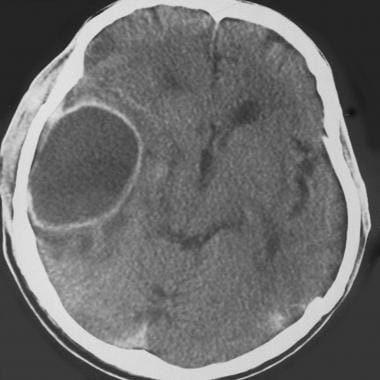 Abscess in a patient with bacterial meningitis. This contrast-enhanced computed tomography scan shows a ring-enhancing, hypoattenuating mass (abscess) with peripheral edema and mass effect.
Abscess in a patient with bacterial meningitis. This contrast-enhanced computed tomography scan shows a ring-enhancing, hypoattenuating mass (abscess) with peripheral edema and mass effect.
Magnetic Resonance Imaging
Routine contrast-enhanced brain MRI is the most sensitive modality for the diagnosis of bacterial meningitis because it helps detect the presence and extent of inflammatory changes in the meninges, as well as complications. The increased sensitivity and specificity of MRI results from direct multiplanar imaging, increased contrast resolution, and the absence of artifact caused by bone. [15, 16, 17, 18]
Nonenhanced MRI studies performed in patients with uncomplicated acute bacterial meningitis may demonstrate unremarkable findings; however, such results do not exclude acute meningitis.
Some authors suggest performing MRI with a high dose of contrast material (0.3 mmol/kg), which is the most important factor. [18] They also recommend imaging immediately after the injection and then performing magnetization transfer imaging, which can help depict abnormal meningeal enhancement and which facilitates the diagnosis of early brain meningitis. Meningeal enhancement is nonspecific, however, and may be caused not only by bacterial meningitis but also by neoplasm, hemorrhage, sarcoidosis, and other noninfectious inflammatory disorders.
Noncontrast MRIs of patients with uncomplicated acute bacterial meningitis may demonstrate obliterated cisterns and the distention of the subarachnoid space with widening of the interhemispheric fissure, which is reported to be an early finding in severe meningitis or may be unremarkable. T2-weighted images are sensitive to abnormal tissue water distribution and, thus, may show cortical hyperintensities that are reversible and believed to represent edema. Diffuse enhancement of the subarachnoid space is characteristic. [15, 16, 17]
(See the images below.)
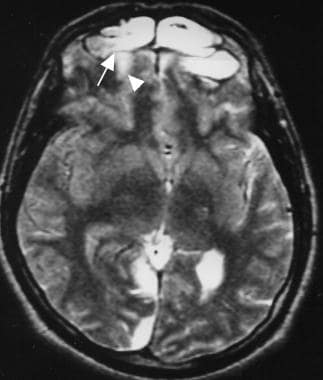 Frontal sinusitis, empyema, and abscess formation in a patient with bacterial meningitis. This T2-weighted axial magnetic resonance image shows frontal sinusitis, a bone defect (arrow) with adjacent cortical edema (arrowhead), and right occipitoparietal subdural fluid collection (empyema).
Acute bacterial meningitis. This axial T2-weighted magnetic resonance image shows only mild ventriculomegaly.
Frontal sinusitis, empyema, and abscess formation in a patient with bacterial meningitis. This T2-weighted axial magnetic resonance image shows frontal sinusitis, a bone defect (arrow) with adjacent cortical edema (arrowhead), and right occipitoparietal subdural fluid collection (empyema).
Acute bacterial meningitis. This axial T2-weighted magnetic resonance image shows only mild ventriculomegaly.
 Pachymeningitis and cerebritis in a patient with bacterial meningitis. This T2-weighted axial magnetic resonance image shows parenchymal focal edema (cerebritis).
Pachymeningitis and cerebritis in a patient with bacterial meningitis. This T2-weighted axial magnetic resonance image shows parenchymal focal edema (cerebritis).
Contrast-enhanced MRI has been shown to be more sensitive than CT scanning in the detection of meningeal inflammation. Gadolinium-enhanced MRI studies can demonstrate abnormal leptomeningeal enhancement that more closely approximates the extent of inflammatory cell infiltration.
(See the images below.)
Frontal sinusitis, empyema, and abscess formation in a patient with bacterial meningitis. This contrast-enhanced, axial T1-weighted magnetic resonance image shows a right frontal parenchymal low intensity (edema), leptomeningitis (arrowheads), and a lentiform-shaped subdural empyema (arrows).
Acute bacterial meningitis. This contrast-enhanced, axial T1-weighted magnetic resonance image shows leptomeningeal enhancement (arrows).
Dural enhancement may occur, and extension of enhancing subarachnoid exudate deep into the sulci can be seen in severe cases.
(See the images below.)
 Pachymeningitis in a patient with bacterial meningitis. This contrast-enhanced, axial T1-weighted magnetic resonance image shows diffuse dural enhancement.
Pachymeningitis in a patient with bacterial meningitis. This contrast-enhanced, axial T1-weighted magnetic resonance image shows diffuse dural enhancement.
 Pachymeningitis and cerebritis in a patient with bacterial meningitis. This contrast-enhanced, T1-weighted axial magnetic resonance image shows left-sided dural enhancement (pachymeningitis) and focal pial enhancement.
Pachymeningitis and cerebritis in a patient with bacterial meningitis. This contrast-enhanced, T1-weighted axial magnetic resonance image shows left-sided dural enhancement (pachymeningitis) and focal pial enhancement.
Revealing the cause of meningeal infection is best accomplished with MRI. MRI can help detect inflammatory changes in the paranasal sinuses and mastoid air cells, which are usually depicted as areas of increased signal intensity on T2-weighted images.
(See the images below.)
Frontal sinusitis, empyema, and abscess formation in a patient with bacterial meningitis. This T2-weighted axial magnetic resonance image shows frontal sinusitis, a bone defect (arrow) with adjacent cortical edema (arrowhead), and right occipitoparietal subdural fluid collection (empyema).
 Frontal sinusitis, empyema, and abscess formation in a patient with bacterial meningitis. This T2-weighted axial magnetic resonance image shows a developing abscess formation with mass effect and bilateral subdural fluid collections (empyema).
Frontal sinusitis, empyema, and abscess formation in a patient with bacterial meningitis. This T2-weighted axial magnetic resonance image shows a developing abscess formation with mass effect and bilateral subdural fluid collections (empyema).
Enhancement may be prominent. (See the image below.)
Frontal sinusitis, empyema, and abscess formation in a patient with bacterial meningitis. This contrast-enhanced, axial T1-weighted magnetic resonance image shows a right frontal parenchymal low intensity (edema), leptomeningitis (arrowheads), and a lentiform-shaped subdural empyema (arrows).
MRI also can help exclude congenital and posttraumatic calvarial defects.
Coronal and sagittal thin-section, heavily T2-weighted MRIs may show CSF leaks, which may be the source of infection in cases of recurrent meningitis.
Plain and contrast-enhanced MRIs help depict the complications of meningitis better than other images. Such complications include empyema/effusion, cerebritis/abscess, venous thrombosis, venous and arterial infarcts, ventriculitis, hydrocephalus, and edema (with or without cerebral herniation).
(See the images below.)
Frontal sinusitis, empyema, and abscess formation in a patient with bacterial meningitis. This T2-weighted axial magnetic resonance image shows a developing abscess formation with mass effect and bilateral subdural fluid collections (empyema).
Pachymeningitis and cerebritis in a patient with bacterial meningitis. This contrast-enhanced, T1-weighted axial magnetic resonance image shows left-sided dural enhancement (pachymeningitis) and focal pial enhancement.
Pachymeningitis and cerebritis in a patient with bacterial meningitis. This T2-weighted axial magnetic resonance image shows parenchymal focal edema (cerebritis).
Subdural Empyema/Effusion
Sterile fluid collections may develop within the subdural space in patients with meningitis. Effusions may be slightly hyperintense relative to CSF on MRIs and are most commonly located in cerebral convexities and interhemispheric fissures.
(See the images below.)
Frontal sinusitis, empyema, and abscess formation in a patient with bacterial meningitis. This contrast-enhanced, axial T1-weighted magnetic resonance image shows a right frontal parenchymal low intensity (edema), leptomeningitis (arrowheads), and a lentiform-shaped subdural empyema (arrows).
Frontal sinusitis, empyema, and abscess formation in a patient with bacterial meningitis. This T2-weighted axial magnetic resonance image shows frontal sinusitis, a bone defect (arrow) with adjacent cortical edema (arrowhead), and right occipitoparietal subdural fluid collection (empyema).
Frontal sinusitis, empyema, and abscess formation in a patient with bacterial meningitis. This T2-weighted axial magnetic resonance image shows a developing abscess formation with mass effect and bilateral subdural fluid collections (empyema).
Occasionally, a portion of the medial subjacent cerebral surface of an effusion demonstrates mild enhancement, presumably from an inflammatory surrounding membrane. These effusions are not empyemas and typically resolve spontaneously.
In the early stages of subdural empyema, T2-weighted images can demonstrate a thin hyperintense convexity and interhemispheric collection usually not visible on CT scans.
Paratentorial and subtemporal extension is well demonstrated on coronal MRIs.
Prominent enhancement of the margin of an empyema is an important diagnostic feature on MRI and results from the formation of a membrane of granulomatous tissue on the leptomeninges and from inflammation in the subjacent cerebral cortex.
Subdural empyema may be differentiated from subacute/chronic subdural hematoma. On MRI, even a noninfected subdural hematoma enhances markedly on gadolinium-enhanced T1- and T2-weighted images because of the presence of extracellular methemoglobin and other forms of iron.
Cerebritis/Abscesses
Cerebritis is the earliest stage of a purulent brain infection. If bacterial cerebritis is not successfully treated medically, the affected portion of the brain liquefies and a surrounding capsule of granulation tissue and collagen forms, resulting in abscess formation. The corticomedullary (gray matter–white matter) junction is the most commonly affected location, and the frontal and parietal lobes are the most frequent sites. Less than 15% of intracranial abscesses occur in the posterior fossa. Multiple abscesses are uncommon except in patients who are immunocompromised. MRI findings of pyogenic brain abscesses are characteristic.
On MRIs, stage I cerebritis appears as an ill-defined edematous area on both T1- and T2-weighted images.
(See the images below.)
Pachymeningitis and cerebritis in a patient with bacterial meningitis. This contrast-enhanced, T1-weighted axial magnetic resonance image shows left-sided dural enhancement (pachymeningitis) and focal pial enhancement.
Pachymeningitis and cerebritis in a patient with bacterial meningitis. This T2-weighted axial magnetic resonance image shows parenchymal focal edema (cerebritis).
In late stage II cerebritis/early abscess, the abscess wall is hyperintense on T1-weighted images and slightly hypointense on T2-weighted images. In stage III (subacute abscess), the abscess wall is hyperintense on both T1- and T2-weighted images. In stage IV (chronic phase), the abscess wall is isointense on T1-weighted MRIs and markedly hypointense on T2-weighted MRIs. Although abscesses in stages II-IV all exhibit ring-type enhancement after the infusion of a paramagnetic contrast agent, better edge definition is seen in the enhancing wall of stage II lesions than in stages III and IV.
Abscesses may imitate brain tumors and can be differentiated with use of proton magnetic resonance spectroscopy. Brain tumors usually demonstrate elevated choline and possibly decreased creatine peaks, as well as N -acetyl-aspartate peaks. Abscesses do not demonstrate these abnormal peaks; instead, they have lactate peaks and the lipid peaks of amino acids.
Venous Thrombosis
Thrombosis of the deep veins, cortical veins, and venous sinuses is an uncommon complication of meningitis; however, thrombosis more often develops in the presence of superimposed dehydration.
Gradient-echo and spin-echo MRIs can demonstrate cortical vein and/or dural sinus thrombosis, as well as the characteristic signal-intensity properties of acute and subacute hemorrhagic infarctions.
MRI-aided diagnosis for acute and chronic sinus thrombosis may be complex; however, sinus thrombosis is readily diagnosed when the thrombus is subacute because they are hyperintense on T1-weighted images.
Magnetic resonance venography (2-dimensional time-of-flight or phase-contrast) can aid the diagnosis of venous sinus thrombosis.
Cavernous sinus thrombosis is an uncommon sequela of meningitis. The signal intensity of this condition varies depending on the state of infection, inflammation, and clot evolution. The sinus may be enlarged with a narrowed or occluded cavernous carotid artery. T2-signal prolongation may occur in the adjacent clivus or petrous apex.
Venous and Arterial Infarcts
Venous infarcts are diagnosed on the basis of their characteristic location and appearance. Typically, infarcts from a sagittal sinus thrombosis involve the parietal lobes; those from the straight sinus/vein of Galen thrombosis involve the thalami; and infarcts from the transverse sinus or sigmoid sinus thrombosis involve the temporal lobe.
Arterial infarctions in bacterial meningitis are usually the result of arteritis caused by involvement of the vascular spaces and the arterial walls. When major cerebral arteries are involved, large cortical infarctions result. Frequently, multiple lacunar infarcts are seen in the distribution of the perforating vessels in the brainstem, basal ganglia, and white matter.
Ventriculitis
In ventriculitis associated with meningitis, the infecting organisms enter the ventricles via the choroid plexuses. On MRIs, as on CT scans, proteinaceous debris in the trigone or occipital horn of the lateral ventricle and intense enhancement of the ependyma are seen.
Hydrocephalus
Ventriculomegaly can occur in the course of meningitis and is usually mild to moderate in severity. (See the image below.)
Acute bacterial meningitis. This axial T2-weighted magnetic resonance image shows only mild ventriculomegaly.
Obstructive hydrocephalus can occur with chronic inflammatory changes in the subarachnoid space or ventricular obstruction.
Gadolinium
Gadolinium-based contrast agents have been linked to the development of nephrogenic systemic fibrosis (NSF) or nephrogenic fibrosing dermopathy (NFD). The disease has occurred in patients with moderate to end-stage renal disease after being given a gadolinium-based contrast agent to enhance MRI or MRA scans. NSF/NFD is a debilitating and sometimes fatal disease. Characteristics include red or dark patches on the skin; burning, itching, swelling, hardening, and tightening of the skin; yellow spots on the whites of the eyes; joint stiffness with trouble moving or straightening the arms, hands, legs, or feet; pain deep in the hip bones or ribs; and muscle weakness.
Ultrasonography
The role of ultrasonography in patients with bacterial meningitis is limited to the evaluation of complications or deterioration in the patient's clinical situation. Commercially available equipment is used with a 3- to 7.5-MHz transducer, depending on the size of the patient's head. Transducers of 5-7.5 MHz are used for newborns, whereas transducers of 3-5 MHz are used for older infants. US is a heavily operator-dependent technique. Experience is needed to demonstrate the meningeal and parenchymal findings of bacterial meningitis. [19, 11]
In newborns and older infants, complications of meningitis that are depicted on cranial CT scans and MRIs can also be demonstrated on cranial sonograms obtained with a transfontanel approach.
Important US findings in infants with bacterial meningitis have been described. These findings include echogenic sulci, ventriculomegaly and obstructive hydrocephalus, ventriculitis, prominent leptomeninges, subdural effusions, empyema, parenchymal echogenicity, and abscess formation. US can help dentify these complications, but the findings are usually not specific.
Echogenic sulci that appear as a result of the accumulation of inflammatory debris are the most common and transient US finding in meningitis; these resolve gradually as the exudate is cleared.
On US, inflammatory debris in the CSF creates low-level intraventricular echoes in acute ventriculitis. This appearance may imitate that which is seen in the breakdown of intraventricular hematomas; however, these 2 clinical settings can usually be distinguished because ventriculitis produces other signs of inflammation.
Ventriculomegaly
Mild to moderate ventriculomegaly, which is usually reversible, can occur in the course of meningitis. Exudates may produce CSF loculations and pathway obstruction, resulting in a communicating hydrocephalus, whereas obstructive hydrocephalus may occur with ventricular obstruction or chronic inflammatory changes in the subarachnoid space. Intraventricular septa formation may result in ventricular compartmentalization. Progressive ventriculomegaly can be excluded with the use of serial sonograms.
Ventriculitis
Ventriculitis, which is seen in 65-90% of patients, is suggested by the US findings of hydrocephalus, which include a thickened, hyperechoic, irregular ependymal surface and echogenic debris and fibrous septa formation within the enlarged ventricles. The septa occur over the 2 weeks following bacterial meningitis; US is best for identifying septa, compared with CT scanning or MRI.
Subdural Effusion
Subdural effusion is a common US finding in infants with Haemophilus influenzae meningitis. Subdural empyemas are uncommon findings and result when the effusions become infected; US features may help differentiate effusions from empyemas. [19]
Abnormal Parenchymal Echogenicity
Areas of abnormal parenchymal echogenicity are a significant finding. The lesions represent cerebritis, infarction, encephalomalacia, or, rarely, abscess formation. Abscesses appear as homogeneous echogenic masses with a hypoechoic center that is surrounded by a thin hyperechoic rim.
Doppler Ultrasonography
Doppler US can easily demonstrate the major intracranial vessels via the anterior transfontanel approach; in older children, these vessels can be demonstrated via the transtemporal approach. The cerebral blood flow can be evaluated qualitatively. Serial transcranial Doppler examinations performed to assess for disease-related arterial narrowing have been described. An association between an unfavorable course of the disease and increased cerebral blood flow velocity in intracranial arteries has been suggested; this probably indicates vasospasm. [20] Transcranial Doppler US can potentially be used to identify high-risk patients who may benefit from adjuvant therapeutic interventions.
Nuclear Imaging
Although CT scanning and MRI are the most common imaging modalities used to evaluate patients with a possible abscess, distinguishing brain abscesses with these 2 modalities is occasionally difficult. Technetium-99 (99mTc) hexamethylpropyleneamine oxime, which is a radionuclide imaging label for leukocytes, and radiolabeled polyclonal immunoglobulin antibodies may be helpful in select patients. Tc-99m hexamethylpropyleneamine oxime may also be used in the evaluation of the cerebral blood flow velocity and perfusion in bacterial meningitis. In addition, radionuclide cisternography may depict CSF leaks, which may be the source in cases of recurrent meningitis. [21]
-
Chronic mastoiditis and epidural empyema in a patient with bacterial meningitis. This axial computed tomography scan shows sclerosis of the temporal bone (chronic mastoiditis), an adjacent epidural empyema with marked dural enhancement (arrow), and the absence of left mastoid air.
-
Frontal sinusitis, empyema, and abscess formation in a patient with bacterial meningitis. This contrast-enhanced, axial T1-weighted magnetic resonance image shows a right frontal parenchymal low intensity (edema), leptomeningitis (arrowheads), and a lentiform-shaped subdural empyema (arrows).
-
Frontal sinusitis, empyema, and abscess formation in a patient with bacterial meningitis. This T2-weighted axial magnetic resonance image shows frontal sinusitis, a bone defect (arrow) with adjacent cortical edema (arrowhead), and right occipitoparietal subdural fluid collection (empyema).
-
Frontal sinusitis, empyema, and abscess formation in a patient with bacterial meningitis. This T2-weighted axial magnetic resonance image shows a developing abscess formation with mass effect and bilateral subdural fluid collections (empyema).
-
Cerebritis and developing abscess formation in a patient with bacterial meningitis. This contrast-enhanced, axial computed tomography scan was obtained 1 month after surgery and shows a small, ring-enhanced, hypoattenuating mass (recurrence of abscess) in the left basal ganglia and a left lentiform-shaped subdural fluid collection with enhanced meninges (arrowhead).
-
Cerebritis and developing abscess formation in a patient with bacterial meningitis. This contrast-enhanced axial computed tomography scan shows leptomeningitis and parenchymal enhancement (cerebritis) with a low-attenuating area (edema) in the left basal ganglia.
-
Cerebritis and developing abscess formation in a patient with bacterial meningitis. This contrast-enhanced axial computed tomography scan shows a ring-enhancing, lobulated, hypoattenuating mass (abscess) in the left basal ganglia.
-
Subdural empyema and arterial infarct in a patient with bacterial meningitis. This contrast-enhanced axial computed tomography scan shows left-sided parenchymal hypoattenuation in the middle cerebral artery territory, with marked herniation and a prominent subdural empyema.
-
Watershed and lacunar infarcts in a patient with bacterial meningitis. This axial computed tomography scan shows a left frontoparietal watershed infarct, a right basal ganglia lacunar infarct, and a bilateral subdural effusion.
-
Subdural empyema and diffuse cerebral edema in a patient with bacterial meningitis. This axial computed tomography scan shows bilateral subdural effusion (empyema) and parenchymal low-attenuating areas.
-
Subdural empyema and diffuse cerebral edema in a patient with bacterial meningitis. This contrast-enhanced computed tomography scan shows diffuse cerebral edema and lacunar infarcts in the thalamus.
-
Abscess in a patient with bacterial meningitis. This contrast-enhanced computed tomography scan shows a ring-enhancing, hypoattenuating mass (abscess) with peripheral edema and mass effect.
-
Acute bacterial meningitis. This axial nonenhanced computed tomography scan shows mild ventriculomegaly and sulcal effacement.
-
Acute bacterial meningitis. This axial T2-weighted magnetic resonance image shows only mild ventriculomegaly.
-
Acute bacterial meningitis. This contrast-enhanced, axial T1-weighted magnetic resonance image shows leptomeningeal enhancement (arrows).
-
Pachymeningitis in a patient with bacterial meningitis. This contrast-enhanced, axial T1-weighted magnetic resonance image shows diffuse dural enhancement.
-
Pachymeningitis and cerebritis in a patient with bacterial meningitis. This contrast-enhanced, T1-weighted axial magnetic resonance image shows left-sided dural enhancement (pachymeningitis) and focal pial enhancement.
-
Pachymeningitis and cerebritis in a patient with bacterial meningitis. This T2-weighted axial magnetic resonance image shows parenchymal focal edema (cerebritis).
-
Subdural empyema with strand in a patient with bacterial meningitis. This contrast-enhanced, axial computed tomography scan shows a bilateral subdural effusion with cortical surface enhancement (empyema). Note that the attenuation of the effusion is higher than that of the cerebrospinal fluid.
-
Ventriculitis in a patient with bacterial meningitis. This contrast-enhanced computed tomography scan shows ependymal enhancement.
-
Lacunar infarct in a patient with bacterial meningitis. This axial computed tomography scan shows the distribution of the perforating vessels in the brainstem, basal ganglia, and white matter.
-
Bilateral subdural empyema in a patient with bacterial meningitis. This computed tomography scan demonstrates the important diagnostic features of meningitis: prominent enhancement of the margin and increased attenuation of the empyema.
-
Abscess formation in a patient with bacterial meningitis. This contrast-enhanced, T1-weighted, axial magnetic resonance image shows an abscess formation in the right frontal lobe (arrows) and a right parasagittal subdural empyema (arrowhead).
-
Pachymeningitis in a patient with bacterial meningitis. This contrast-enhanced, T1-weighted, coronal magnetic resonance image also shows subdural empyemas on the left side.






