Download presentation
Presentation is loading. Please wait.

1
Red cell membrane defects

2
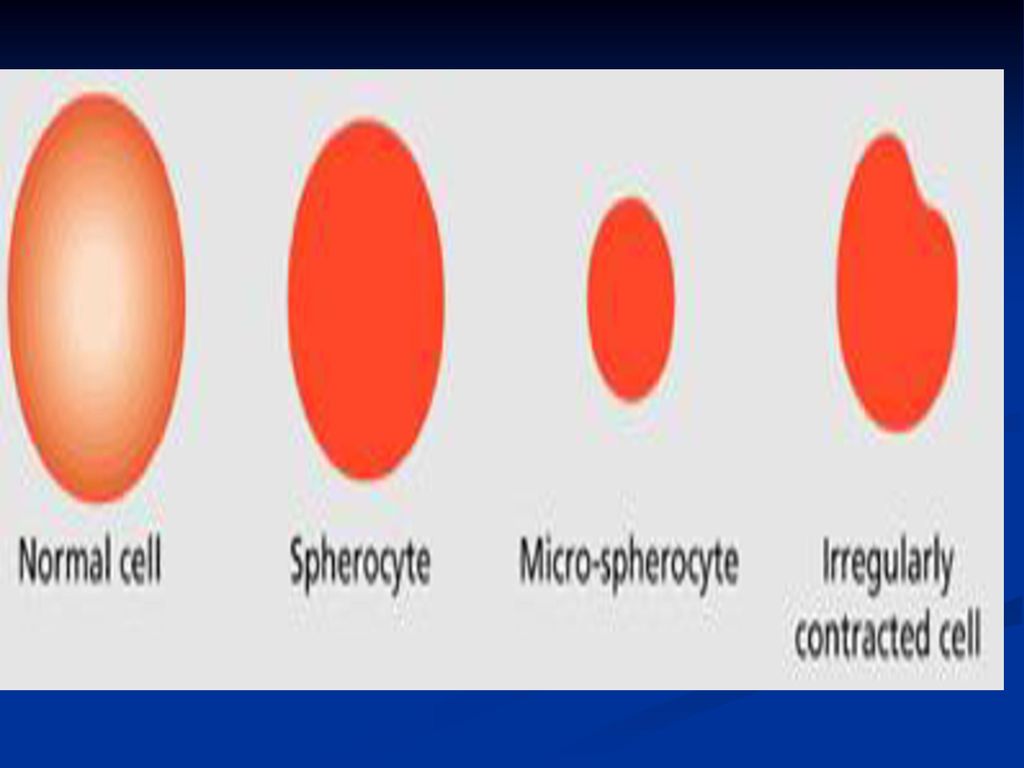
Hereditary spherocytosis (HS)
The most common of the inherited RBC membrane defects, affecting 1 in 5000 individuals. The disorder characterized by RBC that appear spherical on peripheral blood smear. Autosomal dominant disorder. 25% of pts have no family history.

3
Pathophysiology The abnormal red cells lysis is caused by a defect in cytoskeleton : involves a partial deficiency of spectrin (RBC membrane protein). The spherical shape has two effects on RBC. 1.they become trapped in the splenic cord. 2.they have shortened life span. The abnormal membrane also demonstrate an increased permeability of sodium
. The spherical shape has two effects on RBC. 1.they become trapped in the splenic cord. 2.they have shortened life span. The abnormal membrane also demonstrate an increased permeability of sodium.")
4
Clinical manifestation
The typical HS pts is relatively asymptomatic with well compensated hemolysis and palpable spleen. The rare pts with severe HS may present early in childhood with life threatening hemolysis. HS has the usual features of chronic hemolysis : *symptoms of anaemia. *splenomegaly. *gall stones. crisis *Aplastic crisis ,hemolytic and megaloblastic #Family members have mild form of the disorder or are carrier.

5
Diagnosis *Suggested by a family history of HS and characteristic finding on PBS i.e.* spherocytes. Two studies are used to confirm the diagnosis. 1. osmotic fragility test. A positive test shows lysis of the patients red cells at hypotonic saline solution compared to simple swelling in normal cells. 2. Autohemolysis test : Normal autohemolysis is about 1% while HS cells will display Hb release rate of 3% or more 3-flow cytometric tests, detecting binding of eosin-5-maleimide to red cells, are recommended in borderline cases

7
The classic finding is that the osmotic fragility is increased.
Diagnosis-cont. The classic finding is that the osmotic fragility is increased. Autohaemolysis is increased and corrected by glucose. Direct antiglobulin test is negative..

9
Autohaemolysis test in HS
There is increased haemolysis in the patient in comparison with the control. Glucose has given partial correction.

10
Treatment 1.Asymptomatic pts with compensated hemolysis should receive supportive treatment with folate supplements 5mg for life. 2.Aplastic crisis may require short period of blood transfusion. 3.Splenectomy is curative in most pts with HS.

11
Guide line for performing splenectomy
1. performed only when necessary i.e moderate to severe hemolysis with complication (pts who required blood transfusion,gall stones) 2. should be avoided in pts younger than 6 years of age ,associated risk (fatal pneumonia, sepsis) 3. may be performed with cholecystectomy to decrease the amount of hemolysis and the risk of gall stones development.
 2. should be avoided in pts younger than 6 years of age ,associated risk (fatal pneumonia, sepsis) 3. may be performed with cholecystectomy to decrease the amount of hemolysis and the risk of gall stones development.")
12
Management of the splenectomised patient

13
Red cell enzymopathies
G6PD functions to reduce nicotinamide adenine dinucleotide phosphate (NADPH) while oxidizing glucose-6-phosphate. NADPH is needed for the production of reduced glutathione (GSH) which is important to defend the red cells against oxidant stress.
 while oxidizing glucose-6-phosphate. NADPH is needed for the production of reduced glutathione (GSH) which is important to defend the red cells against oxidant stress.")
14
Red cell enzymopathies
Anaerobic glycolysis via; the Embden–Meyerhof pathway generates ATP, and the hexose monophosphate shunt; produces nicotinamide adenine dinucleotide phosphate (NADPH) and glutathione to protect against oxidative stress. In general, defects in the hexose monophosphate shunt pathway result in periodic haemolysis precipitated by episodic oxidative stress, whilst those in the Embden–Meyerhof pathway result in shortened red cell survival and chronic haemolysis. .
 and glutathione to. protect against oxidative stress. In general, defects in the hexose monophosphate shunt pathway result in periodic haemolysis precipitated by episodic oxidative stress, whilst those in the Embden–Meyerhof pathway result. in shortened red cell survival and chronic haemolysis. .")
15
Red cell housekeeping enzymes :
1. The embden-Meyerhof Pathway : for glycolysis provides energy for : a. Na+, K+ and Ca+2 pumps in the cell membrane. b. phosphorylation of membrane components and synthesis of glutathione for protection from oxidative damage. c. reduction of NAD to NADH which is important in reducing met-hemoglobin to hemoglobin.

16
2.The pentose-phosphate shunt :
maintains levels of NADH which is important in the reduction of oxidized glutathione (GSSH) to reduced glutathione (GSH). GSH is important in : a. destroying the oxidant hydrogen peroxide with glutathione peroxidase. b. maintaining sulphhydryl group in Hb. and in various enzymes and within the cell membrane.
 to reduced glutathione (GSH). GSH is important in : a. destroying the oxidant hydrogen peroxide with glutathione peroxidase. b. maintaining sulphhydryl group in Hb. and in various enzymes and within the cell membrane.")
17
Oxidant hemolysis (enzymopathy)
1. Glucose – 6- phosphate dehydrogenase (G6PD) deficiency : X-linked disorder. G6PD is important for generation of both NAD and NADH as well as glutathione, which is required for reduction or protection of sulfhydroxyl groups. Enzyme variants : Normal forms: Two forms of G6PD have normal activity, B form and A form or (A+) & (B+).
 deficiency : X-linked disorder. G6PD is important for generation of both NAD and NADH as well as glutathione, which is required for reduction or protection of sulfhydroxyl groups. Enzyme variants : Normal forms: Two forms of G6PD have normal activity, B form and A form or (A+) & (B+).")
18
Deficiency forms: (A-) isoenzyme & Mediterranean isoenzyme. *Enzyme may exist at normal intracellular levels but have decrease activity. *May be unstable lead to increased break down in red cells.
 isoenzyme & Mediterranean isoenzyme. *Enzyme may exist at normal intracellular levels but have decrease activity. *May be unstable lead to increased break down in red cells.")
19
Pathophysiology the daily destruction of RBC, Hb is being constantly oxidized to met Hb. but a special protective mechanism that uses the E.M pathway reduces it back to Hb this is important because; Met-hemoglobin dissociates into heme and globin and then precipitates as an insoluble mass (Heinz body) in the RBCs. These red cells with Heinz body are non deformable and have difficulty passing through the spleen. Splenic removal of Heinz bodies damages RBCs membrane, forming spherocytes and causing hemolysis.
 in the RBCs. These red cells with Heinz body are non deformable and have difficulty passing through the spleen. Splenic removal of Heinz bodies damages RBCs membrane, forming spherocytes and causing hemolysis.")
20
Precipitating factors
1.oxidant drugs : (antimalarial, antipyretic, sulfonamide and related group, nitrofurantion,) (moth ball) 2.fava beans(Favism). 3.Infection (resp. viruses, hepatitis, infectious mononucleosis , bacterial preumonia, and septicemia). 4.Stressful conditions: diabetic ketoacidosis,uraemia
 (moth ball) 2.fava beans(Favism). 3.Infection (resp. viruses, hepatitis, infectious mononucleosis , bacterial preumonia, and septicemia). 4.Stressful conditions: diabetic ketoacidosis,uraemia.")
21
Clinical manifestations
1. General features, patient with G6PD deficiency display signs and symptoms of IV hemolysis. The deficiency usually is episodic and occasionally is chronic. 2. patient with the common (A-)form of G6PD deficiency generally have mild hemolysis only when stressed.*hemolysis is self-limited,reticulocyte have high levels of the enzyme thus, compensating for the decreased activity. 3. patients with the rare Mediterranean form of G6PD deficiency :- severe hemolysis when exposed to oxidants or stressed by surgery or infectionthe hemolysis persist as long as the stress or oxidant persists.
form of G6PD deficiency generally have mild hemolysis only when stressed.*hemolysis is self-limited,reticulocyte have high levels of the enzyme thus, compensating for the decreased activity. 3. patients with the rare Mediterranean form of G6PD deficiency :- severe hemolysis when exposed to oxidants or stressed by surgery or infectionthe hemolysis persist as long as the stress or oxidant persists.")
22
Diagnosis 1. red cell enzyme levels measured by electrophoresis show very low activities in severe disease and low to normal activity in mild disease depending on when the test is performed. measurement should not be taken at the time of hemolysis and reticulocytosis 2. Heinz bodies can be demonstrated only during early phase of G6PD deficiency. characteristic of IV hemolysis.

23
Diagnosis Heinz bodies
The blood film shows irregularly contracted cells [deep red arrows] and sometimes hemighosts [deep blue arrow] in which all the haemoglobin appears to have retracted to one side of the erythrocyte Heinz bodies

24
Treatment 1.primary therapy is to avoid oxidative agents. 2.recovery is rapid , but if the anaemia is severe transfusion of red cells with normal enzyme complement may be required. 3.Splenectomy is without value.

25
Pyruvate kinase(PK) deficiency
*Congenital non-spherocytic hemolytic anaemia(CNSHA). *Autosomal recessive. *Characterized by decreased generation of ATP. *Impairement of glycolysis lead to increased 2,3 DPG level.
. *Autosomal recessive. *Characterized by decreased generation of ATP. *Impairement of glycolysis lead to increased 2,3 DPG level.")
26
Clinical manifestation
1.-chronic hemolytic syndrome of variable severity. 2.severe deficient may be apparent in neonatal stage. 3.-may be a symptomatic. 4.-manifestation (reticulocytosis, marrow hyperplasia, splenomegaly, jaundice, gall stone).
.")
27
Diagnosis *measuring PK enzyme level in red cells Treatment : 1.depend on severity of anaemia. folate supplements, 2.Splenectomy

Similar presentations



. Introduction Hereditary spherocytosis is a class of hemolytic anemia. The disease occurs due to an intrinsic “membrane.>")






 Course code: MLHE-201 Supervisor: Prof. Dr Magda Sultan Outcome : The student will know : -The types of hemolytic anemias.>")





i.>")
 Course code: MLHE-201 Supervisor: Prof>")


