History
Diagnosis of 5-alpha-reductase type 2 deficiency (5-ARD) is usually made in the newborn period when the infant presents with ambiguous genitalia. [15] No risk factors or clinical markers in pregnancy are known. Genital ambiguity is occasionally diagnosed prenatally when an infant who is demonstrated by amniocentesis or chorionic villus sampling to have XY karyotype fails to have a demonstrable penis on ultrasonography.
If 5-alpha-reductase deficiency is considered in a newborn, a broad approach to ambiguous genitalia should be taken. [1, 14] The utmost care should be taken not to assign a gender to the child before evaluation and consultation with an experienced, multidisciplinary team. The first words spoken to the parents are likely to be remembered and should focus on the overall health of the infant. A sensitive discussion about the uncertainty of the child's gender and explanation of the child's genital anatomy can be aided by online developmental Web sites, such as the ones available on the Sick Kids and DSD Guidelines sites. See Ambiguous Genitalia and Intersexuality for more in depth discussion
Initial evaluation should begin with a careful history. [1] Assess prenatal and maternal past medical and family history. Specific questions should be asked regarding relatives with disorders of sexual development (DSDs), neonatal deaths, amenorrhea, or infertility and consanguinity. Parental consanguinity increases the child's risk for autosomal recessive disorders including 5-alpha reductase type 2 deficiency.
Physical Examination
Workup of ambiguous genitalia must include careful physical examination to characterize the degree of virilization on the Prader scale (see the image below), presence of palpable gonadal tissue, and overall health of the child. [14]
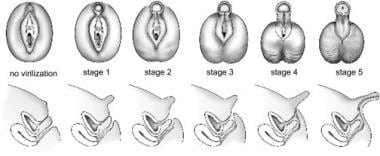 Prader scale reflecting the degree of virilization of the external genitalia. The internal genitalia reflect the changes in the urogenital sinus in response to the presence or absence of mullerian inhibiting hormone (MIH)
Prader scale reflecting the degree of virilization of the external genitalia. The internal genitalia reflect the changes in the urogenital sinus in response to the presence or absence of mullerian inhibiting hormone (MIH)
Neonatal presentation
Phenotypic findings in a newborn are limited to the genitalia. [15, 21] The spectrum of findings ranges from minimal undervirilization presenting with normal male anatomy, except for isolated micropenis or hypospadias, to severe undervirilization presenting as normal female external genitalia with mild clitoral enlargement as the only physical finding. In a study published in 2011, a cohort of 55 patients with 5-alpha-reductase type 2 deficiency displayed widely varied phenotypes in the neonatal period. In this cohort, clitoromegaly was the most common phenotype in 49% of patients, followed by microphallus with varying degrees of hypospadias in 33% of patients. [22]
Most commonly, the external genitalia exhibit labial appearance to the labioscrotal folds with some mild rugation or pigmentation present in some patients.
The phallus is often indeterminate in size and morphology. Its length falls between 1 cm (ie. usual maximum for a clitoris) and 2 cm (ie. lower limit of normal for a penis).
The urethra may empty anywhere from the tip of the phallus to the perineum, with the latter observed more frequently.
The testes are usually in the inguinal canals bilaterally; however, in some individuals with 5-alpha-reductase type 2 deficiency, the testes can be found in the labioscrotal folds or retained in the abdomen.
A pseudovaginal blind-ending introitus may be present with a normal hymen.
The uterus and cervix are absent on imaging and by examination.
The rest of the examination findings are within normal limits.
Presentation of 46XY males at puberty
Clear signs of virilization predominate at puberty. The escutcheon is male in distribution. The phallus exhibits definite enlargement. The shoulders are relatively broad and the hips are narrow.
Muscularity and body hair may increase. Generally, no breast development is present. A prominentia laryngea (Adam's apple) may start to develop. In addition, facial hair develops and the child's voice may begin to deepen.
The mucosa of the vaginal introitus remains atrophic in appearance (remaining red) rather than the thickened pink of estrogen-stimulated mucosa.
Presentation of 46XX females
Females homozygous for 5-alpha-reductase type 2 deficiency have very subtle manifestations, such as delayed menarche, minimal acne, and minimal body hair. [23] Fertility is normal in females.
-
Biochemical effects of 5-alpha-reductase type 2 deficiency in testosterone biosynthesis. Typically levels of testosterone are elevated, whereas levels of dihydrotestosterone (DHT) are significantly decreased, leading to male undervirilization.
-
Prader scale reflecting the degree of virilization of the external genitalia. The internal genitalia reflect the changes in the urogenital sinus in response to the presence or absence of mullerian inhibiting hormone (MIH)









