Download presentation
Presentation is loading. Please wait.

1
Upper GI Bleeding B33

2
Mallory – Weiss Syndrome Epidemiology - 80% of the cases are men - Predominant in 40-60 age group - It accounts for 5-10% of Upper GI Bleeding

3
What is it ? refers to bleeding from tears (a Mallory-Weiss tear) in the mucosa at the junction of the stomach and esophagus. A Mallory Weiss tear is a linear mucousal tear occurring at the esophageogastric junction and produced by a sudden increase in intra-abdominal pressure. Usually after bouts of Coughing or vomiting where gastric contents are pushed through LES forcefully producing tears.
 in the mucosa at the junction of the stomach and esophagus. A Mallory Weiss tear is a linear mucousal tear occurring at the esophageogastric junction and produced by a sudden increase in intra-abdominal pressure. Usually after bouts of Coughing or vomiting where gastric contents are pushed through LES forcefully producing tears..")
4
Causes It is often associated with: alcoholism ( After a bout of severe retching –the try to vomit- or vomiting) eating disorders. (ex. Bulemia Nervosa, Some of those people induce self-vomiting in order to lower loss weight) there is some evidence that presence of a hiatal hernia is a predisposing condition. Hyperemesis gravidarum, which is severe morning sickness associated with vomiting and retching in pregnancy, is also a known cause of Mallory-Weiss tear.
 there is some evidence that presence of a hiatal hernia is a predisposing condition. Hyperemesis gravidarum, which is severe morning sickness associated with vomiting and retching in pregnancy, is also a known cause of Mallory-Weiss tear..")
5
Have a look, He’s An Alcoholic and he’s vomiting fresh red blood, What’s wrong with him ?

6
Signs and Symptoms Hematemesis ( in 85%) usually after violent Vomiting or coughing, and is not profuse and cease without surgical intervention (within 24 hours), but life- threatening hematemesis may occur. Less common presenting symptoms include melena, hematochezia, syncope, and abdominal pain. Tachycardia, hypotension, orthostatic changes, or overt shock may be evident which correlate with the blood loss.

7
Diagnosis & treatment Diagnosis : 1. Taking History 2. Endoscopy: (definitive diagnosis ). Treatment : 1. Supportive ( most commonly ) 2. Cauterization or injection of epinephrine ( to stop bleeding) 3. Arterial embolization 4. Endoscopic band ligation or esophageal clips to cut of the circulation to the dilated veins in cases of portal hypertension and esophageal varices 5. Surgery (rarely)
. Treatment : 1. Supportive ( most commonly ) 2. Cauterization or injection of epinephrine ( to stop bleeding) 3. Arterial embolization 4. Endoscopic band ligation or esophageal clips to cut of the circulation to the dilated veins in cases of portal hypertension and esophageal varices 5. Surgery (rarely).")
8
Esophagitis Epidemiology - accounts for 5% of Upper GI bleeding. - Prevalence in Iran is more than 80% and is also extremely high in china, its not obvious why. BUT both Countries are well known for Ingesting Hot Drinks like tea, so what ?

9
What is it and what causes it ? Esophagitis: Refers to Inflammation of the esophagus Its caused by the following: 1) GERD ( Most common cause, 10-20% in west) 2) Infections ( Common in immunocompromised ) Fungal (Candida) or Viral (CMV or HSV) 3) Irritants and corrosives(acids,hotdrinks or alcohol) 4) Eosiniphilic Esophagitis (food allergy ?) 5) Physical injury by an Nasogastric tube or radiation 6) Crohn’s disease if it affects the esophagus
 GERD ( Most common cause, 10-20% in west) 2) Infections ( Common in immunocompromised ) Fungal (Candida) or Viral (CMV or HSV) 3) Irritants and corrosives(acids,hotdrinks or alcohol) 4) Eosiniphilic Esophagitis (food allergy ) 5) Physical injury by an Nasogastric tube or radiation 6) Crohn’s disease if it affects the esophagus.")
10
Morphology of esophagitis on endoscopy

11
Gastro-esophageal Reflux Disease Pathophysiology Decrease efficacy of the esophageal anti reflux mechanism, so gastric content come up from the stomach to esophagus irritating it and leading to esophagitis/ulceration and sometimes to Barret’s esophagus and eventually AdenoCa. Causes of GERD Pregnancy or obesity Fat, chocolate, coffee or alcohol ingestion Large meals Cigarette smoking Drugs – antimuscarinic, calcium-channel blockers Systemic sclerosis After treatment for achalasia Hiatus hernia

12
Signs and symptoms of GERD Heartburn/chest pain (aggrevated by bending or lying down common at night time which promote acid exposure) Regurgitation (sour taste) Cough Less common symptoms : Increased salivation (also known as water brash) Nausea Haematemesis (from esophagitis) Note: Heartburn is a retrosternal/epigastric pain and may mimic cardiac pain to differentiate Heartburn is relieved by Antiacids, PPI and H2 Blockers. 20% admitted to CCU have GERD instead of Cardiac causes

13
Signs and symptoms of esophagitis Heartburn. Pain when you swallow. Chest pain (may be similar to the pain of a heart attack). A cough. dysphagia haematemsis
. A cough. dysphagia haematemsis.")
14
Diagnosis & treatment Diagnosis 1) History 2) Barium Swallow ( To locate GERD or Hiatus Hernia or Narrowing) 3) Endoscopy and biopsy Treatments for esophagitis are intended to lessen symptoms, manage complications and treat underlying causes of the disorder. A)GERD Antiacids + aliginic acid, PPI, H2 Blockers, Coating Agents “sucralfate”, Prokinetic Agents or baclofen. B) Eosinophilic Esophagitis 6-food elimination diet or Topical swallowed steroids C)Narrowed inflammed esophagus Surgical esophageal dilatation
GERD Antiacids + aliginic acid, PPI, H2 Blockers, Coating Agents sucralfate , Prokinetic Agents or baclofen. B) Eosinophilic Esophagitis 6-food elimination diet or Topical swallowed steroids C)Narrowed inflammed esophagus Surgical esophageal dilatation.")
15
Upper Gastrointestinal Bleeding Peptic Ulcer Disease Anwar Al-Shamasneh

16
Upper gastrointestinal bleeding or hemorrhage (gastrorrhagia): refers to bleeding in the upper GIT, defined as bleeding arising from the a source proximal to the ligament of Treitz, which anatomically separates the duodenum from the jejunum. (Esophagus,Stomach, or Duodenum). Blood may be observed in vomit (Hematemesis) or in altered form in the stool (Melena)
. Blood may be observed in vomit (Hematemesis) or in altered form in the stool (Melena).")
17
Upper GIT bleeding is a life-threatening abdominal emergency and requires hospital care for urgent diagnosis and treatment. It the most common gastrointestinal emergency, accounting for 50–170 admissions to hospital per 100,000 of the population each year in the UK. The mortality of patients admitted to hospital is about 10%

18
The Presentation of bleeding depends on the amount and location of hemorrhage. It includes : Hematemesis : if the volume of bleeding is high enough, and may be fresh and red or dark brown in color (coffee ground vomiting ) Melena : black stool with a rotten odor, It develops when at least 100 mL of blood have been lost. Hematochezia (red or maroon stools) in 10% of cases.
 Melena : black stool with a rotten odor, It develops when at least 100 mL of blood have been lost. Hematochezia (red or maroon stools) in 10% of cases..")
19
Symptoms associated with blood loss : Fatigue Weakness Shortness of breath Diffuse Abdominal pain Jaundice Syncope : hypotension from intravascular volume depletion. Long-term GI bleeding may go unnoticed or may cause fatigue, anemia, black stools, or a positive test for microscopic blood. Rectal bleeding: occurs if the bleed is massive and it’s almost always accompanied by shock.

20
Dyspepsia: seen in ulcer disease, and NSAID or aspirin use. Orthostasis : postural hypotension indicates more rapid and severe blood loss (15%-20%). Dysphagia Epigastric pain Heart burn Weight loss
. Dysphagia Epigastric pain Heart burn Weight loss.")
21
The most common causes of upper gastrointestinal bleeding are: Peptic ulcer disease, gastritis, Mallory- Weiss syndrome, esophagitis, and gastric cancer. Variceal bleeding is common in those with portal hypertension from cirrhosis. Peptic Ulceration is the commonest cause of life-threatening GIT bleeding.

23
1- Intravenous Access The first step is to gain intravenous access using at least one large-bore cannula for fluid replacement, as well as blood transfusions.

24
2. Initial clinical assessment Define circulatory status : Severe bleeding causes tachycardia, hypotension and oliguria. The patient is cold and sweating, and may be agitated. Seek evidence of liver disease Identify co-morbidity

25
3. Basic investigations : Full blood count: Chronic or subacute bleeding leads to anaemia. Urea and electrolytes: This may show evidence of renal failure. Liver function tests : for chronic liver disease. Prothrombin time: Check with clinical suggestion of liver disease or in anticoagulated patients. Cross-matching. At least 2 units of blood should be cross-matched..

26
4. Resuscitation : I.V crystalloid fluids should be given to raise the blood pressure, and blood should be transfused when the patient is actively bleeding with low blood pressure and tachycardia. 5. Oxygen : should be given to all patients in shock. 6. Endoscopy: This should be carried out after adequate resuscitation, ideally within 24 hours and will yield a diagnosis in 80% of cases. Patients who are found to have major endoscopic stigmata of recent hemorrhage can be treated endoscopically.

27
7. Monitoring: Patients should be closely observed, with hourly measurements of pulse, blood pressure and urine output. 8. Surgery: Surgery is indicated when endoscopic haemostasis fails to stop active bleeding, and if re-bleeding occurs on one occasion in an elderly or frail patient, or twice in a younger, fitter patient.

28
The term “peptic ulcer” refers to an ulcer in the lower oesophagus, stomach or duodenum, in the jejunum after surgical anastomosis to the stomach or, rarely, in the ileum adjacent to a Meckel’s diverticulum. Ulcers in the stomach or duodenum may be acute or chronic; both penetrate the muscularis mucosae. The male-to-female ratio for duodenal ulcer varies from 5 : 1 to 2 : 1,whilst that for gastric ulcer is 2 : 1 or less.

29
Chronic gastric ulcer is usually single; 90% are situated on the lesser curvature within the antrum or at the junction between body and antral mucosa. Chronic duodenal ulcer usually occurs in the first part of the duodenum and 50% are on the anterior wall. Gastric and duodenal ulcers coexist in 10% of patients and more than one peptic ulcer is found in 10–15% of patients.

30
The classic peptic ulcer is a round to oval, sharply punched-out defect. The base of peptic ulcers is smooth and clean as a result of peptic digestion of exudate, and on histologic examination is composed of richly vascular granulation tissue.

31
The most common cause of PUD is Helicobacter pylori followed by the use of NSAIDs. Around 90% of duodenal ulcer patients and 70% of gastric ulcer patients are infected with H. pylori. The remaining 30% of gastric ulcers are caused by NSAIDs. Tobacco smoking, alcohol, and the use of steroids by themselves do not cause ulcer disease and can delay healing and are associated with the development of gastritis. Overall, 10 to 20% of ulcers are idiopathic

32
The most common presentation of ulcer disease is mid-epigastric pain. Gastric ulcers have been associated with pain on eating, and duodenal ulcers were thought to be relieved by eating. Because gastric ulcers were thought to be associated with pain on eating, this more frequently led to weight loss. Tenderness of the abdomen is unusual with ulcer disease. More than 80% are not associated with abdominal tenderness in the absence of a perforation.

33
Nausea and vomiting, bloating, anorexia, early satiety, and belching may be present. Persistent and severe pain suggests complications such as penetration into other organs. Back pain suggests a penetrating posterior ulcer. Severe ulceration can occasionally be symptomless, as many who present with acute ulcer bleeding or perforation have no preceding ulcer symptoms.

34
Ulcer disease is best diagnosed with upper endoscopy. Barium studies are inferior, in those age >45–55 or those with alarm symptoms (weight loss, anemia, heme-positive stools, or dysphagia), endoscopy should be performed. Gastric ulcers may occasionally be malignant and therefore must always be biopsied and followed up to ensure healing. Patients should be tested for H. pylori infection. Breath tests or faecal antigen tests are best because of accuracy, simplicity and non-invasiveness.
, endoscopy should be performed. Gastric ulcers may occasionally be malignant and therefore must always be biopsied and followed up to ensure healing. Patients should be tested for H. pylori infection. Breath tests or faecal antigen tests are best because of accuracy, simplicity and non-invasiveness..")
35
1- H. pylori eradication : All patients with proven ulcers who are H. pylori-positive should be offered eradication as primary therapy. - Treatment is based upon a PPI taken simultaneously with two antibiotics (from amoxicillin, clarithromycin and metronidazole) for 7 days. High-dose, twice-daily PPI therapy increases efficacy of treatment, as does extending treatment to 10–14 days. - A quadruple therapy regimen, consisting of omeprazole (or another PPI), bismuth subcitrate, metronidazole and tetracycline (OBMT) for 10–14 days, is recommended.
 for 7 days. High-dose, twice-daily PPI therapy increases efficacy of treatment, as does extending treatment to 10–14 days. - A quadruple therapy regimen, consisting of omeprazole (or another PPI), bismuth subcitrate, metronidazole and tetracycline (OBMT) for 10–14 days, is recommended..")
36
2. Maintenance treatment For the minority who do require it, the lowest effective dose of PPI should be used. 3. General measures Stopping smoking should be strongly encouraged. Routine re- endoscopy at 6 weeks to exclude a malignant tumor of GU. 4. Surgical treatment Surgery is now rarely required for peptic ulcer disease but it is needed in some cases such as: chronic non-healing gastric ulcer In emergency when the bleeding is severe For giant duodenal ulcers

37
1. Bleeding Over a long period of time, a person may become anemic. If a damaged blood vessel is large, bleeding is dangerous and requires prompt medical attention. The symptoms of bleeding include: feeling weak and dizzy when standing, vomiting blood, or fainting. 2. Perforation Sometimes an ulcer eats a hole in the wall of the stomach or duodenum. The symptoms of a perforated ulcer include: sudden, sharp, severe pain. Immediate hospitalization and surgery is usually required.

38
3. Gastric outlet obstruction The obstruction may be pre-pyloric, pyloric or duodenal. The obstruction occurs either because of an active ulcer with surrounding oedema or because the healing of an ulcer has been followed by scarring. After gastric outlet obstruction the stomach becomes full of gastric juice and ingested fluid and food, giving rise to the main symptom of vomiting. Vomiting is infrequent, projectile, large in volume, and the vomitus contains particles of previous meals. On examination of the abdomen there may be a succussion splash.

39
Non-Steriodal Anti-Inflamatory Drugs By Serina A-Rababa’a

40
NSAIDs -- NSAIDs like aspirin, ibuprofen, naproxen etc. are drugs used by many people due to their analgesic, antipyretic and anti-inflammatory effect. -- NSAIDs are a leading cause of gastric and duodenal ulcers which are major contributors for upper GIT bleeding.

41
NSAIDs -- With the over-the-counter use included, more than 30 billion doses of NSAIDs are consumed annually in the US. -- They work primarily by inhibiting the Cyclooxygenase (COX) enzyme, this leads to decreased prostaglandin synthesis with both beneficial and unwanted effects.
 enzyme, this leads to decreased prostaglandin synthesis with both beneficial and unwanted effects..")
42
NSAIDs -- PGI2 which inhibit gastric acid secretion, PGE2 and PGF2 alpha which stimulates production of protective mucus in both stomach and small intestine are all inhibited by NSAIDs resulting in a diminished mucus protection and increased acid secretion. -- This may lead to epigastric distress, ulceration, hemorrhage and iron deficiency anemia.

43
NSAIDs - - COX1 and COX2 isoenzymes are both inhibited. -- COX1 mediates the synthesis of protective prostaglandins which are responsible for keeping the gastric mucosa intact and TXA2 which is essential for clotting mechanism. --Cox2 mediates the synthesis of inflammatory prostaglandins.

44
NSAIDs -- Aspirin inhibit both COX1 and COX2 irreversibly. -- Pts using aspirin and other forms of NSAIDs for long term should use PPI as well to prevent gastro-duodenal distress and ulceration. -- Furthermore Aspirin irreversibly blocks thromboxane production in platelets by inhibiting cyclooxygenase leading to decreased platelets aggregation thus prolonging bleeding time.

45
NSAIDs

46
Upper GIT Bleeding -- Other less common causes of upper GIT bleeding: 1. Osler-Weber-Rendu (hereditary hemorrhagic telangiectasia) is rare autosomal dominant condition which affect blood vessels throughout the body including GIT. IT causes telangiectasias and arteriovenouse malformation which can rupture and bleed, in the GIT they are usually found in the stomach and deodenum.
 is rare autosomal dominant condition which affect blood vessels throughout the body including GIT. IT causes telangiectasias and arteriovenouse malformation which can rupture and bleed, in the GIT they are usually found in the stomach and deodenum..")
47
Upper GIT Bleeding 2. Peutz-Jegher’s Syndrome is a autosomal dominant genetic disease characterized by development of benign hamartomatous polyps in the gastrointestinal tract that may lead to acute or chronic GI bleeding. 3. Dieulafoy lesion is characterized by a large tortuous arteriole stomach wall that may erode and bleed, it accounts for less than 0.5% of all GIT bleeding in adults. 4. Aorto-enteric fistula.

48
Upper GIT Bleeding Osler-Weber- Rendu Syndrome PEUTZ-Jegher’s syndrome Aorto-Enteric Fistula

49
GASTIRTIS By Oroba Al- Tlas

50
GASTRITIS Is the term applied to describe inflammation, erosion or damage of the gastric lining that has not develop to an Ulcer. Gastritis can lead to ulcers and an increased risk of stomach cancer. For most people, however, gastritis isn't serious and improves quickly with treatment

51
Risk Factors 1.Bacterial infection ( H.pylori ) 2.Regular use of pain relievers ( NSAID’S ) 3.Older Ages ( physiological ) 4.Stress 5.Excessive use of alcohol 6. Burns, mechanical ventilation.

52
Acute Gastritis Many cases result from aspirin or NSAID ingestion. Acute gastritis often produces no symptoms but may cause dyspepsia, anorexia, nausea or vomiting, and haematemesis or melaena. Many cases resolve quickly and do not need more investigation. In more severe cases there may be mucosal erosion, ulceration, hemorrhage, hematemesis, melena, or, rarely, massive blood loss. endoscopy and biopsy may be necessary, to exclude peptic ulcer or cancer. Treatment should be directed at the underlying cause.

53
Chronic Gastritis The symptoms and signs associated with chronic gastritis typically are less severe but more persistent than those of acute gastritis. Nausea and upper abdominal discomfort may occur, sometimes with vomiting, but hematemesis is uncommon. The most common cause of chronic gastritis is infection with the bacillus Helicobacter pylori.

54
UPPER GIT BLEEDING ASSESSMENT

55
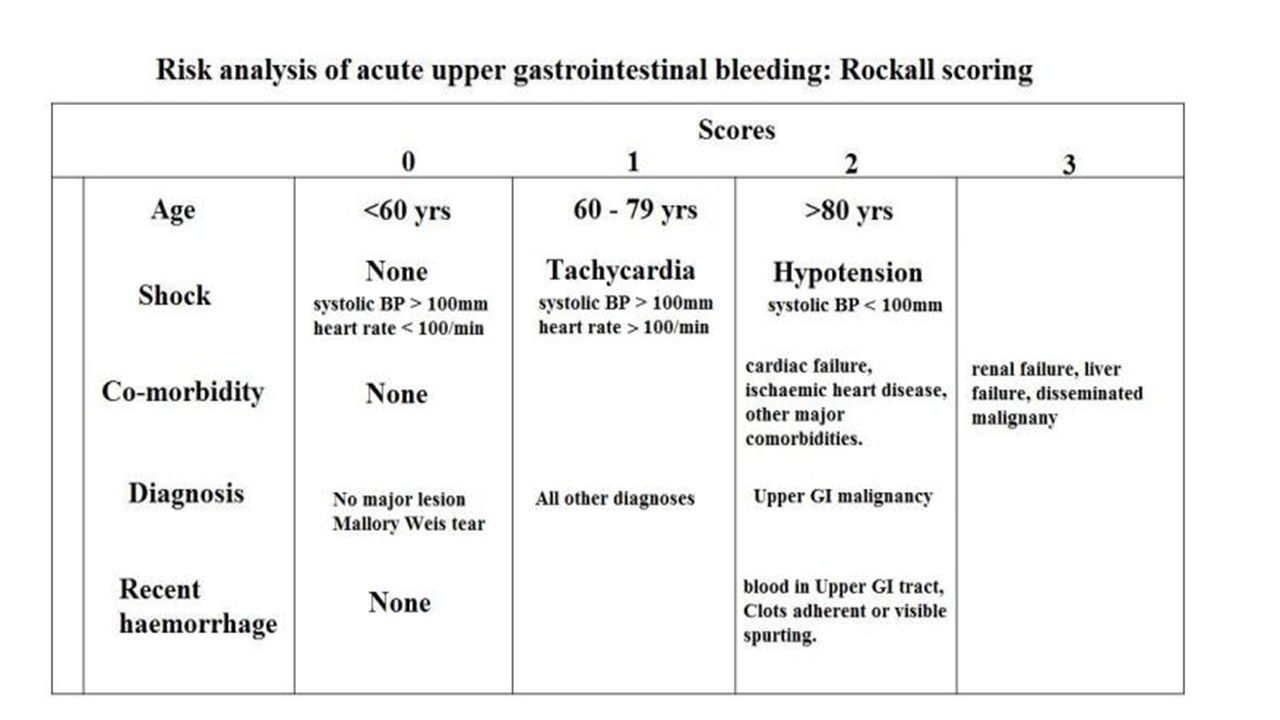
Rockall Risk Assesment Rockall scoring system includes clinical criteria (increasing age, co-morbidity, shock) as well as endoscopic findings (diagnosis, stigmata of acute bleeding)to identify pts. at risk of adverse outcome after upper GI bleeding. The total score is calculated by simple addition. A score of 8 carries a high risk of mortality.

57
Glasgow Blatchford Score Glasgow Blatchford score is a screening tool used to asses if a pt with acute upper GI bleeding requires medical intervention. Total score is calculated by simple adding. Advantages over Rockall scoring system: 1.it lacks subjective variables such as the severity of systemic diseases. 2.Does not require endoscopy to complete score.

58
Glasgow Blatchford Score

59
Score “0” low risk criteria: 1.Urea <6·5 mmol/L 2.Hemoglobin level >12.9 g/dL (men) or >11.9 g/dL (women) 3.Systolic blood pressure >=110 mm H 4.Pulse <100 beats per min 5.absence of melaena, syncope, cardiac failure, or liver disease Score > 6 is high risk patient, medical intervention is required. Score < 6 medical intervention is recommended but can be managed as an outpatient.

60
Gastric Tumors Esophageal Varices Bayan Mohammd

61
GASTRIC TUMOURS 90-95% are carcinomas 4% lymphoma 3%carcinoid 2% stromal T

62
Epidemiology & pathogenesis Gastric cancer is the fourth most common cancer world wide The 2 nd leading cause of cancer related mortality peak incdence50-70 years with types intestinal(associated with chronic gastritis) male predominance 2:1 or diffuse present earlier with female predominance (worse prognosis,denovo)
 male predominance 2:1 or diffuse present earlier with female predominance (worse prognosis,denovo)")
63
There is strong link between gastric cancer and H.pylori diet(salt,nitrosamines, smoked food ) smoking pernicious anaemia due to atrophic gastritis partial gastractomy.
 smoking pernicious anaemia due to atrophic gastritis partial gastractomy.")
64
Signs and symptoms Indigestion, epigastric pain Nausea or vomiting Dysphagia Postprandial fullness Loss of appetite Melena or pallor from anemia Hematemesis Weight loss Palpable enlarged stomach with succussion splash Enlarged lymph nodes such as Virchow nodes (ie, left supraclavicular) and Irish node (anterior axillary) skin lesions (acanthosis nigricans)
 and Irish node (anterior axillary) skin lesions (acanthosis nigricans)")
65
diagnosis Hx & examination Gastroscopy and biopsy (to exclude lymphoma) negative biopsy doesn't rule out the Dx so that 8-10 biopsy should be taken from the suspected lesion * full blood count *barium meal (accuracy 90%) *Tumor markers such as CEA and CA 19-9: Elevated CEA in 45-50% of cases; elevated CA 19-9 in about 20% of cases
 negative biopsy doesn t rule out the Dx so that 8-10 biopsy should be taken from the suspected lesion * full blood count *barium meal (accuracy 90%) *Tumor markers such as CEA and CA 19-9: Elevated CEA in 45-50% of cases; elevated CA 19-9 in about 20% of cases")
66
Treatment *endoscopy (non ulcerated mucosal lesions) *surgery (most effective) Total gastrectomy, Esophagogastrectomy, Subtotal gastrectomy, Lymph node dissection *chemotherapy (epirubicin,cisplatin) over all survival rate has not improved with a max 10-20% 5 years survival * palliative care
 *surgery (most effective) Total gastrectomy, Esophagogastrectomy, Subtotal gastrectomy, Lymph node dissection *chemotherapy (epirubicin,cisplatin) over all survival rate has not improved with a max 10-20% 5 years survival * palliative care")
67
Esophageal varices

68
Esophageal varices are enlarged veins in the wall of the distal part of the esophagus and sometimes the proximal part of the stomach.

69
Causes Portal hypertension 10-12 mmhg (prehepatic, intrahepatic, posthepatic rare) prehepatic : portal vain thrombosis intrahepatic :schistosomiasis,cirrhosis,budd-chiari syndrome posthepatic :RHF,obstructive pericarditis
 prehepatic : portal vain thrombosis intrahepatic :schistosomiasis,cirrhosis,budd-chiari syndrome posthepatic :RHF,obstructive pericarditis")
70
The vessels may leak blood or even rupture, causing life-threatening bleeding. Melena (black tarry stool) hematamesis signs of liver disease (jaundice, spider nevi, palmar erythema,ascites )
 hematamesis signs of liver disease (jaundice, spider nevi, palmar erythema,ascites ).")
71
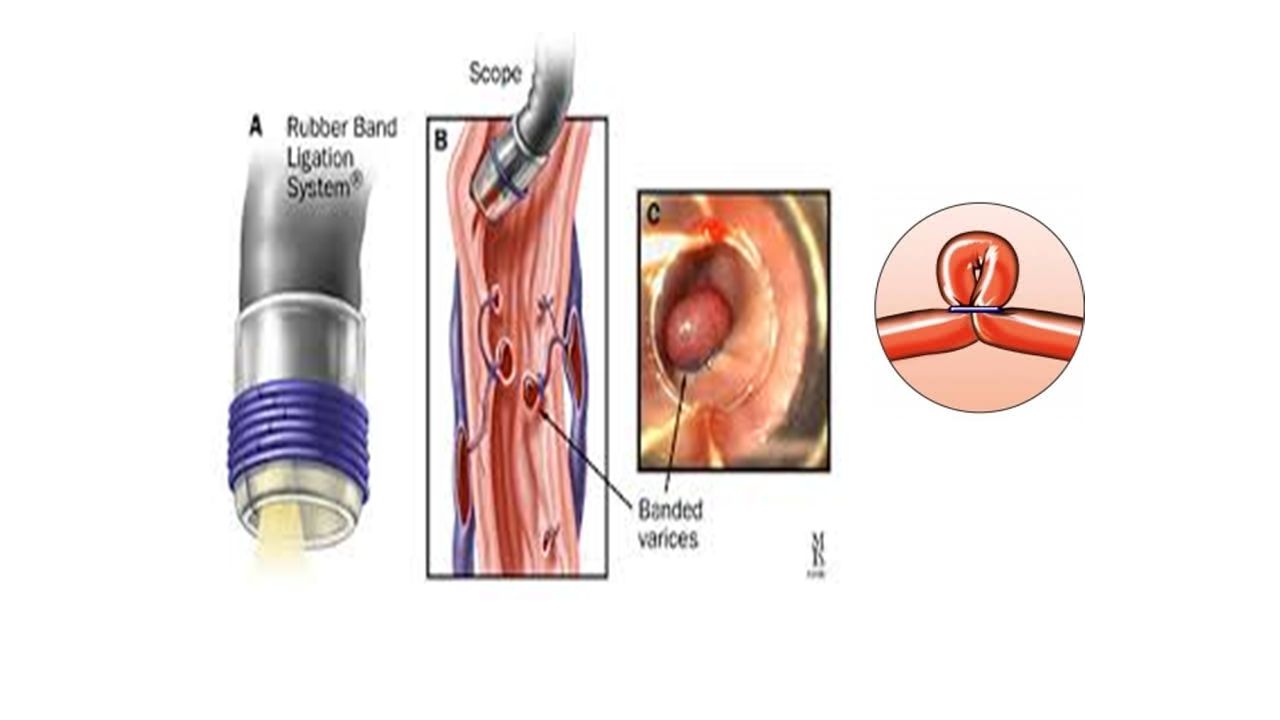
Treatment resuscitation (IV fluid blood trans. Treatment of hypovolmeia) prophylactic antibiotic to treat and prevent infection 3 rd generation cephalosporin emergency endoscopy to place bands around bleeding varices or sclerothrapy (higher complications eg stricture) Octreotide during acute episode to lower portal pressure if ineffective
 prophylactic antibiotic to treat and prevent infection 3 rd generation cephalosporin emergency endoscopy to place bands around bleeding varices or sclerothrapy (higher complications eg stricture) Octreotide during acute episode to lower portal pressure if ineffective.")
73
TIPS(transjagular intrahepatic portosystemic shunting) long term complication worsen hepatic encephalopathy propranolol used in long term management of portal hypertension and decrease frequency of bleeding
 long term complication worsen hepatic encephalopathy propranolol used in long term management of portal hypertension and decrease frequency of bleeding")
Similar presentations





>")
![Peptic Ulcer Disease Dr Maha Arafah. Objectives Upon completion of this lecture the students will : A] Understand the Pathophysiology of acute and chronic.](/13/3809458/big_thumb.jpg "Peptic Ulcer Disease Dr Maha Arafah. Objectives Upon completion of this lecture the students will : A] Understand the Pathophysiology of acute and chronic.>")






>")
 Dr. Gehan Mohamed Dr. Abdelaty Shawky.>")

 682-3793; (p) 413-3222.>")



