Chapter 16 Evaluation of Intracardiac Masses
General Benefits of Three-Dimensional Echocardiography Over Two-Dimensional Echocardiography
Tumors: Generalities
Primary tumors of the heart are extremely rare, with a reported prevalence of 0.001% to 0.03% by autopsy series.1 The most common primary cardiac tumor is the myxoma, even though myxoma is relatively uncommon. Myxomas are most common in the atria, particularly the left atrium. They often have a clear stalk attached to the interatrial septum and clearly visualized with 3DE. Myxomas typically are benign, but the most common primary malignant tumors are sarcomas, which are highly invasive and uniformly fatal tumors. Angiosarcoma is the most common of this group. Metastatic tumors to the heart are much more common than are primary tumors, with the most common being breast and lung tumors; the usual cardiac site of metastasis is the pericardium. In fact, secondary involvement of the heart by extracardiac tumors is 20 to 40 times more common compared with primary cardiac tumors.1–3 Melanoma is a tumor that has particular propensity to metastasize to the heart.4
Individual Tumors: Myxomas
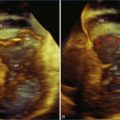
As mentioned, myxomas are the most common primary cardiac tumors (Figures 16-1 to 16-3; Videos 16-1 to 16-6). 3D imaging of atrial myxomas has been reported by transthoracic and transesophageal methods. The main benefits of 3DE over 2DE for myxomas are (1) identification of the stalk of the tumor and (2) evaluation of the heterogeneity of the mass. In fact, both characteristics often are seen with 2DE. The first case of imaging a right atrial myxoma by RT3DTEE was reported by Scohy et al (Figure 16-4).5 At the time of surgical excision, it was noted that the size of the mass correlated extremely well with the estimate by RT3DTEE. In fact, the volume of 6.4 mL was the same as shown by 3DTEE and by ex vivo measurement. Butz et al6 also measured a left atrial myxoma preoperatively by using 3DTEE and determined excellent correlation with the excised mass at the time of surgery. In another case study, a right ventricular and tricuspid valve myxoma was identified by 2DTTE; it measured 5.5 × 3.8 cm but was remarkably larger as shown by 3DTTE (12 × 6 cm). 3DTTE improved the visualization of the special relationship with surrounding structures and identified the involvement of the tricuspid valve, which was not appreciated by 2DTTE (Figure 16-5).7 Two cases of giant myxoma resulting in significant mitral valve obstruction were described by Culp et al.8 RT3DTEE volume measurement coordinated well with the ex vivo measurement. 2DTEE underestimated the volume (Figure 16-6).










Figure 16-6 A giant myxoma of the left atrium causing obstruction of the mitral orifice.
(From Culp WC Jr, Ball TR, Armstrong CS, et al: Three-dimensional transesophageal echocardiographic imaging and volumetry of giant left atrial myxomas. J Cardiothorac Vasc Anesth 23:66–68, 2009.)
Prior to these publications, incremental value for the characterization of internal composition of masses and volume calculation had been appreciated with RT3DTTE imaging for myxomas and a hemangioma. In this small series, four left atrial tumors, including three myxomas and one hemangioma, were imaged by RT3D and correlated with histopathology specimens. Echolucencies suggestive of intramass hemorrhage were more frequently seen with 3D imaging compared with 2DE. In addition, 3DTTE detected more extensive and closely packed echolucencies involving the whole extent of the tumor in the hemangioma compared with more scattered echolucencies in myxomas (Figure 16-7).9


Fibroma
Fibroma is a congenital neoplasm that usually affects children. A right ventricular fibroma was diagnosed by 2DTTE in a patient with previous incomplete resection of the same. The fibroma (Figure 16-8) was dramatically larger (9.0 × 2.8 cm) by RT3DTTE compared with 2DE (2.6 × 2.7 cm).7 A left atrial fibroma (Figure 16-9) was associated with Gardner syndrome.10



Papillary Fibroelastoma
Papillary fibroelastoma is the third most common tumor of the heart, with an incidence of 0.33% among autopsy series.11 It is the most common tumor of the heart valves and is most frequently identified on the aortic valve (Figure 16-10), although all valves have been described (Figure 16-11; Video 16-7). The value of RT3DTTE was illustrated in a case presented by Singh and colleagues12 with a papillary fibroelastoma of the pulmonary valve. RT3DTTE pinpointed the attachment point, which was helpful in planning valve-sparing surgery. Also, 3D cropping through multiple orthogonal planes revealed frondlike projections and no echolucencies, which helped differentiate the mass from a myxoma or thrombus (Figure 16-12). Le Tourneau and associates13 studied seven consecutive patients with this lesion who had surgical resection of the lesion and found feasibility of imaging the mass to be 100%. Correlation of the 3D volume size with the actual resected tumor was very good. They believed RT3DTTE helped with surgical planning in three of the seven patients; surgical planning is key when valve-sparing surgery is planned. Most of the lesions (five of seven) were on the aortic valve.13





Sarcomas
Sarcomas are quite rare primary tumors of the heart but are, in fact, the most common type of primary malignant cardiac tumor, at least in the adult population. Angiosarcoma is the most common among cardiac sarcomas and typically arises in the right atrium, often adjacent to the inferior or superior vena cava. These tumors often are large and aggressive, sometimes occupying much of the right atrium (Figures 16-13 to 16-16; Videos 16-8 to 16-10). Suwanjutah et al14 described a case of leiomyosarcoma imaged by RT3DTTE (Figure 16-17). The notable incremental value of RT3DTTE was the composition of the mass. RT3DTTE, again, thanks to its cropping capability, allowed imaging of an area of echolucency, suggesting necrosis or hemorrhage surrounded by bandlike structures consistent with collagen. This image created a “donut” appearance. Excision and evaluation of the resultant histopathology revealed the same pattern of necrosis and vascular channels within the fibrotic tumor. The morphology seen in this case of the tumor by RT3DTTE was suggestive of tumor as opposed to a thrombus. Just as important, the size of the mass by RT3DTTE was significantly larger than when measured by 2DTTE.


Figure 16-14 Three-dimensional transesophageal echocardiography of a right atrial angiosarcoma (arrow).


Figure 16-16 Right ventricular sarcoma (arrow). LV, left ventricle; RA, right atrium; RV, right ventricle.
(From Reddy VK, Faulkner M, Bandarupalli N, et al: Incremental value of live/real time three-dimensional transthoracic echocardiography in the assessment of right ventricular masses. Echocardiography 26:598–609, 2009.)

Lymphomas
Lymphomas represent 5% of primary cardiac malignancies, although diagnosis is not commonly made during life due to nonspecific presenting symptoms. A case of non-Hodgkin lymphoma in the right atrium that presented as atrial fibrillation was described and imaged by RT3DTTE. Follow-up imaging was useful for chemotherapy cleanup and showed marked shrinkage of the mass.15
Carcinoid Syndrome
Cardiac involvement occurs in more than 50% of patients with carcinoid syndrome. The right-sided heart valves are characteristically involved, with the tricuspid valve particularly affected. As previously mentioned, the pulmonary valve is particularly challenging to image by echocardiography. In a series of cases reported by Nalawadi and colleagues16 in three patients who were diagnosed with cardiac carcinoid, RT3DTEE performed well when determining involvement of the tricuspid and pulmonary valves (Figure 16-18). There was particular incremental value for viewing the tricuspid valve en face, particularly by RT3DTTE, which demonstrated a fixed, open-orifice tricuspid valve with severe tricuspid regurgitation. The pulmonary valve was seen well in only one of the four cases, and notable RT3DTEE findings were not visible in the images provided. However, the authors state that “RT3D was particularly helpful in showing carcinoid involvement of the pulmonic valve with thickening, retraction, and distortion, as well as, if present, identifying a mass on the valve.” Our own experience with RT3DTEE in carcinoid syndrome has been limited, but it is clear that the aortic arch view of the pulmonary valve would be useful in this setting (see Chapter 10).

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


