- Etiology: pharyngitis or upper respiratory infection -> retropharyngeal adenitis -> supprative lymph node rupture into retropharyngeal space -> abscess, bacterial
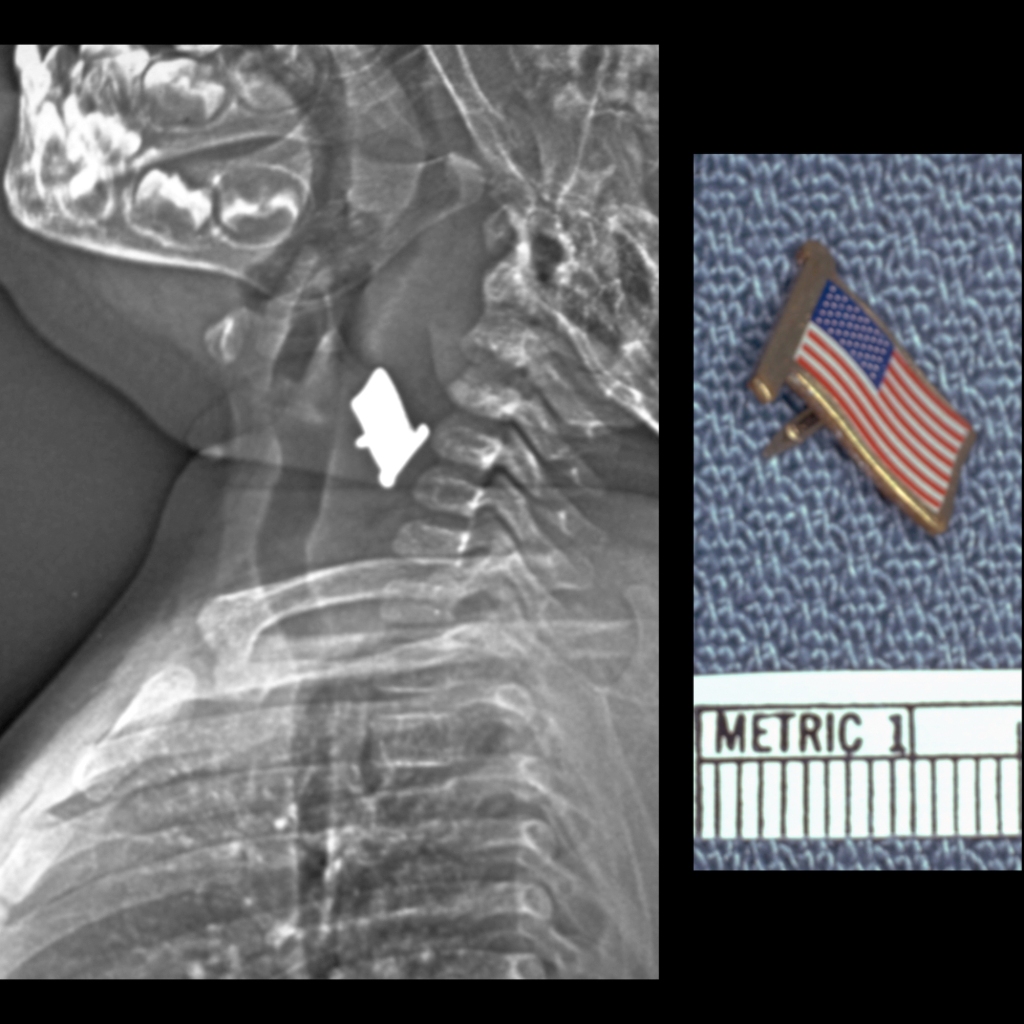
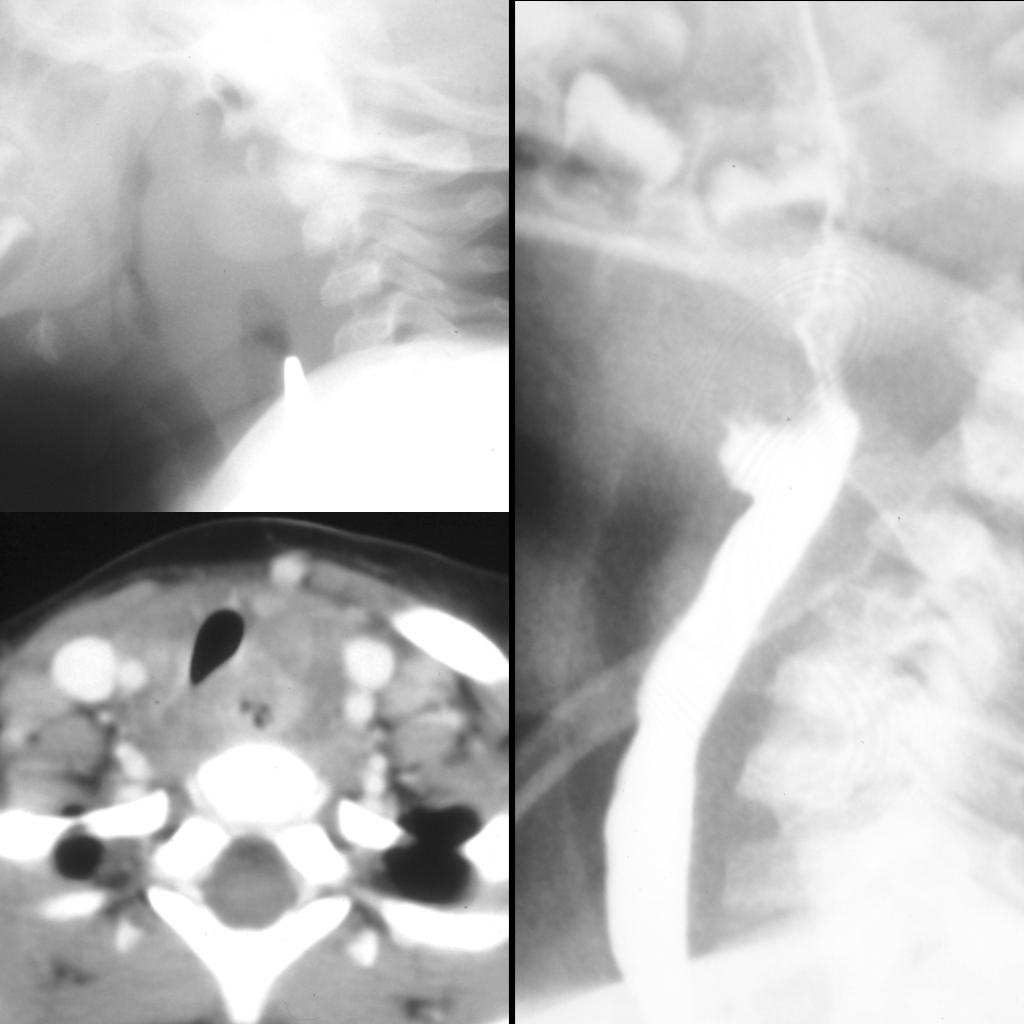
- Imaging: normal prevertebral space is < 1/2 vertebral body at C2, soft tissue thickening of > 1 cervical vertebral body, to diagnose retropharyngeal mass need inspiratory image taken in extension, measurements less important than whether retropharynx changes with respiration, always look for retained foreign body
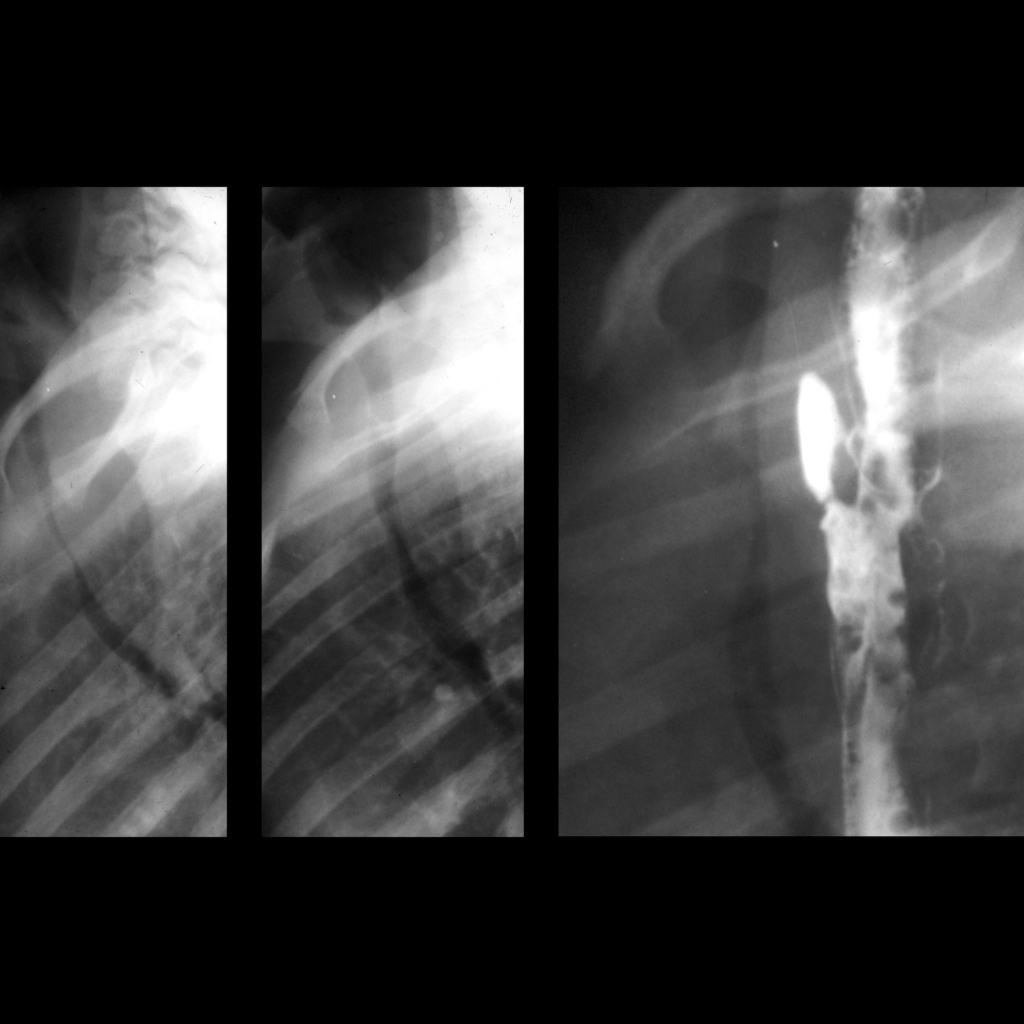
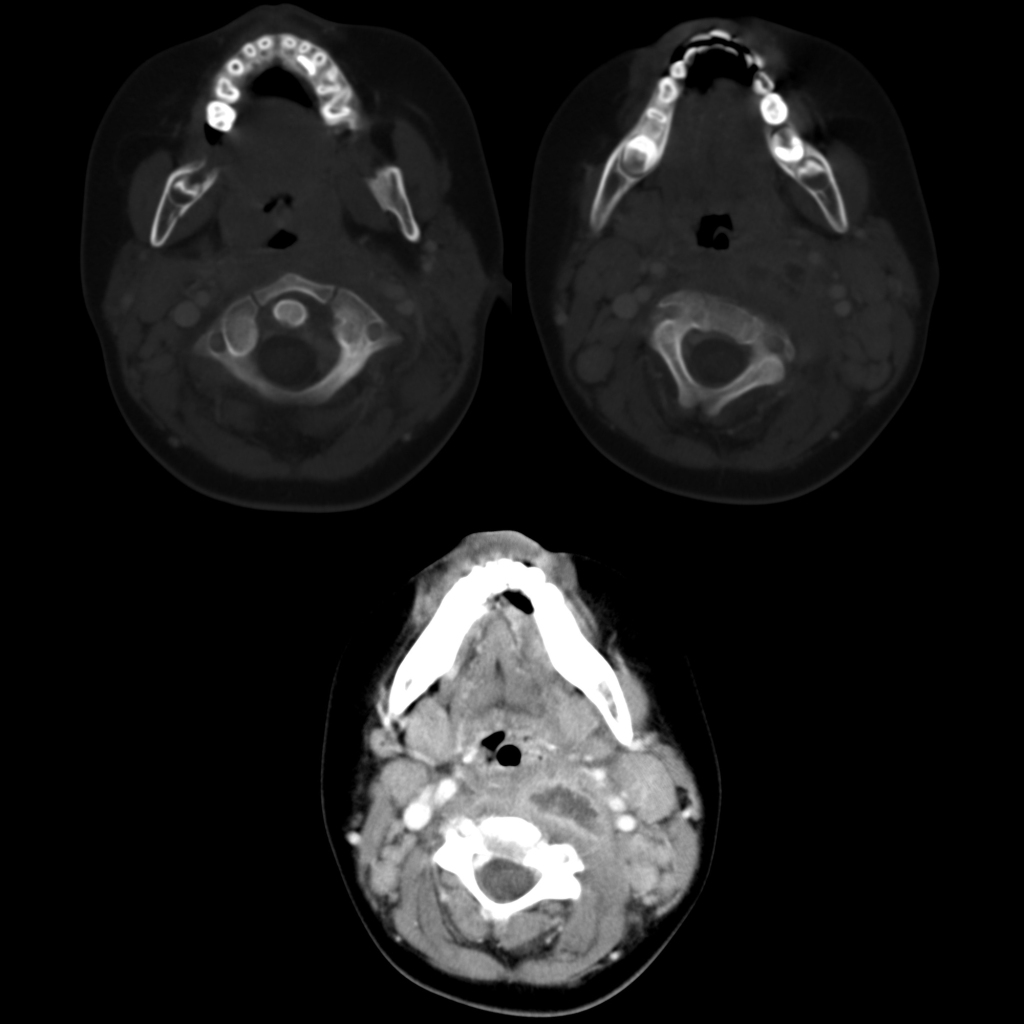
- CT: helpful to look for complications – size of abscess, vascular complication, mediastinal extension
- DDX: pseudothickening – physiological tracheal buckling which can be seen on lateral neck images obtained on expiration + flexion – so beware of false positives due to expiration / flexion – airway radiograph should always be taken in inspiration + extension, retropharyngeal cellulitis / phlegmon, penetrating trauma, vertebral osteomyelitis, mass, anasarca
- Complications: airway compression, arteritis, jugular vein occlusion (Lemierre syndrome), atlanto-axial rotatory subluxation, extension into mediastinum
- Treatment:
- Clinical: seen in infancy and young children – 6 months to 6 years (older children + adults have peritonsillar + parapharyngeal abscess), 50% cases between 6-12 months, fever / stiff neck / dysphagia / stridor
Radiology Cases of Retropharyngeal Abscess

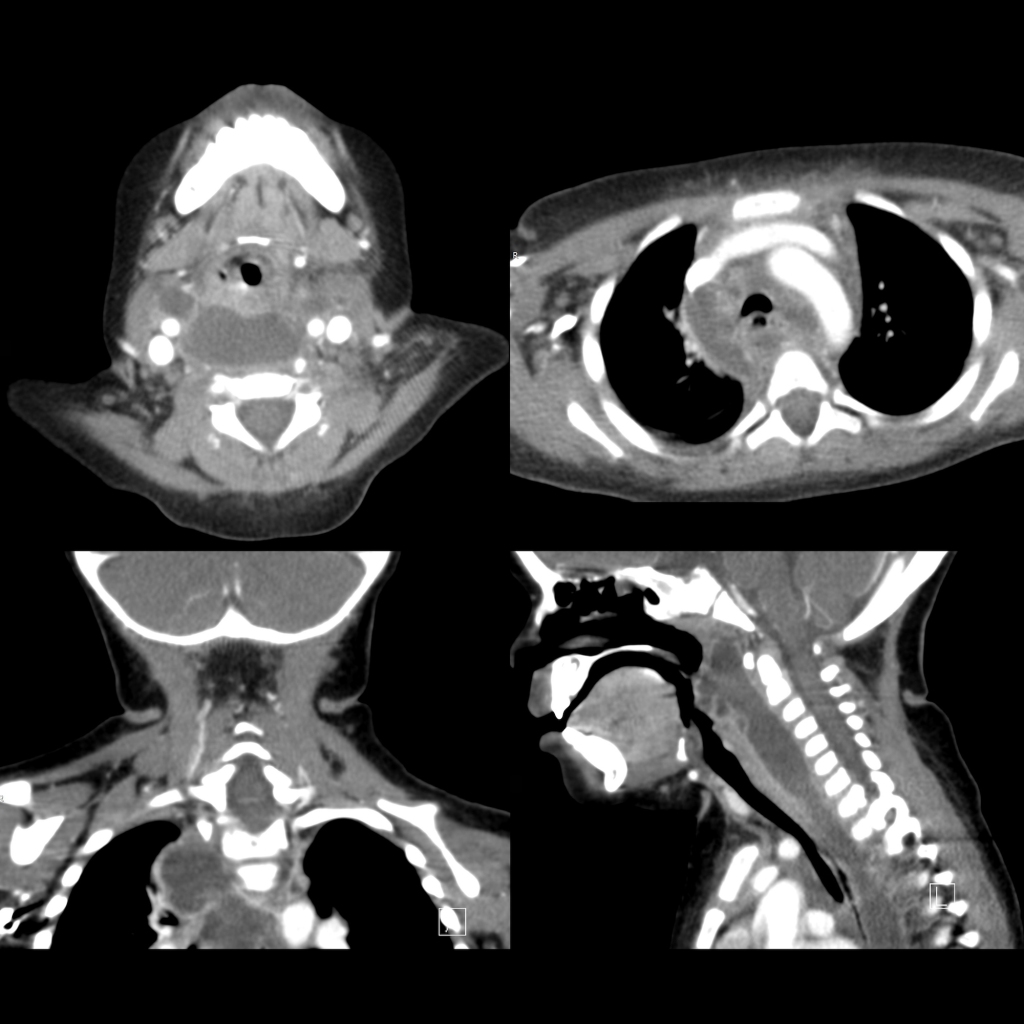
Radiology Cases of Chronic Gastrointestinal Foreign Body Causing Retropharyngeal Abscess