
Abstract
Aims/hypothesis
Tractable precision biomarkers to identify immunotherapy responders are lacking in type 1 diabetes. We hypothesised that proinsulin:C-peptide (PI:C) ratios, a readout of beta cell stress, could provide insight into type 1 diabetes progression and responses to immunotherapy.
Methods
In this post hoc analysis, proinsulin and C-peptide levels were determined in baseline serum samples from 63 participants with stage 2 type 1 diabetes in the longitudinal TrialNet Teplizumab Prevention Study (n=41 in the teplizumab arm; n=22 in the placebo arm). In addition, previously tested demographic, C-peptide, glucose and proinsulin data were used for the new data analyses. The ratio of intact (unprocessed) proinsulin to C-peptide was analysed and relationships with progression to stage 3 diabetes were investigated.
Results
Elevated baseline PI:C was strongly associated with more rapid progression of diabetes in both the placebo and teplizumab treatment groups, but teplizumab abrogated the impact of high pre-treatment PI:C on type 1 diabetes progression. Differential responses of drug treatment in those with high vs low PI:C ratios were independent of treatment effects of teplizumab on the PI:C ratio or on relevant immune cells.
Conclusions/interpretation
High pre-treatment PI:C identified individuals with stage 2 type 1 diabetes who were exhibiting rapid progression to stage 3 disease and who displayed benefit from teplizumab treatment. These data suggest that readouts of active disease, such as PI:C ratio, could serve to identify optimal candidates or timing for type 1 diabetes disease-modifying therapies.
Graphical Abstract

Similar content being viewed by others

Introduction
Type 1 diabetes results from progressive autoimmune beta cell destruction [1]. As type 1 diabetes develops, inflammatory mediators and immune cells inflict direct and metabolic stress on beta cells [2]. These stressors may lead to oxidative stress and endoplasmic reticulum (ER) stress via unfolded protein response (UPR) induction and activation of proapoptotic signals [2,3,4,5,6]. These pathways are intrinsic to beta cells, but a marker of these events in the peripheral blood would be a valuable tool to track the effects of immune therapies on beta cells or to determine when retreatment is appropriate. Our group and others have shown that prior to the clinical diagnosis of type 1 diabetes, the circulating proinsulin:C-peptide ratio (PI:C ratio) can be used as a biomarker of multiple stress pathways, whereby elevations in PI:C identify disease progression [7,8,9,10,11,12]. However, stage-specific impacts of PI:C ratio on progression and relationships with type 1 diabetes prevention are unknown.
The anti-CD3 monoclonal antibody (mAb) teplizumab, was recently approved for treatment to delay type 1 diabetes diagnosis (Stage 3 type 1 diabetes) in persons with multiple islet autoantibodies and dysglycaemia (Stage 2 type 1 diabetes). In the TrialNet teplizumab prevention trial (TN10), beta cell function, measured as the C-peptide response to an OGTT, improved over the first year after therapy compared with deterioration in placebo-treated participants [13, 14]. Despite the improvement in stimulated C-peptide responses, while on-treatment, cross-sectional PI:C values were similar between placebo and teplizumab groups [14]. These findings suggested that in the overall study cohort, beta cell stress persisted despite improved beta cell function with teplizumab treatment. Here, to better understand this surprising finding, we took advantage of this unique and invaluable study cohort to define individual changes in PI:C over time, the relationships between PI:C and progression to stage 3 type 1 diabetes, and relationships to other mechanistic markers of treatment effect in the successful TN10 prevention trial.
Methods
Trial design and participants
The design of the double-blinded, randomised TN10 Teplizumab Prevention Study has been previously reported [13]. Inclusion criteria included: age 8–45 years, family history of type 1 diabetes, confirmed positivity for at least two islet autoantibodies and dysglycaemia on OGTT. Exclusion criteria included: diagnosis of stage 3 type 1 diabetes; abnormalities in blood counts, liver enzymes or international normalised ratio; positive purified protein derivative test; vaccination with live virus within 6 weeks of randomisation; evidence of acute infection; serological evidence of past human immunodeficiency virus; hepatitis B or C infections; current pregnancy or lactation; or treatment with monoclonal antibody in the past year. Race/ethnicity and sex/gender were self-reported. Similar to other type 1 diabetes-related studies [15], the sample underrepresented individuals identifying as Hispanic and non-white; additionally, children under 8 years of age were not included. Briefly, participants received a 14 day intravenous infusion of teplizumab or saline (154 mmol/l NaCl), then were followed longitudinally with OGTTs after 3 months, then every 6 months, for diabetes development. Institutional review board approval with consent and assent as appropriate was obtained as described. The trial was registered on ClinicalTrials.gov (registration no. NCT01030861).
Sample collection and measurements
Serum samples were available for 63 of the 76 study participants. Overall, these participants had similar baseline characteristics to participants for whom samples were not available (n=13; electronic supplementary material [ESM] Table 1). As part of this post hoc analysis, study baseline serum samples were obtained with approval from the TrialNet Collaborative Mechanistic Studies panel and proinsulin and C-peptide testing were performed on these samples. Previously tested and described demographic, C-peptide, glucose and proinsulin data generated by the authors’ prior analyses [16] were used for the new data analyses included in the current manuscript.
Pre-treatment samples were obtained from the screening visit (n=58, randomly timed), the baseline visit (n=17, fasting) and approximately every 6 months (fasting) after the start of treatment. Screening visit samples were utilised for analyses; if a sample at the screening visit was not available, baseline visit samples were used. When available (n=12), randomly collected vs fasting intraindividual PI:C ratios from both visits were highly correlated (r=0.993, p<0.0001). Thus, for participants with only fasting baseline visit samples (n=5), values were transformed using a linear regression model to approximate screening visit values.
OGTT C-peptide levels (pmol/ml) were measured with the TOSOH C-peptide assay (TOSOH Biosciences, Japan). Proinsulin (pmol/ml) was measured using the Teco intact proinsulin ELISA (TECOmedical Group, Switzerland), which quantifies ‘intact’ or unprocessed insulin, but not partially processed split products. Performance characteristics have been externally validated and reported in detail [17]. PI:C values were calculated as an equimolar ratio × 100.
Peripheral blood mononuclear cells (PBMCs) were processed and stored at the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) repository, then analysed via flow cytometry analysis by the Immune Tolerance Network Core at Benaroya Research Institute as described [16, 18].
Statistical methods
In this post hoc analysis, between-group differences were compared using Wilcoxon rank sum tests or χ2 or Fisher’s exact tests. Correlations were assessed using Spearman rank correlation tests. Cut point analyses in relation to time to stage 3 type 1 diabetes used the aggregate mean and were validated with recursive partitioning analyses (using the Comprehensive R Archive Network [CRAN; https://CRAN.R-project.org/package=rpart] in R [v.4.0.3; http://www.R-project.org/]). Ratio and fold change variables were log2 transformed for model inclusion, and C-peptide AUC measures were log(x+1) transformed. Time to stage 3 type 1 diabetes was estimated using the methods of Kaplan and Meier, and Cox regression models were used to assess influence of markers of interest in univariate, multivariable and time-dependent covariate analyses. Time-dependent receiver operating characteristic (ROC) curves and AUC analyses (timeROC package in R) as well as C-indices (compareC package in R) were utilised to evaluate the discriminative ability of baseline PI:C ratio as a prognostic factor for the time to progression to stage 3 type 1 diabetes. Averaged PI:C ratio AUC, used to assess aggregate beta cell stress across study time points, was evaluated using the trapezoidal method, divided by number of months [16]. The pre-treatment PI:C ratio was highly correlated with the on-study averaged AUC of the PI:C ratio (Pearson’s r=0.79, p<0.001) (ESM Fig. 1). Therefore, for modelling and assessment of treatment effects, corrections for the baseline PI:C were made. Given the hypothesis-generating nature of these analyses, multiple comparison corrections were not used, and statistical significance was defined as p<0.05. Analyses were conducted using the R statistical package (v.4.0.3; http://www.R-project.org/).
Results
Evaluable cohort characteristics
Demographic features at baseline (n=63) (ESM Tables 1–3) were similar across treatment groups. The mean pre-treatment PI:C ratio (Fig. 1a) was 0.48 (median: 0.42; range: 0.06–1.42) for teplizumab-treated participants (n=41) and 0.49 (median: 0.36; range: 0.14–1.60) for placebo (n=22) (p=0.87). Pre-treatment absolute proinsulin values were also similar across treatment groups (ESM Table 2, p=0.49). In line with previous observations [8, 17], age at enrolment and the pre-treatment PI:C ratio were inversely related (Fig. 1b; r=−0.36, p=0.004).

In individuals with stage 2 type 1 diabetes, PI:C is inversely associated with age and predicts progression to stage 3 type 1 diabetes. (a) Pre-treatment PI:C values for 63 individuals participating in the TrialNet Teplizumab Prevention Study. Values were not different between treatment groups (p=0.87). The whiskers reflect roughly a 95% CI for the median (thick horizontal line), while the top and the bottom of the box are the 1st and 3rd quartiles (25th and 75th percentiles). (b) Age was inversely related to pre-treatment PI:C ratios (r=−0.36; p=0.004). (c) Kaplan–Meier curve showing distribution of the time to progression to stage 3 diabetes based on high vs low baseline PI:C ratio of the entire cohort, regardless of treatment group, with multivariable Cox regression adjusting for age and baseline C-peptide AUC (high pre-treatment PI:C, n=23; low pre-treatment PI:C, n=40). T1D, type 1 diabetes
The PI:C ratio predicts time to diagnosis of stage 3 type 1 diabetes
Participants were followed for a median of 72 months (95% CI 61, 87 months). Stage 3 type 1 diabetes was diagnosed in 41 participants (23 of 41 in the teplizumab arm and 18 of 22 in the placebo arm). The median time to diagnosis was somewhat longer than reported in the complete study cohort amongst the placebo group (35.4 months for placebo vs 59.7 months for teplizumab, logrank p=0.037).
We evaluated the PI:C ratio and its influence on prognosis (time to progression to stage 2 type 1 diabetes) as both a continuous and a dichotomised measure. First, we evaluated the data based on a continuous measure of the PI:C ratios. When both treatment arms were pooled, the pre-treatment PI:C ratio as a continuous measure was significantly associated with the likelihood of progressing to stage 3 type 1 diabetes (HR 2.29; 95% CI 1.45, 3.61; p<0.001; data not shown), even after adjusting for age and baseline C-peptide AUC. We also examined the association with the pre-treatment absolute proinsulin levels and time to stage 3 diabetes, but this relationship was not significant after adjustment for age and baseline C-peptide AUC (p=0.97; data not shown).
To facilitate comparisons between groups, we also dichotomised the pre-treatment PI:C ratio as ‘high’ vs ‘low’ in approximation to the overall mean and based on partitioning analyses. The cut point identified approximated the mean baseline PI:C ratio for the placebo group (i.e. ~0.50), supporting this approach to this exploratory evaluation. High ratios (i.e. ≥0.5%) were present in seven of 22 (32%) placebo-treated participants and in 16 of 41 (39%) teplizumab-treated participants (p=0.77) (ESM Table 3). Participants with high ratios were younger compared with those with low ratios (median: 15 vs 21 years, respectively; p=0.017). Compared with participants with low ratios, those with a high pre-treatment PI:C ratio had similar pre-treatment C-peptide AUC values (p=0.50); rather, a high pre-treatment PI:C was linked to higher absolute proinsulin values (median: 5.59 vs 1.90 pmol/l; p<0.001). Those with high pre-treatment PI:C ratio values were at significantly greater risk of progressing to stage 3 diabetes (median: 19 months) than those with low pre-treatment PI:C ratios (median: 75 months), even after adjusting for age and baseline C-peptide AUC (HR 3.30; 95% CI 1.63, 6.68; p<0.001) (Fig. 1c, ESM Table 4).
Teplizumab treatment delays progression to stage 3 diabetes in individuals with high PI:C ratio
We determined whether the pre-treatment PI:C ratio affected the outcome of teplizumab treatment and the risk of progression to stage 3 type 1 diabetes (Fig. 2, ESM Table 5). When used as a continuous or dichotomous variable, a high pre-treatment PI:C ratio had a profound impact on the time to stage 3 type 1 diabetes, as did the treatment arm. To further evaluate the discriminative ability of baseline PI:C ratio as a prognostic factor for the time to progression to stage 3 diabetes, as shown in Table 1, we used time-dependent ROC and AUC analyses as well as C-indices, including treatment group, age and baseline PI:C ratio as either a continuous or a dichotomised measure. Overall, models incorporating baseline PI:C ratio performed better with higher AUC across time points (6 year AUC=80.8% for continuous PI:C and 80.5% for dichotomised PI:C compared with a 6 year AUC of 64.1% for the model with treatment arm and age only) and higher C-indices (C=0.71 for continuous PI:C and 0.72 for dichotomised PI:C compared with 0.63 for the model with treatment arm and age only).

Relationship between pre-treatment PI:C, type 1 diabetes progression and teplizumab treatment. The Kaplan–Meier curve shows rates of progression to stage 3 diabetes amongst participants from both the teplizumab and placebo treatment groups, stratified based on high vs low pre-treatment PI:C ratio (above or below 0.5). Cox regression stratified by pre-treatment ratio and treatment group showed that differences in stage 3 progression were only statistically significant for participants starting the trial with a high pre-treatment PI:C ratio (for high baseline PI:C ratio, p=0.002 for placebo vs teplizumab, while for low baseline PI:C ratio, p=0.1). The number at risk are shown for each group.T1D, type 1 diabetes
We further identified a significant interaction between treatment arm and pre-treatment PI:C ratio for the time to progression to type 1 diabetes (p=0.017 for treatment group as effect modifier). In a subset-stratified analysis (Fig. 2), teplizumab mitigated progression to stage 3 diabetes and the treatment effect was most pronounced in those with a high ratio at baseline (p=0.002) vs low ratio (p=0.1) (ESM Table 5).
Drug treatment did not consistently reduce PI:C values in participants with either high or low pre-treatment PI:C
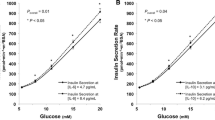
To better understand the potential mechanisms of this effect modification of teplizumab on the influence of high pre-treatment PI:C ratio on risk of stage 3 type 1 diabetes, we evaluated the study average PI:C ratio AUC, adjusted for age and the baseline value, and how this differed between treatment arms. The study average PI:C ratio AUC did not differ significantly between treatment arms (p=0.36) (Fig. 3a,b). We performed an exploratory analysis across all of the time points to determine whether there may be transient differences in the response to drug treatment (ESM Table 6, ESM Fig. 2). This analysis did not identify a consistent impact of treatment on PI:C, with only a transient suggested difference in the values at month 12 (a greater decline in the teplizumab group). This change was seen only in those with high, but not low, pre-treatment PI:C (ESM Table 6).

Average study PI:C ratio AUC values were not different between treatment groups. Average study PI:C ratio AUC values corrected for time in the study were calculated and adjusted for pre-treatment PI:C ratio and age. (a) Average study PI:C ratio AUC by treatment arm. Placebo group, n=21 (missing data for n=1 in placebo group); teplizumab group, n=41. (b) Average study PI:C ratio AUC by treatment arm and progression to stage 3 type 1 diabetes. In total, n=23 of n=41 participants in the teplizumab arm and n=17 of n=21 participants in the placebo arm developed stage 3 type 1 diabetes. One participant in the placebo group developed stage 3 type 1 diabetes before the first follow-up sample and so was not included in this analysis. The whiskers reflect roughly a 95% CI for the median (thick horizontal line), while the top and the bottom of the box are the 1st and 3rd quartiles (25th and 75th percentiles). No significant differences were present for any comparisons. T1D, type 1 diabetes
Relationships between HLA, changes in immune cells with teplizumab and PI:C ratios
In the original study, we found that individuals who were HLA-DR4+ or HLA-DR3− had more robust responses to teplizumab than those who were DR4− or DR3+ [13]. Therefore, we evaluated the influence of HLA-DR3 and HLA-DR4 status in the multivariable models to assess whether PI:C ratio is still influential with the inclusion of these variables. In the model using continuous pre-treatment PI:C ratio (log2 transformed), the PI:C ratio maintained its significance while inclusion of DR3 and/or DR4 status did not affect the findings (data not shown).
There may have been immune cell differences amongst those with high and low pre-treatment PI:C that could account for the effects of teplizumab in the high-PI:C group. At 3 and 6 months, teplizumab has been shown to increase levels of partially exhausted CD8+ T cells, defined by expression of eomesodermin (EOMES), and co-expression of killer cell lectin-like receptor G1 (KLRG1) and T cell immunoreceptor with immunoglobulin and immunoreceptor tyrosine-based inhibitory motif domain (TIGIT) [13]. When the groups, defined by teplizumab vs placebo administration and PI:C ratio, were compared using a mixed model, there was an effect of drug treatment on CD8+CD45RO+CC-motif chemokine receptor 7 (CCR7)+EOMES+ and CD8+CCR7+KLRG1+TIGIT+ T cells (p=0.002 and p=0.0595, respectively), but we did not identify a significant effect of the PI:C ratio on the frequency of these cells or an interaction between drug treatment and either of the T cell subsets (ESM Fig. 3).
Discussion
We found that in participants with stage 2 type 1 diabetes, progression to stage 3 disease was more rapid in those with high (≥0.5%) vs low (<0.5%) PI:C ratios. Teplizumab treatment was most effective in attenuating stage 3 progression in those with high pre-treatment ratios. Here, placebo-treated individuals with high pre-treatment PI:C exhibited rapid development of stage 3 type 1 diabetes, while this relationship was much less pronounced in those receiving teplizumab treatment. The differences in the responses to teplizumab treatment that we found between the individuals with high and low PI:C ratios could not be explained by a differential effect on immune cells. In aggregate, these data suggest that the drug activity may be greatest in the group identified with this biomarker of aggressive disease and that the differential response to teplizumab is due to differences in active beta cell stress rather than differences in the response of immune cells to treatment.
Our observation that teplizumab’s effectiveness was best when there was active islet stress is consistent with preclinical studies of anti-CD3 in non-obese mouse models of diabetes, human studies in recent-onset vs longer duration type 1 diabetes, and the TN10 trial, in which we found that the improvement with treatment was greatest in those in the lower half of C-peptide AUC at entry [13, 19, 20]. Of note, high pre-treatment PI:C was strongly predictive of diabetes progression even with adjustment for pre-treatment C-peptide AUC, suggesting that our findings do not reflect impacts of C-peptide alone. Consistent with prior reports [8, 17], age was an important determinant of the PI:C ratio in this stage 2 population. However, although our sample size was insufficient to analyse the effects between age categories, age in isolation did not significantly impact treatment response [13] and the analyses here were adjusted for age.
Our exploratory analysis did not find consistent drug effects on the PI:C ratio in the overall study population over time. Moreover, there was variability in the PI:C response between individuals as well as heterogeneity in the clinical responses to teplizumab. It is possible that, in the context of stage 2 type 1 diabetes, elevated PI:C ratios may not reflect acute measures of beta cell stressors (such as clinical measures like C-reactive protein) but rather reflect enduring damage to beta cells that is not immediately reversible with immunotherapy and may lead to lasting dysfunction, especially in the context of increasing insulin secretion. In this regard, the anti-TNF mAb golimumab that attenuated beta cell decline in stage 3 type 1 diabetes did not reduce PI:C ratios, but rather prevented the increase that occurred in placebo-treated participants [21]. Therefore, it remains to be established whether a reduction in the PI:C ratio can be used as a marker of improved beta cell stress with interventions that modulate type 1 diabetes progression, particularly those that directly target beta cell health.
The current analysis is the first to examine PI:C values specifically in a group of individuals with stage 2 type 1 diabetes. Our findings suggest that elevations in PI:C are strongly associated with progression to diabetes in individuals of all ages meeting stage 2 criteria. Thus, PI:C could provide useful information to counsel at-risk individuals considering immunotherapies on the expected rate of development of stage 3 type 1 diabetes. Consistent with previously reported increases in proinsulin area in islets from autoantibody-positive individuals [12], in individuals with stage 2 disease from this study, a high PI:C ratio was linked to increases in absolute proinsulin rather than decreased C-peptide values. In contrast, elevations of PI:C at the time of type 1 diabetes diagnosis are more strongly linked to reductions in C-peptide [22]. One explanation for this interesting finding could be that at earlier stages on the spectrum of type 1 diabetes development, increases in PI:C ratio are more a reflection of intrinsic beta cell stress due to autoimmune attack, and less determined by impacts of chronic hyperglycaemia and secretory granule depletion. In this regard, the ratio may better define the risk for progression in general, but also the ‘window’ of treatment opportunity with the drug, i.e. those with the highest ratio showed the greatest drug effect.
There are limitations to this exploratory analysis. The original trial was not powered to formally address this post hoc analysis. Therefore, there may be significant differences that are not identified because of the small sample size. As an example, the treatment curves in the individuals with low PI:C ratio do ultimately diverge but the differences in rates of progression may not have achieved statistical significance. Thus, rather than true treatment ‘responders’, high PI:C may identify a window for a more immediate and clear benefit of drug treatment. We were missing data from five of the original trial participants, but we addressed this limitation using imputation and the results remained remarkably consistent. For example, a multivariable model for continuous pre-treatment PI:C ratio (log2 transformed) in the analysis for time to stage 3 type 1 diabetes has a corresponding HR of 2.53 and a p value of 0.00037 when missing individuals are excluded vs 2.47 and a p value of 0.0003 when they are included (both models adjusting for baseline mean C-peptide AUC, treatment arm and age). Because of sample availability, pre-treatment PI:C values were randomly timed; however, for participants with fasting and random pre-treatment PI:C, these values were highly correlated. Our designation of low and high baseline ratios corresponded to an approximation of the mean pre-treatment levels and was validated with recursive partitioning, but, with a larger sample size, a more conventional approach to division could be utilised. Longitudinal metabolic data were impacted by study participant dropout from OGTT testing due to type 1 diabetes. This disproportionately impacted the placebo group, likely resulting in a progressively increasing bias towards more metabolically ‘normal’ PI:C values in the placebo group over time. We found variability in the measurements of the PI:C ratio, which may reflect true biological variance, but the timing of the sampling may also have contributed to this observation. Finally, our analyses of changes in immune cells and the PI:C ratio are correlative, and we do not have direct evidence linking T cell frequencies and beta cell stress. Despite these limitations, given the unique nature and value of this dataset in type 1 diabetes prevention, these results provide valuable hypothesis-generating data to be prospectively tested as part of future prevention efforts with disease-modifying therapies.
Our findings have important implications for diabetes prediction as well as diabetes prevention. For individuals with stage 2 type 1 diabetes, an elevated PI:C is highly indicative of impending progression to stage 3. Drug treatment delays the progression, and our data would suggest that teplizumab is most effective if individuals have high PI:C ratios. Thus, the PI:C ratio may be used as a biomarker to optimise selection of study participants or timing of dosing for type 1 diabetes prevention trials.
Abbreviations
- CCR7:
-
CC-motif chemokine receptor 7
- EOMES:
-
Eomesodermin
- KLRG1:
-
Killer cell lectin-like receptor G1
- mAb:
-
Monoclonal antibody
- PI:C:
-
Proinsulin:C-peptide
- ROC:
-
Receiver operating characteristic
- TIGIT:
-
T cell immunoreceptor with immunoglobulin and immunoreceptor tyrosine-based inhibitory motif domain
References
DiMeglio LA, Evans-Molina C, Oram RA (2018) Type 1 diabetes. Lancet 391:2449–2462. https://doi.org/10.1016/S0140-6736(18)31320-5
Sims EK, Mirmira RG, Evans-Molina C (2020) The role of beta-cell dysfunction in early type 1 diabetes. Curr Opin Endocrinol Diabetes Obes 27:215–224. https://doi.org/10.1097/MED.0000000000000548
Fonseca SG, Gromada J, Urano F (2011) Endoplasmic reticulum stress and pancreatic β-cell death. Trends Endocrinol Metab 22:266–274. https://doi.org/10.1016/j.tem.2011.02.008
Brozzi F, Nardelli TR, Lopes M et al (2015) Cytokines induce endoplasmic reticulum stress in human, rat and mouse beta cells via different mechanisms. Diabetologia 58:2307–2316. https://doi.org/10.1007/s00125-015-3669-6
Toren E, Burnette KS, Banerjee RR, Hunter CS, Tse HM (2021) Partners in crime: beta-cells and autoimmune responses complicit in type 1 diabetes pathogenesis. Front Immunol 12:756548. https://doi.org/10.3389/fimmu.2021.756548
Mezza T, Ferraro PM, Sun VA et al (2018) Increased β-cell workload modulates proinsulin-to-insulin ratio in humans. Diabetes 67:2389–2396. https://doi.org/10.2337/db18-0279
Rodriguez-Calvo T, Chen YC, Verchere CB et al (2021) Altered β-cell prohormone processing and secretion in type 1 diabetes. Diabetes 70(5):1038–1050. https://doi.org/10.2337/dbi20-0034
Sims EK, Chaudhry Z, Watkins R et al (2016) Elevations in the fasting serum proinsulin-to-c-peptide ratio precede the onset of type 1 diabetes. Diabetes Care 39:1519–1526. https://doi.org/10.2337/dc15-2849
Van Dalem A, Demeester S, Balti EV et al (2016) Prediction of impending type 1 diabetes through automated dual-label measurement of proinsulin:C-peptide ratio. PLoS One 11:e0166702. https://doi.org/10.1371/journal.pone.0166702
Tersey SA, Nishiki Y, Templin AT et al (2012) Islet β-cell endoplasmic reticulum stress precedes the onset of type 1 diabetes in the nonobese diabetic mouse model. Diabetes 61:818–827. https://doi.org/10.2337/db11-1293
Sims EK, Syed F, Nyalwidhe J et al (2019) Abnormalities in proinsulin processing in islets from individuals with longstanding T1D. Transl Res 213:90–99. https://doi.org/10.1016/j.trsl.2019.08.001
Rodriguez-Calvo T, Zapardiel-Gonzalo J, Amirian N et al (2017) Increase in pancreatic proinsulin and preservation of β-cell mass in autoantibody-positive donors prior to type 1 diabetes onset. Diabetes 66(5):1334–1345. https://doi.org/10.2337/db16-1343
Herold KC, Bundy BN, Long SA et al (2019) An anti-CD3 antibody, teplizumab, in relatives at risk for type 1 diabetes. N Engl J Med 381:603–613. https://doi.org/10.1056/NEJMoa1902226
Sims EK, Cuthbertson D, Herold KC, Sosenko JM (2021) The deterrence of rapid metabolic decline within 3 months after teplizumab treatment in individuals at high risk for type 1 diabetes. Diabetes 70(12):2922–2931. https://doi.org/10.2337/db21-0519
Sims EK, Geyer S, Johnson SB et al (2019) Who is enrolling? The path to monitoring in type 1 diabetes TrialNet’s Pathway to Prevention. Diabetes Care 42:2228–2236. https://doi.org/10.2337/dc19-0593
Sims EK, Bundy BN, Stier K et al (2021) Teplizumab improves and stabilizes beta cell function in antibody-positive high-risk individuals. Sci Transl Med 13(583):eabc8980. https://doi.org/10.1126/scitranslmed.abc8980
Leete P, Oram RA, McDonald TJ et al (2020) Studies of insulin and proinsulin in pancreas and serum support the existence of aetiopathological endotypes of type 1 diabetes associated with age at diagnosis. Diabetologia 63:1258–1267. https://doi.org/10.1007/s00125-020-05115-6
Long SA, Thorpe J, Herold KC et al (2017) Remodeling T cell compartments during anti-CD3 immunotherapy of type 1 diabetes. Cell Immunol 319:3–9. https://doi.org/10.1016/j.cellimm.2017.07.007
Chatenoud L, Primo J, Bach JF (1997) CD3 antibody-induced dominant self tolerance in overtly diabetic NOD mice. J Immunol 158:2947–2954. https://doi.org/10.4049/jimmunol.158.6.2947
Hagopian W, Ferry RJ Jr, Sherry N et al (2013) Teplizumab preserves C-peptide in recent-onset type 1 diabetes: two-year results from the randomized, placebo-controlled Protege trial. Diabetes 62:3901–3908. https://doi.org/10.2337/db13-0236
Quattrin T, Haller MJ, Steck AK et al (2020) Golimumab and beta-cell function in youth with new-onset type 1 diabetes. N Engl J Med 383:2007–2017. https://doi.org/10.1056/NEJMoa2006136
Watkins RA, Evans-Molina C, Terrell JK et al (2016) Proinsulin and heat shock protein 90 as biomarkers of beta-cell stress in the early period after onset of type 1 diabetes. Transl Res 168:96–106. https://doi.org/10.1016/j.trsl.2015.08.010
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Data availability
Data are available upon reasonable request to the authors or via submission request via http://www.trialnet.org.
Funding
The Type 1 Diabetes TrialNet Study Group is a clinical trials network funded by the National Institutes of Health (NIH) through the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), the National Institute of Allergy and Infectious Diseases, and the Eunice Kennedy Shriver National Institute of Child Health and Human Development, through cooperative agreements U01 DK061010, U01 DK061034, U01 DK061042, U01 DK061058, U01 DK085465, U01 DK085453, U01 DK085461, U01 DK085466, U01 DK085499, U01 DK085504, U01 DK085509, U01 DK103180, U01 DK103153, U01 DK085476, U01 DK103266, U01 DK103282, U01 DK106984, U01 DK106994, U01 DK107013, U01 DK107014, UC4 DK097835, and UC4 DK106993, and JDRF. EKS receives support from NIH grants R01DK121929, R01DK133881 and U01DK127382-012. EKS was also supported by the Doris Duke Charitable Foundation (grant 2021258) through the COVID-19 Fund to Retain Clinical Scientists collaborative grant programme, and by the John Templeton Foundation (grant 62288). The studies were supported by R01 DK057846 and R01 DK129523 from the NIH, and SRA-2019-833-S-B from JDRF (to KCH). This work utilised core services provided by the Diabetes Research Center grant P30 DK097512 (to Indiana University School of Medicine).
Authors’ relationships and activities
EKS has received compensation for educational lectures on diabetes screening from Medscape and Health Matters CME. KCH has consulted for Provention Bio and is a co-inventor on a patent application for use of teplizumab for delay of stage 3 type 1 diabetes but without financial remuneration. All other authors declare that there are no relationships or activities that might bias, or be perceived to bias, their work.
Contribution statement
EKS, SMG and KCH conceived the project, analysed data, obtained funding, and wrote and edited the manuscript. SAL analysed data and edited the manuscript. All authors approved the final version of the manuscript. KCH is responsible for the integrity of the work as a whole.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Sims, E.K., Geyer, S.M., Long, S.A. et al. High proinsulin:C-peptide ratio identifies individuals with stage 2 type 1 diabetes at high risk for progression to clinical diagnosis and responses to teplizumab treatment. Diabetologia 66, 2283–2291 (2023). https://doi.org/10.1007/s00125-023-06003-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-023-06003-5