Multimodality Imaging:
ABDOMINAL RADIOGRAPHS
- majority of urinary tract calculi are calcium-containing and should therefore be visible on plain radiographs

Fig.: Figure 10: Pre PNL radiograph demonstrates bilateral internal ureteral stents. The proximal left ureter contains an ovoid 2.6 X 0.9cm stone at the UPJ, with three additional smaller calculi in the lower pole measuring up to 5mm. On the right, there is a 2.1 X 1.5cm stone in the renal pelvis as well as multiple additional smaller stones measuring up to 9mm in the lower pole. The patient subsequently underwent bilateral PNL.
- bowel gas,
faecal material in overlying colon,
patient obesity and extra-renal calcifications limit detection
- overall low sensitivity in recent studies for detection of calculi,
ranging from 45-58% [15]
- Nonetheless,
plain radiographs retain a central role in monitoring known radiopaque calculi and in planning fluoroscopically-guided therapeutic procedures such as PNL and ESWL
ABDOMINAL CT
- Over 99% of stones will be visualized on non-contrast stone protocol CT (CT KUB) [16]
- Unrivalled diagnostic accuracy,
visualizing the site and allowing accurate measurement of size of the calculus,
however cranio-caudal size may be overestimated by spiral CT
- Visualizes calculi that are radiolucent on plain radiographs with the exception of indinavir and pure matrix stones

Fig.: Figure 11: Plain abdominal radiograph demonstrates right double J ureteral stent. No radiopaque urinary tract calculus is visualized.

Fig.: Figure 12: CT KUB image in the same patient demonstrating 1cm ovoid calculus in the right renal pelvis (arrow) which was radiolucent on the preceeding plain radiograph
- Assesses for the presence and severity of obstruction
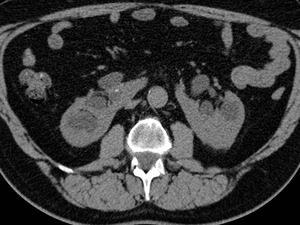
Fig.: Figure 13: CT KUB demonstrates bilateral hydronephrosis in a horseshoe kidney secondary to obstructing calculi in both lower poles
- Allows measurements of “stone density”,
which has been used as a predictor of stone response to ESWL [17]
- Multiplanar reformations (MPR) and volumetric 3D reconstructed images provide additional anatomical information to assist in planning the optimal percutaneous approach
CT ANGIOGRAPHY
- May be necessary in certain situations when PNL is being planned for patients with congenital anomalies such as horseshoe,
ectopic,
crossed fused ectopia and PUJ obstruction to evaluate for the presence of aberrant arterial supply and in the case of PUJ obstruction,
to exclude the presence of a crossing vessel

Fig.: Figure 14: Coronal reformatted image from a CT renal angiogram in a patient with congenital PUJ obstruction being evaluated for PNL. This demonstrates the proximal end of an internal ureteral stent beyond the UPJ stricture in the grossly dilated renal pelvis. Two stones are identified, one in an upper pole calyx and the larger stone in the renal pelvis measuring 2cm in diameter.

Fig.: Figure 15: Reformatted image from a CT renal angiogram in the same patient shows that no crossing vessel is present in this case.

Fig.: Figure 16: Reformatted image from CT renal angiogram in a patient with PUJ obstruction illustrating the presence of anterior impingement caused by an accessory renal artery.
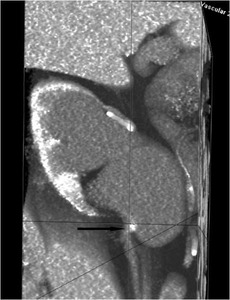
Fig.: Figure 17: Reformatted image from a CT renal angiogram in the same patient demonstrates the presence of an accessory renal artery (arrow) causing anterior impingement at the PUJ. It is crucial that the presence of a crossing vessel (even though uncommon) is appreciated prior to tract planning in cases of PUJ obstruction and a CT renal angiogram should be considered mandatory in patients with PUJ obstruction who are being evaluated for possible PNL.
CT UROGRAPHY

Fig.: Figure 18: Axial image from the delayed phase of a CT Urography study demonstrates multiple filling defects within the dilated collecting system of a horseshoe kidney (arrows).
- Reconstructed images from the delayed phase of a multislice CT urographic study elegantly depict the collecting system anatomy [18]
- May prove invaluable in pre-treatment planning of a number of complex anatomical variants e.g.
calyceal diverticula,
horseshoe kidneys

Fig.: Figure 19: 3D reformatted image from a 5 minute delayed phase of a CT urography study in a patient with a horsehoe kidney (same patient as above axial CT image). This elegantly depicts the stone distribution and calyceal anatomy and aids in planning percutaneous access.
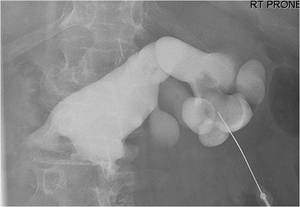
Fig.: Figure 20: Tract planning and ultimately, complete stone clearance in this patient with complex bilateral stone burden in a horsehoe kidney was facilitated by pre-operative CT urography with 3D reformatted images.
ULTRASOUND
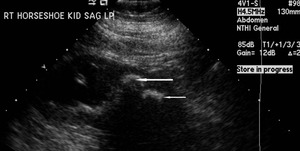
Fig.: Figure 21: Sagittal ultrasound image of the right moiety of a horseshoe kidney demonstrates large calculi (arrows) at the lower pole causing upper pole hydronephrosis.
- Ultrasound is widely used by the interventional radiologist both prior to and during percutaneous tract access
- Its value lies in its ability to provide real-time information regarding position of liver,
spleen and colon and in its utility in assessing the lowermost extent of the aerated lung when planning upper tract punctures
- Can be utilized in conjunction with fluoroscopy to establish access into the desired calyx
Procedure Details:
Preview of PNL imaging
- Assess the adequacy of current imaging i.e.
is it really a stone?

Fig.: Figure 22: Plain abdominal radiograph in a patient referred for PNL due to a presumed right renal calculus which was resistant to ESWL.

Fig.: Figure 23: CT KUB in the above patient demonstrating that the presumed right renal calculus actually represents a calcified gallstone within the gallbladder lumen.

Fig.: Figure 24: Axial CT image from a stone protocol CT demonstrates the left collecting system has been entirely replaced by high attenuation material, thought originally to have represented a large staghorn calculus. The patient was referred to our institution for PNL.
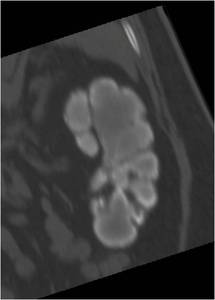
Fig.: Figure 25: Coronal reformatted image demonstrating lower attenuation material centrally within the collecting system without any residual demonstrable renal cortex. The features are suggestive of end-stage TB kidney or "putty kidney". The patient instead underwent a left nephrectomy. The operative specimen is shown below.
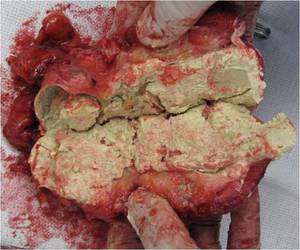
Fig.: Figure 26: Operative nephrectomy specimen bivalved to demonstrate the entire collecting system replaced by soft, putty like material producing the so-called "TB autonephrectomy".

Fig.: Figure 27: Plain abdominal radiograph demonstrates a large calculus in the left renal pelvis. Significant bowel gas overlies both flanks.

Fig.: Figure 28: CT confirms significant colonic interposition. No safe access was available and PNL of the large calculus in the left renal pelvis was not technically feasible.
- Obtain additional imaging as required e.g.
CT urography desirable in ectopic and horseshoe kidneys
- Review renal anatomy and stone distribution

Fig.: Figure 29: Ampullary type system containing large stone burden. The fornices and infundibula are large, making these systems more amenable to PNL.

Fig.: Figure 30: Dendritic system with an associated lower pole calyceal diverticulum. These systems are technically difficult for PNL as their fornices are narrow with long and slender infundibula.

Fig.: Figure 31: Transitional system has features of both the ampullary and dendritic systems as seen above.
- Plan access i.e.
single or multiple,
upper,
lower or interpolar

Fig.: Figure 32: Multiple bilateral calculi in a patient with medullary nephrocalcinosis referred for PNL.
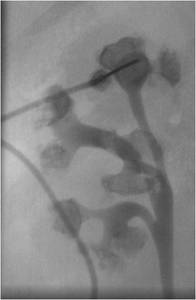
Fig.: Figure 33: Right retrograde pyelogram in the above patient demonstrates multiple calculi in a bifid dendritic system. An upper pole access had initially been planned however multiple tracts were ultimately required intraoperatively in order to achieve maximum stone clearance (see below).

Fig.: Figure 34: Spot fluoroscopic image in the above patient demonstrating three PNL tracts in each kidney.
- Assess whether anatomic modifiers make placement of a retrograde catheter necessary e.g.
lucent stone,
obese patient,
calyceal diverticulum or PUJ obstruction
- Ideally,
the approach should be discussed with the Urologist prior to commencing tract access to maximise stone clearance rates
Patient preparation & positioning
- Anticoagulation status is reviewed

Fig.: Figure 35: Guidelines for stopping anticoagulation medications in patients undergoing PNL.
References: SIR JVIR 2009; 20:S240-S249
- Procedure performed under general anaesthetic
- Reviewed by anaesthetist prior to procedure
- Routine haematological and coagulation parameters including full blood count and coagulation parameters including INR
- Patient intubated and turned prone
- Perioperative antibiotic prophylaxis is administered
Access site planning
Localizing ultrasound performed to identify:
- lung in cases of upper pole puncture
- colon
- liver/spleen
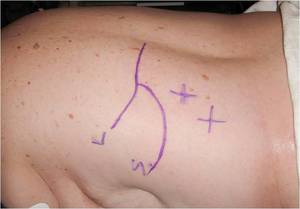
Fig.: Figure 36: The liver, spleen and pleura are marked pre-operatively.
Standard tract access
- With the patient prone on the C-arm fluoroscopy table,
fluoroscopic triangulation technique is employed to access the desired calyx
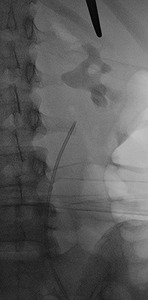
Fig.: Figure 37: Fluoroscopic image demonstrating large staghorn calculus with retrograde ureteral catheter in situ and planned upper pole calyceal access marked by forceps.
- With the C-arm directed parallel to the needle,
adjustments are made in the medial and lateral directions only while the C-arm is rotated in a cranial and caudal direction. The depth of the needle is adjusted while the C-arm is rotated obliquely in the sagittal plane
- This technique requires that the needle orientation should be maintained constant in one plane while adjustments are made in the other plane
- In cases where difficult access is anticipated,
initial access into the collecting system can be attempted using a 22 G needle to opacify the system with contrast
- Definitive access is then achieved using an 18 G needle. Alternatively,
in more straightforward cases,
direct access can be attempted using the 18 G needle
- A 5Fr angle-tipped catheter is used to manipulate a guidewire down the ureter and into the bladder
- The needle is then removed and an 8 French sheath is positioned so that its distal tip lies within the proximal ureter and through this sheath a second safety wire is inserted
- The 8 French sheath is removed and balloon dilatation of the tract up to 30 French is performed,
thus forming the PNL access tract

Fig.: Figure 38: Spot fluoroscopic image demonstrating successful upper pole calyceal access with "safety" and "working" wires which have been negotiated successfully beyond the large staghorn calculus, down the ureter and into the bladder. Balloon dilatation of the tract over the "working" wire up to 30F is illustrated.
- Over the inflated balloon,
a 30 French access sheath is positioned within the calyx and the balloon is removed,
following fixation of the guidewires in situ
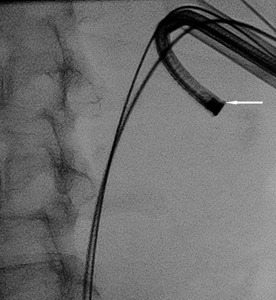
Fig.: Figure 39: Spot fluoroscopic image demonstrating two guidewires and 30F sheath in situ. A flexible nephroscope (arrow) has been advanced via the sheath into the tract, allowing direct endoscopic assessment of the calyces.
- Under direct nephroscopic visualization,
as illustrated above,
the stone burden is removed using fluoroscopic guidance

Fig.: Figure 40: Final image demonstrating 30F sheath and safety wires in situ with complete clearance of the large staghorn calculus achieved.
Catheter options:
- If patient is stone-free post procedure and there is no excessive bleeding,
a 5 Fr DAV "safety" catheter plus either 8-10 Fr nephrostomy or 12 Fr silastic Foley catheter
- If patient is stone-free post procedure with moderate bleeding,
an 8 Fr internal/external stent plus 20 Fr Council Foley + 5 Fr DAV
- If patient is stone-free and there is either urosepsis or a urine leak,
an 8 Fr internal/external stent is left in situ
- If access is supracostal,
internal ureteric stent plus 5 Fr DAV or 8-10 Fr nephrostomy
- If gross residual stone or pyonephrosis,
5 Fr DAV "safety" catheter plus 20 Fr Council Foley or 20 Fr Malecot catheter
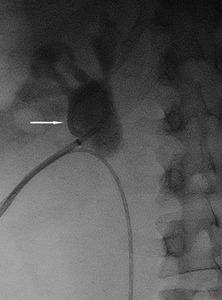
Fig.: Figure 41: Post PNL demonstrating 8.5 F pigtail nephrostomy tube in situ (arrow).
Special access situations
Obesity:

Fig.: Figure 42: Scout image from pre-PNL CT in a morbidly obese patient.

Fig.: Figure 43: Axial non-contrast CT in a morbidly obese patient who weighed 445 pounds who underwent successful PNL for treatment of multiple large calculi in the right renal pelvis and lower pole calyces.
- Morbidly obese patients may exceed the weight limit for ESWL
- Upper pole access is often preferred due to shorter skin to stone distance
- A retrograde catheter may prove invaluable in facilitating opacification of the collecting system and calculus and thus aiding percutaneous access
Retained foreign body:
- Stent fragments,
guidewires and threads from percutaneous nephrostomy tubes can occasionally be encountered in urological practice
- These act as a nidus for stone formation and frequently present with recurrent UTI

Fig.: Figure 44: Coronal reformatted image demonstrating retained basket device that has become wrapped around a calculus in a lower pole calyx. This could not be retrieved at ureteroscopy.
- A retrograde catheter is recommended cases of retained foreign bodies to facilitate opacification of the collecting system
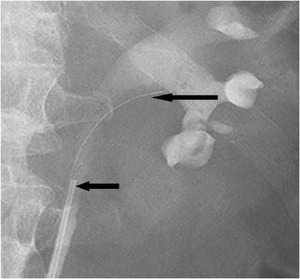
Fig.: Figure 45: Retrograde pyelogram in the same patient illustrates retrograde catheter in situ (small arrow) which has been used to opacify the collecting system with contrast. The retained basket and wire are also seen (large arrow).
- If the foreign body is situated in the renal pelvis,
a lower pole puncture is recommended
- If it is located in a peripheral calyx,
the specific calyx is targeted
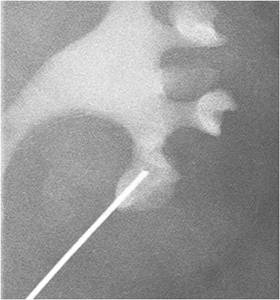
Fig.: Figure 47: Spot fluoroscopic image from the same case demonstrating selective access using an 18 G needle into the lower pole calyx containing the retained basket and stone.
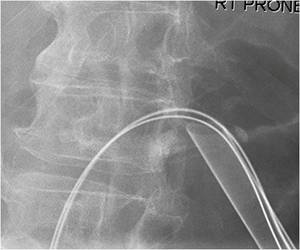
Fig.: Figure 48: The tract has been balloon dilated up to 30 Fr and a 30 Fr sheath has been left in situ.
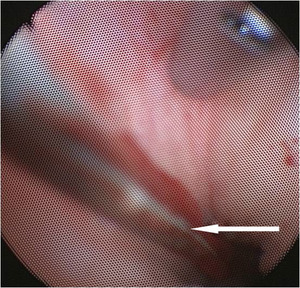
Fig.: Figure 49: Endoscopic view inside the collecting system demonstrating retained basket and wire which was successfully retrieved during PNL.
- A "mini PNL" with a 16-20 Fr sheath may be adequate for foreign body retrieval
Calyceal diverticula:
- PNL is the ideal treatment for patients with stone-bearing calyceal diverticula as it allows stone removal and ablation of the diverticular cavity [14].
- PNL is associated with high stone clearance rates (93-100%) and successful obliteration of the diverticular cavity (76-100%) with a single procedure [19].
- CT is the preferred modality for planning PNL and a retrograde catheter should be placed at the time of PNL to allow retrograde filling of the calyceal diverticulum and opacification of its connecting infundibulum
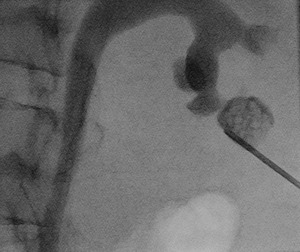
Fig.: Figure 50: Spot fluoroscopic image demonstrates successful access into the stone-bearing lower pole calyceal diverticulum using an 18G needle. Through the needle, a hydrophilic guidewire was negotiated across the connecting infundibulum and positioned within the renal pelvis

Fig.: Figure 51: Spot fluoroscopic image demonstrating 5 Fr DAV catheter advanced into the diverticulum, across the infundibulum and into the renal pelvis.
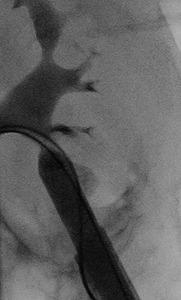
Fig.: Figure 52: Following positioning of a standard J wire into the renal pelvis, down the ureter and into the bladder, an 8 Fr sheath was positioned with its distal tip in the proximal ureter and a second "safety wire" was advanced into the urinary bladder. Tract dilation up to 30 Fr was performed as shown and a 30 Fr sheath was left in situ. The communicating neck of the diverticulum was successfully marsupialized following percutaneous stone clearance.
- In cases in which the "communicating" neck or infundibulum can be successfully crossed,
this can be marsupialized
- If the neck cannot be demonstrated or is demonstrated but cannot be crossed,
it is considered a "non-communicating" diverticulum and thermal ablation is performed
PUJ obstruction with calculi:
- 20% of patients with PUJ obstruction develop calculi
- In carefully selected patients with PUJ obstruction,
PNL combined with endopyelotomy can have success rates of up to 90%,
facilitating stone clearance and correction of the obstructed drainage at a single procedure
- A CT renal angiogram should always be performed prior to PNL
- A retrograde catheter should be placed prior to the procedure to facilitate filling of the renal pelvis and calyceal system with contrast
- Upper pole access is optimal

Fig.: Figure 53: A retrograde catheter is placed prior to PNL.

Fig.: Figure 54: The renal pelvis has been successfully opacified with contrast via the retrograde cathter demonstrating a typical PUJO configuration.
- A retrograde guidewire is advanced beyond the the PUJ into the renal pelvis and snared prom the percutaneous access point
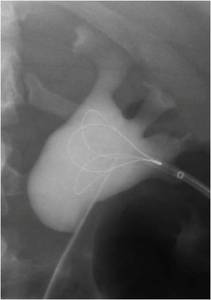
Fig.: Figure 55: A guidewire has been advanced retrogradely into the renal pelvis and is being snared via the percutaneous access tract.
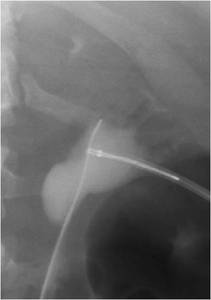
Fig.: Figure 56: The guidewire is snared and brought back into the percutaneous access tract.
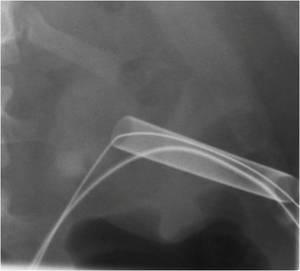
Fig.: Figure 57: The tract is then laid in the usual fashion over the guidewire following balloon dilation up to 30 Fr.
All patients in our unit undergo a routine non-contrast CT on the first post-operative day to assess for stone clearance
Complications:
| COMPLICATION |
% of all cases done |
| All minor complications |
15.3% |
| Pleural effusion |
9.3 |
| Emergency room visit post-op |
7.0 |
| UTI |
6.9 |
| Collecting system perforation |
3.1 |
| Pneumonia |
1.6 |
| Pneumothorax (no chest tube) |
0.5 |
| Urosepsis without ICU admission |
0.5 |
| Hydrothorax |
0.4 |
| Haemothorax |
0.3 |
| Pulmonary embolism |
0.3 |
| Renopleural fistula |
0.3 |
VGH Minor Complications
| COMPLICATION |
% of all cases done |
| All major complications |
8.3 |
| Bleeding requiring transfusion |
3.4 |
| Angioembolization |
0.9 |
| Large pleural effusion/empyema requiring chest tube |
0.8 |
| Urosepsis with ICU admission |
0.7 |
| Pleural decortication |
0.4 |
| MI,
DVT,
exploratory laparotomy |
0.4 |
VGH Major Complications
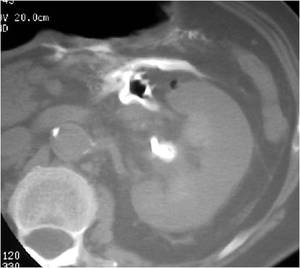
Fig.: Figure 58: Post PNL CT demonstrates extravasation of contrast from the anteromedial wall of the renal pelvis following an intraoperative perforation.

Fig.: Figure 59: Antegrade nephrostogram demonstrates almost complete resolution of urine leak 24 hours following percutaneous nephrostomy drainage.
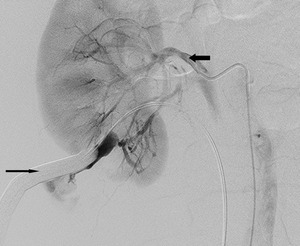
Fig.: Figure 60: Selective right renal artery angiogram in a patient undergoing elective PNL. Following balloon dilation of the tract up to 30 Fr, significant bleeding occurred via the sheath. This failed to tamponade on re-inflation of the balloon and the patient proceeded to angiography. 5 Fr catheter is present within the main renal artery (small arrow). There is active extravasation of contrast from a lower pole branch of the renal artery which is seen refluxing along the inflated balloon (large arrow) and out the tract. Successful selective embolization of the bleeding vessel was performed.

Fig.: Figure 61: Bifid system with upper and lower pole calculi requiring upper and lower pole access tracts.

Fig.: Figure 62: Upper and lower pole access was performed. On fluoroscopic imaging, the upper pole access was thought to be supra-11th rib.

Fig.: Figure 63: Reformatted image from post-procedure CT demonstrates that the upper pole access was in fact supra-10th and transgressed the spleen. The patient was asymptomatic.
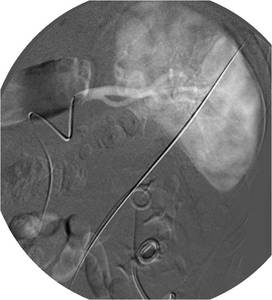
Fig.: Figure 64: All tubes and catheters were left in situ for one week. The patient was brought to the Interventional Radiology suite for tube removal following catheterization of the splenic artery in the event emergency embolization was necessary.

Fig.: Figure 65: Splenic artery angiogram showed no evidence of extravasation and the nephrostomy was removed uneventfully.

Fig.: Figure 66: Upper and lower pole access was obtained for PNL of a large stone burden in the right kidney.
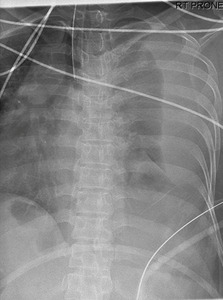
Fig.: Figure 67: During the procedure, the patient became progressively difficult to ventilate. The chest was screened with fluoroscopy demonstrating a large right hydrothorax.
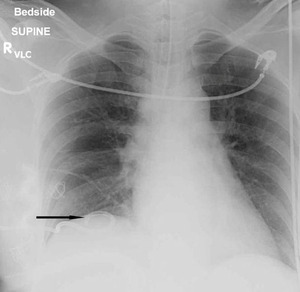
Fig.: Figure 68: An 8 Fr pigtail catheter (arrow) was inserted under ultrasound guidance to drain the large right effusion. Supracostal puncture is associated with a 15% risk of hydrothorax compared with 1.4% when a subcostal approach is used. On table fluoroscopy of the thorax provides quick assessment in cases where the patient suffers compromised respiratory status during PNL, particularly in upper pole punctures.

