Download presentation
Presentation is loading. Please wait.

1
Anemia of Chronic Disease
Etiology Infections, cancer, endocrine disorders (e.g. thyroid). Inflammatory and rheumatologic disease. Renal disease. Pathophysiology A mild hemolytic component is often present, red blood cell survival is moderately decreased. Erythropoietin levels are normal or slightly elevated but are inappropriately low for the degree of anemia, erythropoietin level is low in renal failure Iron cannot be removed from its storage pool in hepatocytes and RES cells.
. Inflammatory and rheumatologic disease. Renal disease. Pathophysiology. A mild hemolytic component is often present, red blood cell survival is moderately decreased. Erythropoietin levels are normal or slightly elevated but are inappropriately low for the degree of anemia, erythropoietin level is low in renal failure. Iron cannot be removed from its storage pool in hepatocytes and RES cells.")
2
Anemia of Chronic Disease
Diagnosis RBC are usually normocytic normochromic if the anemia is mild, but may be microcytic normochromic, or even microcytic hypochromic,Hb rarely < 9 g/dL except in renal failure. Serum iron, TIBC, and % saturation all normal or slightly reduced, serum ferritin is normal or increased. Normal or increased iron stores in bone marrow, decreased “normal” sideroblasts. Management Resolves if underlying disease is treated. Erythropoietin may normalize the hemoglobin value especially in chronic renal failure. Dose of erythropoietin required is lower for patients with renal disease

3
Case Presentation A 50 year old female presented with one month history of progressive pallor, multiple ecchymoses ,epistaxis and attacks of fever and sore throat. Her clinical examination revealed severe pallor, multiple bleeding spots on her legs . Blood counts revealed pancytopenia What is your differential diagnosis? 1-Aplastic Anemia. 2-Acute leukemia. 3-Myelodysplasia.

4
Aplastic Anemia Etiology Radiation Drugs • anticipated (chemotherapy)
• idiosyncratic (chloramphenicol, phenylbutazone) Chemicals • benzene and other organic solvents • DDT and insecticides Post viral e.g. hepatitis B, parvovirus,HIV. Idiopathic • often immune (cell mediated) Paroxysmal nocturnal hemoglobinuria Marrow replacement Congenital: Fanconi anemia, associated with dysmorphic features.
 Chemicals. • benzene and other organic solvents. • DDT and insecticides. Post viral e.g. hepatitis B, parvovirus,HIV. Idiopathic. • often immune (cell mediated) Paroxysmal nocturnal hemoglobinuria. Marrow replacement. Congenital: Fanconi anemia, associated with dysmorphic features.")
5
Abnormal Thumbs in Fanconi Anemia
6
Clinical Presentation of Aplastic Anemia
Occurs at any age Slightly more common in males. Can present acutely or insidiously. Features of anemia or neutropenia or thrombocytopenia (any combination). Thrombocytopenia as bruising, bleeding gums, epistaxis. Anemia as SOB, pallor and fatigue. Presentation of neutropenia ranges from infection in the mouth to septicemia.
. Thrombocytopenia as bruising, bleeding gums, epistaxis. Anemia as SOB, pallor and fatigue. Presentation of neutropenia ranges from infection in the mouth to septicemia.")
7
Aplastic Anemia Diagnosis 1- CBC: Pancytopenia
• normochromic normocytic anemia. • neutrophil count < 1.5 x 109/L. • platelet count < 20 x 109/L. • corrected reticulocyte count < 1%. 2- Bone marrow aspirate and biopsy • aplasia or hypoplasia of marrow cells with fat replacement.

8
Aplastic Bone Marrow Biopsy

9
Aplastic Anemia Management Removal of offending agents.
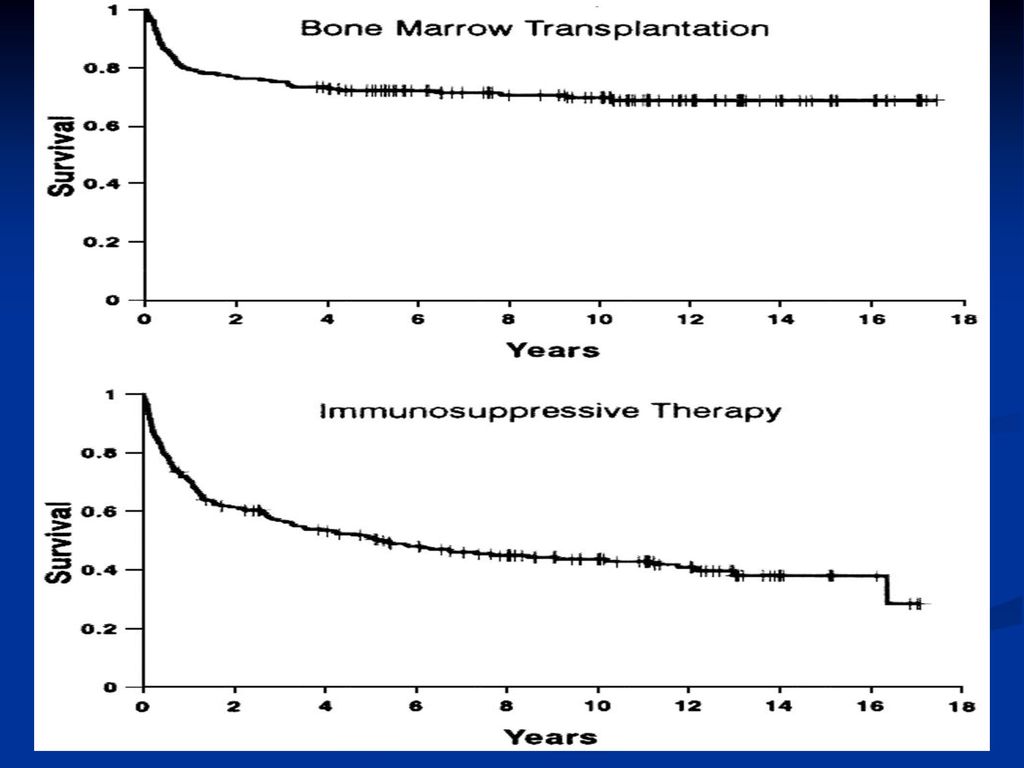
Supportive care (red cell and platelet transfusions, antibiotics). Antithymocyte globulin (50-60% of patients respond) for patients who are >45 years of age and those who have no donor for bone marrow transplant Cyclosporin A,mainly useful for mild cases. Allogeneic bone marrow transplantation for patients<45 y • minimize blood products on presentation. • only irradiated, leuko-depleted blood products should be used to minimize CMV transmission. • CMV negative blood for CMV negative patients.
. Antithymocyte globulin (50-60% of patients respond) for patients who are >45 years of age and those who have no donor for bone marrow transplant. Cyclosporin A,mainly useful for mild cases. Allogeneic bone marrow transplantation for patients<45 y. • minimize blood products on presentation. • only irradiated, leuko-depleted blood products should be used to minimize CMV transmission. • CMV negative blood for CMV negative patients.")
11
MYELODYSPLASTIC SYNDROMES (MDS)
Pathophysiology A group of clonal bone marrow stem cell disorders characterized by one or more cytopenias. Ineffective hematopoiesis despite presence of adequate numbers of progenitor cells (bone marrow is usually hyper-cellular). Dysplastic changes affect all the hematopoietic cell lines due to abnormal maturation and differentiation which include abnormal size , nuclear shape and cytoplasmic granules The blood elements are dysfunctional. There is increased liability for transformation to AML.
. Dysplastic changes affect all the hematopoietic cell lines due to abnormal maturation and differentiation which include abnormal size , nuclear shape and cytoplasmic granules. The blood elements are dysfunctional. There is increased liability for transformation to AML.")
12
Dysplastic nuclear features in circulating cells
Dysplastic nuclear features in circulating cells. Composite image taken from several cases of myelodysplastic syndrome showing dysplastic nuclear features seen in circulating granulocytes and nucleated RBCs. The right lower figure shows numerous Pappenheimer bodies.

13
MDS Refractory anemia (RA).
Types Refractory anemia (RA). Refractory anemia with ring sideroblasts (RARS). Refractory anemia with excess blasts (RAEB). Refractory anemia with excess blasts in transformation (RAEB-T). Chronic myelomonocytic leukemia (CMML).
. Refractory anemia with ring sideroblasts (RARS). Refractory anemia with excess blasts (RAEB). Refractory anemia with excess blasts in transformation (RAEB-T). Chronic myelomonocytic leukemia (CMML).")
14
MDS Clinical Presentation
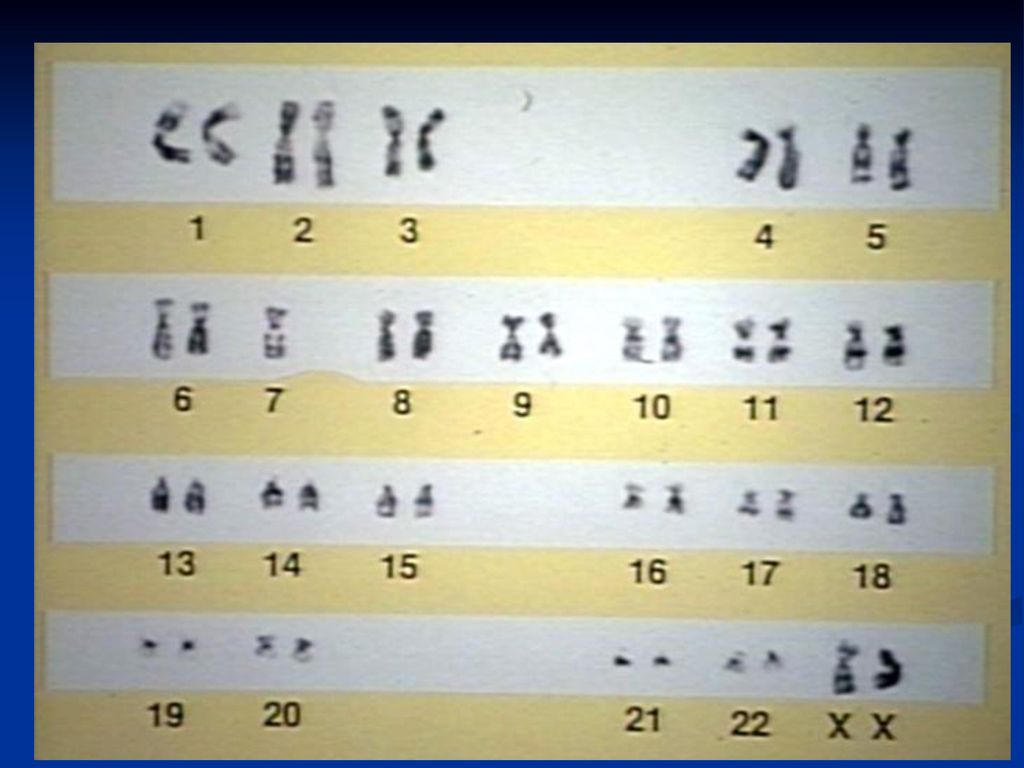
Related to bone marrow failure, most common in elderly, usually > 70 and post-chemotherapy or radiation Usually insidious in onset: fatigue, weakness, pallor, infections, bruising and rarely weight loss, and hepatosplenomegaly Diagnosis 1- Anemia ± thrombocytopenia ± neutropenia RBC: variable morphology with decreased reticulocyte count. WBC: decrease in granulocytes and abnormal function. Platelet: either too large or too small and thrombocytopenia. 2- Bone marrow : dysmyelopoiesis in bone marrow precursors 3- Chromosomal Abnormalities:5,7,8 ,others

16
MDS Management 1- Symptomatic (transfusion, antibiotics)
2- Growth factors: Erythropoietin,G-CSF. 3- Cytotoxics for RAEB & RAEB-T&CMML 4- Bone marrow transplant for young patients with advanced disease. 5- Immune modulating and differentiating agents .

17
Summary Anemia of chronic disease may be confused with iron deficiency anemia, but the serum ferritin is normal. Anemia of chronic disease is usually mild except in chronic renal failure were it responds well to erythropoietin injections. Aplastic anemia presents with anemia ,repeated infections and bleeding tendency due to pancytopenia and hypocelluar marrow. Idiopathic aplastic anemia is best treated with allogeneic bone marrow transplantation for patients younger than 45 years old. Idiopathic aplastic anemia of older patients is treated with antithymocye globulin and ciclosporin A. Supportive treatment is essential for aplastic anemia. Myelodysplastic syndrome is a group of disorders affecting bone marrow stem cells that result in dysplastic changes, di or pancytopenia and tendency to transform into AML. Patients need supportive treatment. Chemotherapy and bone marrow transplantation are reserved for fit patients with transformation into AML.

Similar presentations



















:>")