- Etiology: malignant neoplasm of striated muscle
- Imaging: arise from bladder or prostate or vagina
- MRI: intermediate to hypointense on T1WI, intermediate to hyperintense on T2WI, enhances heterogeneously, improved conspicuity on DWI
- Complications: metastasis to lung
- Clinical: most common childhood soft tissue sarcoma, 50% head and neck / 30% genitourinary / 20% musculoskeletal, embryonal cell type seen in infants is most common, alveolar cell type seen in older children and affects musculoskeletal system and is more aggressive, orbital has best prognosis
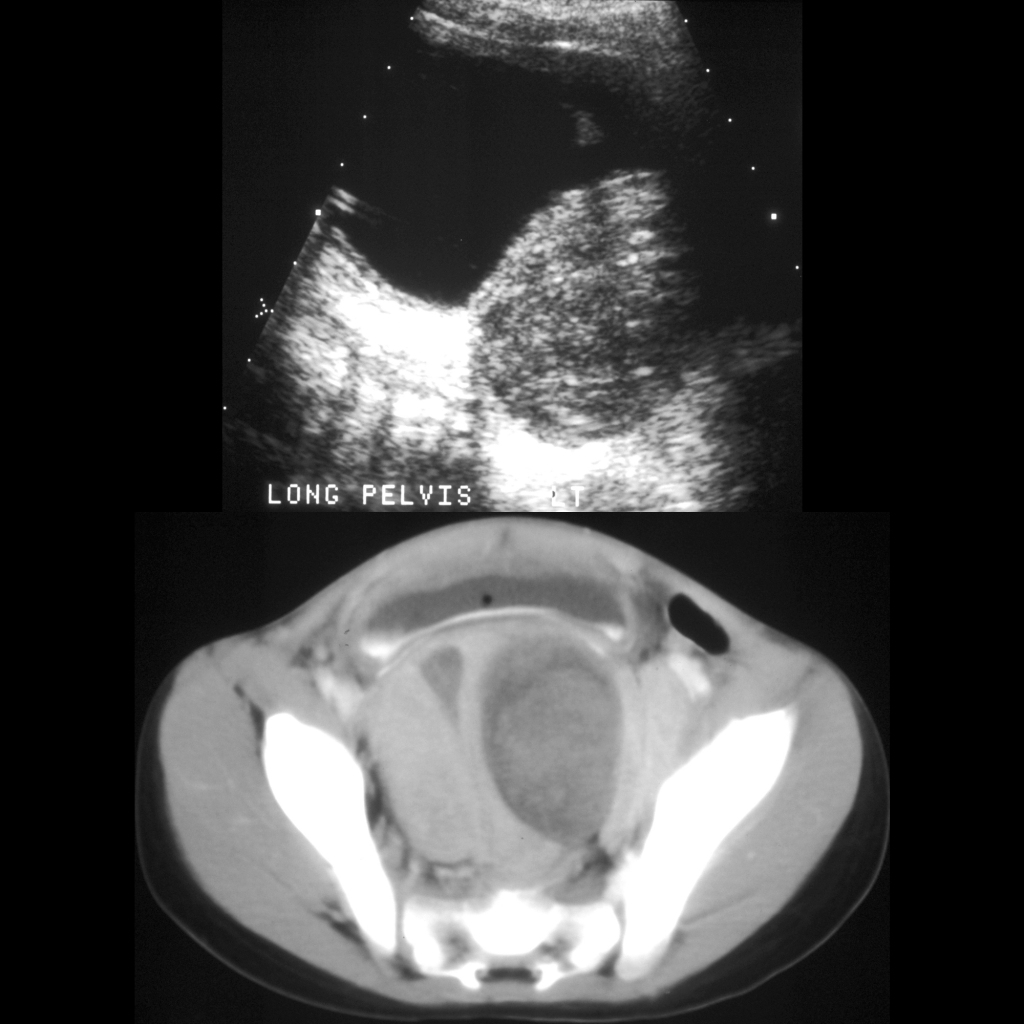
Radiology Cases of Genitourinary Rhabdomyosarcoma
Radiology Cases of Bladder Rhabdomyosarcoma

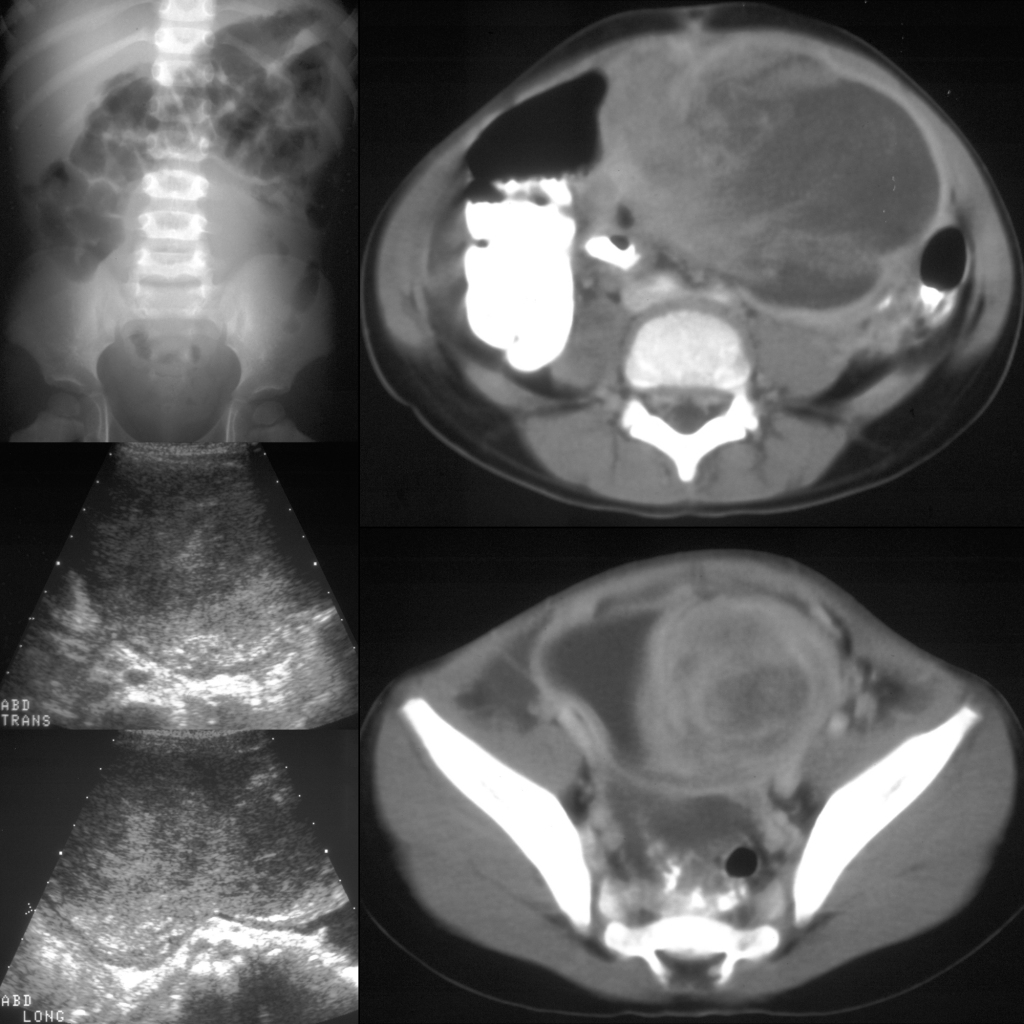
Radiology Cases of Prostatic Rhabdomyosarcoma

Clinical Cases of Genitourinary Rhabdomyosarcoma
Clinical Cases of Sarcoma Botryoides

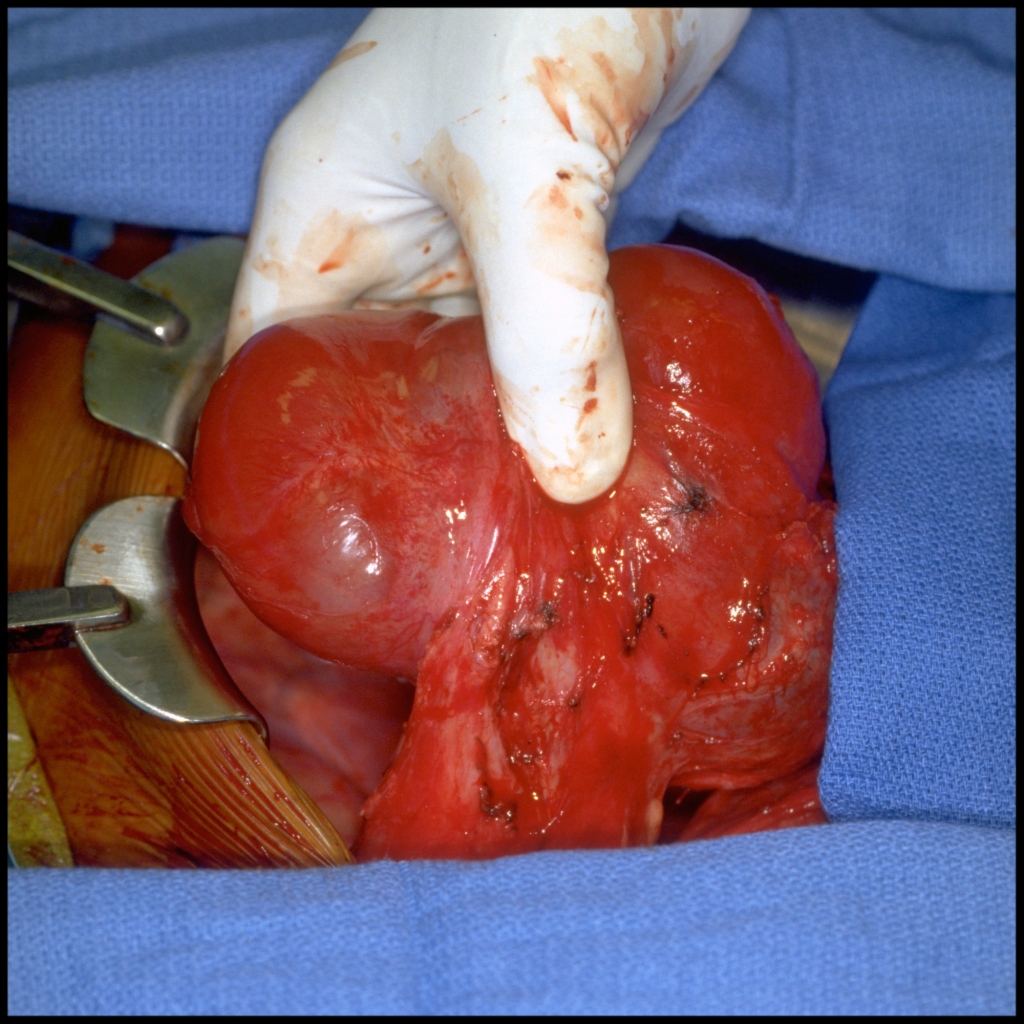
Surgery Cases of Genitourinary Rhabdomyosarcoma
Surgery Cases of Bladder Embryonal Rhabdomyosarcoma
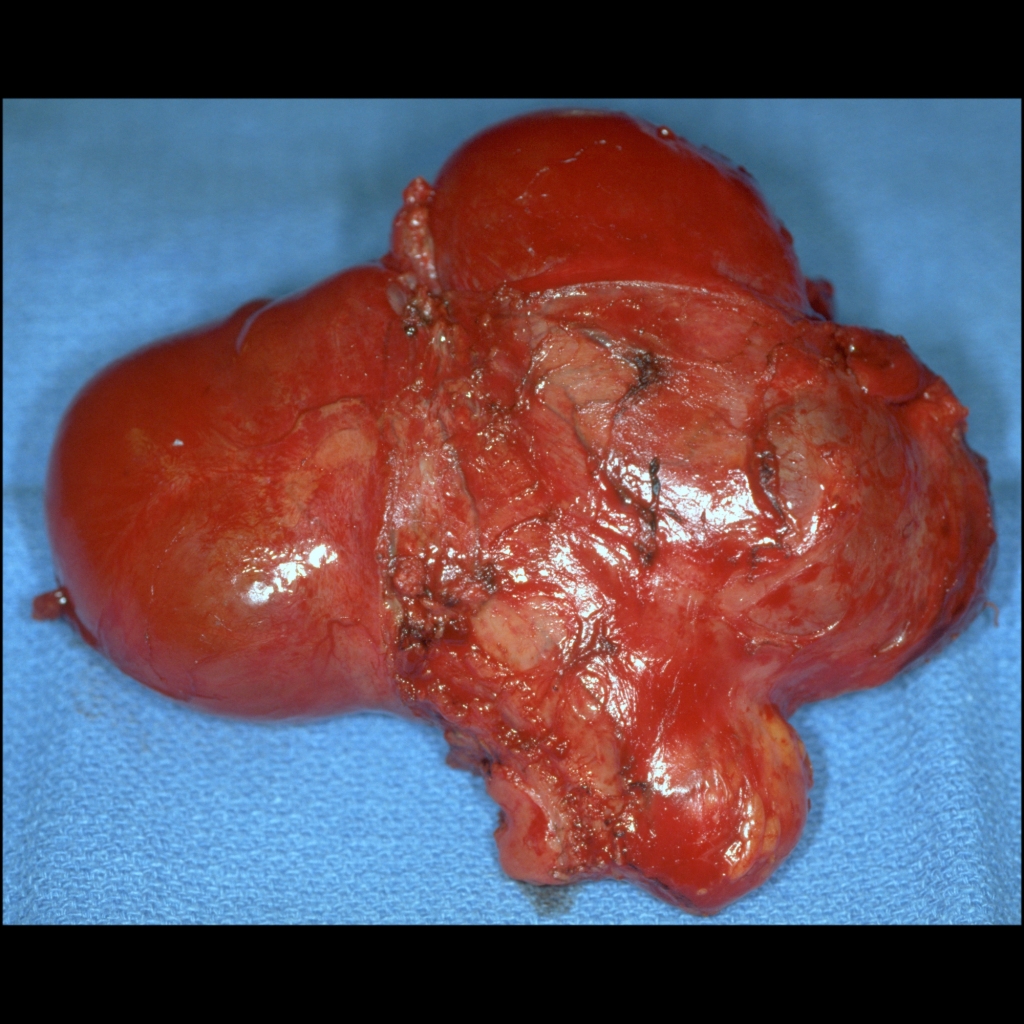
Gross Pathology Cases of Genitourinary Rhabdomyosarcoma
Gross Pathology Cases of Bladder Embryonal Rhabdomyosarcoma
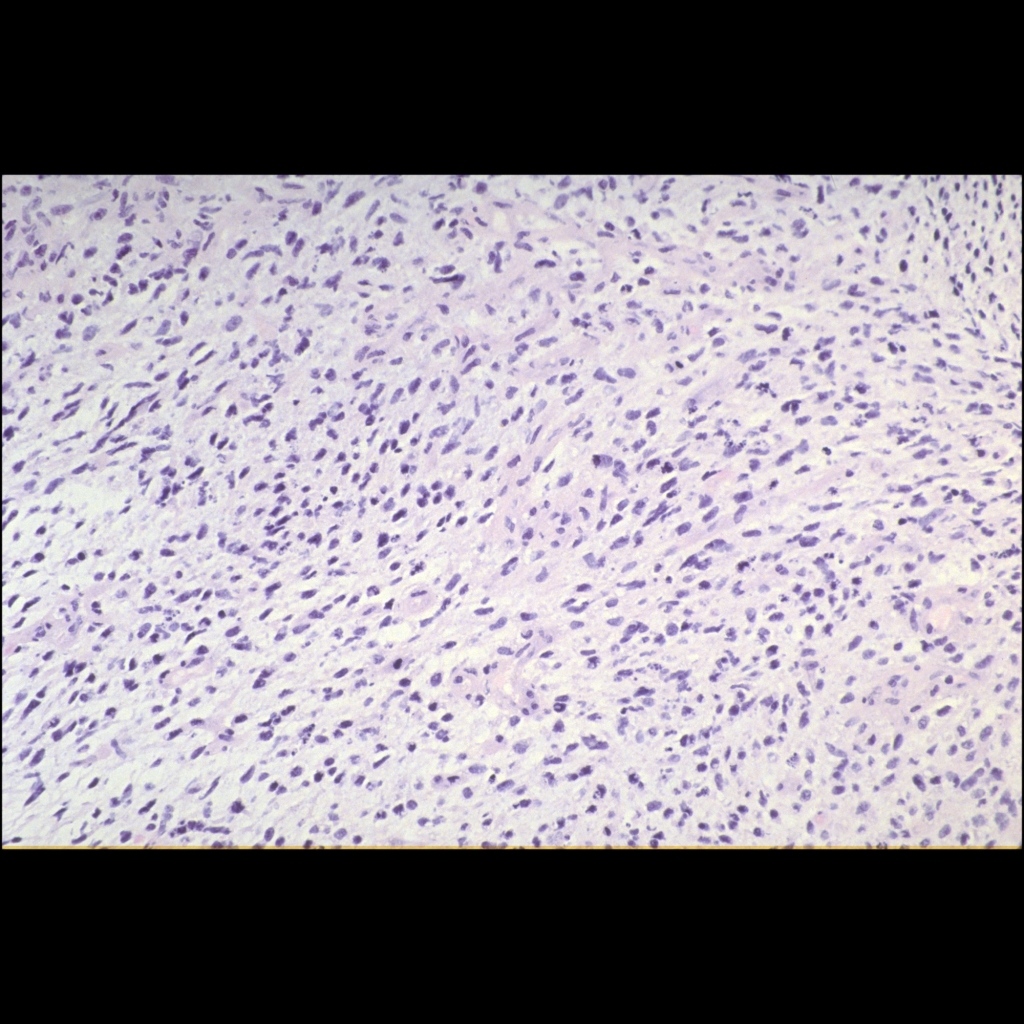
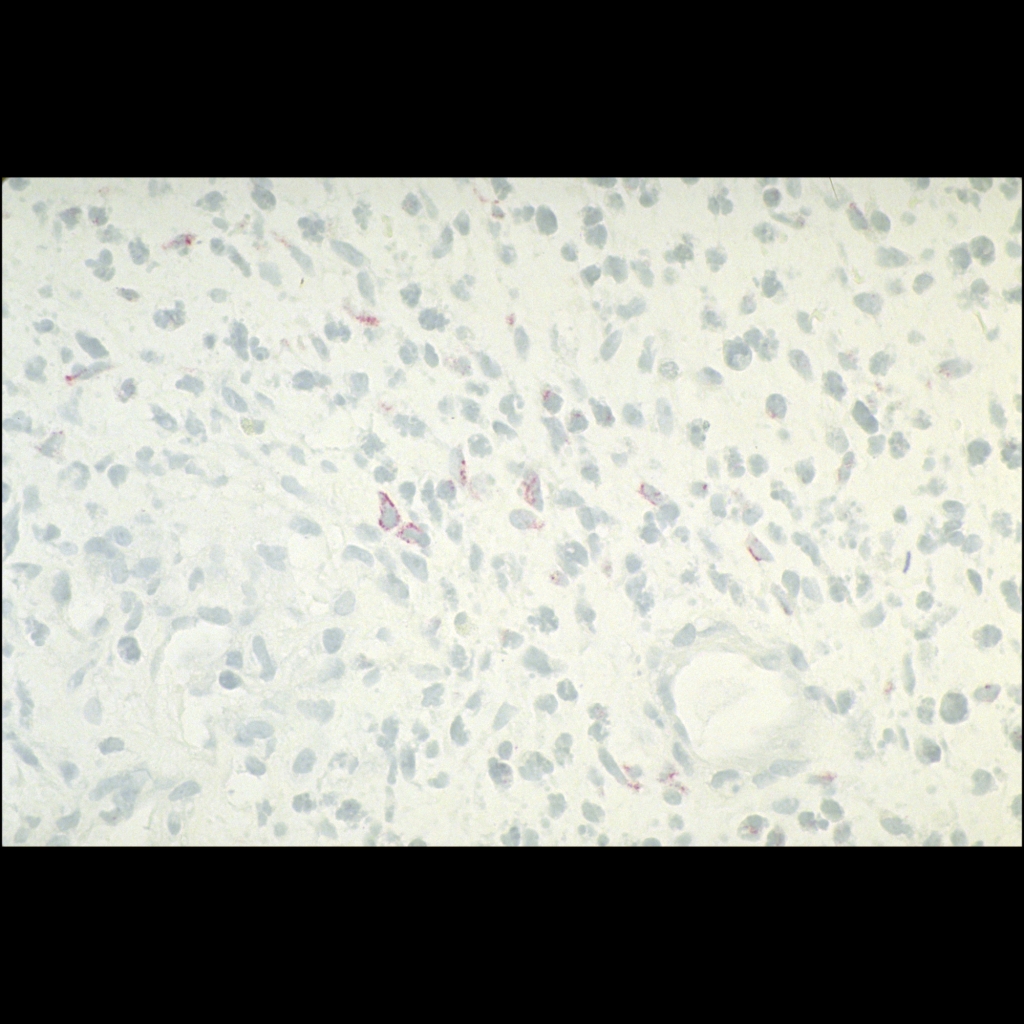
Histopathology Cases of Genitourinary Rhabdomyosarcoma
Histopathology Cases of Bladder Embryonal Rhabdomyosarcoma