


INTRODUCTION
The periosteum is a thin layer of connective tissue that covers the outer surface of the bone in all places except at joints. It consists of two layers, the outer aspect is a fibrous layer, and the inner aspect is a cambium layer.1,2 The word cambium was coined by Duhamel comparing the growth pattern of a tree trunk.3 The progenitor cells develop into osteoblasts that are responsible for bone growth and fracture union.4–7 The primary goal of orthopedic surgeons in fracture management is the union of fracture, and they rely on intact periosteum. Periosteum, along with fracture hematoma, has been considered vital for fracture healing.8–11 How far traumatized periosteum contributes to fracture healing is still a matter of debate. Specifically, the layer of traumatized periosteum contributing significantly to fracture healing is yet to be ascertained. Without knowing the viability of the traumatized periosteum, its role in fracture healing is uncertain. The periosteum is always treated like a newborn baby during fracture fixation. This not only increases the surgical time for fracture fixation but, in many cases, leads to nonunion as no other additional procedure is advocated to promote union. The instances of nonunion can also be due to severe damage to the periosteum at the fracture site. Histologically, it is differentiated into three zones (Zone I, II, and III). Zone I is tightly adherent to the bone surface (innermost layer), primarily consisting of osteoblasts and smaller cells resembling fibroblasts.12 Zone II is a relatively translucent zone with many capillaries and less number of cells. Zone III consists of cells intermingled with collagen fibrils and fibrous tissue. The population of osteogenic cells in the cambium layer is morphologically distinct from fibroblasts.13 The microscopic examination of the periosteum from both palate and skull revealed a zonal organization with a variable overall thickness of each layer. The thickness of these zones varied greatly in absolute terms, but Zone I is always relatively thinner (10-20 /tm), whereas Zones II and III were several times thicker (20-80 /tm).14 The cambium layer is thickest in the fetus and becomes progressively thinner with age. In the adult, it is thin and cannot be distinguished from the overlying fibrous layer.15 Brownlow documented that raising the periosteum with cortical bone chips (Shingling) or with a periosteal elevator removed both layers of the periosteum and caused considerable damage to the surface of the cortex. Raising the periosteum with a sharp scalpel or simply pulling removed the fibrous layer leaving the osteogenic layer intact and adherent to the cortex.12,16 I presume separation of periosteum during fracture would be similar to that of merely pulling the periosteum. In this process, the inner layer remains attached to the bone surface, and the outer layer gets separated off the bone.
Lexer first suggested the importance of periosteal integrity in routine fracture healing.17 Free periosteal graft has been used in various nonunion and delayed union conditions of bones with a satisfactory outcome.18,19 Injury induces the release of growth factors and pluripotential mesenchymal cells from the undersurface of the periosteum, essential for fracture healing. The periosteum should always be preserved and protected during surgical management of a fracture.20 The periosteum provides mechanical support to the bone and amplifies the biomechanical capacity of intact long bones in bending, probably due to its fibrous and elastic properties.21 All these studies by eminent scholars have no documentation on the histology and anatomy of traumatized periosteum. Part of traumatized periosteum involved in fracture healing is not well known and needs to be evaluated.
MATERIAL AND METHODS
Closed fractures of long bone within the age group 20 years to 60 years who were operated on within 72 hours of fracture were included in the study. Fractures of femur or tibia managed by closed nailing were excluded from the study. Fractures like clavicle fracture, radius fracture, ulna fracture, humerus fracture, distal femur fracture, proximal or distal tibia fracture where the fracture was managed with open reduction and internal fixation were included in the study. We selected this age group of 20 years to 60 years because, with age, the periosteum becomes thinner and challenging to harvest. We included cases operated within 72 hours, as with time, there will be tissue response that may interfere with the histology of traumatized periosteum. As per patient fitness for surgery and pre-operative evaluation, we could operate some patients within 6 hours of the fracture without violating any operative protocol or ethical aspect. The study period was for six months as per the guideline of ICMR funded project. Within these six months after considering inclusion and exclusion criteria, 20 patients were enrolled in the study. After institute ethical permission and consent from the patient, six samples of 1cm*1cm periosteum at 1cm, 3cm, and 5cm proximal and distal to fracture site wherever practicable were harvested by a single orthopedic surgeon. We used periosteal elevators to harvest the periosteum. Where the periosteum is already peeled off by trauma, the appropriate size was harvested by mere cutting with a scissor. The biopsy specimen was transferred onto a bottle containing formalin and transported to the pathology laboratory. The pathologist, after gross examination of the sample, processed the sample in the following manner:
Fixing with 10% buffered formalin for 24 hours, labeling of sample, slicing, decalcification, and tissue processing. Tissue processing involves dehydration, clearing, blocking, sectioning, deparaffinization, fixation, staining with hematoxylin and eosin, and finally clearing with xylene wash.
RESULTS
The results of all 20 patients have been depicted in Tables 1 and 2. Out of 20 patients, we could harvest six samples in nine patients, five samples in three patients, four samples in four patients, and three samples in four patients. Loss of sample was either due to grossly ragged periosteum to harvest, fracture close to joint so not possible to harvest in one side of fracture or due to difficulty in fixing the sample. The periosteum was damaged in 11 sites which were difficult to harvest and send for histopathological examination. Occasionally it is ragged and difficult to differentiate from the surrounding lacerated tissue. Looking at their gross anatomy, the viability of the periosteum is questionable. Due to the above reasons, we could harvest and study only 97 samples instead of 120 samples from 20 fractured bones. The degree of damage to the periosteum depends on the degree of trauma that occurred at the time of fracture. Wherever the periosteum is on the surface of the bone, we had to separate it with the help of a periosteal elevator. Histology of the periosteum in all 97 samples from 20 patients revealed:
-
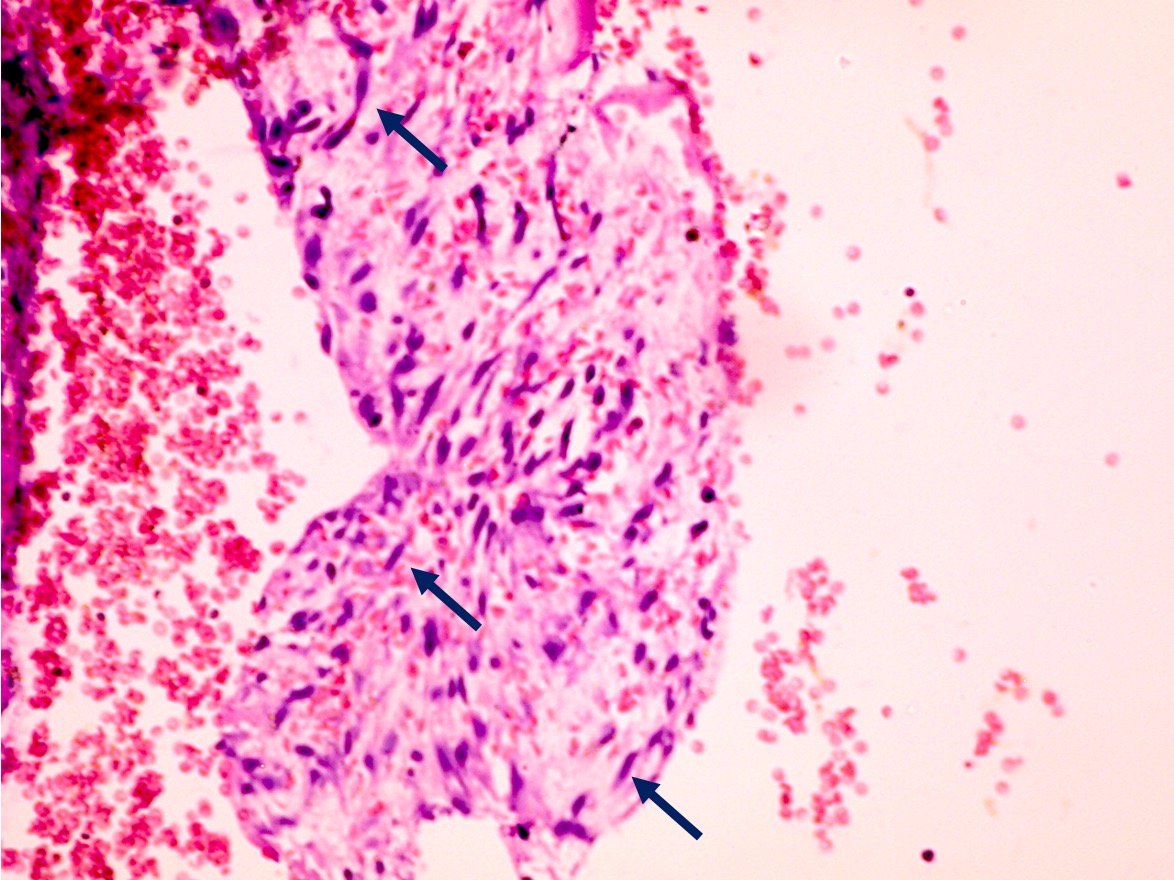
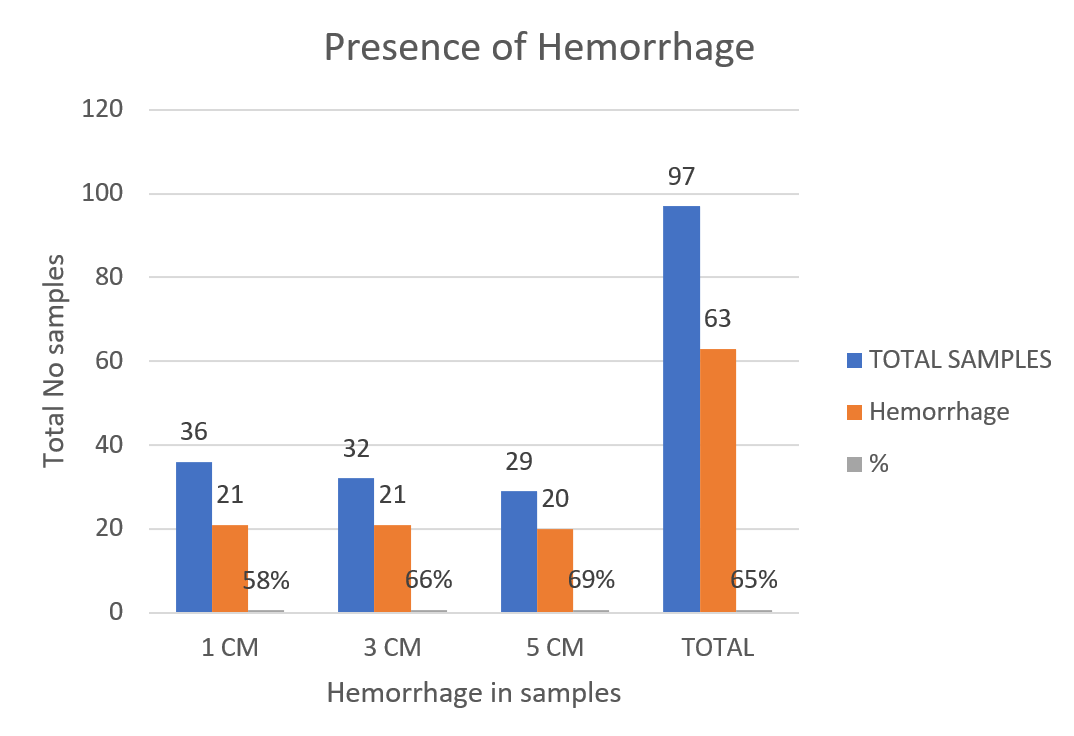
Hemorrhagic fields (Figure 4) were seen in 62 samples out of 97 samples. The degree of a hemorrhage depends on the degree of comminution of fracture, degree of violence that caused the fracture (Chart 1).
-
There were slides showing vessels and capillaries (Figure 4). It could be the vessels of a less traumatized Zone II layer of the periosteum or could be the neo-vascularization in the process of fracture healing. Some vessels were congested and dilated.
-
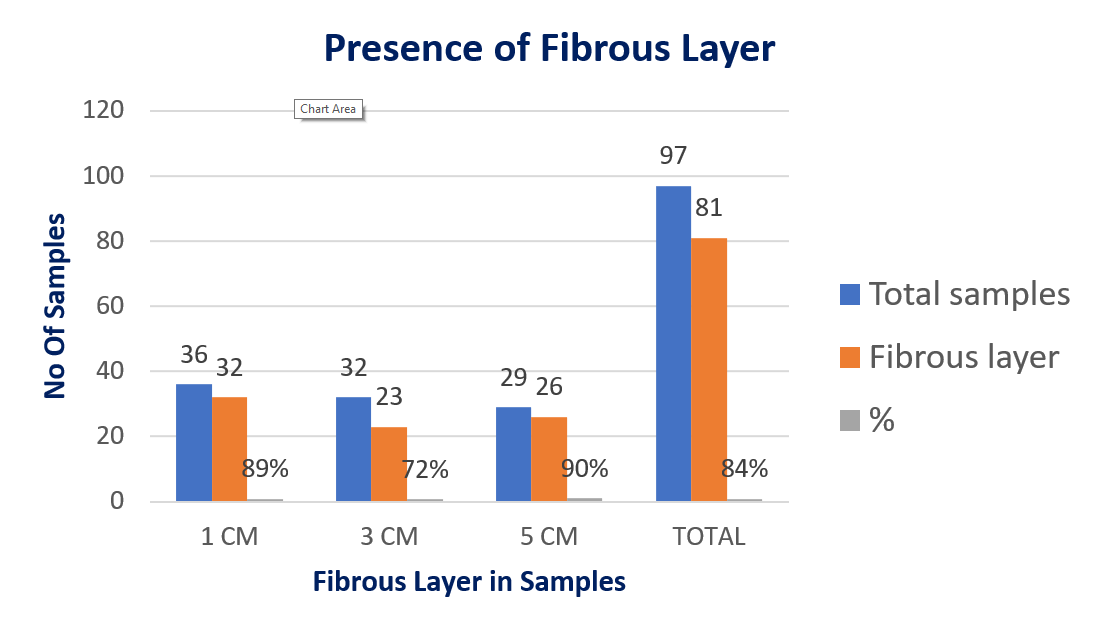
The outermost layer depicted mostly fibroblasts and fibrous connective tissue (Figure 3) (Chart 2). We could visualize the fibrous layer in most samples (81 samples out of 97, 84% of slides), but fibrocyte was not there in every sample (seen in 23 out of 97 samples, 24% of slides). Fibrocytes are long elongated cells, primarily seen in samples harvested 5 cm from the fracture site (Table 1).
-
Adipose tissue is seen sparsely in between the fibrous connective tissue. It is seen in 28 of 97 slides accounting for 29%. Adipocytes are primarily seen in slides 3cm and 5cm from the fracture site (Table 1).
-
Skeletal muscle fibers were seen in 50% of samples, which may be the remnants of skeletal muscle that remained attached to the outer surface of the periosteum during the process of harvesting the periosteum (Table 1).
-
Even microchips of bony tissue were observed in 4 samples, and this could be from the fractured bone and mostly in samples near the fracture site.
-
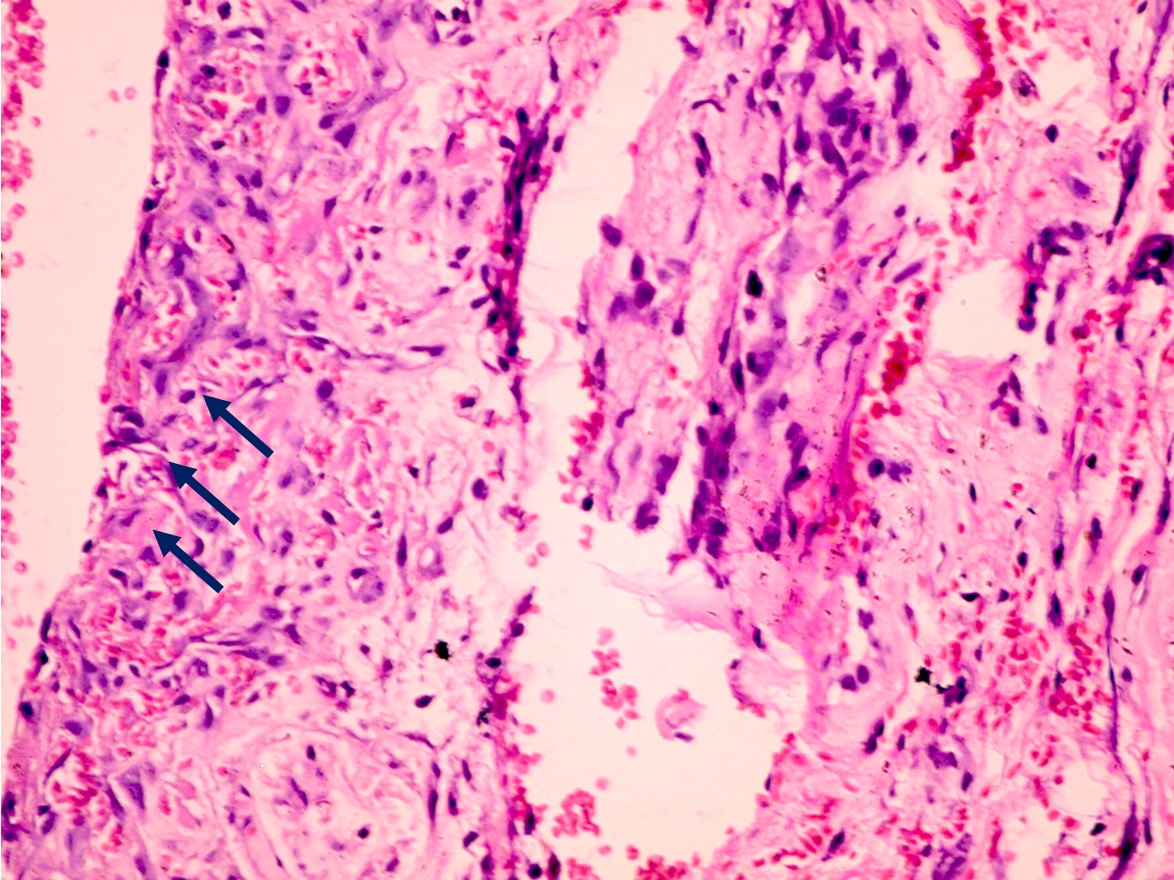
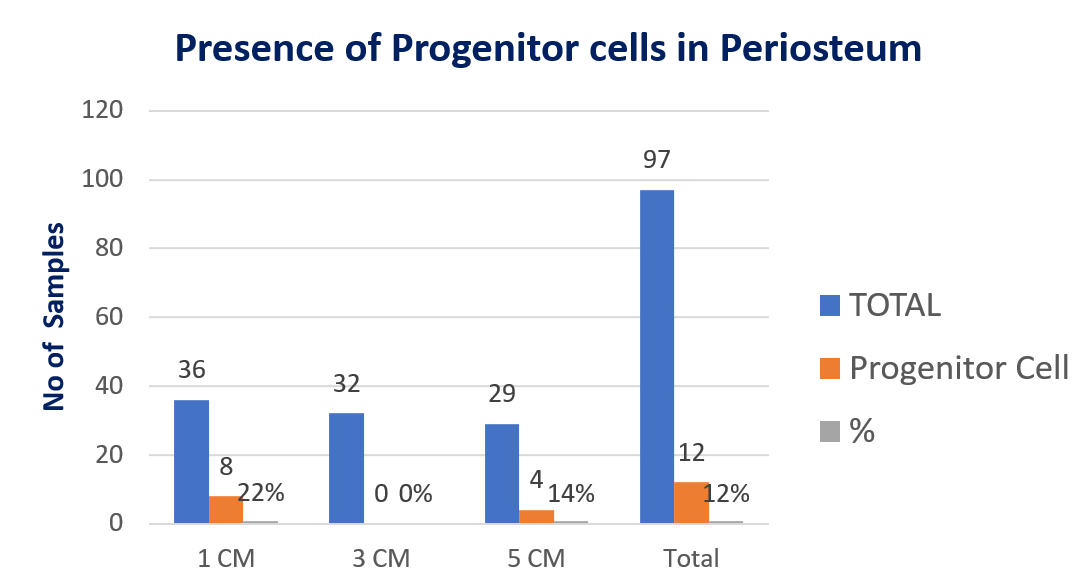
Osteoprogenitor cells (Figure 2) are triangular in shape seen only in 12 out of all 97 samples (Chart 4). Most of the slides are from 1cm or 5cm away from the fracture site. No slide at 3cm from the fracture site revealed any osteoprogenitor cells. These cells were arranged in sheets; it was a pure, simple fracture of clavicle operated within 6 hours of trauma. Wherever the osteoprogenitor cells were present, all were in the innermost layer of the harvested periosteum. The number of cells in the outer fibrous layer was negligible or countable compared to the periosteum’s innermost layer
-
The cambium layer (Figure 1, Chart 3) was seen in 13 slides near the fracture site with connective tissue and osteoprogenitor cells in some slides. All slides with the cambium layer did not reveal osteoprogenitor cells.








DISCUSSION
Studies have revealed the histology of periosteum into inner proliferative or cambial layer and outer fibrous layer; also, into three different zones (Zone I, II, and III). Zone I is the innermost cellular layer adjacent to the bone surface and tightly adherent to it. Zone III is the outermost fibrous layer. Zone II is a relatively translucent zone with many capillaries between Zone I and Zone III.1,12,13 Our finding simulates the previous outcome that most harvested periosteum lack cells and mainly consist of fibrous tissue and blood-filled capillaries. There were many colloid congested vessels along with areas of hemorrhage depicting the degree of trauma during fracture. Comparing the three zones, Zone I is thinnest and inseparable from the bony surface. It was challenging to separate Zone I from the bone surface, as we experienced while harvesting with a periosteal elevator.
Similar to our study, previous studies have mentioned that Zone I is very thin and tightly adherent to the bony surface and is the most cellular layer of the periosteum. Our study depicts the degree of damage to the periosteum as there were few cells in many samples and mostly consisted of hemorrhagic and fibrous tissue. We still doubt the viability of the periosteum with such a degree of bleeding. The presence of skeletal muscle tissue depicts the secure attachment of muscles to the periosteum. The number of osteocytes was sparse, as all the samples harvested were within 72 hours of fracture. Maybe the osteocytes are formed later in the process of fracture healing. Whether the separated outer layer or the adherent layer to the bony surface is vital for fracture healing is debated. From our study, we presume a minor role of the outer layer of the periosteum in terms of osteogenesis. But definitely, it has a role in fracture healing, mainly in the containment of fracture hematoma and the supply of fibroblasts and pericytes that transform to progenitor cells in the process of fracture healing. We believe the layer of periosteum that is tightly adherent to the bone surface is highly cellular, has maximum contribution to fracture healing. It has progenitor cells, and there may be a need to transform fibroblast to osteocytes for fracture healing. In our opinion, the bone-ends in a fracture have to be dealt with like a newborn baby rather than the separated traumatized periosteum at the fracture site. Methods of indirect fracture reduction can be adopted in treating fracture managed by open reduction and internal fixation. Less use of periosteal elevator too can decrease the damage to the innermost layer of the periosteum as periosteal elevator causes more damage to the innermost layer of the periosteum and the underlying cortex.19 We suggest using a scalpel or gentle pulling of periosteum from the bone surface during fracture fixation. This may allow more viable osteocytes available for fracture healing. Respecting the whole periosteum in fracture fixation is mandatory for fracture union. We presume an active part of periosteum, i.e., the Zone I vital for fracture union whose further damage should be avoided.
CONCLUSION
The innermost layer of the periosteum, which is tightly adherent to the bony surface, is vital for fracture healing. Fracture leading to separation of periosteum from bony surface spares this layer, which remains attached to the bony surface. Most osteoprogenitor cells lie in the innermost layer that accounts for fracture healing and new bone formation. Our study shows that part of traumatized periosteum, which is usually detachable from the bone surface, consists of mainly fibrous tissue, hemorrhagic tissue, and few cells. Using a periosteal elevator on the bone surface during fracture fixation further damages the periosteum’s innermost layer. Using a scalpel to separate the periosteum or merely pulling it away from the bone surface will decrease damage to the inner cambium layer. We found osteoprogenitor cells only in 12 samples out of 97 samples. Mostly the outer layer is structural, supporting the bone, giving attachment to muscles, and containment of fracture hematoma that helps in fracture union. Our results and previous studies suggest not using periosteal elevators or giant bone holders and clamps during fracture fixation. Fracture reduction can be achieved indirectly at least 5 cm away from the fracture site and using a scalpel to elevate the periosteum. Respecting the periosteum is vital for fracture healing; understanding the periosteum, avoiding periosteal elevators, and giving more importance to the inner layer of the periosteum is the only message we would receive to convey to future scholars and Orthopedic surgeons.