
Abstract
The incidence of syphilis has been increasing in the USA since 2000. Notably, the coronavirus disease 2019 pandemic negatively impacted the public health efforts to contain the spread of sexually transmitted diseases including syphilis and congenital syphilis. Clinical manifestations of syphilis are predominantly mucocutaneous lesions, thus dermatologists are primed to recognize the myriad presentations of this disease. Primary syphilis is classically characterized by a painless transient chancre most often located in the genital area. Secondary syphilis typically manifests clinically as systemic symptoms in addition to a mucocutaneous eruption of which a variety of forms exist. Although less common in the era of effective penicillin treatment, late clinical manifestations of syphilis are described as well. In addition to recognition of syphilis on physical examination, several diagnostic tools may be used to confirm infection. Treponema pallidum spirochetes may be detected directly using histopathologic staining, darkfield microscopy, direct fluorescent antibody, and polymerase chain reaction assays. A table detailing the histopathologic features of syphilis is included in this article. Serologic testing, non-treponemal and treponemal tests, is the preferred method for screening and diagnosing syphilis infections. Two serologic testing algorithms exist to aid clinicians in diagnosing positive syphilis infection. Determining the correct stage of syphilis infection combines results of serologic tests, patient history, and physical examination findings. Using the current Centers for Disease Control and Prevention case definitions and treatment guidelines, a management algorithm is proposed here. Penicillin remains the pharmacological treatment of choice although specific clinical situations allow for alternative therapies. Syphilis is a reportable disease in every state and should be reported by stage according to individual state requirements. Screening recommendations are largely based upon risks encountered through sexual exposures. Likewise, sexual partner management includes evaluating and treating persons exposed to someone diagnosed with an infective stage of syphilis. Close clinical follow-up and repeat testing are recommended to ensure appropriate response to treatment. This guide will discuss the current epidemiology of syphilis and focus on practice aspects of diagnosis and management, including public health reporting.
Similar content being viewed by others


The incidence of syphilis infection is increasing in the USA. |
Dermatologists play an important role in the recognition and management of syphilis. |
Penicillin remains the gold standard treatment. |
Public health staging and reporting are necessary for addressing the rise in cases. |
1 Introduction
Infection by the spirochete bacteria Treponema pallidum subspecies pallidum is the cause of syphilis. Since 2000, the incidence of syphilis has been increasing [1]. Although the coronavirus disease 2019 (COVID-19) pandemic disrupted public health efforts, reporting of syphilis, and interpretation of data collected in 2020 and 2021, preliminary data for 2021 show a continued increase in primary and secondary syphilis among adults as well as congenital syphilis [2]. Thus, timely recognition and appropriate management are of utmost importance in preventing and controlling this disease. The predominant mucocutaneous clinical manifestations of syphilis lend to the expertise of dermatologists who, historically, were early specialists in venereal diseases [3]. This paper serves as an updated and practical guide to the diagnosis and management of syphilis.
2 Epidemiology
Syphilis has a worldwide distribution, and its incidence is increasing substantially in the USA. In 2000, the US incidence of all cases reached a historic nadir of 11.2 cases per 100,000, a result of widespread use of penicillin for treatment beginning in the 1940s and 1950s and years of public health prevention and control efforts. Every year since 2000, the incidence rate of syphilis has increased in the USA. The COVID-19 pandemic introduced a tremendous challenge for the control and prevention of syphilis and will likely continue to impact trends for years to come. Statistics from the 2020 Centers for Disease Control and Prevention (CDC) case surveillance of primary and secondary (P&S) syphilis were complicated by shelter-in-place orders in March and April 2020 such that case counts dropped below 2019 levels during this time. Contributing factors to this change include reduced screening, limited public health resources, and fluctuating social-distancing measures. Yet, case counts rebounded and then surpassed 2019 percentages throughout the year. In 2020, the final number of reported cases of P&S syphilis, the infectious stages, was 41,655, a 6.8% increase from 2019. The incidence of reported cases of syphilis (all stages) for 2020 was 40.8 per 100,000, representing a 3.3% increase from 2019 [1, 4, 5].
Diagnosed cases of P&S syphilis are highest among men, with a disproportionate number of cases among men who have sex with men (MSM). The majority of P&S syphilis cases from 2016 to 2020 were among MSM at 51.2%, with a small decrease of 2.2% from 2019 to 2020. A strong association between incident syphilis infections and an increased risk of HIV infection continues to be reflected in 2020 data where 45.9% of cases among MSM were HIV positive [6, 7]. Since 2015, however, the majority of the P&S cases among MSM have been in those who are HIV negative. In 2020, the incidence rates of P&S syphilis cases were highest among non-Hispanic Black or African American persons (34.1 per 100,000) and in the US Census West region (16.7 per 100,000; WA, OR, CA, NV, AZ, UT, ID, MT, WY, CO, NM, AK, and HI). An alarming increase in incident cases has been experienced by women in recent years. From 2016 to 2020, the rate of P&S syphilis infections among women increased by 147.4% (from 1.9 to 4.7% per 100,000). This dramatic increase in incidence among women is focused within those aged 15–44 years, leading to a parallel increase in congenital syphilis cases because the early stages of syphilis carry the highest risk of transmission to the fetus. Indeed, the incidence rate of congenital syphilis has increased by 500.0% from 2011 to 2020 [1].
3 Clinical Manifestations
3.1 Background
Primary and secondary syphilis are periods defined by protean clinical manifestations that last for several months [8]. Transmission to others occurs through direct contact with the lesions of primary syphilis (chancres), or the mucocutaneous lesions of secondary syphilis (“syphilids”). Public health efforts focus on identifying and treating disease during these stages because they are infectious and the clinical manifestations, while varied, are more readily apparent. This contrasts with the non-infectious latent stages where the clinical manifestations take years to develop and are more systemically devastating to the patient. Adults acquire syphilis most commonly through sexual transmission during the infectious primary and secondary stages, while congenital syphilis (infection of the fetus in utero) may be transmitted to the fetus at any stage, even latent [9].
3.2 CDC Case Definitions
The most up-to-date CDC staging nomenclature was published in 2018 [10]. Classification guides management, including treatment decisions and partner notification systems. Primary syphilis is defined by the presence of one or more ulcerative lesions (chancres) at the inoculation site days to weeks following exposure. Secondary syphilis is defined by polymorphic mucocutaneous lesions most often accompanied by generalized lymphadenopathy (among other clinical manifestations) presenting concurrently or weeks following the primary chancre. Early non-primary non-secondary syphilis is defined by serologic confirmation of infection without signs or symptoms of primary or secondary syphilis acquired within the past 12 months. Latent syphilis is defined by serologic confirmation of infection without signs or symptoms of primary or secondary syphilis acquired greater than 12 months prior; it may be further differentiated as “late” or of “unknown duration”. Late clinical manifestations, neurologic or otherwise, may be present for months or years following initial infection [10].
3.3 Primary Syphilis
Chancres are the hallmark manifestation of primary syphilis. These lesions are classically ulcerative, indurated, and painless with raised borders (Fig. 1). The ulcers are clean based, may be pink, red, or grayish, and range in size from 0.5 to 3 cm [11]. Chancres form at the site of inoculation 3–90 days (average 3 weeks) following exposure and will heal without scarring in 3–6 weeks if the infection is untreated [8, 9, 12]. Single or multiple lesions may occur and are most commonly found in the genital area; however, chancres are not limited to this location as inoculation can occur at any exposed site [8]. Extragenital chancres may be found on the mucosal or keratinized surfaces of the mouth or anogenital area, nipples, and fingers, and are more likely to have an atypical appearance [8, 11, 13,14,15,16,17]. Up to 80% of patients will have accompanying painless regional lymphadenopathy, particularly if the chancre is located in the genital area [8, 14, 18, 19].

Primary syphilis (chancre) of the urethral meatus
Genital ulcers prompt a broad differential diagnosis, but certain features are sensitive and/or specific to syphilitic chancres. A painless ulcerated lesion with a clean base is a combination of features that has a sensitivity of 31% and specificity of 98% [19]. A lack of purulence (involving less than 30% of the base) has been reported to be the single most sensitive finding [19]. The single most specific sign is induration of the ulcer, occurring in 47–92% of patients [18, 19]. Despite these distinguishing features, the presentation of chancres is variable and other causes of genital ulcers should be ruled out.
3.4 Secondary Syphilis
Clinical manifestations of secondary syphilis are caused by hematogenous and lymphatic dissemination of spirochetes. Although distinctive signs and symptoms exist, secondary syphilis is infamously protean, presenting with a wide array of subtle signs and symptoms that mimic other diseases [20].
Secondary syphilis is characterized by localized or diffuse mucocutaneous lesions often accompanied by generalized lymphadenopathy [10, 14, 20, 21]. Common regions of lymphadenopathy are suboccipital, cervical, postauricular, epitrochlear, and inguinal; nodes are discrete, rubbery, and typically non-tender and non-suppurative [20, 21]. Clinical manifestations typically present 3–12 weeks following resolution of the primary chancre, as many as one-third of patients with secondary syphilis have a concurrent chancre [12, 14, 20]. Other less common systemic signs include malaise, a sore throat, myalgias, weight loss, and low-grade fevers [8, 12, 14, 20]. Untreated secondary syphilis manifestations take weeks to months to resolve [9].
The mucocutaneous manifestations of syphilis, other than the chancre of primary syphilis, are termed “syphilids”. Distribution and character of syphilids vary. Syphilids have a generalized and symmetric distribution although localization to the palms and soles or genitals is common [20]. Pruritus may or may not be present [8, 20].
A mucocutaneous eruption is the most common syphilid of secondary syphilis. It classically presents in a diffuse and symmetric pattern involving the trunk and extremities, including the palms and soles, with discrete 0.5–2 cm macules or papules that are red-brown (“copper-colored” or “ham-colored”) and scaly (Figs. 2 and 3). Consistent with “the Great Imitator” moniker of syphilis, the mucocutaneous eruption of secondary syphilis frequently deviates from this classic morphology. Psoriasiform, follicular, pustular, lichenoid, nodular, or annular morphologies have all been reported [8, 11]. Furthermore, the mucocutaneous eruption may be inconspicuous and thus overlooked by patients and physicians alike [8].

Secondary syphilis of the plantar surface

Secondary syphilis of the palmar surfaces
Mucous patches and condyloma lata are two syphilids that are highly infectious. Mucous patches are primarily found on the tongue, buccal mucosa, and lips; several subtypes exist. One subtype is characterized by well-defined, slightly elevated oval plaques (at times ulcerated) with an overlying gray or white pseudomembrane. Multiple mucous patches may also coalesce, forming serpiginous “snail track ulcers.” A final common subtype is “leukoplakia-like” mucous patches that have a verrucous surface [22]. Specifically, on the dorsum of the tongue, erythema, grooves, fissures, or patches of depapillation may occur. A painful, unilateral, and fissured papule of the labial commissure, “false cheilitis,” may be misdiagnosed as angular cheilitis; however, these “split papules” are associated with additional oral lesions and submandibular lymphadenopathies, thus suggestive of secondary syphilis [23]. As expected, atypical oral presentations of secondary syphilis are not uncommon, and a high index of suspicion is warranted [22].
Condyloma lata are papules or nodules found in moist warm areas of skin apposition (anogenital area, medial thighs, inframammary creases, periumbilical area, and pedal interdigital spaces), and multiple areas may be affected at once (Fig. 4) [11, 24,25,26]. Condyloma lata also commonly exist adjacent to the location of the primary chancre likely due to the direct spread of treponemes [8]. The surface may be covered with an exudate, smooth, hypertrophic, or verrucous, and lesions may be painful [11, 27]. Because of similar morphology, condyloma acuminata and carcinoma are included in the differential diagnosis [28]. The unique histopathology of syphilis stages can be found in Table 1 [29,30,31,32,33,34,35].

Condyloma lata of the anus
Alopecia is an uncommon manifestation of secondary syphilis, occurring in less than 10% of patients. Alopecia syphilitica (AS) is nonscarring with non-inflammatory hair loss, and hair regrowth will be achieved following 5–12 weeks of treatment. Alopecia syphilitica may be accompanied by syphilitic lesions on the scalp (symptomatic AS) or alone (essential AS). Subclassifications of essential AS are moth-eaten, diffuse, or mixed pattern, with the moth-eaten pattern being the most common manifestation. Moth-eaten AS presents as a patchy pattern of alopecic areas throughout the scalp and mimics other causes of alopecia, including alopecia areata, tinea capitis, and trichotillomania [36]. The diffuse subtype may mimic telogen effluvium. Alopecia syphilitica is usually accompanied by other secondary syphilis manifestations, but in some cases may be the only clinical sign of disease [37].
Lues maligna, also called malignant or ulceronodular syphilis, is a rare and aggressive manifestation of secondary syphilis that is found most often in immunocompromised individuals, such as those with HIV [38]. Lesions of lues maligna are oval, ulcerative, or necrotic papules and plaques with a thick scale or crust that mainly affects the trunk and extremities. Lesions on the face, scalp, palms, soles, and mucous membranes may also occur. Lues maligna is associated with high treponemal titers, systemic symptoms, and severe Jarisch–Herxheimer reaction. Associated comorbidities include HIV infection, diabetes mellitus, alcoholism, drug abuse, psoriasis, and hepatitis [39]. Other notable dermatologic manifestations of secondary syphilis can be observed in the nails (onycholysis, onychomadesis, brittleness, splitting, paronychia) and through pigmentation changes (“leucoderma syphiliticum,” scattered hypomelanotic macules at sites of previous inflammation or within an area of hyperpigmentation on the neck) [11, 40].
3.5 Early Non-primary Non-secondary
The diagnosis of early non-primary non-secondary syphilis is made through positive serologic studies combined with an absence of signs or symptoms of primary or secondary syphilis and evidence that initial infection was acquired within the past 12 months [10]. Previously referred to as “early latent” syphilis, this stage is still considered infectious because of the 25% risk of relapse to secondary syphilis, most often occurring within the first year [41].
3.6 Unknown Duration or Late Syphilis
The stage classified as late syphilis or unknown duration differs from early non-primary non-secondary syphilis through evidence that infection occurred > 12 months previously or a lack of evidence to support infection occurred < 12 months previously, respectively. This stage of infection is supported by positive serologic studies and clinical evidence of late manifestations and/or neurologic syphilis; as before, signs and symptoms of primary or secondary syphilis are absent.
Late clinical manifestations are likely to present in this stage as these inflammatory processes take years to develop. “Tertiary syphilis” is no longer considered a stage with the updated classification system. Research on the natural history of untreated syphilis estimates that one-third of patients will develop late manifestations, including cardiovascular syphilis, late benign syphilis (“gummatous syphilis,” involving the skin, mucous membranes, bones, and joints), and neurosyphilis [41]. Cardiovascular and late benign syphilis are rare in the modern era of antibiotics, while neurosyphilis is still prevalent. Although included as one of several probable criteria in the revised case definition of unknown duration of late syphilis, neurologic syphilis (including otic and ocular syphilis) may occur at any stage of infection.
Cardiovascular syphilis predominantly affects the heart and great vessels. It may present as an aneurysm of the ascending aorta, aortic valve insufficiency, aortitis, myocarditis, and coronary vessel disease [9, 42].
Late benign syphilis is perhaps most closely associated with lesions of the skin, but virtually any tissue may be affected. Lesions of the skin may be of two forms: gummatous or noduloulcerative. Arising from a reactive granulomatous process, gummatous lesions of the skin are painless and rubbery nodules that are usually grouped and few in number. Gummas typically perforate the skin, leaving a distinctive punched-out ulcer from which necrotic material drains. Large lesions are destructive, heal with retracted and hyperpigmented scars, and may invade deeper tissues or arise from another tissue entirely. The noduloulcerative form appears as indurated and elevated papules or nodules that are red-brown in color. They expand to form serpiginous or arciform plaques, often healing centrally and occasionally eroding or ulcerating with thick crusts [43].
3.7 Neurosyphilis, Ocular Syphilis, and Otic Syphilis
Infection of the nervous system by T. pallidum results in neurosyphilis, ocular syphilis, or otic syphilis. Each is considered a separate disease state but may occur concomitantly. Within days of the primary infection, treponemes invade the nervous system, thus neurologic involvement may occur at any stage of infection.
3.8 Late Benign (Tertiary) Syphilis
Early tertiary lesions may lack granulomata. Nodular lesions will show granulomatous inflammation (multinucleated giant cells, lymphocytes, plasma cells, and scattered epithelioid cells), inconspicuous necrosis, and possible endothelial swelling of vessels; at times, nodular lesions will lack granulomata. Gummatous lesions will also show granulomatous inflammation in addition to foci of acellular necrosis, and endarteritis obliterans of the dermal and subcutaneous vessels [29].
3.9 Congenital Syphilis
Clinical signs of congenital syphilis appear within the first 4–8 weeks of life. Cutaneous manifestations of early congenital syphilis include persistent rhinitis (“snuffles”), a vesiculobullous or maculopapular rash, and generalized nontender lymphadenopathy [44]. Condylomata, mucous patches, and fissures may also be observed at mucous membrane sites similar to cutaneous lesions found in infected adults [45].
4 Diagnosis
4.1 Direct Detection
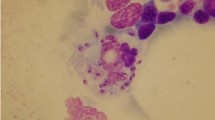
For the diagnosis of primary or secondary syphilis, direct detection of T. pallidum spirochetes from lesion exudate or within a tissue is preferred and confirmatory, but not available in all clinical settings. Direct detection is especially useful during primary syphilis when serologies may not be reactive yet. Options for direct detection include histopathologic staining (silver stains or immunohistochemistry), darkfield microscopy, direct fluorescent antibody, and polymerase chain reaction assays. Neither darkfield microscopy nor polymerase chain reaction assays are widely available in the USA. Classically, histological identification of spirochetes has been performed using silver-impregnation staining techniques such as Warthin–Starry and Levaditi stains. Artifactual staining of background tissue elements, however, may lead to false-negative or false-positive results. A study comparing Warthin–Starry staining and immunohistochemical analysis using specific polyclonal antibodies to T pallidum found that immunohistochemistry showed a higher diagnostic sensitivity in the identification of spirochetes in biopsy specimens from primary and secondary syphilis mucocutaneous lesions [33].
4.2 Serologic Testing
Serological testing, non-treponemal and treponemal tests, is the preferred approach for screening, diagnosis, and following treatment response of syphilis infections. A serologic test that detects antibodies is considered reactive, and those that do not detect antibodies are considered nonreactive.
4.2.1 Non-treponemal Tests
Non-treponemal tests detect antigens that are not unique to T. pallidum. Instead, they detect host-derived lipids (cardiolipin, lecithin, cholesterol) that were incorporated into the membrane of T. pallidum organisms. The rapid plasma reagin (RPR) and venereal disease research laboratory are non-treponemal tests that detect both IgG and IgM antibodies and the resulting titers correspond generally to the stage of the disease. Titers may be undetectable in very early syphilis, will rise during primary disease, peak within secondary or early latent disease, and may decline expectedly with treatment (become nonreactive, i.e., seroversion) or spontaneously without treatment [9, 46]. Changes in non-treponemal antibody titers may be used to assess response to therapy [47]; however, venereal disease research laboratory titers are typically lower than RPR titers and thus, cannot be compared directly [48].
An incomplete resolution of non-treponemal titers is referred to as a serofast state. This situation is more likely to occur in those with lower initial nontreponemal test titers, later stage of disease, and if older in age (> 40 years); notably, research has found that titers do not decline significantly further following additional treatment [49, 50].
False-positive RPR or venereal disease research laboratory tests may be found in the setting of anti-lipoidal antibody reactivity, including tissue damage from infectious diseases (hepatitis) or autoimmune diseases (rheumatoid arthritis, systemic lupus erythematosus, and older age) [46]. Other disorders that promote high circulating immunoglobulins may also cause false reactive nontreponemal tests, including pregnancy, chronic infections, and parenteral drug use [9]. The chance of a false-positive result from a non-treponemal test is the justification for following the “traditional” algorithm and confirming the non-treponemal test result with a more specific treponemal test.
False-negative nontreponemal tests will most often occur in early or late infections owing to insufficient amounts of antibodies for detection and with the prozone phenomenon where excessive antibodies interfere with test performance [51]. The prozone phenomenon is associated with primary and secondary syphilis stages, pregnancy, neurosyphilis, and a range of RPR titers [52]
4.2.2 Treponemal Tests
Treponemal tests detect antibodies to antigens specific to T. pallidum. In general, these tests are more sensitive than nontreponemal tests during early infection. Following the traditional algorithm, treponemal tests are not ordered unless a nontreponemal test is reactive; however, specifically requesting the more sensitive treponemal test may be warranted if suspicion of primary syphilis is high but an initial nontreponemal test was non-reactive. Prototypes include the fluorescent treponemal antibody adsorbed (FTA-ABS) and T. pallidum particle agglutination tests. Automatic high-throughput treponemal tests in the forms of chemiluminescence immunoassays and enzyme-linked immunoassays are becoming more widely used owing to their ease and lesser expense to perform; for these reasons, following a “reverse” algorithm—where a treponemal test is initially performed and a nontreponemal test is used to confirm if the first test was positive—has become more popular [51]. In contrast to the quantitative non-treponemal tests, the treponemal tests are considered qualitative. These tests often remain positive regardless of treatment and thus cannot differentiate between previous and current infections. For this reason, the reverse algorithm is most useful in low-prevalence areas where few people are or have been infected with syphilis and persisting antibodies are less likely to be detected [9]. Following the “reverse” algorithm may produce discordant results. For example, in the setting of a positive treponemal test followed by a negative nontreponemal test (the “reverse” algorithm), the CDC recommends performing a second unrelated treponemal test to confirm [53].
4.3 Other Diagnostic and Screening Considerations
Both screening algorithms are sanctioned by the CDC. When considering which algorithm to follow, it is important to know the strengths and weaknesses of serologic testing as discordant results complicate interpretation. When suspicion is high based on history and a physical examination, empiric treatment should be considered [54]. For appropriate interpretation of serologic test results, physicians should be aware of which algorithm their laboratory uses and whom they can contact regarding discordant cases.
Diagnosis of neurosyphilis is complex and includes serologic tests and CSF analysis. Complete details are covered in the 2021 CDC Sexually Transmitted Infections (STIs) Treatment Guidelines [53]. Patients with suspected neurosyphilis, ocular syphilis, or otic syphilis should be immediately referred to a specialist for further evaluation.
Rapid point-of-care tests are currently being developed and have the potential to increase testing, particularly in resource-limited areas, urgent care settings, and recently during the COVID-19 pandemic where decentralized self-testing was valuable. Early results for rapid tests are promising, and some tests may be combined to test for HIV as well [55, 56].
5 Management
5.1 General
Basic tenets of syphilis management include ordering appropriate serologic tests, determining the stage of infection, assessing for neurologic involvement then referring appropriately, and administering the appropriate antibiotic treatment. Serologic tests should be ordered for all patients regardless of stage. Non-treponemal testing establishes a baseline titer and, when repeated, enables evaluation of serologic response to treatment. A treponemal test is unnecessary if the patient has a history of syphilis with a reactive treponemal test. A complete clinical picture of the patient is paramount to appropriate staging. A detailed sexual and medical history, physical examination, and the patient’s serologic history (from the patient or the public health department) all inform the physician. Staging active disease (primary and secondary syphilis) may be more straightforward while staging latent disease introduces some complexity. In the setting of positive serologies and an absence of signs or symptoms of primary, secondary, and tertiary syphilis, serologies may represent a previously treated infection (successful or not) or a new infection (in which the duration of infection will determine the stage).
5.2 Treatment
Penicillin is still the treatment of choice for all syphilis stages. Benzathine penicillin G is the specifically recommended formulation owing to its long half-life. Several factors determine the duration of treatment and route of administration. Stage of infection, pregnancy status, presence of a penicillin allergy, and diagnosis of neurosyphilis, otic syphilis, and ocular syphilis are all necessary considerations. Notably, HIV status or a nontreponemal test titer do not affect the CDC treatment recommendations for all stages and for neurosyphilis, ocular, and otic syphilis. Alternative antibiotic therapies (tetracycline/doxycycline, ceftriaxone, or azithromycin) or non-preferred formulations of penicillin are appropriate in certain situations such as in the case of a penicillin allergy or if having difficulty with administering intravenously. It should be noted, however, that alternative antibiotics are never recommended for the treatment of pregnant women, those diagnosed with neurosyphilis (including ocular or otic), or those who are HIV positive; desensitization and administration of penicillin is always recommended in such cases. Empiric treatment should be considered when the index of suspicion is high based on clinical presentation and risk factors, especially when follow-up is uncertain [53].
A proposed staging and treatment algorithm based on current case definitions and guidelines can be found in Fig. 5 [10, 53, 57]. Further recommendations may be found in the 2021 CDC STI Treatment Guidelines [53].

Proposed management algorithm for the staging of treatment of syphilis using the Centers for Disease Control and Prevention (CDC) 2018 Case Definitions and the 2021 CDC Sexually Transmitted Infections Treatment Guidelines; adapted from Clement et al. 2014. a An alternative treatment for neurosyphilis is intramuscular (IM) benzathine penicillin G (BPG) plus probenecid for 10–14 days; this should be reserved for those in which compliance can be ensured. Upon completion of neurosyphilis treatment, the treatment regimen for latent or unknown duration syphilis stages may be added for extended treatment. b When administering 2.4 million U of BPG, 1.2 million U of BPG should be intramuscularly injected per side. aPG aqueous penicillin G, CSF cerebrospinal fluid, d days, IV intravenous
5.3 Jarisch–Herxheimer Reaction
Final management recommendations include counseling patients about possible treatment reactions and assessing clinical and serologic response following treatment. The Jarisch–Herxheimer reaction is a known reaction to syphilis treatment and patients should be counseled about its possible occurrence. Within 1 day of treatment, the typical presentation consists of fever, headache, myalgia, and possible rash exacerbation. This reaction is thought to be caused by an acute inflammatory response upon destruction of spirochetes. Higher nontreponemal test titers, a higher clinical burden of disease, early syphilis, and previous penicillin treatment are associated with more common and severe reactions [48, 58, 59]. In pregnant women, uterine contractions and premature labor may occur during this reaction, thus obstetricians should manage treatment and monitoring [60, 61]. Symptomatic relief can be provided by antipyretics and hydration although the reaction typically resolves within 24 h. Taking acetaminophen and antihistamines prior to penicillin treatment is not helpful in preventing the reaction.
5.4 Assessment of Clinical and Serologic Response to Treatment
Clinical and serologic responses to treatment are evaluated at follow-up visits. Patients should be advised to return for clinical care if there is a lack of improvement in symptoms within 2 weeks. For those uninfected with HIV, the CDC recommends a follow-up evaluation at 6, 12, and 24 months. For those infected with HIV, the CDC recommends more frequent follow-up evaluations, at 3, 6, 9, 12, and 24 months. A four-fold or greater decline in nontreponemal test titers indicates a successful serologic response to treatment. Despite successful treatment, titers may be stable or only decline a single dilution, referred to as a serofast state.
6 Prevention and Reporting
6.1 Reporting
Syphilis, like other STIs and HIV/AIDS, is a reportable disease in every state and should be reported according to the state and local statutory requirements. Reports of STI and HIV cases are confidential and typically are protected by statute or regulation. Providers, laboratories, or both can submit reports of syphilis cases. Providers/dermatologists should contact their state or local health department STI programs to familiarize themselves with the appropriate reporting requirements within their jurisdictions as they may differ between state and/or which STI is being reported. Syphilis cases should be reported by stage to the local or state health department as soon as possible.
When possible, healthcare providers should be consulted by public health professionals who are following up on a patient with a positive syphilis (or other STI) case. This consult serves to inform the provider of the purpose of the public health visit, verify the diagnosis, determine the treatments received, and determine the best approaches to patient follow-up.
Population-based prevention is enhanced with repeat testing following treatment of syphilis. Follow-up serological testing should be conducted for any person who has received a syphilis diagnosis. Additionally, follow-up testing for HIV is recommended [53].
6.2 Screening
Screening for syphilis is guided by risk factors, in particular those acquired by sexual activity. Detailed screening recommendations can be found in the CDC STI Treatment Guidelines, the US Preventive Services Task Force screening guidelines, and the most recent review of STI diagnosis and treatment guidelines authored by Tuddenham et al. [53, 62,63,64,65].
6.3 Management of Sex Partners
Evaluation and treatment of persons sexually exposed to a person diagnosed with syphilis is recommended under certain conditions, namely which stage of infection was present at exposure and if the exposure occurred within the relevant time frame where infectivity was possible. As sexual transmission of T. pallidum occurs through contact with mucocutaneous syphilitic lesions, exposure to a person diagnosed with primary, secondary, or early latent syphilis (the stages when these lesions are present) poses the greatest risk of transmission to sex partners.
7 Conclusions
The increasing prevalence of syphilis in the USA represents a resurgence of a preventable and treatable disease after decades of sustained reduction. The COVID-19 pandemic has negatively impacted public health efforts to contain the spread of sexually transmitted diseases including syphilis. Dermatologists play an important role in the recognition and management of syphilis. Timely diagnosis, appropriate management as well as public health interventions are key to controlling syphilis infection and its spread.
References
Centers for Disease Control and Prevention. Sexually transmitted disease surveillance 2020. Atlanta (GA): U.S. Department of Health and Human Services; 2021.
Centers for Disease Control and Prevention. Sexually transmitted disease surveillance: preliminary 2021 data. Atlanta (GA): U.S. Department of Health and Human Services; 2022.
Chu MB, Tarbox M. The role of syphilis in the establishment of the specialty of dermatology. JAMA Dermatol. 2013;149:426.
Wright SS, Kreisel KM, Hitt JC, Pagaoa MA, Weinstock HS, Thorpe PG. Impact of the COVID-19 pandemic on Centers for Disease Control and Prevention-funded sexually transmitted disease programs. Sex Transm Dis. 2022;49:e61–3.
Pagaoa M, Grey J, Torrone E, Kreisel K, Stenger M, Weinstock H. Trends in nationally notifiable sexually transmitted disease case reports during the US COVID-19 pandemic, January to December 2020. Sex Transm Dis. 2021;48:798–804.
Buchacz K, Klausner JD, Kerndt PR, Shouse RL, Onorato I, McElroy PD, et al. HIV incidence among men diagnosed with early syphilis in Atlanta, San Francisco, and Los Angeles, 2004 to 2005. J Acquir Immune Defic Syndr. 1988;2008(47):234–40.
Buchacz K, Patel P, Taylor M, Kerndt PR, Byers RH, Holmberg SD, et al. Syphilis increases HIV viral load and decreases CD4 cell counts in HIV-infected patients with new syphilis infections. AIDS. 2004;18:2075–9.
Holmes KK, editor. Sexually transmitted diseases. 4th ed. New York: McGraw-Hill; 2008.
Hook EW. Syphilis Lancet. 2017;389:1550–7.
Centers for Disease Control and Prevention. Syphilis (Treponema pallidum) 2018 case definition. 2018. https://ndc.services.cdc.gov/case-definitions/syphilis-2018/. Accessed 6 May 2022.
Forrestel AK, Kovarik CL, Katz KA. Sexually acquired syphilis: Historical aspects, microbiology, epidemiology, and clinical manifestations. J Am Acad Dermatol. 2020;82:1–14.
Singh AE, Romanowski B. Syphilis: review with emphasis on clinical, epidemiologic, and some biologic features. Clin Microbiol Rev. 1999;12:187–209.
Tucker HA, Mulherin JL. Extragenital chancres; a survey of 219 cases. Am J Syph Gonorrhea Vener Dis. 1948;32:345–64.
Mindel A, Tovey SJ, Timmins DJ, Williams P. Primary and secondary syphilis, 20 years’ experience. 2. Clinical features. Genitourin Med. 1989;65:1–3.
Oh Y, Ahn SY, Hong SP, Bak H, Ahn SK. A case of extragenital chancre on a nipple from a human bite during sexual intercourse. Int J Dermatol Int J Dermatol. 2008;47:978–80.
Sim JH, Lee MG, In SL, Park BC, Kang HY, Lee E-S, et al. Erythematous erosive patch on the left nipple—quiz case. Diagnosis: extragenital syphilitic chancres. Arch Dermatol. 2010;146:81–6.
Ramoni S, Riva D, Spigariolo CB, Cusini M. Primary syphilis of the finger: report of four cases. Int J STD AIDS. 2022;33:728–30.
Chapel TA. The variability of syphilitic chancres. Sex Transm Dis Sex Transm Dis. 1978;5:68–70.
Dicarlo RP, Martin DH. The clinical diagnosis of genital ulcer disease in men. Clin Infect Dis. 1997;25:292–8.
Chapel TA. The signs and symptoms of secondary syphilis. Sex Transm Dis. 1980;7:161–4.
Mullooly C, Higgins SP. Secondary syphilis: the classical triad of skin rash, mucosal ulceration and lymphadenopathy. Int J STD AIDS. 2010;21:537–45.
de Paulo LFB, Servato JPS, Oliveira MTF, Durighetto AF, Zanetta-Barbosa D. Oral manifestations of secondary syphilis. Int J Infect Dis. 2015;35:40–2.
Gilligan G, Leonardi N, Garola F, Sanfedele A, Beltramo A, Piemonte E. False cheilitis (fausse cheilitis) as a clinical manifestation of oral secondary syphilis. Int J Dermatol. 2022;61:180–3.
Kim JS, Kang MS, Sagong C, Ko JY, Yu HJ. An unusual extensive secondary syphilis: condyloma lata on the umbilicus and perineum and mucous patches on the lips. Clin Exp Dermatol. 2009;34:299–301.
Rosen T, Hwong H. Pedal interdigital condylomata lata: a rare sign of secondary syphilis. Sex Transm Dis Sex Transm Dis. 2001;28:184–6.
Hua H, Zhu X, Yang L, Li M, Jiang P, Haikang HC. Multiple condylomata lata: a case report. Int J Dermatol. 2008;47:56–8.
Pourang A, Fung MA, Tartar D, Brassard A. Condyloma lata in secondary syphilis. JAAD Case Rep. 2021;10:18–21. https://doi.org/10.1016/j.jdcr.2021.01.025.
Aung PP, Wimmer DB, Lester TR, Tetzlaff MT, Prieto VG. Perianal condylomata lata mimicking carcinoma. J Cutan Pathol. 2022;49:209–14.
Barnhill RL, editor. Dermatopathology. 4th ed. New York: McGraw-Hill Education; 2020.
Pandhi R, Singh N, Ramam M. Secondary syphilis: a clinicopathologic study. Int J Dermatol. 1995;34:240–3.
Engelkens H, ten Kate F, Vuzevski V, van der Sluis J, Stolz E. Primary and secondary syphilis: a histopathological study. Int J STD AIDS. 1991;2:280–4.
Flamm A, Parikh K, Xie Q, Kwon EJ, Elston DM. Histologic features of secondary syphilis: a multicenter retrospective review. J Am Acad Dermatol. 2015;73:1025–30. https://doi.org/10.1016/j.jaad.2015.08.062.
Martín-Ezquerra G, Fernandez-Casado A, Barco D, Jucglà A, Juanpere-Rodero N, Manresa JM, et al. Treponema pallidum distribution patterns in mucocutaneous lesions of primary and secondary syphilis: an immunohistochemical and ultrastructural study. Hum Pathol. 2009;40:624–30.
Tanabe J, Huntley A. Granulomatous tertiary syphilis. J Am Acad Dermatol. 1986;15:341–4.
Pereira T, Fernandes J, Vieira A, Sousa BA. Tertiary syphilis. Int J Dermatol. 2007;46:1192–5.
Mohammad K, Shalabi M, Burgess B, Khan S, Ehrsam E, Khachemoune A. Alopecia syphilitica, from diagnosis to treatment. Proc (Bayl Univ Med Cent). 2022;35:180–3. https://doi.org/10.1080/08998280.2021.2021761.
Katayama S, Ota M. Rapidly progressive hair loss may be the only sign of syphilis. Am J Med. 2022;135:e121–2. https://doi.org/10.1016/j.amjmed.2022.01.041.
Tucker JD, Shah S, Jarell AD, Tsai KY, Zembowicz A, Kroshinsky D. Lues maligna in early HIV infection case report and review of the literature. Sex Transm Dis. 2009;36:512–4.
Wibisono O, Idrus I, Djawad K. Malignant syphilis: a systematic review of the case reports published in 2014–2018. Actas Dermosifiliogr. 2021;112:725–34.
Bolognia J, Schaffer JV, Cerroni L. Dermatology. 4th ed. Philadelphia: Elsevier; 2018.
Clark EG, Danbolt N. The Oslo study of the natural history of untreated syphilis. J Chronic Dis. 1955;2:311–44.
Ghanem KG, Ram S, Rice PA. The modern epidemic of syphilis. N Engl J Med. 2020;382:845–54.
Goette DK, Prescott CE. Late benign syphilis of the skin. South Med J. 1978;71:505–8.
Kwak J, Lamprecht C. A review of the guidelines for the evaluation and treatment of congenital syphilis. Pediatr Ann. 2015;44:e108–14.
Woods CR. Congenital syphilis-persisting pestilence. Pediatr Infect Dis J. 2009;28:536–7.
LaFond RE, Lukehart SA. Biological basis for syphilis. Clin Microbiol Rev. 2006;19:29–49.
Romanowski B, Sutherland R, Fick GH, Mooney D, Love EJ, et al. Serologic response to treatment of infectious syphilis. Ann Intern Med. 1991;114:1005–9.
Forrestel AK, Kovarik CL, Katz KA. Sexually acquired syphilis: laboratory diagnosis, management, and prevention. J Am Acad Dermatol. 2020;82:1–14. https://doi.org/10.1016/j.jaad.2019.02.074.
Tong ML, Lin LR, Liu GL, Zhang HL, Zeng Y-L, Zheng W-H, et al. Factors associated with serological cure and the serofast state of HIV-negative patients with primary, secondary, latent, and tertiary syphilis. PLoS ONE. 2013;8:e70102. https://doi.org/10.1371/journal.pone.0070102.
Seña AC, Wolff M, Behets F, van Damme K, Martin DH, Leone P, et al. Response to therapy following retreatment of serofast early syphilis patients with benzathine penicillin. Clin Infect Dis. 2013;56:420–2.
Morshed MG, Singh AE. Recent trends in the serologic diagnosis of syphilis. Clin Vaccine Immunol. 2015;22:137–47.
Liu LL, Lin LR, Tong ML, Zhang HL, Huang S-J, Chen Y-Y, et al. Incidence and risk factors for the prozone phenomenon in serologic testing for syphilis in a large cohort. Clin Infect Dis. 2014;59:384–9.
Workowski KA, Bachmann LH, Chan PA, et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep 2021;70(No. RR-4):1–187. https://doi.org/10.15585/mmwr.rr7004a1.
Gao Y, Katz KA. Clinical and serologic evolution of multiple penile chancres in a man who has sex with men. JAMA Dermatol. 2018;154:108–9.
Tsang RS, Shuel M, Hayden K, van Caeseele P, Stein D. Laboratory evaluation of two point-of-care test kits for the identification of infectious syphilis. Can Commun Dis Rep. 2022;48:82–8.
Wang CI, Ong JJ, Zhao P, Marie Weideman AI, Tang WI, Kumi Smith MI, et al. Expanding syphilis test uptake using rapid dual self-testing for syphilis and HIV among men who have sex with men in China: a multiarm randomized controlled trial. PLoS Med. 2022;19:1–18. https://doi.org/10.1371/journal.pmed.1003930.
Clement ME, Okeke NL, Hicks CB. Treatment of syphilis: a systematic review. JAMA. 2014;312:1905–17.
Aronson IK, Soltani K. The enigma of the pathogenesis of the Jarisch-Herxheimer reaction. Sex Transm Infect. 1976;52:313–5.
Yang CJ, Lee NY, Lin YH, Lee HC, Ko WC, Liao CH, et al. Jarisch-Herxheimer reaction after penicillin therapy among patients with syphilis in the era of the HIV infection epidemic: incidence and risk factors. Clin Infect Dis. 2010;51:976–9.
Butler T. The Jarisch-Herxheimer reaction after antibiotic treatment of spirochetal infections: a review of recent cases and our understanding of pathogenesis. Am J Trop Med Hyg. 2017;96:46–52.
Rac MWF, Revell PA, Eppes CS. Syphilis during pregnancy: a preventable threat to maternal-fetal health. Am J Obstet Gynecol. 2017;216:352–63.
Tuddenham S, Hamill MM, Ghanem KG. Diagnosis and Treatment of Sexually Transmitted Infections: A Review. JAMA - J Am Med Assoc. 2022;327:161–72.
Lin JS, Eder ML, Bean SI. Screening for syphilis infection in pregnant women updated evidence report and systematic review for the us preventive services task force. JAMA - J Am Med Assoc. 2018;320:918–25.
Cantor AG, Pappas M, Daeges M, Nelson HD. Screening for syphilis: Updated evidence report and systematic review for the US preventive services task force. JAMA - J Am Med Assoc. 2016;315:2328–37.
Bibbins-Domingo K, Grossman DC, Curry SJ, Davidson KW, Epling JW, García FAR, et al. Screening for Syphilis Infection in Nonpregnant Adults and Adolescents: US Preventive Services Task Force Recommendation Statement. JAMA - J Am Med Assoc. 2016;315:2321–7.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No funding was received for the preparation of this article.
Conflicts of Interest/Competing Interests
There are no financial disclosures, commercial associations, or any other conditions posing a conflict of interest to report for any of the authors.
Ethics Approval
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Availability of Data and Material.
Data were obtained from public domain resources.
Code Availability
Not applicable.
Authors’ Contributions
All authors contributed to the conception and design of the manuscript. The literature search was performed by Cleo Whiting. The first draft of the manuscript was written by CW and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Rights and permissions
About this article

Cite this article
Whiting, C., Schwartzman, G. & Khachemoune, A. Syphilis in Dermatology: Recognition and Management. Am J Clin Dermatol 24, 287–297 (2023). https://doi.org/10.1007/s40257-022-00755-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40257-022-00755-3