I.
Oropharyngeal Functional Abnormalities
The most common cause of oropharyngeal functional abnormalities are neurologic causes including cerebrovascular accidents,
multiple sclerosis,
alzheimer,
amyotrophic lateral sclerosis,
myasthenia gravis among others.
A.
Cricopharyngeal Dysfunction
The upper esophageal sphincter main component is the cricopharyngeal muscle,
it must completely relax for the upper esophageal sphincter (UES) to be able to open and let the bolus pass.
Cricopharyngeal dysfunction refers to incomplete relaxation or an early closure of the muscle that can cause a dilatation of the proximal esophagus and trapping of the bolus leading to possible complications as are aspiration and penetration.
On imaging findings we expected to find a prominent cricopharyngeal muscle which as been associated with a muscle weakness.
A prominent cricopharyngeal muscle can be seen as a posterior indentation on barium studies 4.
II.
Esophageal Motility Disorders
A.
Diffuse Esophageal Spasms
Diffuse esophageal spasms is a motility disorder that consists of multiple spontaneous,
uncoordinated and non peristaltic esophageal contractions that obliterate the lumen 4,7.
It commonly presents in patients older than 50 years old causing intermittent chest pain or dysphagia.
On fluoroscopy studies the esophagus can present with the classic presentation of a corkscrew appearance on a few amount of patients,
more commonly the patients can present with a normal barium swallow because most patients have mild to moderate severity contractions that don’t give the corkscrew appearance.
Some cases may present with esophageal diverticulum formation11.
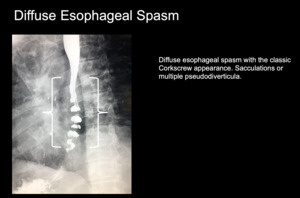
Fig. 1
References: Department of Diagnostic Radiology, University of Puerto Rico
B.
Achalasia
Achalasia is a motility disorder that is caused by a loss of the inhibitory neurons at the myenteric plexus preventing the relaxation of the lower esophageal sphincter (LES).
As a consequence the pressure at the LES is increased which leads to a dilatation of the distal esophagus.
Patients present clinically with dysphagia to solids and liquids,
chest pain and regurgitation.
On barium swallow achalasia presents as esophageal dilatation with a tapered beak-like narrowing distally adjacent to the gastroesophageal junction 4,7.
Loss of normal peristaltic waves can also be seen at the lower two thirds of the esophagus11.
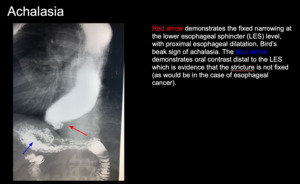
Fig. 2
References: Department of Diagnostic Radiology, University of Puerto Rico
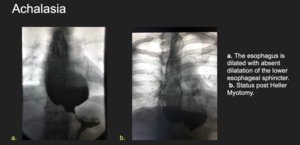
Fig. 3
References: Department of Diagnostic Radiology, University of Puerto Rico
C.
Scleroderma
Scleroderma is an autoimmune disorder of collagen deposition in the body,
as collagen deposits in the smooth muscle of the esophagus it leads to a diminished or absent peristalsis.
The lower esophageal sphincter (LES) loses its tone and develops hypotension,
resulting in an incompetent LES which leads to constant gastroesophageal reflux and a dilated esophagus 11.
Patient present clinically with a chronic heartburn,
acid regurgitation and dysphagia due to the strictures that occur as a consequence of the relentless gastroesophageal reflux disease (GERD).
11
On barium swallow scleroderma presents as esophageal dilatation with a patulous distal esophagus and GEJ 4.

Fig. 4
References: Department of Diagnostic Radiology, University of Puerto Rico
III.
Structural Abnormalities
A.
Zenker diverticulum
A zenker diverticulum is a pseudodiverticulum (containing only mucosa and submucosa) that herniates at the level of the hypopharynx at an area of focal weakness called Killian triangle,
which is located between the cricopharyngeal and thyropharyngeus muscle.
Patients present clinically with symptoms related to the presence of undigested bolus material at the diverticulum.
Symptoms can include: dysphagia,
halitosis,
regurgitation,
globus sensation.
On barium swallow the zenker diverticulum is seen as a diverticulum protruding at midline in the posterior wall of the pharynx.
If the diverticulum is large enough it can be seen extending to the lateral aspect of the esophagus 4.
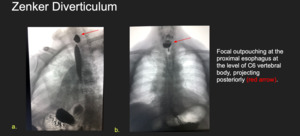
Fig. 5
References: Department of Diagnostic Radiology, University of Puerto Rico
B.
Killian-Jamieson Diverticula
Killian-Jamieson diverticulum is a pseudodiverticulum that arises more inferiorly than the Zenker diverticulum,
specifically it arises at the Killian Jamieson space which is located below the cricopharyngeal muscle 4.
This diverticulum occurs most commonly unilateral on the left side,
only a 25% of cases are bilateral.
Patients are usually asymptomatic.
On barium studies it appears as an outpouching arising from the lateral and anterior wall of the cervical esophagus.
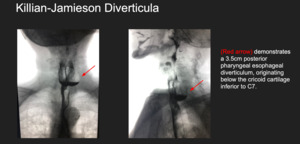
Fig. 6
References: Department of Diagnostic Radiology, University of Puerto Rico
C.
Epiphrenic Diverticula
Epiphrenic diverticula are pulsion pseudodiverticulum that occur at the distal one third of the esophagus resulting from an increased intraluminal pressure.
They have been strongly associated to motility abnormalities 4.
Patients present clinically with dysphagia and regurgitation.
On barium swallow it presents as an outpouching above the LES.

Fig. 7
References: Department of Diagnostic Radiology, University of Puerto Rico
D.
Esophageal Intramural Pseudodiverticula
Esophageal Intramural Pseudodiverticula are the result of dilated excretory ducts of the deep mucous glands in the esophagus 7.
Depending on the location of the diverticula the etiology can be determined,
if the diverticula are arranged in a cluster on the distal aspect of the esophagus most likely are the result of reflux esophagitis; if the diverticula have a diffuse distribution along the esophagus most like are associated with high esophageal strictures or an isolated finding 7.
On barium swallow it can be seen as flag shaped outpouchings in a row parallel to the longitudinal axis of the esophagus.
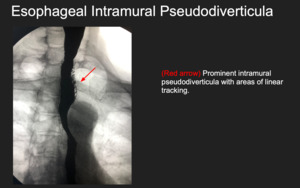
Fig. 8
References: Department of Diagnostic Radiology, University of Puerto Rico
E.
Esophageal Webs
Esophageal webs are mucosal membranes that project into the esophageal lumen.
Webs occur most commonly on the anterior aspect of the cervical esophagus but can occur circumferentially.
Patients can be asymptomatic but depending on the degree of luminal obstruction patients may have symptoms of dysphagia and regurgitation.
On barium swallow esophageal webs present as a filling defect 4 and can lead to proximal esophageal dilation depending on the degree of luminal obstruction.
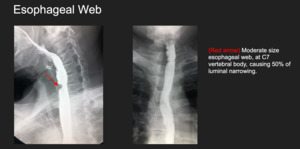
Fig. 9
References: Department of Diagnostic Radiology, University of Puerto Rico
F.
Schatzki Ring
Schatzki ring is the most common esophageal ring,
occuring at the level of the distal esophagus.
It has been associated with the presence of a hiatal hernia.
Patients present clinically with intermittent or episodic dysphagia and food impaction.
The frequency and severity of symptoms correlate with the amount of esophageal luminal diameter at the area of the ring.
If the luminal diameter is less than 13mm patients will frequently be symptomatic,
on the contrary if the luminal diameter is greater than 20mm patients will rarely be symptomatic.
On barium swallow schatzki ring presents as a circumferential narrowing at the distal esophagus 4.
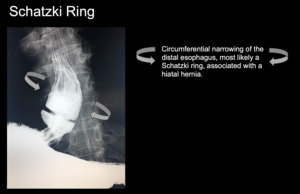
Fig. 10
References: Department of Diagnostic Radiology, University of Puerto Rico
IV.
Esophageal Infections
A.
Candidiasis
Esophageal candidiasis is the most common infection among immunocompromised patients.
Clinically it presents with odynophagia as well as dysphagia.
On barium swallow esophageal candidiasis presents as plaque or nodular lesions that are longitudinally oriented along the esophagus and are separated by normal mucosa.
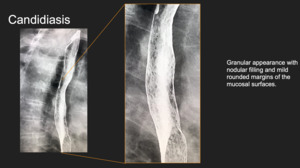
Fig. 11
References: Department of Diagnostic Radiology, University of Puerto Rico
V.
Gastroesophageal reflux disease
Gastroesophageal reflux disease (GERD) is a spectrum of disease in which the acidic gastric contents pass into the esophagus as a consequence of a weakened lower esophageal sphincter.
Patients typically will present with heartburn that is worse with spicy foods and recumbency and better with sitting up and antacids.
Some atypical presentations of GERD include: dry cough,
hoarseness,
adult onset asthma.
Using barium swallow studies doctors can document the presence of gastroesophageal reflux,
the presence of a hiatal hernia and asses the possible complications of the disease.
On barium studies GERD can have several presentations:
-
The esophagus can have a finely nodular or granular appearance with poorly defined radiolucencies that fade peripherally due to edema and inflammation of the mucosa 7.
-
Also we can expect to see shallow ulcers and erosions on the distal aspect of the esophagus.
-
An inflammatory esophagogastric polyp can be present; it’s a single enlarge fold that arises from the gastric cardia and extends upward into the distal esophagus 7.
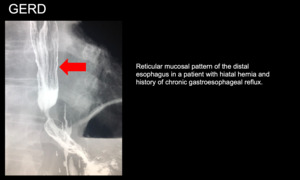
Fig. 12
References: Department of Diagnostic Radiology, University of Puerto Rico
VI.
Esophageal Strictures
A.
Distal Esophageal Strictures
Distal esophageal strictures are most commonly caused by GERD.
Usually they have a concentric symmetric appearance but may also present asymmetrically.
The scarring caused by the chronic GERD may lead to saculations or esophageal intramural pseudodiverticulosis 7.
Distal esophageal strictures can also be caused by scleroderma,
zollinger-ellison syndrome,
indwelling nasogastric tube,
among others 4.
On barium swallow they appear as a smooth tapered narrowing that extends for a distance of 1-4cm and is usually concentric.
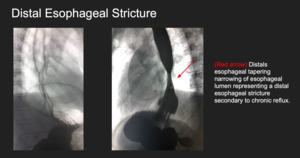
Fig. 13
References: Department of Diagnostic Radiology, University of Puerto Rico
B.
Upper to Mid-Esophageal Strictures
Strictures located on the upper two thirds of the esophagus are most likely a consequence of Barrett esophagus,
a condition that occurs as a sequelae of longstanding GERD.
Barrett esophagus occurs due to a metaplastic change from the normal squamous epithelium of the esophagus to a columnar epithelium,
increasing the risk for the development of esophageal adenocarcinoma.
Upper to Mid-Esophageal strictures can also be caused by mediastinal radiation therapy,
caustic ingestions,
medication induced,
congenital esophageal stenosis,
among others 4.
On barium swallow a highly specific sign of Barrett esophagus is a reticular mucosal pattern (tiny barium filled grooves) 7.
Upper to Mid-Esophageal strictures appear as a concentric focal decrease in the lumen of the esophagus.
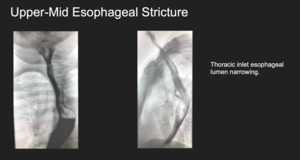
Fig. 14
References: Department of Diagnostic Radiology, University of Puerto Rico
VII.
Esophageal Cancer
There are two types of esophageal cancer adenocarcinoma and squamous cell carcinoma.
Historically the most common was squamous cell carcinoma,
but recently the incidence of adenocarcinoma has dramatically increased.
Theories for the increasing incidence of adenocarcinoma include a higher incidence of GERD,
obesity,
dietary changes.
Esophageal cancer clinically presents as dysphagia to solids progressing to liquids as the tumor expands,
weight loss,
chronic worsening GERD.
Adenocarcinoma is mostly found on the distal third of the esophagus and may arise as a consequence of Barrett or gastric cancer invading the esophagus.
Squamous cell carcinoma is commonly found in the upper two thirds of the esophagus,
in patients with a long standing history of tobacco or alcohol consumption 7.
On Barium swallow cancerous lesions may appear with an infiltrative,
ulcerative,
polypoid pattern.
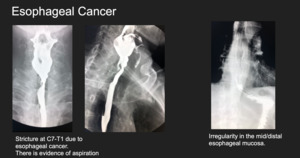
Fig. 15
References: Department of Diagnostic Radiology, University of Puerto Rico
