
ZIAC Bisoprolol Fumarate / Hydrochlorothiazide 2.5mg / 6.25mg Film-Coated Tablet 1's

RXDRUG-DR-XY26004-1pc
Discreet Packaging
We recognize that purchasing medications can be a deeply personal matter. To respect your privacy, we ensure that all orders are packaged discreetly, with no indication of the contents on the packaging. This means that even our couriers remain unaware of the package contents.
Furthermore, we uphold strict confidentiality standards. We guarantee that your order information will never be disclosed to any third party. Your trust is paramount to us, and we are committed to safeguarding your privacy at every step of the process. Our dedication to discretion and confidentiality is part of our unwavering commitment to you, our valued customer.
FDA-registered Products
FDA-licensed Pharmacies
Features
Brand
Ziac
Full Details
Dosage Strength
2.5mg / 6.25mg
Drug Ingredients
- Bisoprolol Fumarate
- Hydrochlorothiazide
Drug Packaging
Film-Coated Tablet 1's
Generic Name
Bisoprolol Fumarate / Hydrochlorothiazide
Dosage Form
Film-Coated Tablet
Registration Number
DR-XY26004
Drug Classification
Prescription Drug (RX)
Description
Indications/Uses
Treatment of essential hypertension.
Dosage/Direction for Use
The usual starting dose is one tablet bisoprolol + hydrochlorothiazide (Ziac) 2.5 mg/6.25 mg once daily. If the antihypertensive effect of this dosage is inadequate, the dose will be increased to one tablet bisoprolol + hydrochlorothiazide (Ziac) 5 mg/6.25 mg once daily and, if response is still inadequate, to one tablet bisoprolol + hydrochlorothiazide (Ziac) 10 mg/6.25 mg once daily.
Duration of treatment: Treatment with bisoprolol + hydrochlorothiazide (Ziac) is generally a long-term therapy.
Gradual discontinuation of bisoprolol treatment is recommended, since abrupt withdrawal of bisoprolol may lead to an acute deterioration of the patient's condition, in particular in patients with ischemic heart disease.
Administration: Take bisoprolol + hydrochlorothiazide (Ziac) tablet in the morning, with or without food. Swallow the tablet with some liquid. Do not chew.
Special Populations: Patients with renal or hepatic impairment: No dose adjustment is necessary in patients with mild-to-moderate hepatic impairment or mild-to-moderate renal impairment (creatinine clearance > 30 mL/min).
Elderly: No dosage adjustment is normally required in the elderly.
Pediatric patients: Experience with bisoprolol + hydrochlorothiazide (Ziac) in pediatric patients is limited, therefore its use cannot be recommended in this population.
Duration of treatment: Treatment with bisoprolol + hydrochlorothiazide (Ziac) is generally a long-term therapy.
Gradual discontinuation of bisoprolol treatment is recommended, since abrupt withdrawal of bisoprolol may lead to an acute deterioration of the patient's condition, in particular in patients with ischemic heart disease.
Administration: Take bisoprolol + hydrochlorothiazide (Ziac) tablet in the morning, with or without food. Swallow the tablet with some liquid. Do not chew.
Special Populations: Patients with renal or hepatic impairment: No dose adjustment is necessary in patients with mild-to-moderate hepatic impairment or mild-to-moderate renal impairment (creatinine clearance > 30 mL/min).
Elderly: No dosage adjustment is normally required in the elderly.
Pediatric patients: Experience with bisoprolol + hydrochlorothiazide (Ziac) in pediatric patients is limited, therefore its use cannot be recommended in this population.
Overdosage
Symptoms: The most common signs expected with overdose of a betablocker are slow heart rate (bradycardia), marked drop in blood pressure (hypotension), bronchospasm, acute cardiac insufficiency and hypoglycemia. There is a wide interindividual variation in sensitivity to one single high dose of bisoprolol and patients with heart failure are probably very sensitive.
The clinical picture in acute or chronic overdose of hydrochlorothiazide is characterized by the extent of fluid and electrolyte loss. Most common signs are dizziness, nausea, somnolence, hypovolemia, hypotension, hypokalemia.
Management: In general, if overdose occurs, discontinuation of bisoprolol + hydrochlorothiazide (Ziac) and supportive and symptomatic treatment is recommended.
Limited data suggest that bisoprolol is hardly dialyzable. The degree to which hydrochlorothiazide is removed by hemodialysis has not been established.
The clinical picture in acute or chronic overdose of hydrochlorothiazide is characterized by the extent of fluid and electrolyte loss. Most common signs are dizziness, nausea, somnolence, hypovolemia, hypotension, hypokalemia.
Management: In general, if overdose occurs, discontinuation of bisoprolol + hydrochlorothiazide (Ziac) and supportive and symptomatic treatment is recommended.
Limited data suggest that bisoprolol is hardly dialyzable. The degree to which hydrochlorothiazide is removed by hemodialysis has not been established.
Administration
May be taken with or without food: Take in the morning. Swallow whole w/ some liqd, do not chew.
Contraindications
Bisoprolol + hydrochlorothiazide (Ziac) is contraindicated in patients with: hypersensitivity to bisoprolol, hydrochlorothiazide, other thiazides, sulphonamides, or any of the excipients; acute heart failure or during episodes of heart failure decompensation requiring intravenous inotropic (substances increasing the contractility of the heart) therapy; cardiogenic shock (acute serious heart condition causing low blood pressure and circulatory failure); second or third degree AV block (severe disturbances of atrioventricular conduction) without a pacemaker; sick sinus syndrome; sinoatrial block; symptomatic bradycardia (slowed heart rate, causing problems); severe bronchial asthma; severe forms of peripheral arterial occlusive disease or Raynaud's syndrome; untreated pheochromocytoma (a rare tumor of the adrenal gland); severe renal impairment (creatinine clearance <30 mL/min); severe hepatic impairment; metabolic acidosis (increase of blood acidity as a result of severe illness); refractory hypokalemia (low blood levels of potassium, not responding to treatment).
Special Precautions
Treatment with bisoprolol must not be withdrawn abruptly unless clearly indicated, since abrupt withdrawal of bisoprolol may lead to an acute deterioration of the patient's condition in particular in patients with ischemic heart disease (see Dosage & Administration).
Bisoprolol + hydrochlorothiazide (Ziac) must be used with caution in patients with: accompanying heart failure; diabetes mellitus showing large fluctuations in blood glucose values; symptoms of hypoglycemia (e.g. tachycardia, palpitations or sweating) can be masked; strict fasting; first degree AV block.
Prinzmetal's angina: Cases of coronary vasospasm have been observed. Despite its high beta1-selectivity, angina attacks cannot be completely excluded when bisoprolol is administered to patients with Prinzmetal's angina. Utmost caution must be exercised.
Peripheral arterial occlusive disease. Aggravation of symptoms may occur especially when starting therapy; hypovolemia; impaired liver function.
As with other beta-blockers, bisoprolol may increase both the sensitivity towards allergens and the severity of anaphylactic reactions. This also applies to desensitization therapy. Epinephrine treatment may not always yield the expected therapeutic effect.
Patients with psoriasis or with a history of psoriasis should only be given beta-blockers (e.g. bisoprolol) after careful balancing of benefits against risks.
The symptoms of thyrotoxicosis may be masked under treatment with bisoprolol.
In patients with pheochromocytoma, bisoprolol must not be administered until after alpha-receptor blockade.
In patients undergoing general anesthesia, the anesthetist must be aware of beta-blockade. If it is thought necessary to withdraw beta-blocker therapy before surgery, this should be done gradually and completed about 48 hours before anesthesia.
Although cardioselective (beta1) beta-blockers may have less effect on lung function than non-selective betablockers, as with all beta-blockers, these should be avoided in patients with obstructive airways diseases, unless there are compelling clinical reasons for their use. Where such reasons exist, bisoprolol + hydrochlorothiazide (Ziac) may be used with caution. In bronchial asthma or other chronic obstructive pulmonary diseases, which may cause symptoms, concomitant bronchodilating therapy is recommended. Occasionally an increase of the airway resistance may occur in patients with asthma, therefore the dose of beta2-stimulants may have to be increased.
Photosensitivity reactions may occur with thiazide diuretics. If photosensitivity reactions occur, it is recommended to protect exposed areas to the sun or to artificial UVA light. In severe cases it may be necessary to stop the treatment.
An increased risk of non-melanoma skin cancer (NMSC) [basal cell carcinoma (BCC) and squamous cell carcinoma (SCC)] with increasing cumulative dose of hydrochlorothiazide exposure has been observed in two epidemiological studies based on the Danish National Cancer Registry. Photosensitizing actions of hydrochlorothiazide could act as a possible mechanism for NMSC.
Patients taking hydrochlorothiazide should be informed of the risk of NMSC and advised to regularly check their skin for any new lesions and promptly report any suspicious skin lesions. Possible preventive measures such as limited exposure to sunlight and UV rays and, in case of exposure, adequate protection should be advised to the patients in order to minimize the risk of skin cancer. Suspicious skin lesions should be promptly examined potentially including histological examinations of biopsies. The use of hydrochlorothiazide may also need to be reconsidered in patients who have experienced previous NMSC (see Adverse Reactions).
Long-term, continuous administration of hydrochlorothiazide may lead to fluid and electrolyte disturbances, in particular to hypokalemia, hyponatremia, hypomagnesemia, hypochloremia, and hypercalcemia. Hypokalemia facilitates the development of severe arrhythmias, particularly torsade de pointes, which may be fatal.
During long term-therapy with bisoprolol + hydrochlorothiazide (Ziac), monitoring of serum electrolytes (especially potassium, sodium, calcium), creatinine, urea, serum lipids (cholesterol and triglycerides), uric acid as well as blood glucose is recommended.
In patients with hyperuricemia, the risk for attacks of gout may be increased.
Metabolic alkalosis may worsen due to disturbance of fluid and electrolyte hemostasis.
In patients with cholelithiasis acute cholecystitis has been reported. Hydrochlorothiazide can cause an idiosyncratic reaction, resulting in choroidal effusion with visual field defect, acute transient myopia and acute angle-closure glaucoma. Symptoms include acute onset of decreased visual acuity or ocular pain and typically occur within hours to weeks of drug initiation. Untreated acute angle-closure glaucoma can lead to permanent vision loss. The primary treatment is to discontinue hydrochlorothiazide as rapidly as possible.
Acute Respiratory Toxicity: Very rare severe cases of acute respiratory toxicity, including acute respiratory distress syndrome (ARDS) have been reported after taking hydrochlorothiazide.
Pulmonary oedema typically develops within minutes to hours after hydrochlorothiazide intake. At the onset, symptoms include dyspnoea, fever, pulmonary deterioration and hypotension. If diagnosis of ARDS is suspected, Bisoprolol fumarate + Hydrocholorothiazide (Ziac) should be withdrawn and appropriate treatment given. Hydrochlorothiazide should not be administered to patients who previously experienced ARDS following hydrochlorothiazide intake.
Effects on the ability to drive and use machines: In general bisoprolol + hydrochlorothiazide (Ziac) has no or negligible influence on the ability to drive and use machines.
However, depending on the individual patient's response to treatment, the ability to drive a vehicle or to use machines may be impaired. This needs to be considered particularly at start of treatment, upon change of medication, or in conjunction with alcohol.
Bisoprolol + hydrochlorothiazide (Ziac) must be used with caution in patients with: accompanying heart failure; diabetes mellitus showing large fluctuations in blood glucose values; symptoms of hypoglycemia (e.g. tachycardia, palpitations or sweating) can be masked; strict fasting; first degree AV block.
Prinzmetal's angina: Cases of coronary vasospasm have been observed. Despite its high beta1-selectivity, angina attacks cannot be completely excluded when bisoprolol is administered to patients with Prinzmetal's angina. Utmost caution must be exercised.
Peripheral arterial occlusive disease. Aggravation of symptoms may occur especially when starting therapy; hypovolemia; impaired liver function.
As with other beta-blockers, bisoprolol may increase both the sensitivity towards allergens and the severity of anaphylactic reactions. This also applies to desensitization therapy. Epinephrine treatment may not always yield the expected therapeutic effect.
Patients with psoriasis or with a history of psoriasis should only be given beta-blockers (e.g. bisoprolol) after careful balancing of benefits against risks.
The symptoms of thyrotoxicosis may be masked under treatment with bisoprolol.
In patients with pheochromocytoma, bisoprolol must not be administered until after alpha-receptor blockade.
In patients undergoing general anesthesia, the anesthetist must be aware of beta-blockade. If it is thought necessary to withdraw beta-blocker therapy before surgery, this should be done gradually and completed about 48 hours before anesthesia.
Although cardioselective (beta1) beta-blockers may have less effect on lung function than non-selective betablockers, as with all beta-blockers, these should be avoided in patients with obstructive airways diseases, unless there are compelling clinical reasons for their use. Where such reasons exist, bisoprolol + hydrochlorothiazide (Ziac) may be used with caution. In bronchial asthma or other chronic obstructive pulmonary diseases, which may cause symptoms, concomitant bronchodilating therapy is recommended. Occasionally an increase of the airway resistance may occur in patients with asthma, therefore the dose of beta2-stimulants may have to be increased.
Photosensitivity reactions may occur with thiazide diuretics. If photosensitivity reactions occur, it is recommended to protect exposed areas to the sun or to artificial UVA light. In severe cases it may be necessary to stop the treatment.
An increased risk of non-melanoma skin cancer (NMSC) [basal cell carcinoma (BCC) and squamous cell carcinoma (SCC)] with increasing cumulative dose of hydrochlorothiazide exposure has been observed in two epidemiological studies based on the Danish National Cancer Registry. Photosensitizing actions of hydrochlorothiazide could act as a possible mechanism for NMSC.
Patients taking hydrochlorothiazide should be informed of the risk of NMSC and advised to regularly check their skin for any new lesions and promptly report any suspicious skin lesions. Possible preventive measures such as limited exposure to sunlight and UV rays and, in case of exposure, adequate protection should be advised to the patients in order to minimize the risk of skin cancer. Suspicious skin lesions should be promptly examined potentially including histological examinations of biopsies. The use of hydrochlorothiazide may also need to be reconsidered in patients who have experienced previous NMSC (see Adverse Reactions).
Long-term, continuous administration of hydrochlorothiazide may lead to fluid and electrolyte disturbances, in particular to hypokalemia, hyponatremia, hypomagnesemia, hypochloremia, and hypercalcemia. Hypokalemia facilitates the development of severe arrhythmias, particularly torsade de pointes, which may be fatal.
During long term-therapy with bisoprolol + hydrochlorothiazide (Ziac), monitoring of serum electrolytes (especially potassium, sodium, calcium), creatinine, urea, serum lipids (cholesterol and triglycerides), uric acid as well as blood glucose is recommended.
In patients with hyperuricemia, the risk for attacks of gout may be increased.
Metabolic alkalosis may worsen due to disturbance of fluid and electrolyte hemostasis.
In patients with cholelithiasis acute cholecystitis has been reported. Hydrochlorothiazide can cause an idiosyncratic reaction, resulting in choroidal effusion with visual field defect, acute transient myopia and acute angle-closure glaucoma. Symptoms include acute onset of decreased visual acuity or ocular pain and typically occur within hours to weeks of drug initiation. Untreated acute angle-closure glaucoma can lead to permanent vision loss. The primary treatment is to discontinue hydrochlorothiazide as rapidly as possible.
Acute Respiratory Toxicity: Very rare severe cases of acute respiratory toxicity, including acute respiratory distress syndrome (ARDS) have been reported after taking hydrochlorothiazide.
Pulmonary oedema typically develops within minutes to hours after hydrochlorothiazide intake. At the onset, symptoms include dyspnoea, fever, pulmonary deterioration and hypotension. If diagnosis of ARDS is suspected, Bisoprolol fumarate + Hydrocholorothiazide (Ziac) should be withdrawn and appropriate treatment given. Hydrochlorothiazide should not be administered to patients who previously experienced ARDS following hydrochlorothiazide intake.
Effects on the ability to drive and use machines: In general bisoprolol + hydrochlorothiazide (Ziac) has no or negligible influence on the ability to drive and use machines.
However, depending on the individual patient's response to treatment, the ability to drive a vehicle or to use machines may be impaired. This needs to be considered particularly at start of treatment, upon change of medication, or in conjunction with alcohol.
Use In Pregnancy & Lactation
Pregnancy: Bisoprolol has pharmacological effects that may cause harmful effects on pregnancy and/or the fetus/newborn.
In general, beta-adrenoceptor blockers reduce placental perfusion, which has been associated with growth retardation, intrauterine death, abortion or early labor. Adverse effects (e.g. hypoglycemia and bradycardia) may occur in the fetus and newborn infant. If treatment with beta-adrenoceptor blockers is necessary, beta1-selective adrenoceptor blockers are preferable.
Diuretics may give rise to fetoplacental ischemia with the attendant risk of fetal hypotrophy.
Hydrochlorothiazide is suspected to cause thrombocytopenia in the neonate.
Bisoprolol + hydrochlorothiazide (Ziac) is not recommended during pregnancy.
Lactation: Bisoprolol + hydrochlorothiazide (Ziac) is not recommended in breastfeeding women because bisoprolol may be, and hydrochlorothiazide is excreted in breast milk in minimal amounts. Hydrochlorothiazide can inhibit the milk production.
Fertility: No human data on fertility are known for the combination product. Bisoprolol or hydrochlorothiazide had no influence on fertility or on general reproduction performance in animal studies.
In general, beta-adrenoceptor blockers reduce placental perfusion, which has been associated with growth retardation, intrauterine death, abortion or early labor. Adverse effects (e.g. hypoglycemia and bradycardia) may occur in the fetus and newborn infant. If treatment with beta-adrenoceptor blockers is necessary, beta1-selective adrenoceptor blockers are preferable.
Diuretics may give rise to fetoplacental ischemia with the attendant risk of fetal hypotrophy.
Hydrochlorothiazide is suspected to cause thrombocytopenia in the neonate.
Bisoprolol + hydrochlorothiazide (Ziac) is not recommended during pregnancy.
Lactation: Bisoprolol + hydrochlorothiazide (Ziac) is not recommended in breastfeeding women because bisoprolol may be, and hydrochlorothiazide is excreted in breast milk in minimal amounts. Hydrochlorothiazide can inhibit the milk production.
Fertility: No human data on fertility are known for the combination product. Bisoprolol or hydrochlorothiazide had no influence on fertility or on general reproduction performance in animal studies.
Adverse Reactions
Common (≥ 1% and < 10%), Uncommon (≥ 0.1% and < 1%), Rare (≥ 0.01% and < 0.1%), Very rare (< 0.01%) including isolated cases. (See table.)
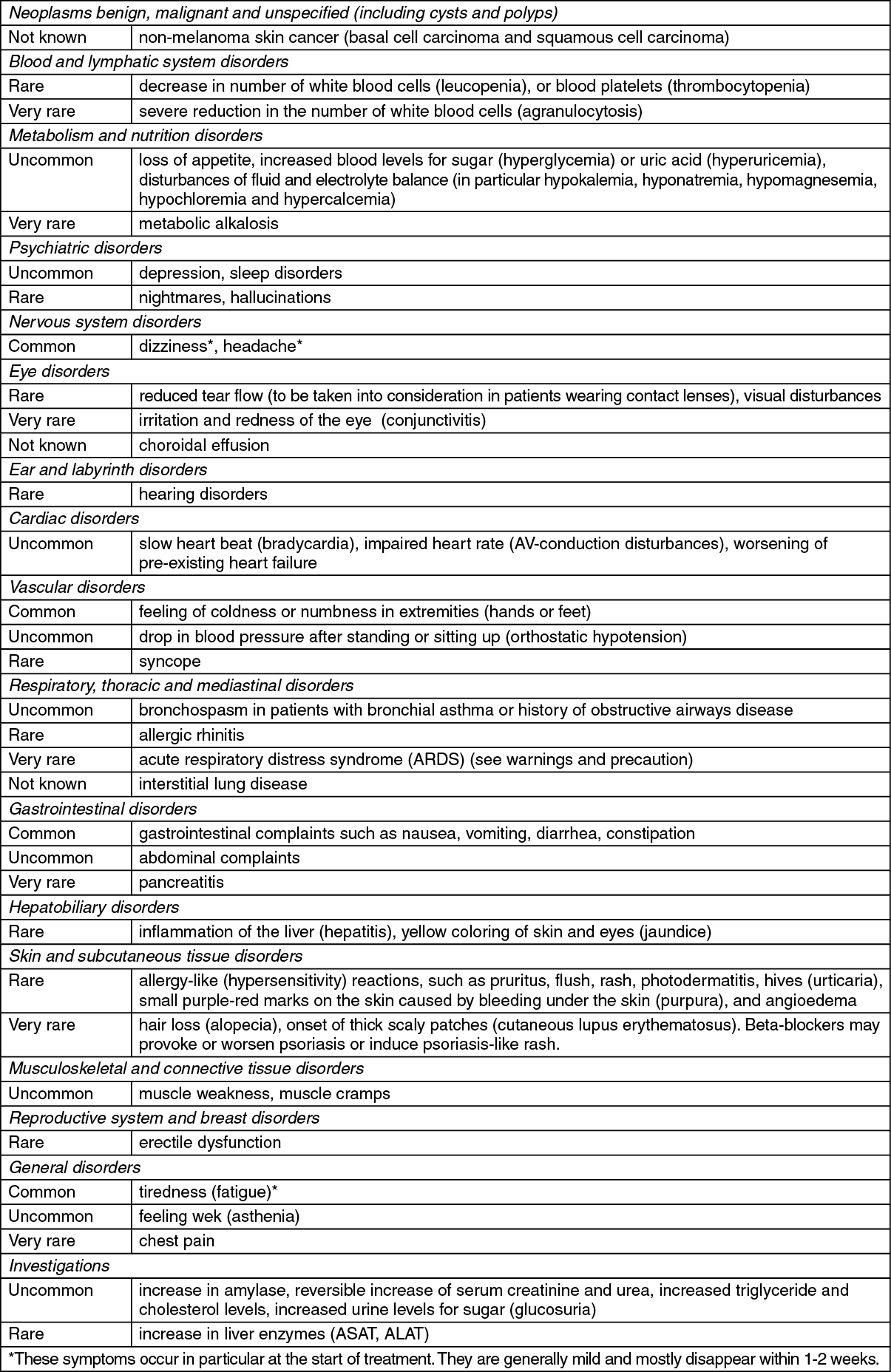
Description of selected adverse reactions: Non-melanoma skin cancer: Based on available data from epidemiological studies, cumulative dose dependent association between hydrochlorothiazide and NMSC has been observed (see also Precautions and Pharmacology: Pharmacodynamics under Actions).
At the first sign of any adverse drug reaction, patient must seek medical attention immediately.
At the first sign of any adverse drug reaction, patient must seek medical attention immediately.
Drug Interactions
Combinations not recommended: Lithium: Bisoprolol + hydrochlorothiazide (Ziac) may intensify the cardiotoxic and neurotoxic effect of lithium through a reduction of lithium excretion.
Calcium antagonists of the verapamil type and to a lesser extent of the diltiazem type: Negative effect on contractility and atrio-ventricular conduction. Intravenous administration of verapamil in patients on s-blocker treatment may lead to profound hypotension and atrioventricular block.
Centrally-acting antihypertensive agents (e.g. clonidine, methyldopa, moxonidine, rilmenidine): Concomitant use of centrally-acting antihypertensive agents may lead to a further reduction in heart rate and cardiac output and to vasodilatation. Abrupt withdrawal, particularly if prior to beta-blocker discontinuation, may increase the risk of 'rebound hypertension'.
Combinations to be used with caution: Calcium antagonists of the dihydropyridine type (e.g. nifedipine, amlodipine): Concomitant use may increase the risk of hypotension, and an increase in the risk of a further deterioration of the ventricular pump function in patients with heart failure cannot be excluded.
Concomitant use with other antihypertensive agents or with other medicinal products with blood pressure lowering potential (e.g. tricyclic antidepressants, barbiturates, phenothiazines) may increase the risk of hypotension.
ACE inhibitors (e.g. captopril, enalapril), Angiotensin II antagonists: Risk of significant fall in blood pressure and/or acute renal failure during initiation of ACE inhibitor therapy in patients with preexisting sodium depletion (particularly in patients with renal artery stenosis).
If prior diuretic therapy has produced sodium depletion, either stop the diuretic 3 days before starting ACE inhibitor therapy, or initiate ACE inhibitor therapy at a low dose.
Class-I antiarrhythmic agents (e.g. quinidine, disopyramide, lidocaine, phenytoin; flecainide, propafenone): Effect on atrio-ventricular impulse conduction time may be potentiated and negative inotropic effect increased.
Class-III antiarrhythmic agents (e.g. amiodarone): Effect on atrio-ventricular conduction time may be potentiated.
Antiarrhythmic agents that may induce torsade de pointes (Class IA e.g. quinidine, hydroquinidine, disopyramide, and Class III e.g. amiodarone, sotalol, dofetilide, ibutilide): Hypokalemia may facilitate the occurrence of torsades de pointes.
Nonantiarrhythmic agents that may induce torsade de pointes (e.g. astemizole, i.v. erythromycin, halofantrine, pentamidine, sparfloxacin, terfenadine, vincamine): Hypokalemia may facilitate the occurrence of torsades de pointes.
Parasympathomimetic agents: Concomitant use may increase atrio-ventricular conduction time and the risk of bradycardia.
Topical beta-blockers (e.g. eye drops for glaucoma treatment) may add to the systemic effects of bisoprolol.
Insulin and oral antidiabetic agents: Increase of blood sugar lowering effect.
Blockade of beta-adrenoceptors may mask symptoms of hypoglycemia.
Anesthetic agents: Attenuation of the reflex tachycardia and increase of the risk of hypotension (see Precautions).
Digitalis glycosides: Increase of atrio-ventricular conduction time, reduction in heart rate. If hypokalemia and/or hypomagnesemia develop during treatment with bisoprolol + hydrochlorothiazide (Ziac), the myocardium may show increased sensitivity to cardiac glycosides, leading to an enhanced effect and adverse effects of the glycosides.
Non-steroidal anti-inflammatory drugs (NSAIDs): NSAIDs may reduce the hypotensive effect. In patients developing hypovolemia, the concomitant administration of NSAIDs can trigger acute renal failure.
Beta-sympathomimetics (e.g. isoprenaline, dobutamine): Combination with bisoprolol may reduce the effect of both agents.
Sympathomimetics that activate both beta- and alpha-adrenoceptors (e.g. norepinephrine, epinephrine): Combination with bisoprolol may lead to blood pressure increase and exacerbated intermittent claudication. Such interactions are considered to be more likely with nonselective beta-blockers.
Potassium-wasting medicinal products (e.g. corticosteroids, ACTH, carbenoxolone, amphotericin B, furosemide, or laxatives): Concomitant use may result in increased potassium losses.
Methyldopa: Hemolysis due to the formation of antibodies to hydrochlorothiazide has been described in isolated cases.
The effect of uric-acid-lowering agents may be attenuated in concomitant administration of bisoprolol + hydrochlorothiazide (Ziac).
Cholestyramine and colestipol: Reduces the absorption of the hydrochlorothiazide component of bisoprolol + hydrochlorothiazide (Ziac).
Combinations to be considered: Mefloquine: Increased risk of decelerating the heart rate (bradycardia).
Monoamine oxidase inhibitors (except MAO-B inhibitors): Enhanced hypotensive effect of the beta-blockers but also risk of hypertensive crisis.
Corticosteroids: Reduced antihypertensive effect due to corticosteroid-induced water and sodium retention.
Rifampicin: Slight reduction of the half-life of bisoprolol possible due to the induction of hepatic drug-metabolizing enzymes. Normally no dosage adjustment is necessary.
Ergotamine derivatives: Exacerbation of peripheral circulatory disturbances.
In high-dose salicylate administration the toxic effect of salicylates on the central nervous system may be enhanced.
Calcium antagonists of the verapamil type and to a lesser extent of the diltiazem type: Negative effect on contractility and atrio-ventricular conduction. Intravenous administration of verapamil in patients on s-blocker treatment may lead to profound hypotension and atrioventricular block.
Centrally-acting antihypertensive agents (e.g. clonidine, methyldopa, moxonidine, rilmenidine): Concomitant use of centrally-acting antihypertensive agents may lead to a further reduction in heart rate and cardiac output and to vasodilatation. Abrupt withdrawal, particularly if prior to beta-blocker discontinuation, may increase the risk of 'rebound hypertension'.
Combinations to be used with caution: Calcium antagonists of the dihydropyridine type (e.g. nifedipine, amlodipine): Concomitant use may increase the risk of hypotension, and an increase in the risk of a further deterioration of the ventricular pump function in patients with heart failure cannot be excluded.
Concomitant use with other antihypertensive agents or with other medicinal products with blood pressure lowering potential (e.g. tricyclic antidepressants, barbiturates, phenothiazines) may increase the risk of hypotension.
ACE inhibitors (e.g. captopril, enalapril), Angiotensin II antagonists: Risk of significant fall in blood pressure and/or acute renal failure during initiation of ACE inhibitor therapy in patients with preexisting sodium depletion (particularly in patients with renal artery stenosis).
If prior diuretic therapy has produced sodium depletion, either stop the diuretic 3 days before starting ACE inhibitor therapy, or initiate ACE inhibitor therapy at a low dose.
Class-I antiarrhythmic agents (e.g. quinidine, disopyramide, lidocaine, phenytoin; flecainide, propafenone): Effect on atrio-ventricular impulse conduction time may be potentiated and negative inotropic effect increased.
Class-III antiarrhythmic agents (e.g. amiodarone): Effect on atrio-ventricular conduction time may be potentiated.
Antiarrhythmic agents that may induce torsade de pointes (Class IA e.g. quinidine, hydroquinidine, disopyramide, and Class III e.g. amiodarone, sotalol, dofetilide, ibutilide): Hypokalemia may facilitate the occurrence of torsades de pointes.
Nonantiarrhythmic agents that may induce torsade de pointes (e.g. astemizole, i.v. erythromycin, halofantrine, pentamidine, sparfloxacin, terfenadine, vincamine): Hypokalemia may facilitate the occurrence of torsades de pointes.
Parasympathomimetic agents: Concomitant use may increase atrio-ventricular conduction time and the risk of bradycardia.
Topical beta-blockers (e.g. eye drops for glaucoma treatment) may add to the systemic effects of bisoprolol.
Insulin and oral antidiabetic agents: Increase of blood sugar lowering effect.
Blockade of beta-adrenoceptors may mask symptoms of hypoglycemia.
Anesthetic agents: Attenuation of the reflex tachycardia and increase of the risk of hypotension (see Precautions).
Digitalis glycosides: Increase of atrio-ventricular conduction time, reduction in heart rate. If hypokalemia and/or hypomagnesemia develop during treatment with bisoprolol + hydrochlorothiazide (Ziac), the myocardium may show increased sensitivity to cardiac glycosides, leading to an enhanced effect and adverse effects of the glycosides.
Non-steroidal anti-inflammatory drugs (NSAIDs): NSAIDs may reduce the hypotensive effect. In patients developing hypovolemia, the concomitant administration of NSAIDs can trigger acute renal failure.
Beta-sympathomimetics (e.g. isoprenaline, dobutamine): Combination with bisoprolol may reduce the effect of both agents.
Sympathomimetics that activate both beta- and alpha-adrenoceptors (e.g. norepinephrine, epinephrine): Combination with bisoprolol may lead to blood pressure increase and exacerbated intermittent claudication. Such interactions are considered to be more likely with nonselective beta-blockers.
Potassium-wasting medicinal products (e.g. corticosteroids, ACTH, carbenoxolone, amphotericin B, furosemide, or laxatives): Concomitant use may result in increased potassium losses.
Methyldopa: Hemolysis due to the formation of antibodies to hydrochlorothiazide has been described in isolated cases.
The effect of uric-acid-lowering agents may be attenuated in concomitant administration of bisoprolol + hydrochlorothiazide (Ziac).
Cholestyramine and colestipol: Reduces the absorption of the hydrochlorothiazide component of bisoprolol + hydrochlorothiazide (Ziac).
Combinations to be considered: Mefloquine: Increased risk of decelerating the heart rate (bradycardia).
Monoamine oxidase inhibitors (except MAO-B inhibitors): Enhanced hypotensive effect of the beta-blockers but also risk of hypertensive crisis.
Corticosteroids: Reduced antihypertensive effect due to corticosteroid-induced water and sodium retention.
Rifampicin: Slight reduction of the half-life of bisoprolol possible due to the induction of hepatic drug-metabolizing enzymes. Normally no dosage adjustment is necessary.
Ergotamine derivatives: Exacerbation of peripheral circulatory disturbances.
In high-dose salicylate administration the toxic effect of salicylates on the central nervous system may be enhanced.
Storage
Ziac 2.5 mg/6.25 mg Film-coated Tablet: Store at temperatures not exceeding 30°C.
Ziac 5 mg/6.25 mg Film-coated Tablet: Store at temperatures not exceeding 25°C.
Ziac 10 mg/6.25 mg Film-coated Tablet: Store at temperatures not exceeding 25°C.
Ziac 5 mg/6.25 mg Film-coated Tablet: Store at temperatures not exceeding 25°C.
Ziac 10 mg/6.25 mg Film-coated Tablet: Store at temperatures not exceeding 25°C.
Action
Pharmacology: Pharmacodynamics: Clinical studies have shown that the antihypertensive effects of bisoprolol and hydrochlorothiazide are additive, and the efficacy of the lowest dose, 2.5 mg/6.25 mg, in the treatment of mild-to-moderate essential hypertension has been demonstrated.
The pharmacodynamic effects, including hypokalemia (hydrochlorothiazide), and bradycardia, asthenia, and headache (bisoprolol) are dose-related. Combining both drugs at one-fourth/half the doses used in single-agent therapy (2.5 mg/6.25 mg) aims to reduce those effects.
Bisoprolol: Bisoprolol is a highly selective beta1-adrenoceptor blocking agent with no intrinsic sympathomimetic activity and without significant membrane-stabilizing activity.
As with other beta1-receptor blocking agents, the mechanism of bisoprolol's antihypertensive effect has not been completely established. However, it has been shown that bisoprolol produces a marked decrease in plasma renin and a reduction in heart rate.
Hydrochlorothiazide: Non-melanoma skin cancer: Based on available data from epidemiological studies, cumulative dose dependent association between hydrochlorothiazide and NMSC has been observed. One study included a population comprised of 71,533 cases of BCC and of 8,629 cases of SCC matched to 1,430,833 and 172,462 population controls, respectively. High hydrochlorothiazide use (≥50,000 mg cumulative) was associated with an adjusted OR of 1.29 (95% CI: 1.23-1.35) for BCC and 3.98 (95% CI: 3.68-4.31) for SCC. A clear cumulative dose response relationship was observed for both BCC and SCC. Another study showed a possible association between lip cancer (SCC) and exposure to hydrochlorothiazide: 633 cases of lip-cancer were matched with 63,067 population controls, using a risk-set sampling strategy. A cumulative dose-response relationship was demonstrated with an adjusted OR 2.1 (95% CI: 1.7-2.6) increasing to OR 3.9 (3.0-4.9) for high use (~25,000 mg) and OR 7.7 (5.7-10.5) for the highest cumulative dose (~100,000 mg) (see Precautions).
Hydrochlorothiazide is a thiazide diuretic with antihypertensive activity. Its diuretic effect is due to inhibition of active Na+ transport from the renal tubules to the blood, affecting Na+ reabsorption.
Pharmacokinetics: Bisoprolol: Absorption: Tmax varies from 1-4 hours. Bioavailability is high (88%); hepatic first-pass extraction is very low; and absorption is not affected by the presence of food.
Kinetics are linear for doses from 5-40 mg.
Distribution: Plasma protein binding is 30%, and the volume of distribution is high (approximately 3 L/Kg).
Biotransformation: 40% of a bisoprolol dose is metabolized in the liver. Bisoprolol metabolites are inactive.
Elimination: The plasma elimination half-life is 11 hours.
Renal clearance and hepatic clearance are approximately comparable, and half of a dose (unchanged) as well as the metabolites are excreted in the urine. The total clearance is approximately 15 L/h.
Hydrochlorothiazide: Absorption: The bioavailability of hydrochlorothiazide shows between-subject variability and ranges from 60-80%. Tmax varies from 1.5-5 hours (mean >4 hrs).
Distribution: Plasma protein binding is 40%.
Elimination: Hydrochlorothiazide is not metabolized and is excreted almost entirely as unchanged substance by glomerular filtration and active tubular secretion. The terminal t½ of hydrochlorothiazide is approximately 8 hours.
The renal clearance of hydrochlorothiazide is reduced and the elimination half-life prolonged in patients with renal and/or cardiac insufficiency. The same applies to elderly subjects, who also show an increase in Cmax. Hydrochlorothiazide crosses the placental barrier and is excreted in human milk.
The pharmacodynamic effects, including hypokalemia (hydrochlorothiazide), and bradycardia, asthenia, and headache (bisoprolol) are dose-related. Combining both drugs at one-fourth/half the doses used in single-agent therapy (2.5 mg/6.25 mg) aims to reduce those effects.
Bisoprolol: Bisoprolol is a highly selective beta1-adrenoceptor blocking agent with no intrinsic sympathomimetic activity and without significant membrane-stabilizing activity.
As with other beta1-receptor blocking agents, the mechanism of bisoprolol's antihypertensive effect has not been completely established. However, it has been shown that bisoprolol produces a marked decrease in plasma renin and a reduction in heart rate.
Hydrochlorothiazide: Non-melanoma skin cancer: Based on available data from epidemiological studies, cumulative dose dependent association between hydrochlorothiazide and NMSC has been observed. One study included a population comprised of 71,533 cases of BCC and of 8,629 cases of SCC matched to 1,430,833 and 172,462 population controls, respectively. High hydrochlorothiazide use (≥50,000 mg cumulative) was associated with an adjusted OR of 1.29 (95% CI: 1.23-1.35) for BCC and 3.98 (95% CI: 3.68-4.31) for SCC. A clear cumulative dose response relationship was observed for both BCC and SCC. Another study showed a possible association between lip cancer (SCC) and exposure to hydrochlorothiazide: 633 cases of lip-cancer were matched with 63,067 population controls, using a risk-set sampling strategy. A cumulative dose-response relationship was demonstrated with an adjusted OR 2.1 (95% CI: 1.7-2.6) increasing to OR 3.9 (3.0-4.9) for high use (~25,000 mg) and OR 7.7 (5.7-10.5) for the highest cumulative dose (~100,000 mg) (see Precautions).
Hydrochlorothiazide is a thiazide diuretic with antihypertensive activity. Its diuretic effect is due to inhibition of active Na+ transport from the renal tubules to the blood, affecting Na+ reabsorption.
Pharmacokinetics: Bisoprolol: Absorption: Tmax varies from 1-4 hours. Bioavailability is high (88%); hepatic first-pass extraction is very low; and absorption is not affected by the presence of food.
Kinetics are linear for doses from 5-40 mg.
Distribution: Plasma protein binding is 30%, and the volume of distribution is high (approximately 3 L/Kg).
Biotransformation: 40% of a bisoprolol dose is metabolized in the liver. Bisoprolol metabolites are inactive.
Elimination: The plasma elimination half-life is 11 hours.
Renal clearance and hepatic clearance are approximately comparable, and half of a dose (unchanged) as well as the metabolites are excreted in the urine. The total clearance is approximately 15 L/h.
Hydrochlorothiazide: Absorption: The bioavailability of hydrochlorothiazide shows between-subject variability and ranges from 60-80%. Tmax varies from 1.5-5 hours (mean >4 hrs).
Distribution: Plasma protein binding is 40%.
Elimination: Hydrochlorothiazide is not metabolized and is excreted almost entirely as unchanged substance by glomerular filtration and active tubular secretion. The terminal t½ of hydrochlorothiazide is approximately 8 hours.
The renal clearance of hydrochlorothiazide is reduced and the elimination half-life prolonged in patients with renal and/or cardiac insufficiency. The same applies to elderly subjects, who also show an increase in Cmax. Hydrochlorothiazide crosses the placental barrier and is excreted in human milk.
MedsGo Class
Beta-Blockers / Diuretics
Please sign in so that we can notify you about a reply