- Etiology: renal origin, 30% of unilateral and 100% of bilateral Wilms tumor are due to nephrogenic rests
- Imaging screening: in hemihypertrophy and Beckwith Wiedemann syndrome – baseline at 6 months, get US every 3 months until 8 years old, becoming larger or rounder suggests malignant degeneration
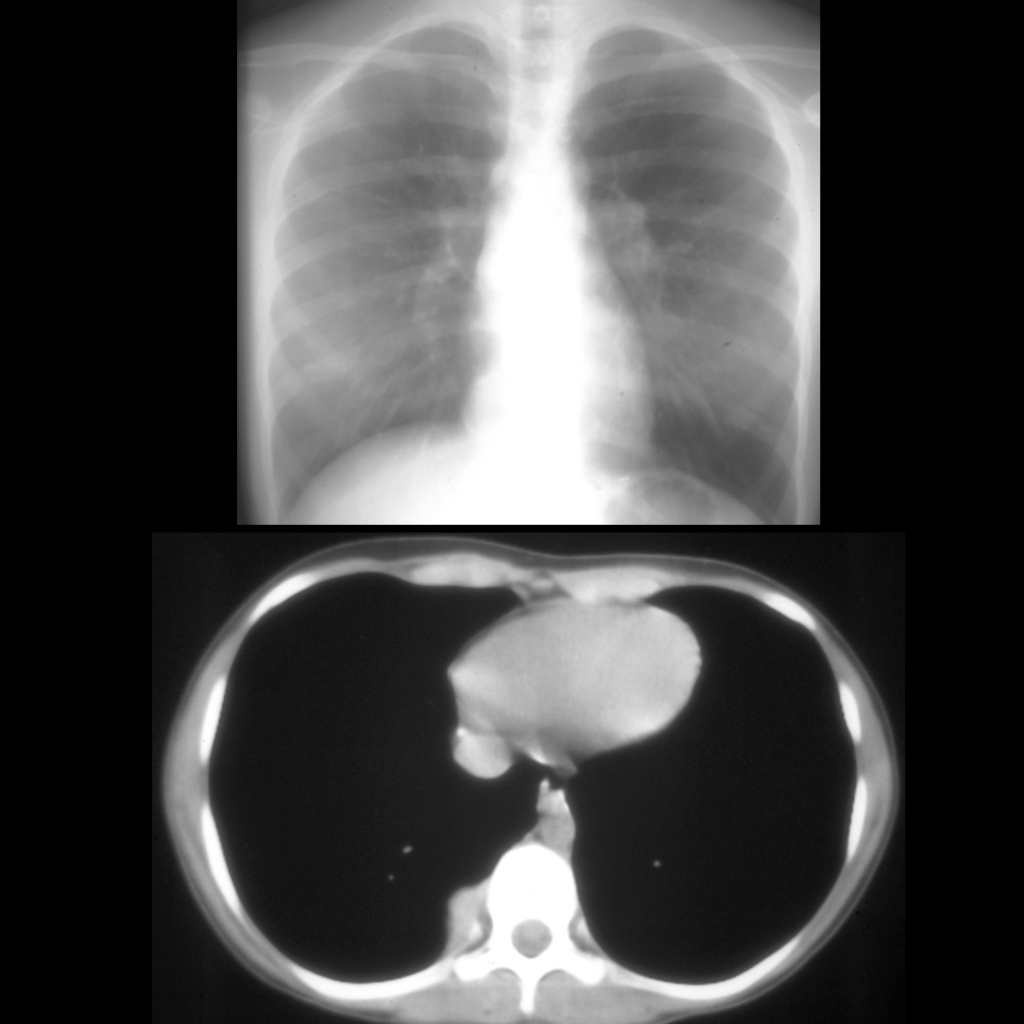
- Imaging at presentation: establish the stage of tumor – local / locoregional / metastatic, look for tumor rupture and ipsilateral / contralateral synchronous tumor and vascular invasion in renal vein and IVC, chest CT for pulmonary metastatic disease, MRI superior for detecting bilateral renal disease
- Imaging: well circumscribed, round, heterogenous, some cystic components, may contain small amounts of fat, fine calcifications in 9%, multicentric in 10-15%, enhance less than normal parenchyma, venous invasion, claw sign, deforms the collecting system showing it is an intrarenal mass, pushing tumor that displaces vessels
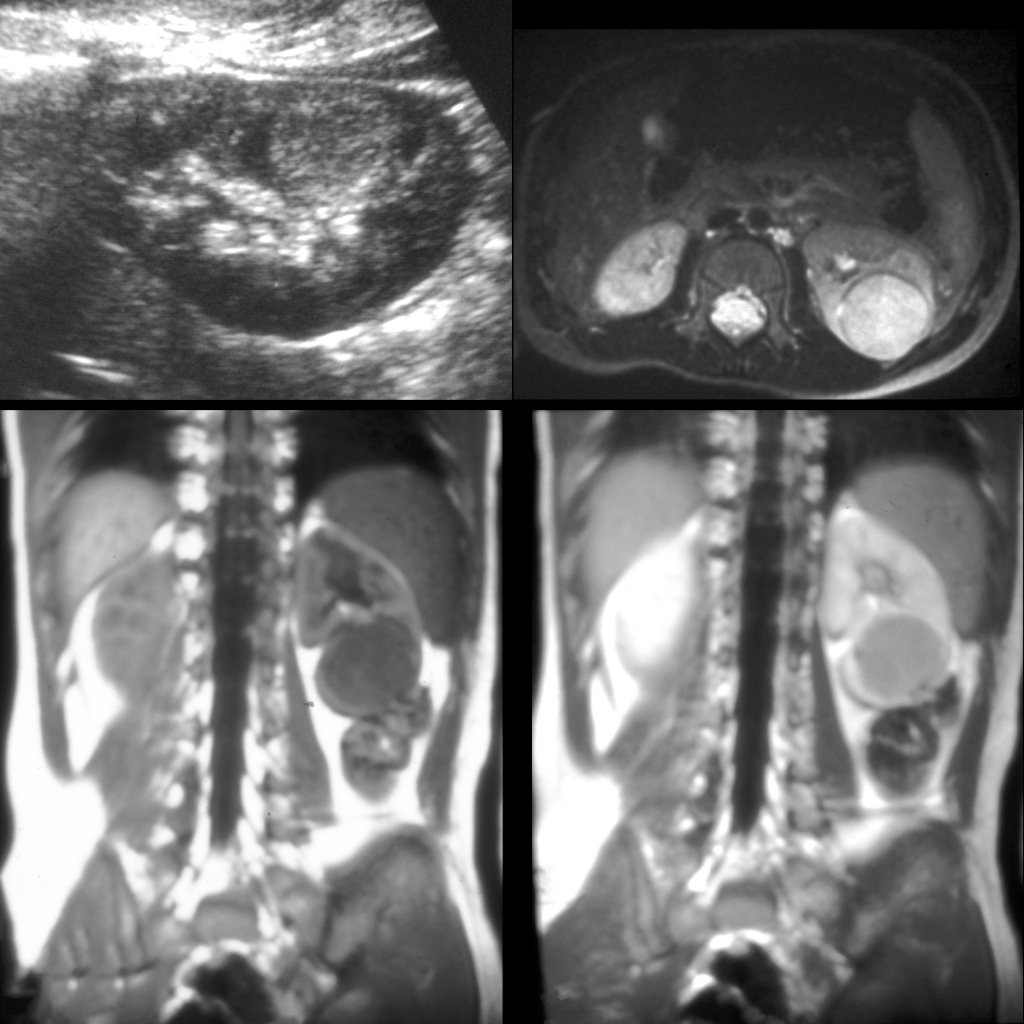
- MR: T1 isointense and T2 hyperintense
- Complications: regional lymph nodes, renal vein / inferior vena cava / right atrium tumor thrombus, contralateral kidney – synchronous or metachronous 10%, metastasis to lung / liver / bone in 12%
- Clinical: most common abdominal malignancy of childhood, 87% of kidney masses in children, peak at 3 1/2 years, 80% < 5 years, rare in neonates, palpable mass in 75-95%, presentation most commonly as palpable mass and infrequently with pain / hematuria / constitutional symptoms, associated with Beckwith-Wiedemann syndrome (macroglossia, omphalocele, visceromegaly – liver / kidneys / pancreas, gigantism / hemihypertrophy / Wilms tumor in 10%), bilateral Wilms is virtually always genetic or syndrome associated
Radiology Cases of Wilms Tumor
Radiology Cases of Unilateral Wilms Tumor
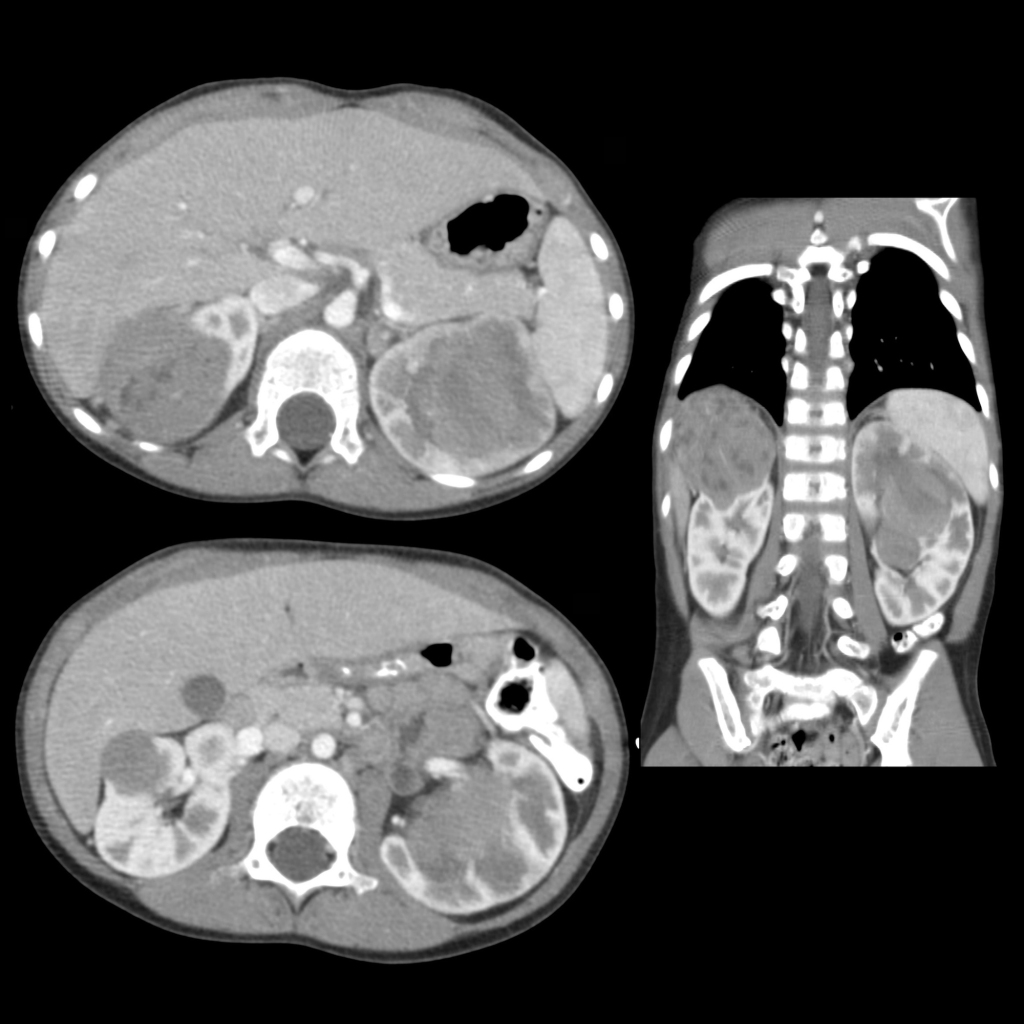
Radiology Cases of Bilateral Wilms Tumor
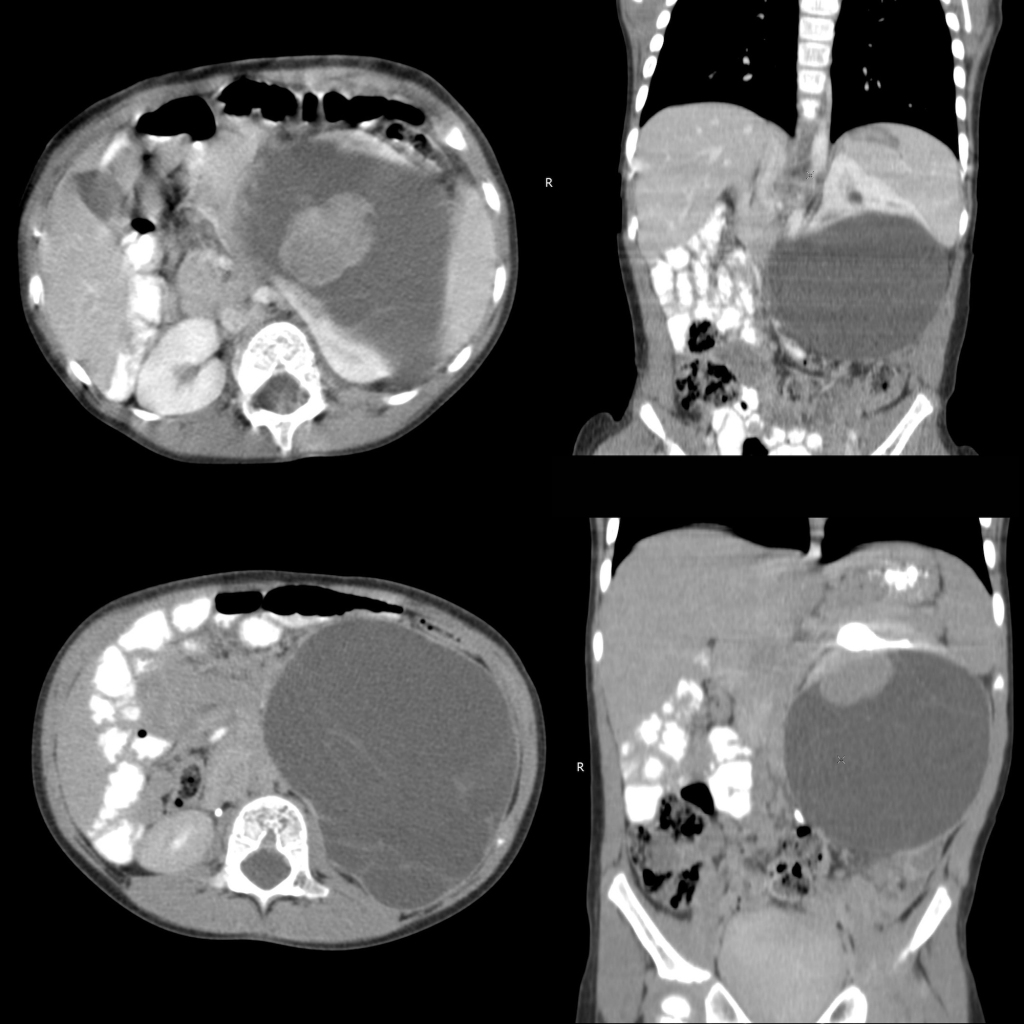
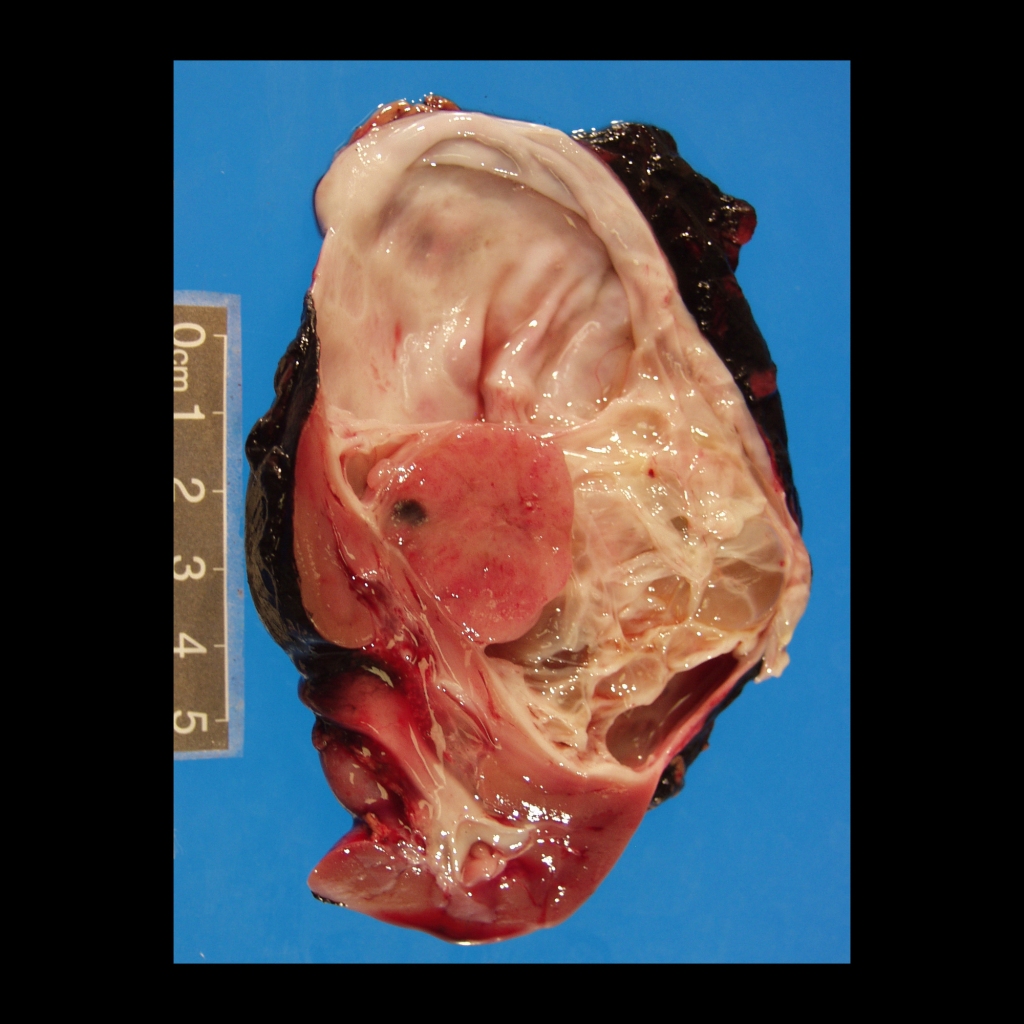
Radiology Cases of Cystic Wilms Tumor
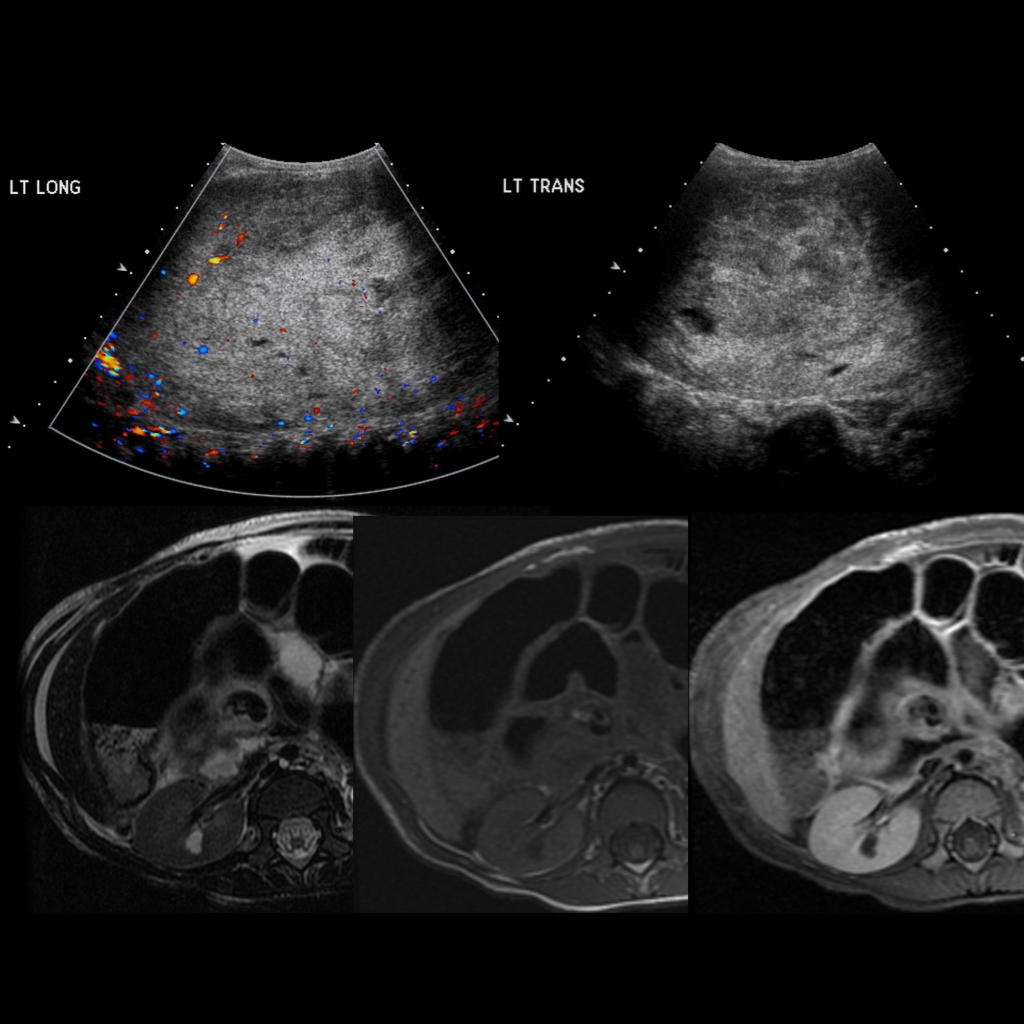
Radiology Cases of Wilms Tumor in the Left Kidney and Nephroblastomatosis in the Right Kidney
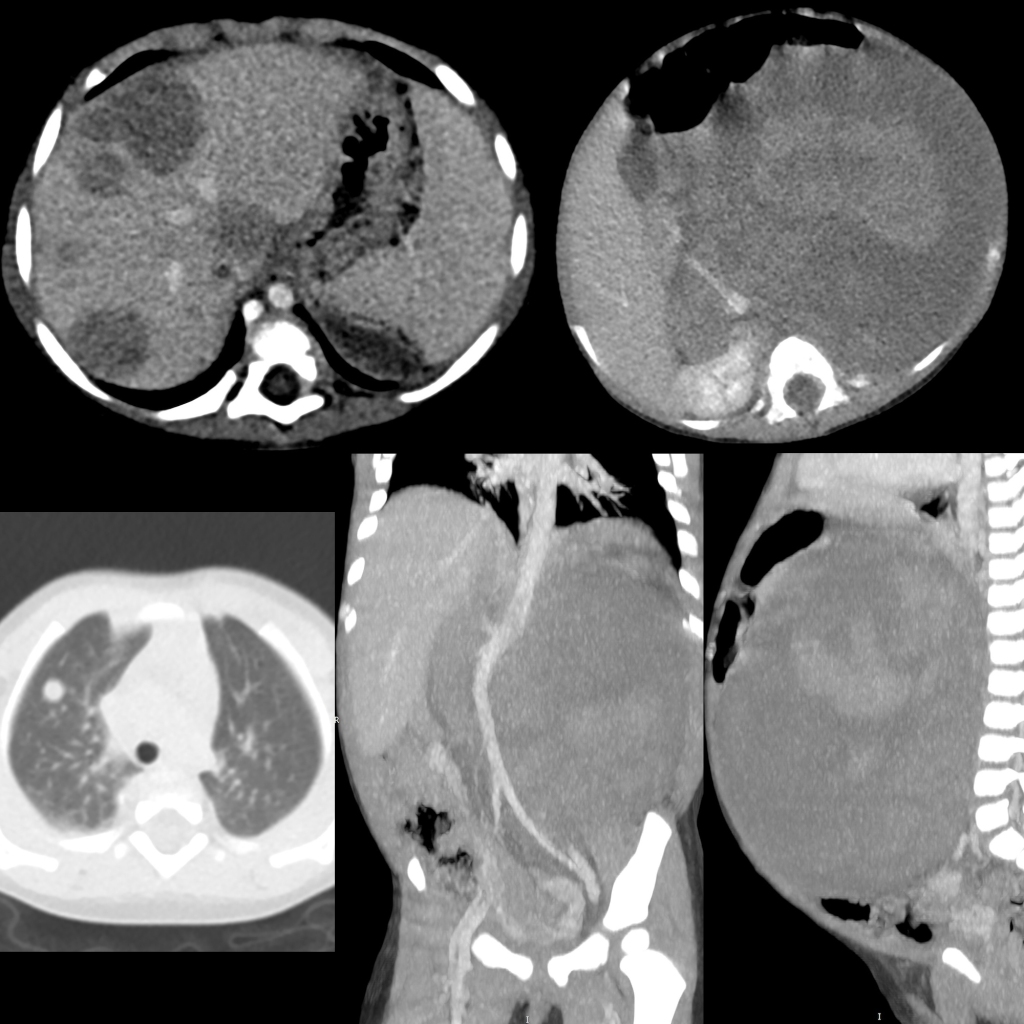
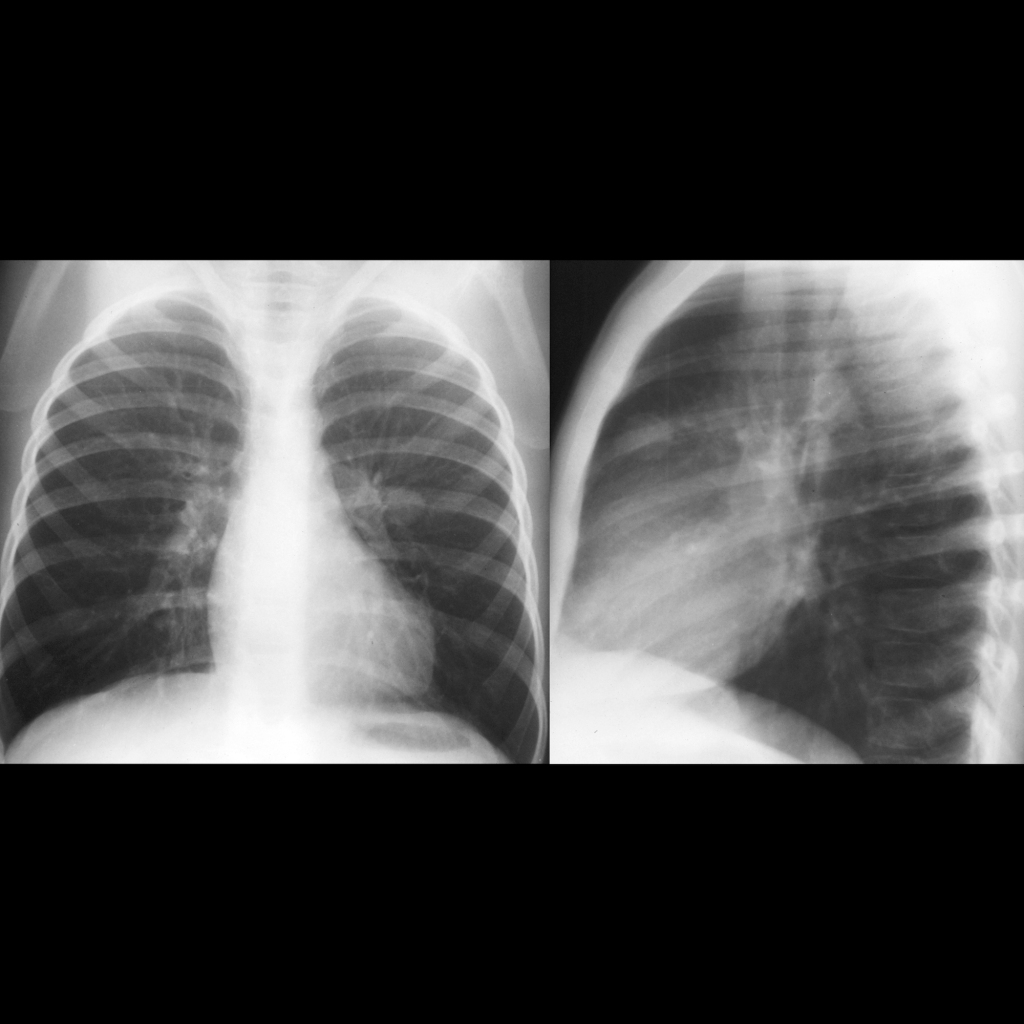
Radiology Cases of Lung Metastases in Wilms Tumor
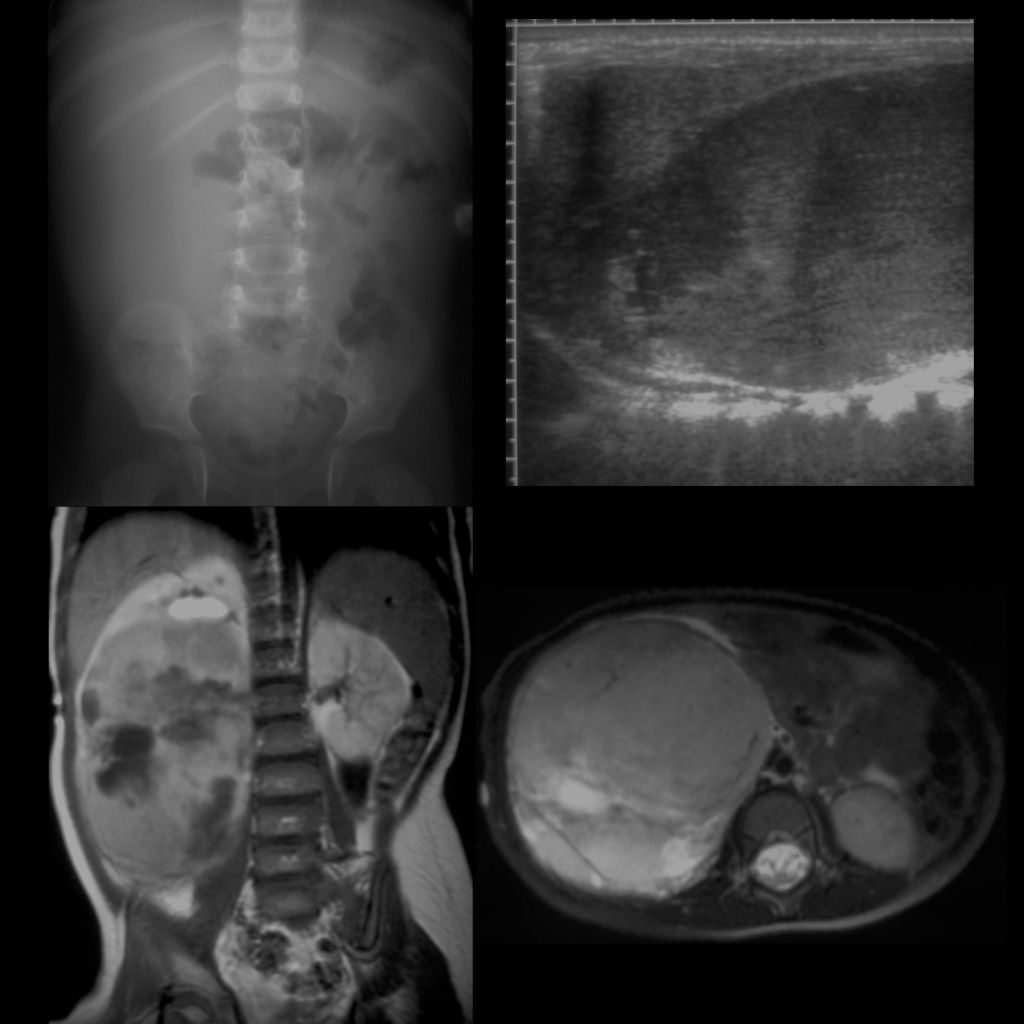
Radiology Cases of Hepatic Metastases in Wilms Tumor
Radiology Cases of Inferior Vena Cava Invasion in Wilms Tumor
Clinical Cases of Wilms Tumor

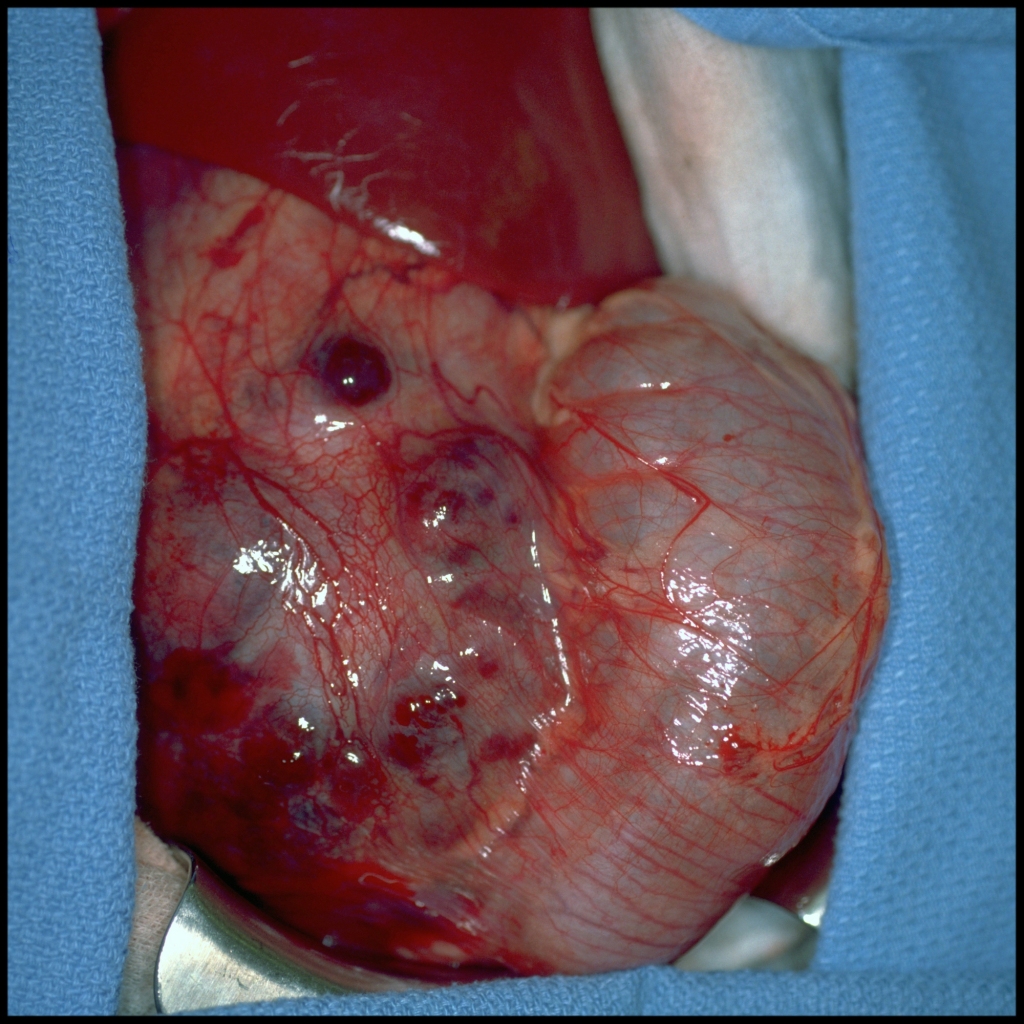
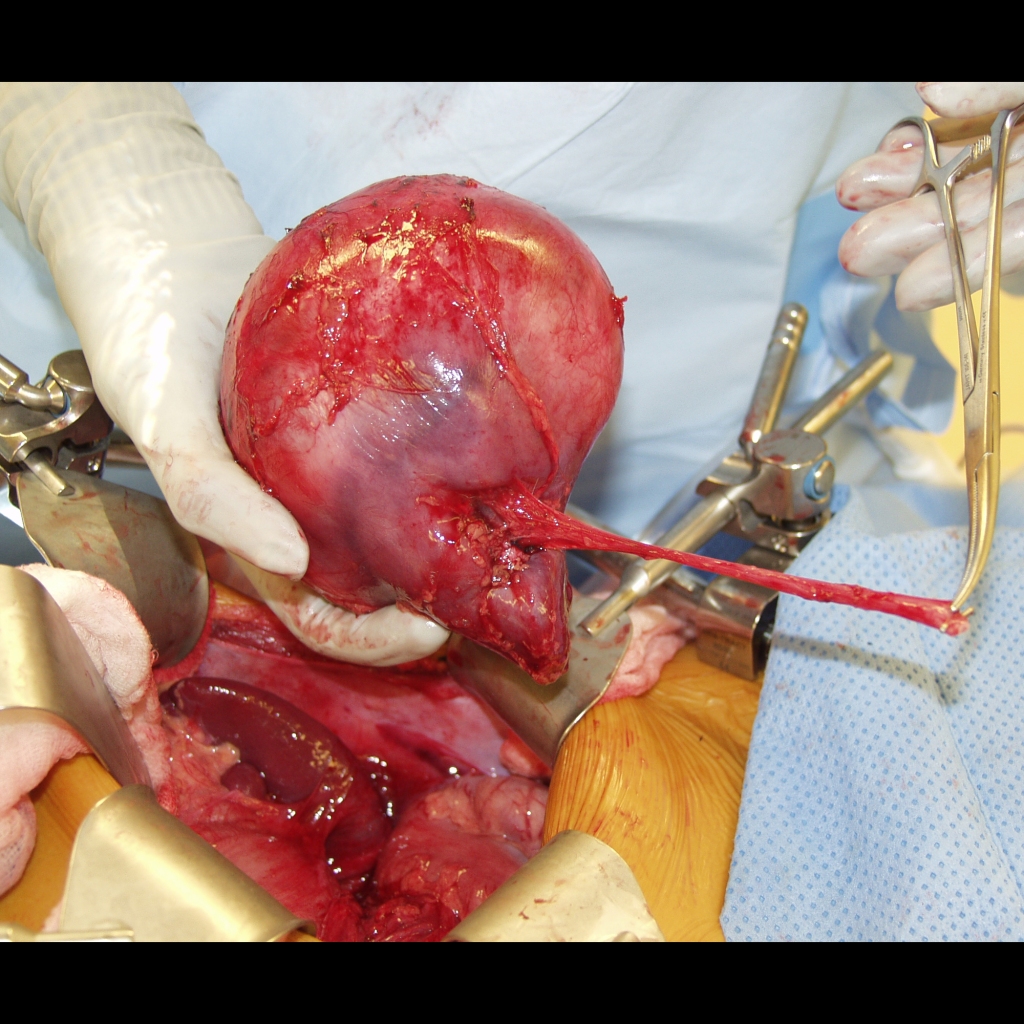
Surgical Cases of Wilms Tumor

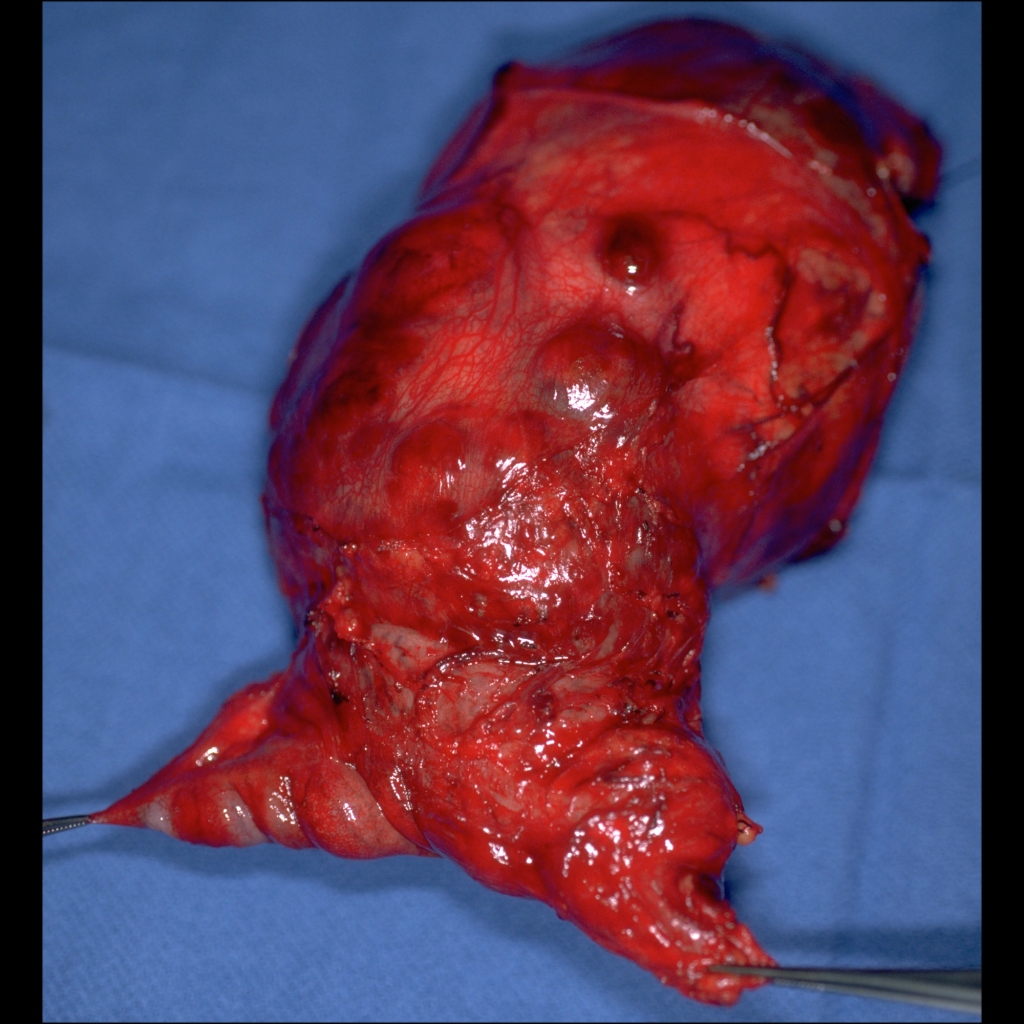
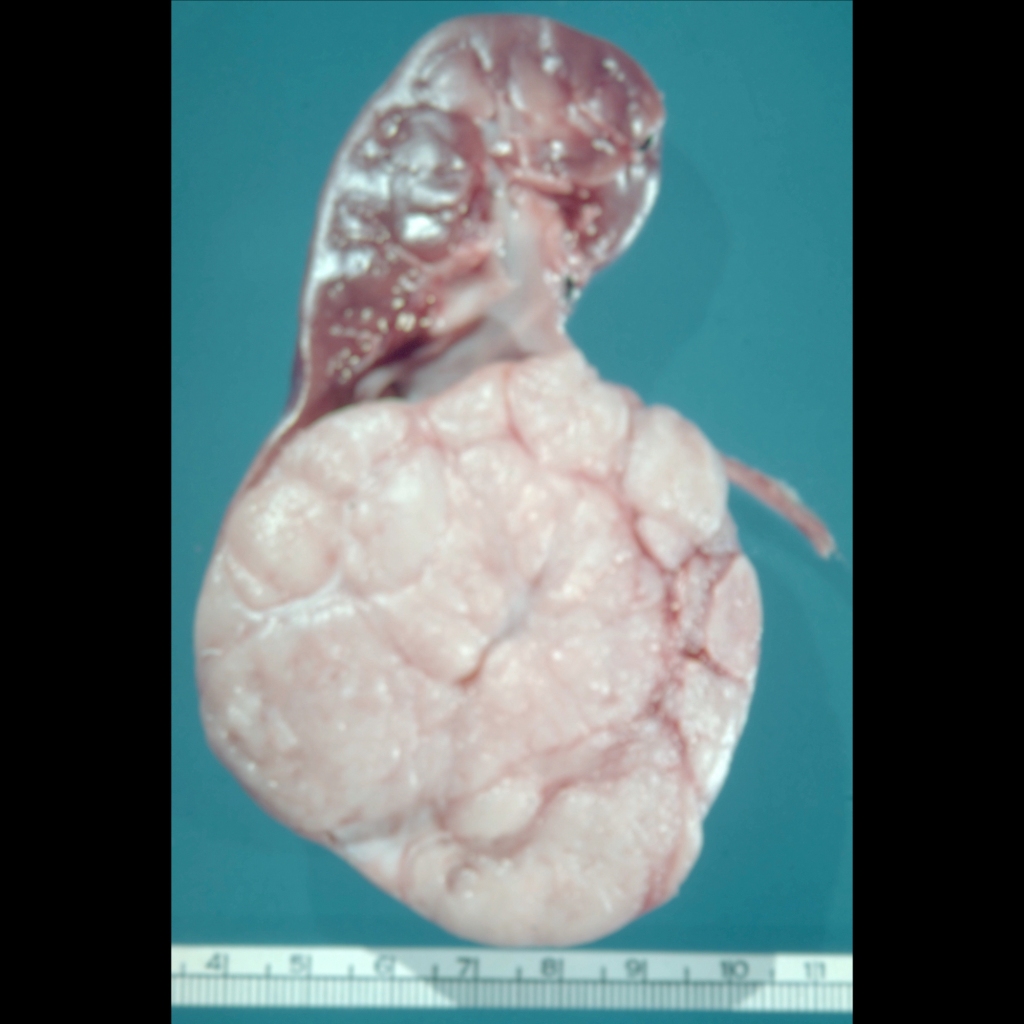
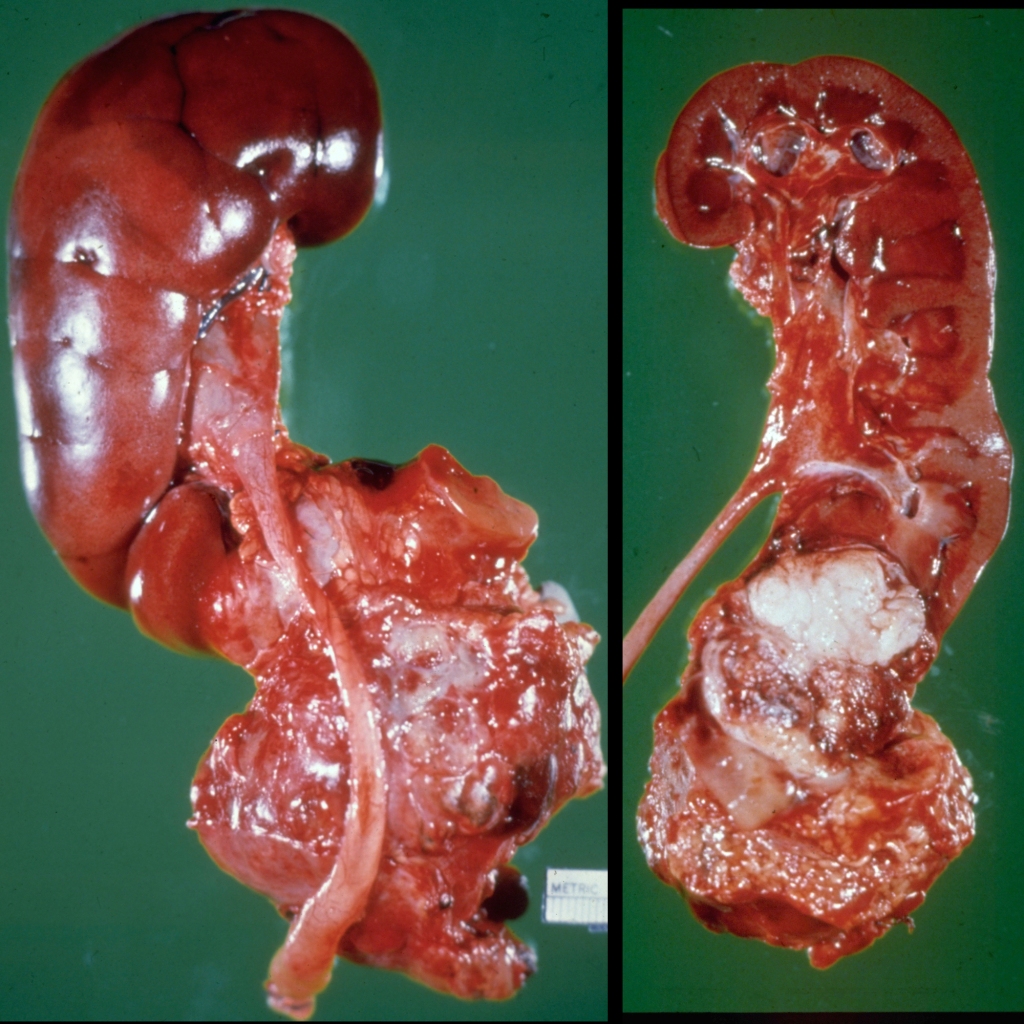
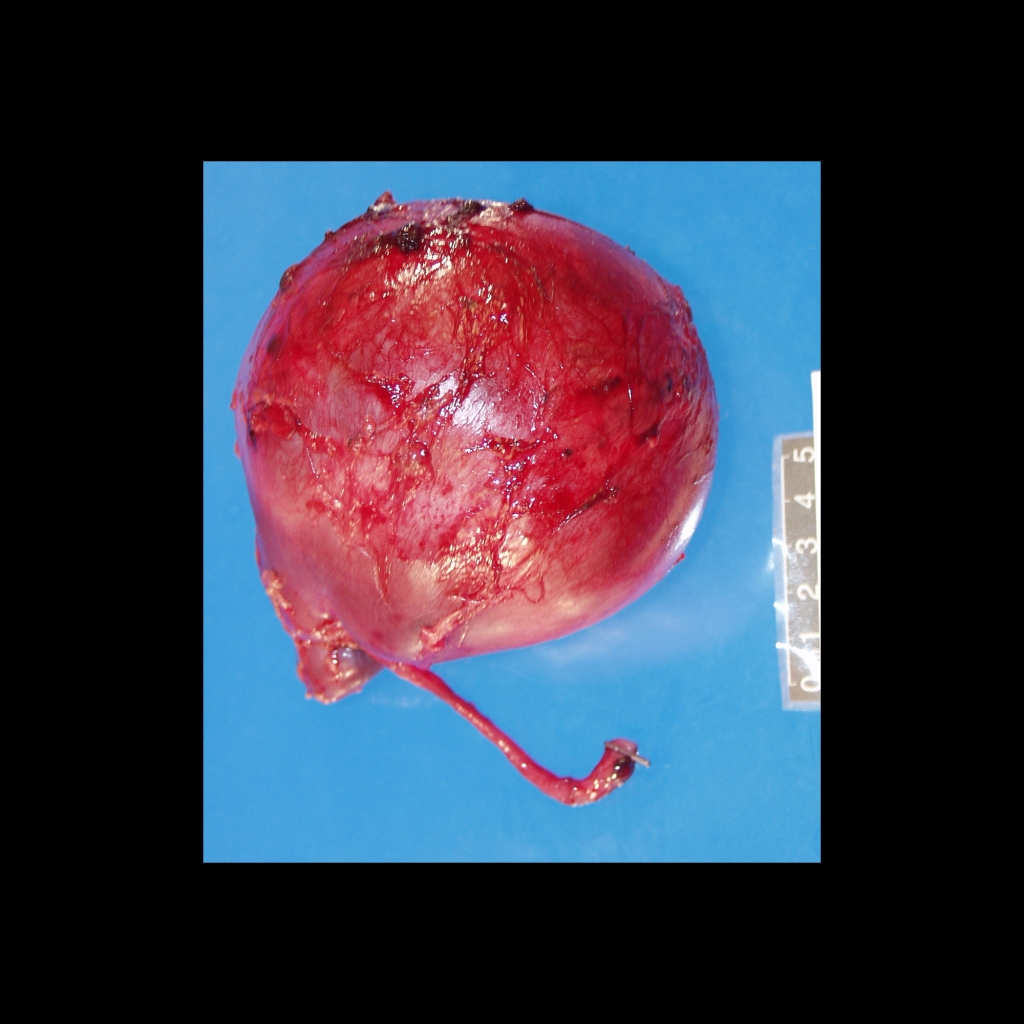
Gross Pathology Cases of Wilms Tumor


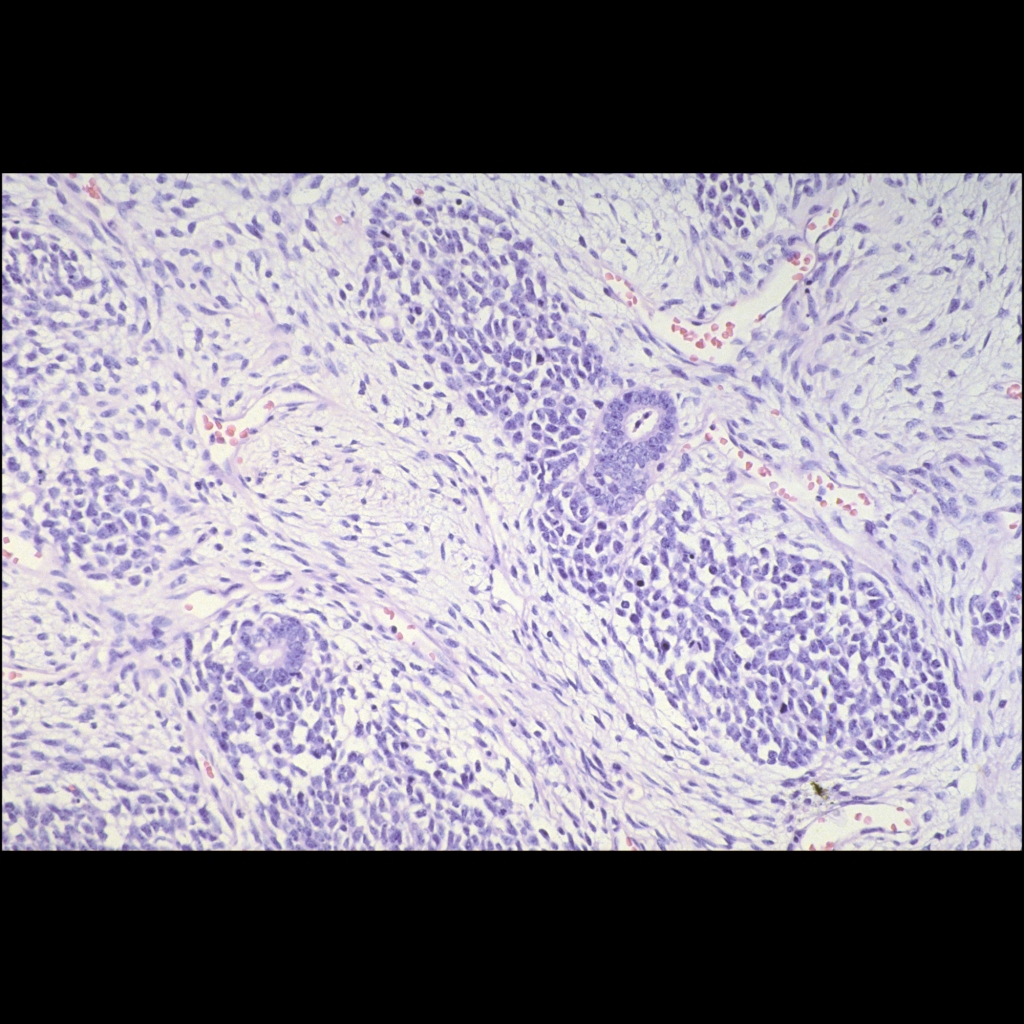
Histopathology Cases of Wilms Tumor