Corynebacterium diphtheriae is a Gram-positive, non-spore forming, aerobic, rod-shaped and motile bacterium that causes diphtheria, an upper respiratory tract illness. They are pleomorphic organisms exhibiting different characteristic morphological shapes including V-shapes, irregular shapes and club-shapes.C. diphtheriae and other species in the genera Corynebacteria grow on the mucous membrane of the upper respiratory tract, skin, nares and wounds of humans. The bacterium is known to possess a characteristic irregular swelling at one end that contains polyphosphate inclusions called metachromatic granules.
Cells of Corynebacterium undergo snapping movement after cell division, and this brings them into characteristic forms that resembles Chinese letters because the bacterium lie at acute angles or equivalent to one another. C. diphtheriae is an airborne bacterial pathogen that is resistant to drying, and can be transmitted in human populations via nasal secretions.
Diphtheria, a strictly human disease is a highly infectious disease characterized by low fever, sore throat and infection is initiated following the inhalation of aerosolized secretions of infected individuals. C. diphtheriae is a toxin-producing bacterium that produces diphtheria toxin, an exotoxin that propagates the pathogenicity of the bacterium in vivo. Other strains of Corynebacterium diphtheriae that causes infections in humans include gravis, intermedius and mitis.
Though diphtheria still occurs in small proportions worldwide affecting both children and adults, the disease has been drastically controlled in the developed countries through the use of DTaP (diphtheria toxoid, tetanus toxoid, and acellular pertussis) vaccine. Total eradication in developing nations including Africa is still in progress as vaccination using the DTaP vaccine is yet to reach a global coverage. Diphtheria affects mostly children than adults, and it is a treatable and preventable bacterial infection.
PATHOGENESIS OF CORYNEBACTERIUM DIPHTHERIAE INFECTION
C. diphtheriae causes both local and systemic infections in humans. Local infections can occur in the tonsils, wounds, nose, conjunctiva and the pharynx while systemic infections may affect the kidneys, cardiac muscles of the heart, adrenal glands and the liver cells. Following the invasion of C. diphtheriae into the body through the respiratory route, the bacterium becomes deposited on the local tissues of the throat and tonsils.
C. diphtheriae harbours the β prophage that contains the tox gene responsible for the production of diphtheria toxin. β prophage is a temperate bacteriophage, and it is what controls the production of diphtheria toxin by C. diphtheriae. Diphtheria toxin contains two domains: the A and B domains. The A domain is the active chain of the toxin which invades the cell while the B domain is the binding chain of the toxin which binds specifically to host receptors, and provides the pathway for entry of the A chain that enters the cell.
Diphtheria toxin can cause the death of eukaryotic cells and tissues by inhibition protein synthesis in the host cells. After production, diphtheria toxin become absorbed by the damaged mucous membranes of the tonsils and throat, and this leads to destruction of epithelial cells coupled with an inflammatory reaction, all of which culminates to the formation of a grayish-white exudates called pseudomembrane that surrounds the tonsils, larynx and pharynx.
Pseudomembrane is a lesion that contains cells of C. diphtheriae and damaged host cells, and the manifestation of pseudomembrane on the tonsils, larynx and pharynx can eventually result in suffocation due to blockage of air passage. Swelling of the lymph nodes in the neck region can also occur, and profuse bleeding can ensue following the clinical attempt to remove the pseudomembrane. Death can occur if left untreated. Clinical signs and symptoms of diphtheria may include fever, cough, and discharge of thick mucopurulent secretions from the nares. Absorption and dissemination of diphtheria toxin via the blood leads to systemic infections which affects the kidneys, heart muscles, liver and spleen.
LABORATORY DIAGNOSIS OF CORYNEBACTERIUM DIPHTHERIAE INFECTION
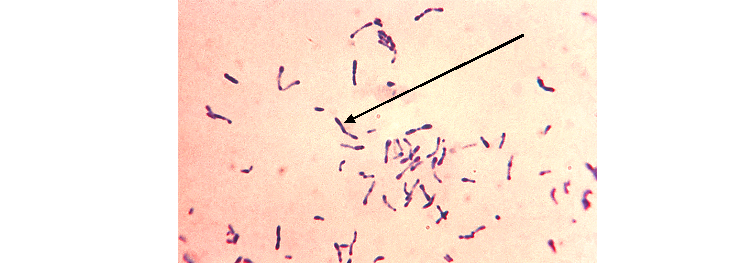
Laboratory diagnosis of C. diphtheriae infection is mainly dependent on identification of the pathogen from clinical specimens including throat and nose swabs. Physical examination of the throat and tonsil regions of infected patients for pseudomembrane appearance also aids diagnosis. Specimens are examined microscopically by Gram staining for the detection of beaded heads of C. diphtheriae containing metachromatic granules (Figure 1).
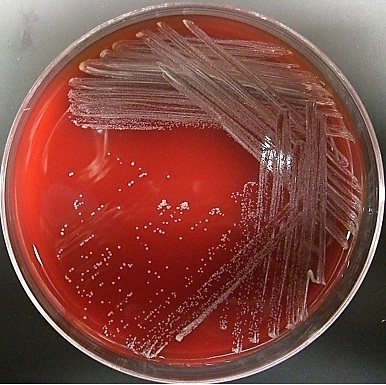
Bacterial culture in Loeffler serum medium and Tellurite blood agar are used for the primary isolation of C. diphtheriae from nose and throat swabs (Figure 2). PCR tests and serological tests including ELISA can also be used to diagnose the infection.
IMMUNITY TO CORYNEBACTERIUM DIPHTHERIAE INFECTION
Children are often susceptible to C. diphtheriae infection especially in regions where vaccination using DTaP is poor. Some level of active immunity can also develop in children and adults that have been previously exposed to the disease because natural infection with C. diphtheriae stimulate the production of antitoxin antibodies in affected individuals since the diphtheria toxin is antigenic in nature.
Massive artificial immunization of children at an early age after childbirth and booster doses in susceptible individuals with DTaP vaccine is ongoing in all parts of the world especially in developing countries where the disease is yet to be eradicated, and this trend will help to rollback the infection of C. diphtheriae in the world.
TREATMENT OF CORYNEBACTERIUM DIPHTHERIAE INFECTION
The antibiotics used for treating diphtheria include penicillin, erythromycin, clindamycin, gentamicin and vancomycin. Diphtheria antitoxin which counters the effect of diphtheria toxin in vivo can also be used in severe diphtheria infections. Early treatment of diphtheria using antibiotics and antitoxin will help to eliminate and neutralize the toxigenicity the pathogen.
PREVENTION AND CONTROL OF CORYNEBACTERIUM DIPHTHERIAE INFECTION
The control and prevention of diphtheria is largely dependent on sustained massive immunization of susceptible individuals using the DTaP vaccine. This approach will help to maintain a high level of active immunity in terms of herd immunity in a population and drastically reduce the spread and distribution of toxin-producing C. diphtheriae in a particular geographical area.
Since humans are the only known reservoir of C. diphtheriae, active immunization and boosters especially in children using the DTaP vaccine still remains the mainstay of preventing diphtheria. Antibodies produced in active immunization against C. diphtheriae is only directed against the toxin-producing structure of the pathogen, thus infection can still occur in immunized individuals but the episode will be mild without death as mortality only occurs in unimmunized individuals.
OTHER SPECIES OF CORYNEBACTERIA
- Corynebacterium ulcerans: C. ulcerans is an emerging pathogen that can cause zoonotic infections; and the bacterium causes diphtheria-like infections in humans. It can also cause skin infections.
- Corynebacterium pseudotuberculosis: C. pseudotuberculosis is the causative agent for human lymphadenitis, ulcerative lymphangitis (lymphangitis is an infection of the lower limbs of animals) in cattle, equine lymphangitis in horses, and caseous lymphadenitis in sheep and goats.
- Corynebacterium xerosis:C. xerosis is a commensal microorganism of the human skin and mucous membranes. It is infrequently responsible for human infections but the organism causes infections in immunocompromised hosts.
- Corynebacterium minutissimum: C. minutissimum, a normal skin inhabitantis associated with erythrasma, a type of skin rash – which typically presents as reddish-brown macular patches especially around the axillae and groins. It is more prevalent in diabetic patients.
- Corynebacterium striatum:C. striatum is an emerging nosocomial pathogen infrequently associated with wound infections, pneumonia and meningitis. It is a nondiphtherial Corynebacterium that is ubiquitous in nature and commonly colonizes the skin and mucous membranes of humans. C. striatum rarely cause any clinical infection in humans. Generally, they are considered as normal flora and not potentially pathogenic bacterium.
- Corynebacterium glucuronolyticum: C. glucuronolyticum is an increasingly recognized as opportunistic pathogen that is implicated in infections of the genital tract.
- Corynebacterium amycolatum:C. amycolatum isa nondiphtherial Corynebacterium that is commonly isolated from clinical samples; and the organism is an opportunistic pathogen capable of causing serious human disease such as endocarditis and sepsis in humans.
- Corynebacterium urealyticum: C. urealyticum is a urease-producing, opportunistic bacterium that is not commonly found in healthy people; and it is a common cause of urinary tract infection (UTI), pyelonephritis, cystitis or pyelitis especially in patients with chronic urological diseases.
- Corynebacterium jeikeium: C. jeikeium is an opportunistic pathogen that commonly colonizes the skin. It causes infection in immunocompromised hosts.
References
Brooks G.F., Butel J.S and Morse S.A (2004). Medical Microbiology, 23rd edition. McGraw Hill Publishers. USA. Pp. 248-260.
Madigan M.T., Martinko J.M., Dunlap P.V and Clark D.P (2009). Brock Biology of microorganisms. 12th edition. Pearson Benjamin Cummings Publishers. USA. Pp.795-796.
Prescott L.M., Harley J.P and Klein D.A (2005). Microbiology. 6th ed. McGraw Hill Publishers, USA. Pp. 296-299.
Ryan K, Ray C.G, Ahmed N, Drew W.L and Plorde J (2010). Sherris Medical Microbiology. Fifth edition. McGraw-Hill Publishers, USA.
Singleton P and Sainsbury D (1995). Dictionary of microbiology and molecular biology, 3rd ed. New York: John Wiley and Sons.
Talaro, Kathleen P (2005). Foundations in Microbiology. 5th edition. McGraw-Hill Companies Inc., New York, USA.