Decreased Ankle Dorsiflexion
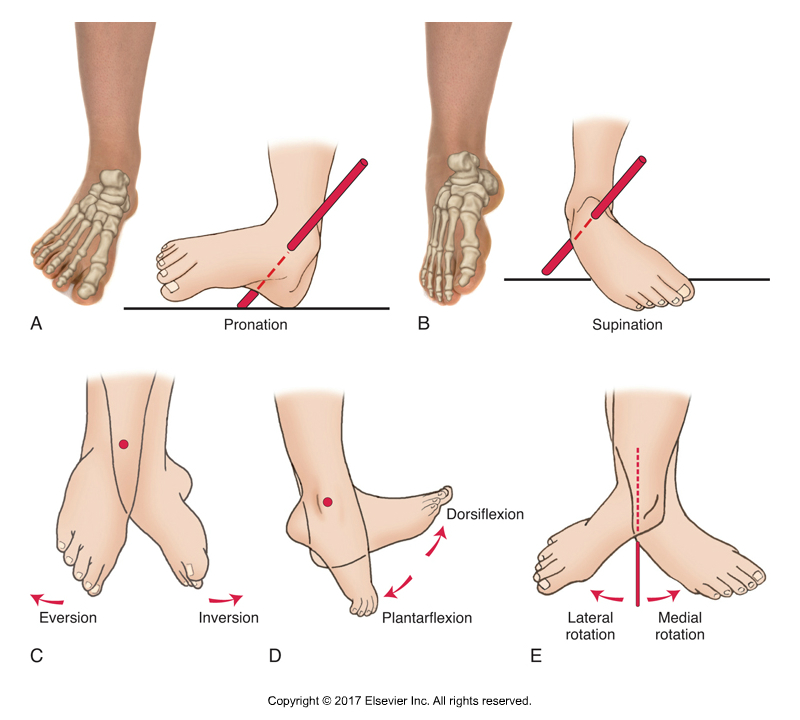
Ankle joint dorsiflexion and plantarflexion. Permission Joseph E. Muscolino. Kinesiology – The Skeletal System and Muscle Function, 3rd ed. (Elsevier, 2017).
Decreased ankle dorsiflexion has been reported as a risk factor for some lower extremity conditions, such as patellar tendinopathy, Achilles tendinopathy, chronic ankle instability, metatarsal stress fractures, plantar fasciitis, and anterior knee pain.
Decreased Ankle Dorsiflexion and Knee Valgus
Decreased ankle dorsiflexion has also been reported as a possible contributor to excessive knee valgus (genu valgus), also known as dynamic knee valgus. Dynamic knee valgus is a combination of excessive femoral adduction and internal rotation, and tibial internal rotation and “abduction” relative to the femur, with medial displacement of the knee. In other words, restricted dorsiflexion has been associated with a relatively large internal rotation distortion pattern of the lower extremity relative to a fixed foot and pelvis.
Effects of Limited Ankle Dorsiflexion
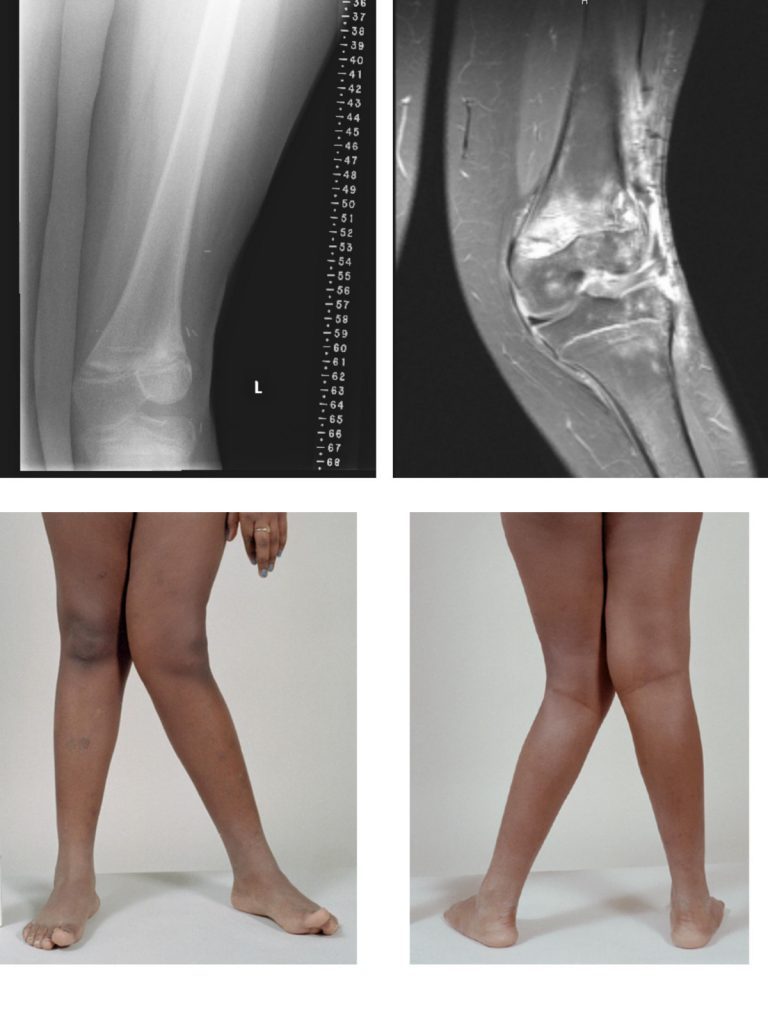
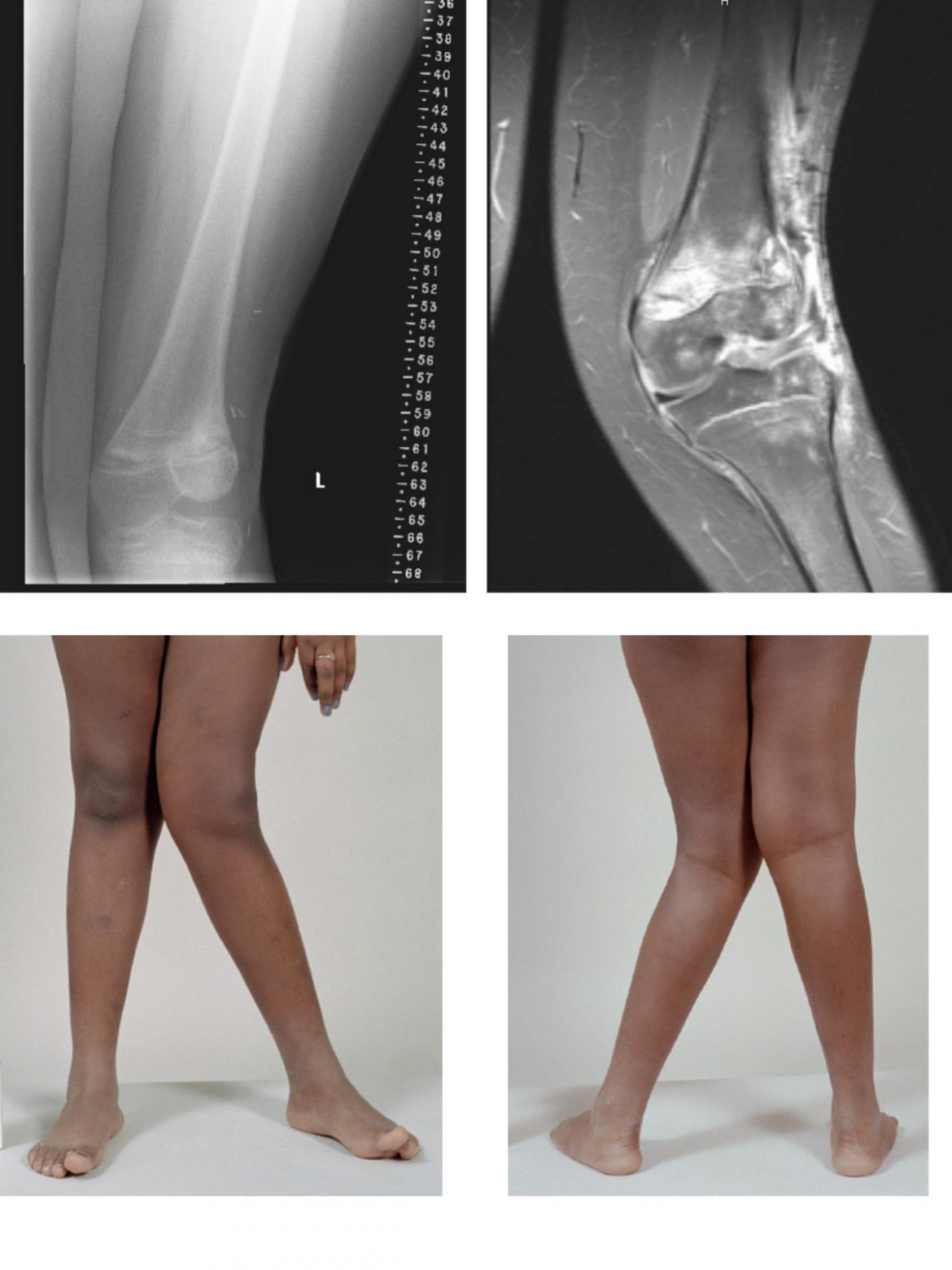
Genu Knee Valgus. X-Ray and MRI at top. Photographs of same individual seen at bottom (anterior view at left and posterior view at right). Knee valgus effectively involves “abduction” of the tibia/leg at the knee joint.
It has been hypothesized that decreased ankle dorsiflexion is due to the decreased extensibility of the gastrocnemius/soleus complex and restricted posterior talar glide on the tibia. It is further hypothesized that as subjects perform activities that increase knee flexion, this requires the tibia to move forward over the foot, thus increasing dorsiflexion. However, if the ankle has restricted restricted dorsiflexion, then subjects may try to compensate for this lack of sagittal plane knee joint flexion range of motion with movement in the frontal and/or transverse planes throughout the kinetic chain. This compensation may come from the pronation of the foot, the internal rotation of the tibia, internal hip rotation and adduction, or pelvic drop, thus causing the dynamic knee valgus.
Comment by Joseph E. Muscolino
Another possible biomechanical explanation might be that the restricted ankle joint dorsiflexion directly results in overpronation of the foot at the subtalar joint, which then in turn causes the knee valgus. The following reasoning is used: During the gait cycle (walking), the foot lands in supination at heel strike, then moves into pronation during midstance, and then returns to a supinated position during toe off. Therefore, if ankle dorsiflexion is limited, it will be difficult for the foot to transition from midstance to toe off because this transition requires the foot to dorsiflex. So without the necessary dorsiflexion, the foot ends up leaving the ground while still in the collapsed-arch position of midstance pronation.
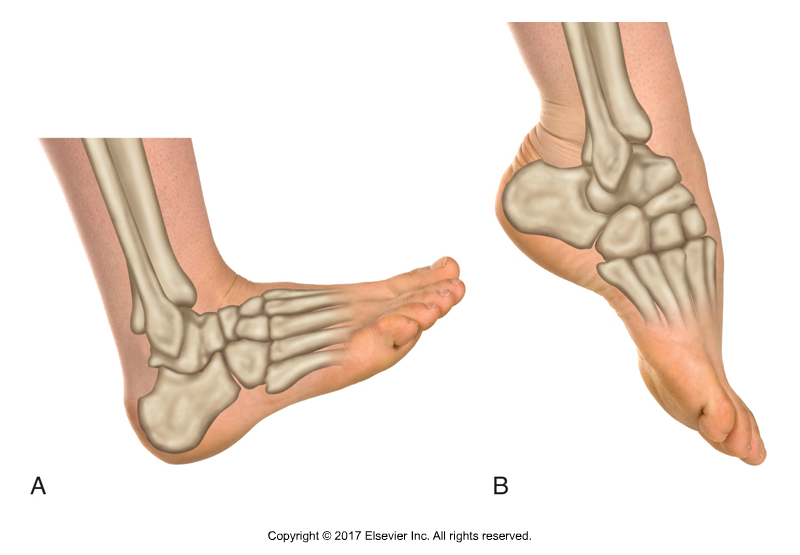
Pronation and Supination of the foot at the subtalar joint. Permission Joseph E. Muscolino. Kinesiology – The Skeletal System and Muscle Function, 3rd ed. (Elsevier, 2017).
Pronation then directly causes the internal (medial) rotation of the talus because the closed-chain reverse action of open-chain calcaneal pronation involves talar medial (internal) rotation. But the ankle joint does not allow any transverse plane rotation to occur, so if the talus internally rotates, the tibia must internally rotate with it. And when standing in full or near full extension, the knee joint does not allow any rotation, so if the tibia rotates internally, the femur must internally rotate with it (and the patella rides on the femur, so it follows whatever the femur does). So the entire tibia/femur (and patella) complex ends up rotating inward.
This then puts a strain on the external (lateral) rotation musculature at the hip joint to try to restrain the femoral internal rotation. Unable to do this, the musculature loses to the femoral rotation and lengthens. But given that this musculature is also abduction musculature of the thigh at the hip joint, when this musculature lengthens, the thigh is allowed to fall not only into internal rotation, but adduction as well. Once the thigh adducts, the (lower) leg must have a valgus (abducted) position outward if we are to have an approximate shoulder-width stance of our feet. Therefore, we end up with dynamic genu valgus!
Did you know that Digital COMT (Digital Clinical Orthopedic Manual Therapy), Dr. Joe Muscolino’s video streaming subscription service for manual and movement therapists, has an entire folder of video lessons on pathomechanics of common musculoskeletal conditions? Digital COMT adds seven new video lessons each and every week. And nothing ever goes away! Click here for more information.
Study

Excessive genu valgum and genu varum. Permission Joseph E. Muscolino. Kinesiology – The Skeletal System and Muscle Function, 3rd ed. (Elsevier, 2017).
To provide an evidence for their hypothesis, researchers from Federal University of Ceará, Brazil conducted a systematic review to evaluate the association between ankle dorsiflexion and dynamic knee valgus. The review was published in Physical Therapy in Sport journal.
The researchers searched publications related to the conditions and found seventeen studies which met the inclusion criteria.
Results
The meta-analysis showed that reduced ankle dorsiflexion is associated with participants presenting with dynamic knee valgus compared to controls.
Further analysis showed consistent results regarding different forms of ankle dorsiflexion measurement which were correlated with dynamic knee valgus: restriction in active dorsiflexion measured in a weight-bearing position, non-weight-bearing with knee flexed, or non-weight-bearing with knee extended.
Application?
Thus, this review provided evidence that reduced ankle dorsiflexion is correlated with dynamic knee valgus (although the exact causal relationship between the two is not yet fully clear). Because of this correlation, it was suggested that therapists should include ankle joint dorsiflexion assessment in their practices as it might indicate the risk of injurious lower limb distortional posture and movement patterns.
Final Comment by Joseph E. Muscolino
The lower extremity kinematic chain of elements is extremely interdependent. If any one joint loses mobility, then because of the closed-chain stance that occurs during 60% of the gait cycle with the foot, the distal element of the kinematic chain of elements, fixed on the ground, every other joint in the kinematic chain also becomes restricted. For this reason, a hypomobile lower extremity joint tends to have greater repercussions upon the rest of the joints of the kinematic chain, than a hypomobile joint in the upper extremity kinematic chain.
This blog post article was created in collaboration with www.terra.rosa.com.au.
(Click here for the blog post article: What is Overpronation and what are its Causes?)
Did you know that Digital COMT (Digital Clinical Orthopedic Manual Therapy), Dr. Joe Muscolino’s video streaming subscription service for manual and movement therapists, has an entire folder of video lessons on pathomechanics of common musculoskeletal conditions? Digital COMT adds seven new video lessons each and every week. And nothing ever goes away! Click here for more information.
