An interesting case here showing an unusual symptom referral pattern of the upper trapezius. Read on.
A patient sought medical assistance of her primary care physician due to constant right lateral 5th digit numbness. Although no specifics of why the symptoms arose, she did say her activity increased a few days prior while participating in a tennis match and coaching volleyball in the same day. She did state for a few days she had symptoms in the lateral brachium but that did not last and didn’t think anything much of it until numbness arose, which is why she sought medical care.
Upon arrival to me, her main complaint (numbness in 5th digit) was constant even after medical interventions of prednisone series and cortizone shot in the contralateral arm. She has also had magnetic resonance imaging of the cervical spine that was basically unremarkable (most of the degenerative and stenotic changes were actually shown on the contralateral side of the symptoms). Otherwise, she was pain-free. No neck pain but noticed lifting anything over shoulder height was difficult, not symptomatic though.
She had no pain with cervical range of motion and no change in symptoms with a repeated movement exam with and without PT overpressure. She had full, pain-free active range of motion of the shoulder (yes, full range and no impingement arch) but 3-/5 MMT of the infraspinatus and teres minor tested at neutral by side. Abduction and flexion were 4-/5 but pain-less, just weak. No pain to provocation at the subacromial space. Negative impingement test (Neers and Hawkins-Kennedy of the shoulder too).
She did have hypomobility at the cervicothoracic junction and at the C5-6 joint that led to performing joint manipulation but no change in symptoms. Otherwise, no myofascial trigger points were found through a palpatory examination to elicit concordant symptoms.
Considering no change in symptoms through a movement and arthrogenic approach, and not satisfied with the outcome, I decided to dig further into one of the main findings, weakness of the rotator cuff (but not your typical impingement symptoms). I hypothesized that she was compensating for altered glenohumeral mechanics due to this motor performance loss by performing a shoulder shrug sign. This was not visible by the naked eye but made sense.
I opted to perform dry needling to the upper trapezius after finding a myofascial trigger point upon pincer palpation, even though just local discomfort and not concordant. After entering approximately 30mm, there was reproduction of concordant signs (in addition to local twitch response) that eventually lessened after completion of both a static and dynamic influence.
The symptoms dampened but did not completely abolish after the treatment. However, upon the following visit, she reported that they were abolished the next day. Not exactly what I was expecting, but hey it worked.
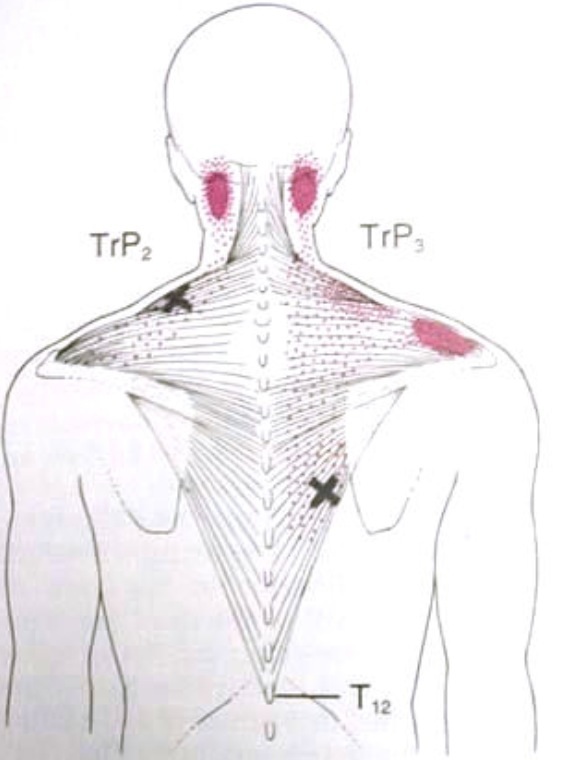
So the change in symptoms could have come from some of the other interventions, but considering concordant symptoms were found after penetration and not by palpation by hands, this was quite interesting to me and worth sharing. The referral pattern is quite different from the proposed ones by Travell and Simons.
Have you had any cases of true referral patterns from the upper trapezius, and if so, where?



How old was the patient? You mentioned degenerative changes were found on imaging on the contra lateral side.. I would think this side could be hypo mobile which would shift the axis of rotation from midline toward the degenerative side, making the symptomatic side hyper mobile thus perpetuating a facilitated segment that could explain the 5th digit numbness. You mentioned C5-6 and CT was hypo, so this could explain a hyper mobility below at c6-7 to make up for mobility loss as C5-6 and CTJ which again would explain segmental facilitation showing up on the 5th digit. Did you do a thorough sensory screening? Any tropic changes or sympathetic changes? I have never seen a referral by UT like this but I guess it could be possible. I just question if it might be coming from the neck and the UT is a secondary finding that also produced similar symptoms
Hey Steve,
Great inquiries below. The patient is 55 i think. I do think too it would be referral from the lower cervical spine. Main interesting finding is reproduction of concordant symptoms (intensified) with penetration of upper trap. I am working on the spine of course too.
Hello,
I recently saw 3 patients (all in their mid 20 twenties with no degenerative changes in the spine) in the past one month with complaints of 5th digit numbness. I was surprised that palpation of upper trapezius revealed trigger points which actually intensified numbness along the 5th digit. When I performed dry needling to the trigger points of the upper trapezius, LTR were obtained. The numbness in the 5th digit disappeared the next session. This happened with all the three patients whom i treated last month. I’m sure this new pattern needs to be investigated and glad I bumped into this case description you gave.
Thanks for commenting. Yes, referral patterns can be quite interesting. It is difficult to say if needling the UT was the actual cause for decrease in numbness, or the tonal effects that dampened from that procedure, which could alter the lower cervical spine.
Either way, great results. Keep it up!
H