


click on thumbnail to enlarge; advance with cursor over border
return to: Laryngology
see also: Bechet's Syndrome (Neuro-Beçhet) Rythmic Myoclonus Laryngeal - Pharyngeal and Lower Lip Bump (Mucocele) Minor Salivary Gland Traumatic Lesion with Histopathology

Image A: Watercolor drawing of the face and neck of a man affected with pemphigus.
Medical Photographic Library Keywords: Godart, Thomas with permission from wikimedia commons. By http://wellcomeimages.org/indexplus/obf_images/b2/73/6680f836ba1456bfd46...
{kind=link}

Microscopic image of direct immunofluorescence using an anti-IgG antibody. The tissue is skin from a patient with Pemphigus vulgaris. Note the intercellular IgG deposits in the epidermis and the early intraepidermal vesicle caused by acantholysis.
Photo with permissions from Wikimedia Commons. By Emmanuelm at English Wikipedia, CC BY 3.0, https://commons.wikimedia.org/w/index.php?curid=9915157
Background
- Pemphigus vulgaris (PV) is an autoimmune, intraepithelial, bullous disease. It involves the skin and/or mucosa. Ig(G) antibodies to desmoglein 1 and 3 cause blisters due to acantholysis. It is a rare disease (0.1-0.5 cases/100,000 inhabitants/year) [Bascones-Martinez 2010]
Clinical presentation
- PV usually begins with mucosal involvement with or without skin lesions. Oral lesions are hallmark of pemphigus vulgaris and occur in almost all cases [Mustafa 2015]. Oral lesions are the first manifestations in 50-90% of cases. They typically precede cutaneous lesions by 2-6 months [Bascones-Martinez 2010].
- Mucosal lesions are usually located in the oral and pharyngeal mucosa [Mustafa 2015].
- PV can also involve mucosal tissue other than oral mucosa. Lesions can occur on nasal, pharyngeal, laryngeal, and esophageal mucosa. Conjunctive, genital and anal mucosa can also be involved [Bascones-Martinez 2010].
- Oropharyngeal and laryngeal lesions may present with sore throat, dysphagia, hoarseness, and in severe cases airway impairment.
- Cutaneous lesions may be the first sign in patients with asymptomatic mucosal lesions. Patients presenting to primary care providers or dermatology with suspected PV should be referred to otolaryngology for orolaryngeal evaluation.
Diagnosis
- Biopsy from affected tissue shows suprabasilar acantholysis.
- Immunoflourescence testing reveals a reticular pattern of IgG antibodies around epidermal cells.
- ELISA positive for anti-desmoglein (Dsg) 3 is consisent with mucosal PV; ELISA positive for Dsg 1 and 3 is consistent with mucocutaneous PV [Abasq 2009].
- Nikolsky sign: (epidermis separates upon manual stroking of skin). Reported to be 96.3% specific in the oral setting [Bascones-Martinez 2010].
Treatment
- Corticosteroids (oral or IV) are first line.
- Immunosuppresants (such as methotrexate, cyclophosphamide, or rituximab) for patients with poor response to corticosteroids.
- Intravenous immunoglobulin treatment may be appropriate for patients with refractory disease or with contraindications to immunosuppresant therepy [Gregoriou].
- Patients with oropharnygeal PV have high rates of achieving long-lasting clinical remission (94.6%) using conventional immunosuppresive therapy [Mignogna 2010].
Case Example
History:
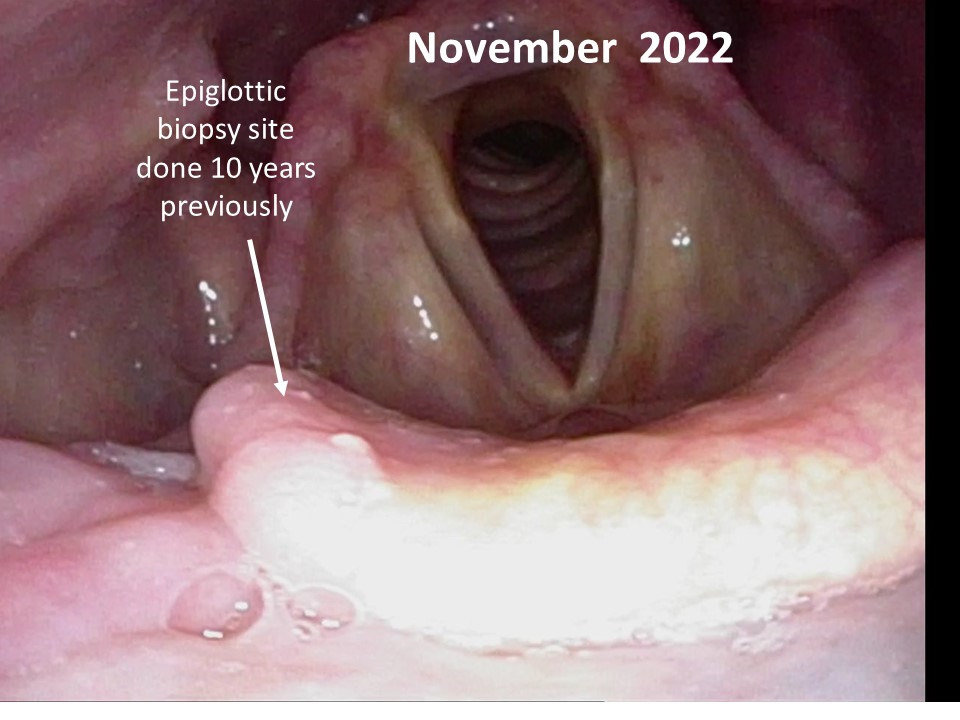
A 67 year old male presented to UIHC on Sept 2012 with a several month history of throat pain, described as feeling like something had scratched his throat, with waxing and waning discomfort. He had been treated in February/March with amoxicillin and antifungals without improvement. A dentist also commented to him that he had a 'canker sore' on his gum. Direct laryngoscopy and a biopsy from an outside hospital was read as squamous papiloma of the tip of the epiglottis. Pain was more prominent with swallowing than at rest. He had been treated with antibiotics for laryngeal candidiasis without resolution of pain.
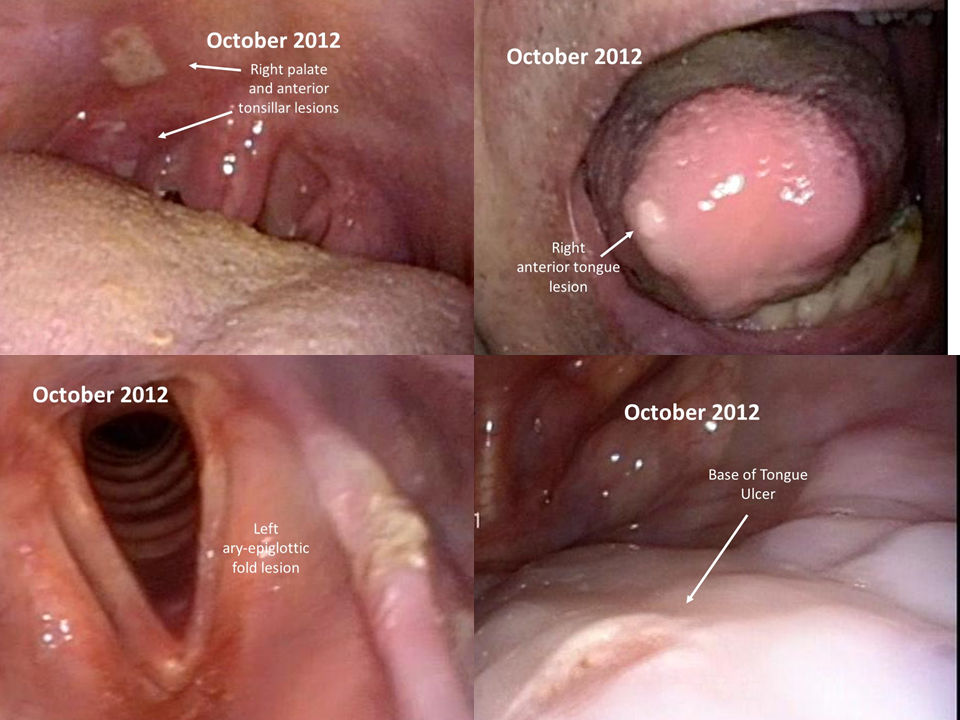
Exam with transnasal fiberoptic laryngoscopy showed a superficial ulceration on the left base of tongue and right lateral confluence between the base of tongue and lateral pharyngeal wall as well as the right tip of the epiglottis with whitish material along the left aryepiglottic fold. Labs were positive for ANA, negative for SSA/SSB, and consultation with rheumatology was arranged on 10/19/2012 at the advice of the Tumor Board. UIHC pathologists, with consultation from dermatopathologists, reviewed the outside biopsy of the epiglottis and thought the biopsy showed suprabasilar acantholysis highly suspicious for pemphigus. Further lab studies showed ELISA positivity (Dsg 3 levels positive, Dsg 1 negative) for mucosal pemphigus vulgaris.
Oct 2012: New lesions have developed on the palate and tonsils.
Nov 2012: Steroid treatment was initiated by dermatology. Patient noted marked improvement with prednisone 20mg/day at follow up on 11/29/2012.
Jan 2013: Noted that the patient continues to have throat discomfort. Treatment with clotrimazole troches for suspected Candida is initiated. The patient continues on prednisone 20mg/day.
Later Jan 2013: Due to persistence of throat symptoms and unchanging ulcers, the patient is started on rituximab 375 mg/m2 weekly for 4 weeks (first dose scheduled 2/8/2017). The prednisone is continued at 20 mg/day.
Feb 2013: The patient called into OTO clinic to share that he awoke with no sore throat for the first time in over a year the morning after his first rituximab infusion.
March 2013: Unlike previous exams, there were no signs of ulcerations intraorally or in the oropharnx. The patient has completed 3 of 4 rituximab infusions. He reports complete relief of sore throat for a period of about three days after infusion, then notices recurrence of discomfort. The prednisone is continued at 20 mg/day
July 2013: Patient has completed 4 rituximab infusions. Predisone has been tapered to 5 mg/day. His only symptoms are some throat irritation that he attributes to use of CPAP. Physical exm and flexible fiberoptic laryngoscopy show no signs of ulcers.
August 2014: Patient reports he cannot recall having throat pain for over a year now. Prednisone taper was completed in November.
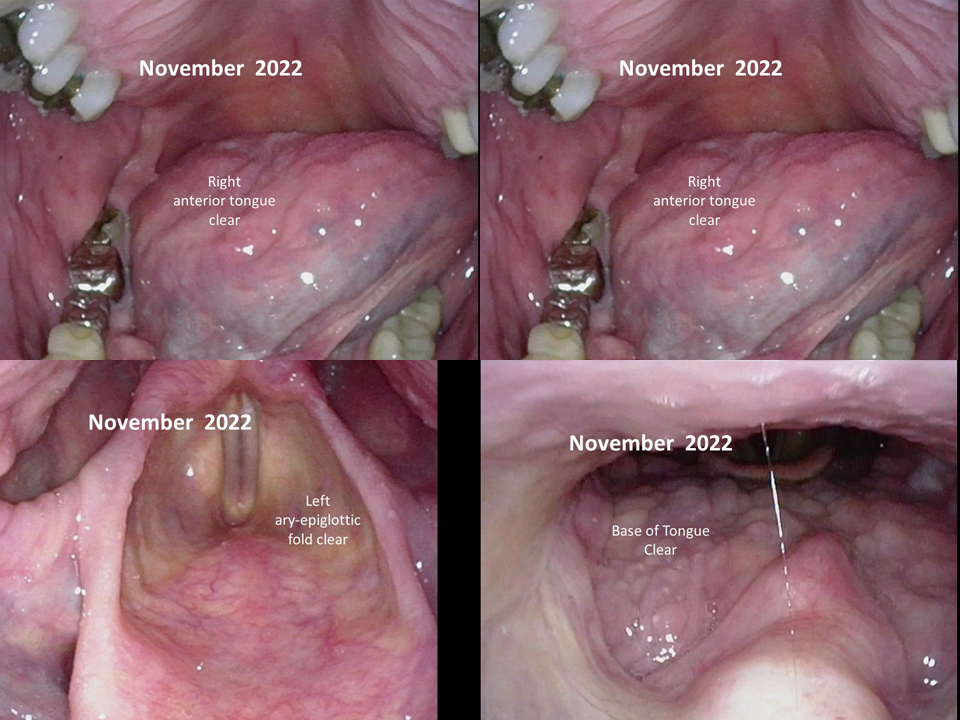
June 2017: At the most recent follow-up, the patient has no breathing, speaking, or swallowing problems and no recurrence of oral ulcerations or symptoms. Transnasal laryngoscopy showed no lesions in the laryngopharynx.
Images from the initial patient presentation to UIHC Otolaryngology
References
Abasq, C. et al ELISA Testing of Anti-Desmoglein 1 and 3 Antibodies in the Management of Pemphigus (2009)
Bascones-Martinez, A. et al Oral Manifestations of Pemphigus Vulgaris: Clinical Presentaion, Differential Diagnosis and Management (2010)
Gregoriou, S. et al Management of Pemphigus Vulgaris: challenges and solutions
Mahmoud, A. et al Laryngeal involvement in pemphigus vulgaris: a proposed classification system (2012)
Mignogna, M. et al Oropharyngeal Pemphigus Vulgaris and Clinical Remission (2010)
Mustafa, M. et al Oral mucosal manifestations of autoimmune skin diseases (2015)