Download presentation
Presentation is loading. Please wait.

1
Autoimmune Liver Disease
Title Slide Autoimmune Liver Disease Slide 1 Title Slide

2
Definition Chronic cholestatic liver disease
Definition – PSC Primary Sclerosing Cholangitis Definition Chronic cholestatic liver disease Unknown etiology, frequently associated with Inflammatory Bowel Disease Diffuse inflammation and fibrosis of the biliary tree Leads to biliary cirrhosis and portal hypertension Slide 5 Definition – PSC These features help define primary sclerosing cholangitis. Recent reviews include: Mendes FD, Lindor KD. Primary sclerosing cholangitis. Clin Liver Dis 2004;8: Talwalkar JA, Lindor KD. Primary sclerosing cholangitis. Inflamm Bowel Dis 2005;11:62-72.

3
Etiology Unknown Disordered immunoregulation
Primary Sclerosing Cholangitis Etiology Unknown Disordered immunoregulation T-cell subsets altered T-cell suppressor function abnormal Circulating immune complexes Abnormal complement levels Infections and bacterial products Portal bacteremia Slide 6 Etiology Unknown The etiology of primary sclerosing cholangitis is unknown. Potential etiologies are described on this slide and include: disordered immunoregulation, infectious or bacterial products, and portal bacteremia.

4
Clinical Picture Cholestasis (elevated alkaline phosphatase)
Primary Sclerosing Cholangitis Clinical Picture Cholestasis (elevated alkaline phosphatase) Usually in setting of colitis May be asymptomatic Abnormal cholangiogram diagnostic Slide 7 Clinical Picture Most patients with primary sclerosing cholangitis come to medical attention because of the finding of elevated cholestatic liver enzymes, sometimes in the setting of symptoms, other times because of screening of patients with colitis because of the predisposition to liver disease. Patients now less frequently present with symptoms of cholestasis such as jaundice or itching, and many patients now are totally asymptomatic. An abnormal cholangiogram is the diagnostic study of choice. The role of a liver biopsy is being redefined. Not every patient appears to need a liver biopsy.
 Usually in setting of colitis. May be asymptomatic. Abnormal cholangiogram diagnostic. Slide 7. Clinical Picture. Most patients with primary sclerosing cholangitis come to medical attention because of the finding of elevated cholestatic liver enzymes, sometimes in the setting of symptoms, other times because of screening of patients with colitis because of the predisposition to liver disease. Patients now less frequently present with symptoms of cholestasis such as jaundice or itching, and many patients now are totally asymptomatic. An abnormal cholangiogram is the diagnostic study of choice. The role of a liver biopsy is being redefined. Not every patient appears to need a liver biopsy.")
5
Clinical Presentation
Primary Sclerosing Cholangitis Clinical Presentation Asymptomatic % Symptomatic Fatigue 75 Pruritus 70 Jaundice 30-69 Hepatomegaly Abdominal pain 16-37 Weight loss 10-34 Splenomegaly 30 Ascending cholangitis 5-28 Hyperpigmentation 25 Variceal bleeding 2-14 Ascites 2-10 Slide 8 Clinical Presentation The symptoms at presentation can vary between patients. An increasing proportion of patients are found to be asymptomatic at presentation and signs of more advanced liver disease are becoming less frequent at the time of diagnosis. Vierling JM. In: Zakim & Boyer, eds. Hepatology 2003:1221.

6
Relationship to Inflammatory Bowel Disease
Relationship to IBD Primary Sclerosing Cholangitis Relationship to Inflammatory Bowel Disease IBD in 60-80% of PSC patients CUC more common than Crohn’s disease (2:1) In PSC, Crohn’s disease almost always involves the colon 4-5% of CUC patients have PSC Slide 11 Relationship to IBD This slide summarizes the relationship of inflammatory bowel disease to primary sclerosing cholangitis.
 In PSC, Crohn’s disease almost always involves the colon. 4-5% of CUC patients have PSC. Slide 11. Relationship to IBD. This slide summarizes the relationship of inflammatory bowel disease to primary sclerosing cholangitis.")
7
Primary Sclerosing Cholangitis in Colitis
Chronic ulcerative colitis PSC Slide 10 Primary Sclerosing Cholangitis in Colitis Primary sclerosing cholangitis is commonly associated with ulcerative colitis. It is estimated that 3-7% of patients with ulcerative colitis will develop primary sclerosing cholangitis. In contrast, about 70% of patients with primary sclerosing cholangitis will have underlying ulcerative colitis. The approximate prevalence of these conditions is shown here. 50/106 2000/106 100/106 (Estimated prevalence)
")
8
Diagnostic Criteria Primary Sclerosing Cholangitis Diagnostic Criteria Typical cholangiographic abnormalities involving any part of the biliary tree Compatible clinical and biochemical findings History of IBD, cholestatic symptoms Two- to three-fold increase in serum alkaline phosphatase level > 6 mos. Slide 12 Diagnostic Criteria The diagnostic criteria rely mostly on cholangiographic abnormalities, although a small proportion of patients (about 5%) may have a normal cholangiogram but compatible histological features. This is small-duct PSC.
 may have a normal cholangiogram but compatible histological features. This is small-duct PSC.")
9
Diagnostic Criteria Exclude: AIDS cholangiopathy
Primary Sclerosing Cholangitis Diagnostic Criteria Exclude: AIDS cholangiopathy Bile duct neoplasm (unless previous diagnosis of PSC) Biliary tract surgery or trauma Choledocholithiasis Congenital abnormalities of biliary tract Caustic treatment of intrahepatic cysts Ischemic stricturing of bile ducts Stricturing related to intra-arterial infusion of chemotherapy Slide 13 Diagnostic Criteria Diagnostic criteria include the exclusion of a variety of other causes of a similar cholangiographic feature as outlined on this slide.
 Biliary tract surgery or trauma. Choledocholithiasis. Congenital abnormalities of biliary tract. Caustic treatment of intrahepatic cysts. Ischemic stricturing of bile ducts. Stricturing related to intra-arterial infusion of chemotherapy. Slide 13. Diagnostic Criteria. Diagnostic criteria include the exclusion of a variety of other causes of a similar cholangiographic feature as outlined on this slide.")
10
Liver Tests Alkaline phosphatase nearly always elevated
Primary Sclerosing Cholangitis Liver Tests Alkaline phosphatase nearly always elevated AST and ALT usually <5 times normal Bilirubin, albumin, prothrombin time usually normal at diagnosis Slide 14 Liver Tests Typical biochemical findings are seen here. Cholestatic enzymes such as alkaline phosphatase are prominently elevated.

11
Prevalence of Autoantibodies in PSC
Primary Sclerosing Cholangitis Prevalence of Autoantibodies in PSC p-ANCA 80% AMA <2% ANA % SMA 35% Slide 15 Prevalence of Autoantibodies in PSC A variety of autoantibodies can be seen in primary sclerosing cholangitis. Antinuclear and p-ANCA antibodies are the most common. Antimitochondrial antibodies are characteristic in PBC and are rare in patients with PSC. Autoantibodies shown in the slide are: p-ANCA=.perinuclear antineutrophil cytoplasmic antibody, AMA = antimitochondrial, ANA = antinuclear, SMA = smooth muscle antibodies

12
Diagnosis – Cholangiography
Primary Sclerosing Cholangitis Diagnosis - Cholangiography ERCP most commonly used Percutaneous cholangiography infrequently used Magnetic resonance cholangiography non-invasive no radiation cost-effective Slide 17 Diagnosis – Cholangiography Diagnosis is based on cholangiography. Magnetic resonance cholangiography is certainly emerging as a cost-effective initial step in the diagnosis of suspected PSC and CT cholangiography is being evaluated as well.

13
PSC Involving Intrahepatic Ducts
Primary Sclerosing Cholangitis PSC Involving Intrahepatic Ducts Slide 22 PSC Involving Intrahepatic Ducts

14
Concentric Fibrosis in PSC
Bile duct Concentric fibrosis Slide 27 Concentric Fibrosis in PSC In PSC, the concentric fibrosis encasing the interlobular bile duct is the “classic” histologic lesion.

15
Biliary Cirrhosis Slide 33 Biliary Cirrhosis
Biliary cirrhosis is frequently characterized by inhomogenous involvement of the liver parenchyma, thus, as illustrated, there is a complete nodule on the top right, but only bridging fibrosis on the left part of the field. The terminal hepatic venule is not incorporated into septa until very late, if at all. Ultimately, the pattern is one referred to as “jig saw”, and can be seen in this photomicrograph.

16
Small-Duct PSC 5% of PSC Normal cholangiogram but biopsy showing PSC
Primary Sclerosing Cholangitis Small-Duct PSC 5% of PSC Normal cholangiogram but biopsy showing PSC Can progress to classic PSC May exist with or without colitis Slide 37 Small-Duct PSC Small-duct PSC is a relatively uncommon variant of primary sclerosing cholangitis characterized by an abnormal cholangiogram but compatible histology. Angulo P, Maor-Kendler Y, Lindor KD. Small-duct primary sclerosing cholangitis: A long-term follow-up study. Hepatology :

17
Differentiating PSC from PBC
Primary Sclerosing Cholangitis Differentiating PSC from PBC PSC PBC Cholestasis + + History of colitis + - AMA - + Liver biopsy onion skin florid duct fibrosis lesion Cholangiogram abnormal normal Slide 39 Differentiating PSC from PBC Primary biliary cirrhosis is the most common chronic cholestatic condition in adults but can be differentiated from primary sclerosing cholangitis by the presence of antimitochondrial antibodies in PBC and the presence of abnormal cholangiograms in patients with PSC.

18
Features Used In Prognostic Models
Primary Sclerosing Cholangitis Features Used in Prognostic Models Mayo Clinic King’s Multicenter Swedish New Mayo College Model (n=174) (n=126) (n=426) (n=305) (n=405) Age Age Age Age Age Bilirubin Hepatomegaly Bilirubin Bilirubin Bilirubin Biopsy Stage Biopsy Stage Biopsy Stage Biopsy Stage AST Hemoglobin Splenomegaly Splenomegaly Variceal Bleed Inflammatory Alkaline Albumin Bowel Phosphatase disease Slide 42 Features Used In Prognostic Models This is a tabulation of the various prognostic models that have been used. Age, bilirubin, and histological stage are commonly used factors. The new Mayo model has the advantage of not requiring histology.
 (n=126) (n=426) (n=305) (n=405) Age Age Age Age Age. Bilirubin Hepatomegaly Bilirubin Bilirubin Bilirubin. Biopsy Stage Biopsy Stage Biopsy Stage Biopsy Stage AST. Hemoglobin Splenomegaly Splenomegaly Variceal. Bleed. Inflammatory Alkaline Albumin. Bowel Phosphatase. disease. Slide 42. Features Used In Prognostic Models. This is a tabulation of the various prognostic models that have been used. Age, bilirubin, and histological stage are commonly used factors. The new Mayo model has the advantage of not requiring histology.")
19
Disease Specific Therapy
Primary Sclerosing Cholangitis Disease Specific Therapy Surgical therapy seldom used Dilation for dominant strictures No proven medical therapy Slide 43 Disease Specific Therapy A variety of therapies have been tested, but none have been shown to be of clear benefit for the treatment of primary sclerosing cholangitis.

20
Management of Cholestasis
Primary Sclerosing Cholangitis Management of Cholestasis Vitamin Deficiency A 40% D 14% E 2% K Slide 45 Management of Cholestasis Fat-soluble vitamin deficiencies as shown in this table are common and are more frequently found in patients with advanced disease. Jorgensen RA, Lindor KD, Sartin JS, LaRusso NF, Wiesner RH. Serum lipid and fat-soluble vitamin levels in primary sclerosing cholangitis. J Clin Gastroenterol 1995;20(3):215-9. Unknown
: Unknown.")
21
Management of Cholestasis
Primary Sclerosing Cholangitis Management of Cholestasis Metabolic Bone Disease Osteoporosis much more common than osteomalacia Hormone replacement in women Calcium + vitamin D helpful Bisphosphonates may be helpful Steroid therapy may worsen bone disease Calcitonin not helpful Slide 46 Management of Cholestasis Metabolic bone disease can be quite troublesome in patients with primary sclerosing cholangitis, just as in PBC. A variety of therapies have been tested in cholestatic osteoporosis, but almost always in PBC rather than PSC. Recently, oral bisphosphonates appear to be the best option for patients with cholestatic osteoporosis. Osteomalacia from vitamin D deficiency is rare but occurs particularly in patients with advanced disease. This can be readily managed with vitamin D replacement. All patients with cholestasis should receive supplemental calcium. Angulo P, Therneau TM, Jorgensen R, et al. Bone disease in patients with primary sclerosing cholangitis: prevalence, severity and prediction of progression. J Hepatol 1998;29: Zein CO, Jorgensen RA, Clarke B, Wenger DE, Keach, JC, Angulo P, Lindor KD. Alendronate improves bone mineral density in primary biliary cirrhosis: a randomized placebo-controlled trial. Hepatology 2005;42:

22
Management of Cholestasis
Primary Sclerosing Cholangitis Management of Cholestasis Steatorrhea Diminished bile salts in gut Chronic pancreatitis Co-existent celiac disease Slide 47 Management of Cholestasis Patients with primary sclerosing cholangitis can develop steatorrhea. The most common reason is diminished bile salt delivery to the gut, but chronic pancreatitis and celiac disease can underlie some cases.

23
Management of Biliary Strictures
Primary Sclerosing Cholangitis Management of Biliary Stricture Uncommon Cytology insensitive Molecular methods being evaluated Long-term stents may cause problems Dilatation alone seems preferable Slide 49 Management of Biliary Strictures Biliary strictures are uncommon but worrisome when they occur. The etiology needs to be determined. Causes include isolated dominant strictures, impacted stones, or development of cholangiocarcinoma. Biopsies and particularly brush cytology have been insensitive for detecting malignancies within strictures. Digital image analysis and fluorescent in situ hybridization are more sensitive. Elevated CA-19-9 level in a patient with a dominant stricture is a worrisome sign that carcinoma might be present. Dilation for strictures is recommended. However, long-term stenting is not recommended because of the increased risk of biliary obstruction from the stent and the need for repeat stent changes.

24
Other cancers: pancreatic, liver, and colon
Cancer Risk Primary Sclerosing Cholangitis Cancer Risk Cholangiocarcinoma Lifetime risk 7-15% Incidence 0.5 to 1% Smoking and IBD may increase risk Slide 50 Cancer Risk Cholangiocarcinoma is the most feared complication of PSC. Life-time risk is in the range of 7-15%. These patients are also at risk of other GI malignancies. Other cancers: pancreatic, liver, and colon

25
Risk of Colon Cancer in CUC and PSC
Primary Sclerosing Cholangitis Risk of Colon Cancer in CUC and PSC Compared to CUC Alone Cumulative probability 0.2 0.6 0.8 1.0 0.4 Years p=0.0571 CUC + PSC CUC alone 3 7 10 1 5 8 2 4 6 9 Slide 59 Risk of Colon Cancer in CUC and PSC Compared to CUC Alone Ulcerative colitis is a risk factor for colon cancer, and according to two recent studies this risk may be increased in the setting of primary sclerosing cholangitis. Loftus EV et al Gut; 2005:91

26
Liver Transplantation for PSC
Primary Sclerosing Cholangitis Liver Transplantation for PSC Survival 1 year 90-97% 5 years 85-88% Problems with rejection, infection, recurrence, colon cancer Slide 60 Liver Transplantation for PSC Liver transplantation has an excellent outcome for patients with primary sclerosing cholangitis with a one year survival sometimes approaching 97 percent. These patients can develop problems with rejection and have an increased risk of rejection and infection compared to patients with other liver diseases. As with many other liver diseases, PSC can recur post-transplant, and the risk of colon cancer in the setting of CUC may be increased.

27
Treatment Recommendations
Primary Sclerosing Cholangitis Treatment Recommendations No standard medical therapy Cancer surveillance Hepatitis A & B vaccination Antibiotics for cholangitis Screen for varices Dilate symptomatic strictures Assess for osteoporosis and vitamin deficiency in advanced disease Slide 61 Treatment Recommendations Primary sclerosing cholangitis has no known standard medical therapy. Avoidance of other causes of liver disease and management of the complications of portal hypertension and advanced cholestasis are all warranted.

28
Overview Definition Natural history Clinical features Diagnosis
Primary Biliary Cirrhosis Overview Definition Natural history Clinical features Diagnosis Pathology Management Complications Transplantation Slide 63 Overview – PBC

29
Definition Chronic cholestatic liver disease
Definition - PBC Primary Biliary Cirrhosis Definition Chronic cholestatic liver disease Serum anti-mitochondrial antibody Non-suppurative destructive cholangitis on liver histology Slide 64 Definition – PBC Primary biliary cirrhosis is a chronic cholestatic liver disease of adults. This disorder is characterized histologically by chronic non-suppurative destruction of interlobular bile ducts leading to advanced fibrosis, cirrhosis, and liver failure. Presence of antimitochondrial antibody in serum is almost diagnostic of the disorder. The portal tract in the picture shows a dense mixed chronic inflammatory infiltrate and the bile duct (in the right portion of the portal tract) has a florid duct lesion. Talwalkar JA, Lindor KD. Primary biliary cirrhosis. Lancet 2003;362:53-61. Talwalkar JA, Lindor KD. Lancet 2003
 has a florid duct lesion. Talwalkar JA, Lindor KD. Primary biliary cirrhosis. Lancet 2003;362: Talwalkar JA, Lindor KD. Lancet")
30
Natural History: Risk Factors
Natural History – PBC Primary Biliary Cirrhosis Natural History: Risk Factors Female gender Autoimmune thyroid disease Prior urinary tract infection History of previous tonsillectomy Smoking Inflammatory skin disease (psoriasis, eczema) Genetic predisposition Slide 68 Natural History – PBC Several case-control investigations have attempted to determine what exposures may be responsible for the development of PBC in susceptible hosts. The major potential risk factors observed in patients with PBC versus unaffected controls are female sex, cigarette smoking, inflammatory diseases of the skin and thyroid, history of urinary tract infection, previous tonsillectomy, and genetic predisposition. Parikh-Patel A, Gold EB, Worman H, Krivy KE, Gershwin ME. Risk factors for primary biliary cirrhosis in a cohort of patients from the united states. Hepatology 2001;33:16-21. Howel D, Fischbacher CM, Bhopal RS, Gray J, Metcalf JV, James OF. An exploratory population-based case-control study of primary biliary cirrhosis. Hepatology 2000;31: Howel D et al, Hepatology Parikh-Patel A et al, Hepatology 2001
 Genetic predisposition. Slide 68. Natural History – PBC. Several case-control investigations have attempted to determine what exposures may be responsible for the development of PBC in susceptible hosts. The major potential risk factors observed in patients with PBC versus unaffected controls are female sex, cigarette smoking, inflammatory diseases of the skin and thyroid, history of urinary tract infection, previous tonsillectomy, and genetic predisposition. Parikh-Patel A, Gold EB, Worman H, Krivy KE, Gershwin ME. Risk factors for primary biliary cirrhosis in a cohort of patients from the united states. Hepatology 2001;33: Howel D, Fischbacher CM, Bhopal RS, Gray J, Metcalf JV, James OF. An exploratory population-based case-control study of primary biliary cirrhosis. Hepatology 2000;31: Howel D et al, Hepatology 2000 Parikh-Patel A et al, Hepatology")
31
Clinical Features at Presentation – PBC
Primary Biliary Cirrhosis Clinical Features at Presentation Asymptomatic 40-60% Fatigue +++ Pruritus ++ Sicca symptoms +++ Hepatomegaly + Splenomegaly + Jaundice uncommon Xanthelasma uncommon Slide 71 Clinical Features at Presentation – PBC The frequency and severity of clinical features associated with PBC at initial presentation have changed over time. Nearly 50% of cases are now identified among patients without symptoms. While fatigue and sicca syndrome remain common, the frequency and intensity of pruritus have lessened over time. Symptoms and signs of advanced disease including hepatosplenomegaly, jaundice, and xanthelasma are rarely observed in current clinical practice. Talwalkar JA, Lindor KD. Primary biliary cirrhosis. Lancet 2003;362:53-61.

32
Fatigue in PBC Most common symptom Frequency 0 - 80%
Primary Biliary Cirrhosis Fatigue in PBC Most common symptom Frequency % No association with age, sex, histological stage, bilirubin, and Mayo Risk score Etiology unknown Slide 72 Fatigue in PBC Natural history and controlled trial investigations have reported the presence of fatigue variably ranging from 0% to 76% of affected patients. For asymptomatic patients at diagnosis, the cumulative risk for developing fatigue over a 5-year period is substantial at nearly 50%. Further investigation reveals that fatigue is independent of hepatic disease severity, sleep disturbance, or depression. Fatigue is not significantly improved with ursodeoxycholic acid therapy. Alterations in central neurotransmission and impaired corticotrophin-releasing hormone response have been hypothesized as mechanisms of fatigue in PBC. Leuschner U. Primary biliary cirrhosis--presentation and diagnosis. Clin Liver Dis 2003;7: Leuschner U. Clin Liv Dis 2003; 7:741

33
Biochemical Features of PBC
Primary Biliary Cirrhosis Biochemical Features of PBC Alkaline Phosphatase almost always elevated (generally 3-4x normal) AST, ALT < 200 U/L Bilirubin - usually rises late Cholesterol elevated in 85% IgM - commonly elevated Slide 73 Biochemical Features of PBC The most characteristic biochemical abnormality in PBC is an elevated serum alkaline phosphatase (usually 3 to 4 times the upper limit of normal). No association exists between the level of serum alkaline phosphatase elevation and prognosis prior to initiation of medical therapy. Modestly increased values for alanine aminotransferase (ALT) and aspartate aminotransferase (AST) are common, but significant elevations (greater than 200 U/L) requires the exclusion of superimposed viral or drug-induced hepatic injury. Serum total bilirubin levels often rise during disease progression but are commonly within normal limits at the time of diagnosis. Hypercholesterolemia is observed in up to 85% of cases at diagnosis. Serum IgM levels and bile acids (cholic acid, chenodeoxycholic acid) are also elevated in patients with PBC. Talwalkar JA, Lindor KD. Primary biliary cirrhosis. Lancet 2003;362:53-61.
 AST, ALT < 200 U/L. Bilirubin - usually rises late. Cholesterol elevated in 85% IgM - commonly elevated. Slide 73. Biochemical Features of PBC. The most characteristic biochemical abnormality in PBC is an elevated serum alkaline phosphatase (usually 3 to 4 times the upper limit of normal). No association exists between the level of serum alkaline phosphatase elevation and prognosis prior to initiation of medical therapy. Modestly increased values for alanine aminotransferase (ALT) and aspartate aminotransferase (AST) are common, but significant elevations (greater than 200 U/L) requires the exclusion of superimposed viral or drug-induced hepatic injury. Serum total bilirubin levels often rise during disease progression but are commonly within normal limits at the time of diagnosis. Hypercholesterolemia is observed in up to 85% of cases at diagnosis. Serum IgM levels and bile acids (cholic acid, chenodeoxycholic acid) are also elevated in patients with PBC. Talwalkar JA, Lindor KD. Primary biliary cirrhosis. Lancet 2003;362:")
34
Serum Antibodies in PBC
Primary Biliary Cirrhosis Serum Antibodies in PBC Type Prevalence AMA ++++ ANA +++ ASMA ++ Anti-Centromere + Anti-Gp210 ++ Anti-Sp100 ++ p-ANCA + Slide 74 Serum Antibodies in PBC A number of serum autoantibodies are recognized in association with PBC. Between 90% and 95% of patients have positive serum AMA tiers. Of note, an estimated 8-10% of cases with autoimmune hepatitis and a small proportion of PSC cases are AMA seropositive. Serum antinuclear antibody (ANA) and/or smooth muscle antibody (SMA) in 35% -66% of cases. Serum anti-centromere antibodies occur mainly in patients with scleroderma (10%-15% of PBC cases). Other autoantibodies include anti-Gp210, anti-Sp100, and p-ANCA. Jones DE. Autoantigens in primary biliary cirrhosis. J Clin Pathol 2000;53:
 and/or smooth muscle antibody (SMA) in 35% -66% of cases. Serum anti-centromere antibodies occur mainly in patients with scleroderma (10%-15% of PBC cases). Other autoantibodies include anti-Gp210, anti-Sp100, and p-ANCA. Jones DE. Autoantigens in primary biliary cirrhosis. J Clin Pathol 2000;53:")
35
AMA-Negative PBC Occurs in 5%-10% of all cases
Primary Biliary Cirrhosis AMA-Negative PBC Occurs in 5%-10% of all cases No evidence of extrahepatic biliary obstruction No difference in clinical presentation, natural history and prognosis compared to AMA-positive cases Response to medical therapy similar to AMA- positive individuals High prevalence of serum ANA Slide 75 AMA-Negative PBC Approximately 5% to 10% of patients with features otherwise consistent with primary biliary cirrhosis (PBC) lack antimitochondrial antibodies (AMA). In controlled trials, the characteristics of AMA-negative patients at presentation were similar to those of AMA-positive patients with PBC. The clinical outcomes and sequential liver biochemistries of UDCA treatment were also comparable with those of AMA-positive patients. Among 6 patients with AMA-negative PBC compared to 79 patients with AMA-positive PBC, graft and patient survival rates and subsequent histological changes (disease recurrence and steroid-resistant or late rejections) were similar. Kim WR, Poterucha JJ, Jorgensen RA, Batts KP, Homburger HA, Dickson ER, Krom RA, Wiesner RH, Lindor KD. Does antimitochondrial antibody status affect response to treatment in patients with primary biliary cirrhosis? Outcomes of ursodeoxycholic acid therapy and liver transplantation. Hepatology Jul;26(1):22-6.
 lack antimitochondrial antibodies (AMA). In controlled trials, the characteristics of AMA-negative patients at presentation were similar to those of AMA-positive patients with PBC. The clinical outcomes and sequential liver biochemistries of UDCA treatment were also comparable with those of AMA-positive patients. Among 6 patients with AMA-negative PBC compared to 79 patients with AMA-positive PBC, graft and patient survival rates and subsequent histological changes (disease recurrence and steroid-resistant or late rejections) were similar. Kim WR, Poterucha JJ, Jorgensen RA, Batts KP, Homburger HA, Dickson ER, Krom RA, Wiesner RH, Lindor KD. Does antimitochondrial antibody status affect response to treatment in patients with primary biliary cirrhosis Outcomes of ursodeoxycholic acid therapy and liver transplantation. Hepatology Jul;26(1):22-6.")
36
Florid Duct Lesion Slide 83 Florid Duct Lesion
The portal tract is markedly expanded by a mixed chronic inflammatory infiltrate; numerous plasma cells and eosinophils are present. In the center is a bile duct that is being infiltrated by inflammatory cells. This is the “florid duct lesion” of PBC.

37
Pruritus Frequency between 20-60% of cases Insidious onset
Puritus Primary Biliary Cirrhosis Pruritus Frequency between 20-60% of cases Insidious onset May be intractable No association with age, sex, histological stage, and Mayo Risk score Etiology unknown Slide 90 Puritus Pruritus is reported in 25%-70% of patients affected by PBC. Increased serum alkaline phosphatase levels and Mayo risk score are independently associated with the development of pruritus, but symptom severity is not associated with any clinical features. The underlying pathogenesis of pruritus in PBC remains obscure. Recent hypotheses include the accumulation of serum bile acids and an increased release of endogenous opioids. Talwalkar JA, Lindor KD. Primary biliary cirrhosis. Lancet 2003;362:53-61. Leuschner U. Clin Liv Dis 2003; 7:741

38
Sicca Syndrome Present in up to 70%
Primary Biliary Cirrhosis Sicca Syndrome Present in up to 70% Keratoconjunctivitis and xerostomia are most common symptoms Therapies include increased fluid intake oral sialogogues artificial tears vaginal lubricants Slide 93 Sicca Syndrome The symptoms of keratoconjunctivitis sicca (dry eyes and dry mouth) occur in over 70% of patients with PBC. Secondary involvement of salivary and lacrimal glands with inflammation is thought to be the underlying cause. The majority of patients, however, do not satisfy criteria for the diagnosis of Sjögren’s syndrome. In contrast, patients with classical features of Sjögren’s syndrome and serum AMA positivity often develop PBC at a later date. Treatment is directed at symptomatic improvement using artificial tears and oral sialagogues as first line agents. Topical cyclosporine for keratoconjunctivitis has not been tested in PBC. Oral pilocarpine and cemeviline, which have been used in patients with primary Sjögren's syndrome, have not been extensive tested in PBC. Talwalkar JA, Lindor KD. Primary Biliary Cirrhosis. In Wolfe MM (ed). Therapy of Digestive Diseases, 2005.
 occur in over 70% of patients with PBC. Secondary involvement of salivary and lacrimal glands with inflammation is thought to be the underlying cause. The majority of patients, however, do not satisfy criteria for the diagnosis of Sjögren’s syndrome. In contrast, patients with classical features of Sjögren’s syndrome and serum AMA positivity often develop PBC at a later date. Treatment is directed at symptomatic improvement using artificial tears and oral sialagogues as first line agents. Topical cyclosporine for keratoconjunctivitis has not been tested in PBC. Oral pilocarpine and cemeviline, which have been used in patients with primary Sjögren s syndrome, have not been extensive tested in PBC. Talwalkar JA, Lindor KD. Primary Biliary Cirrhosis. In Wolfe MM (ed). Therapy of Digestive Diseases,")
39
Xanthomata Frequency: 15 - 50% Involve extensor tendon surfaces
Primary Biliary Cirrhosis Xanthomata Frequency: % Involve extensor tendon surfaces Xanthelasma affects eyelids Associated with elevated serum cholesterol levels May resolve with disease progression or with UDCA therapy Slide 94 Xanthomata Xanthomata (subcutaneous cholesterol-based deposits) are found in patients with PBC. Once a common observation in patients with advanced disease, these cutaneous lesions are now observed in < 15% of new diagnoses. Xanthomata primarily involve the extensor tendon surfaces and eyelids (known as xanthelasma). No relationship between serum cholesterol levels and xanthomata is observed. Importantly, the regression or disappearance of xanthomata is observed in association with advancing liver disease or UDCA therapy. Talwalkar JA, Lindor KD. Primary biliary cirrhosis. Lancet 2003;362:53-61. Leuschner U. Primary biliary cirrhosis--presentation and diagnosis. Clin Liver Dis 2003;7: Talwalkar J, et al. Clin Gastro Hepatol 2003
 are found in patients with PBC. Once a common observation in patients with advanced disease, these cutaneous lesions are now observed in < 15% of new diagnoses. Xanthomata primarily involve the extensor tendon surfaces and eyelids (known as xanthelasma). No relationship between serum cholesterol levels and xanthomata is observed. Importantly, the regression or disappearance of xanthomata is observed in association with advancing liver disease or UDCA therapy. Talwalkar JA, Lindor KD. Primary biliary cirrhosis. Lancet 2003;362: Leuschner U. Primary biliary cirrhosis--presentation and diagnosis. Clin Liver Dis 2003;7: Talwalkar J, et al. Clin Gastro Hepatol")
40
Asymptomatic Disease – PBC
Primary Biliary Cirrhosis Asymptomatic Disease Frequency: % Increasingly common Asymptomatic phase may last up to 10 years Liver tests and autoantibody profiles same as for symptomatic patients Slide 96 Asymptomatic Disease – PBC The frequency of detecting PBC in asymptomatic patients has increased over time with rates between 40%-60% reported in recent experience. When compared to symptomatic patients, the patients without symptoms have advanced disease in terms of biochemical and histological criteria. The majority of initially asymptomatic patients developed symptoms of liver disease if they were followed up for long enough (Kaplan-Meier estimate of proportion developing symptoms: 50% after five years, 95% after 20 years). However, 45% of patients remained asymptomatic at the time of death. The median survival of patients with asymptomatic disease who remain symptom-free is greater than among patients with symptomatic disease. However, the median survival of asymptomatic patients is less than age- and sex-matched healthy individuals. Prince MI, Chetwynd A, Craig WL, Metcalf JV, James OF. Asymptomatic primary biliary cirrhosis: clinical features, prognosis, and symptom progression in a large population based cohort. Gut 2004;53: Springer J, Cauch-Dudek K, O'Rourke K, Wanless IR, Heathcote EJ. Asymptomatic primary biliary cirrhosis: a study of its natural history and prognosis. Am J Gastroenterol. 1999;94:47-53.
. However, 45% of patients remained asymptomatic at the time of death. The median survival of patients with asymptomatic disease who remain symptom-free is greater than among patients with symptomatic disease. However, the median survival of asymptomatic patients is less than age- and sex-matched healthy individuals. Prince MI, Chetwynd A, Craig WL, Metcalf JV, James OF. Asymptomatic primary biliary cirrhosis: clinical features, prognosis, and symptom progression in a large population based cohort. Gut 2004;53: Springer J, Cauch-Dudek K, O Rourke K, Wanless IR, Heathcote EJ. Asymptomatic primary biliary cirrhosis: a study of its natural history and prognosis. Am J Gastroenterol. 1999;94:")
41
Potential Mechanisms for the Development of PBC
Microorganism infection Xenobiotics Genetic Apoptosis Slide 98 Potential Mechanisms for the Development of PBC A number of mechanisms have been suggested in association with the development of PBC. The most frequently cited mechanism is exposure to infectious agents such as bacteria and viruses. The use of drugs such as antibiotics may also play a putative role in the development of PBC. While no specific genetic predisposition is known for PBC, this is probably essential for disease expression. Apoptosis is commonly observed in many chronic liver diseases including PBC.

42
Extrahepatic Autoimmune Diseases
Primary Biliary Cirrhosis Extrahepatic Autoimmune Diseases (%) Sicca syndrome 70 Thyroid disease 40 Arthritis 20 Scleroderma 15 Raynaud’s phenomenon 10 CREST syndrome 5 Slide 107 Extrahepatic Autoimmune Diseases The most common extrahepatic autoimmune disease in association with PBC is keratconjunctivitis sicca in up to 70% of patients. Hypothyroidism is seen in up to 40% of patients and often predates the recognition of PBC. Inflammatory arthritis is less well-defined as degenerative joint disease is often observed. Localized or systemic scleroderma is observed in up to 20% of patients. Talwalkar JA, Lindor KD. Zakim/Boyer, 2005
 Sicca syndrome 70. Thyroid disease 40. Arthritis 20. Scleroderma 15. Raynaud’s phenomenon 10. CREST syndrome 5. Slide 107. Extrahepatic Autoimmune Diseases. The most common extrahepatic autoimmune disease in association with PBC is keratconjunctivitis sicca in up to 70% of patients. Hypothyroidism is seen in up to 40% of patients and often predates the recognition of PBC. Inflammatory arthritis is less well-defined as degenerative joint disease is often observed. Localized or systemic scleroderma is observed in up to 20% of patients. Talwalkar JA, Lindor KD. Zakim/Boyer,")
43
Metabolic Bone Disease: Osteopenia, Osteoporosis, and Osteomalacia
Primary Biliary Cirrhosis Metabolic Bone Disease: Osteopenia, Osteoporosis, and Osteomalacia Etiology related to cholestasis Frequency osteopenia: 0% - 50% osteoporosis: 0% - 20% osteomalacia: 0% - 5% Risk factors include age, low body weight, smoking, and advanced histological stage Independent of menopausal status Slide 108 Metabolic Bone Disease: Osteopenia, Osteoporosis, and Osteomalacia Metabolic bone disease in PBC is related to osteopenia rather than osteomalacia (defective bone mineralization). Potential etiologies include defective osteoblast activity in pre-menopausal women, increased osteoclast activity in pre- and post-menopausal women, polymorphisms of vitamin D metabolism which predispose to bone disease, and cigarette smoking which reduces serum vitamin D levels. Approximately one-third of patients with PBC has osteopenia and 11% have osteoporosis defined by a Z score < -2.5 by lumbar spine bone mineral densitometry testing. The increased risk for osteoporosis from PBC remains controversial, however, as other studies observe similar rate of bone loss when compared to age-matched healthy postmenopausal women. Risk factors for metabolic bone disease in PBC include age, body mass index, and stage 3 or 4 histological disease. Talwalkar JA, Lindor KD. Primary biliary cirrhosis. Lancet 2003;362:53-61. Leuschner U. Clin Liv Dis 2003;7:741-58
. Potential etiologies include defective osteoblast activity in pre-menopausal women, increased osteoclast activity in pre- and post-menopausal women, polymorphisms of vitamin D metabolism which predispose to bone disease, and cigarette smoking which reduces serum vitamin D levels. Approximately one-third of patients with PBC has osteopenia and 11% have osteoporosis defined by a Z score < -2.5 by lumbar spine bone mineral densitometry testing. The increased risk for osteoporosis from PBC remains controversial, however, as other studies observe similar rate of bone loss when compared to age-matched healthy postmenopausal women. Risk factors for metabolic bone disease in PBC include age, body mass index, and stage 3 or 4 histological disease. Talwalkar JA, Lindor KD. Primary biliary cirrhosis. Lancet 2003;362: Leuschner U. Clin Liv Dis 2003;7:")
44
Management of Metabolic Bone Disease
Primary Biliary Cirrhosis Management of Metabolic Bone Disease Osteoporosis much more common than osteomalacia Hormone replacement in women Calcium + vitamin D helpful Bisphosphonates may be helpful Steroid therapy may worsen bone disease Calcitonin not helpful Slide 109 Management of Metabolic Bone Disease First-line therapy for metabolic bone disease includes weight-bearing exercise, oral calcium (1000 to 1200 mg daily), sun exposure, and vitamin D replacement (25,000 to 50,000 IU two to three times weekly) when low serum levels are documented. Hormone replacement therapy (HRT) is safe and effective among post-menopausal patients with PBC. If HRT is to be used; a repeat serum liver biochemical evaluation at 2-week intervals for 8 weeks is advised to exclude worsening cholestasis. The use of oral bisphosphonates is associated with improvements in lumbar spine bone mineral density, but no data is available regarding the effect of treatment on reducing incident fractures. Calcitonin is ineffective therapy. Talwalkar JA, Lindor KD. Primary Biliary Cirrhosis. In Wolfe MM (ed). Therapy of Digestive Diseases, 2005.
, sun exposure, and vitamin D replacement (25,000 to 50,000 IU two to three times weekly) when low serum levels are documented. Hormone replacement therapy (HRT) is safe and effective among post-menopausal patients with PBC. If HRT is to be used; a repeat serum liver biochemical evaluation at 2-week intervals for 8 weeks is advised to exclude worsening cholestasis. The use of oral bisphosphonates is associated with improvements in lumbar spine bone mineral density, but no data is available regarding the effect of treatment on reducing incident fractures. Calcitonin is ineffective therapy. Talwalkar JA, Lindor KD. Primary Biliary Cirrhosis. In Wolfe MM (ed). Therapy of Digestive Diseases,")
45
Portal Hypertension – PBC
Primary Biliary Cirrhosis Portal Hypertension Most common in cirrhotics Esophageal varices from presinusoidal causes in some Serum albumin, bilirubin, and platelet count are independent predictors of esophageal varices Clinical outcomes similar to other liver diseases Slide 110 Portal Hypertension – PBC Portal hypertension most often results from the development of cirrhosis in PBC. Complications including variceal bleeding, ascites, and hepatic encephalopathy occur in PBC as with other parenchymal liver diseases. In certain cases, the development of portal hypertension and esophageal varices may occur with presinusoidal fibrosis in the absence of cirrhosis. Leuschner U. Primary biliary cirrhosis--presentation and diagnosis. Clin Liver Dis 2003;7: Leuschner U. Clin Liv Dis 2003; 7:741-58

46
Management of PBC Evaluation Interval Clinical visit 6-12 months
Primary Biliary Cirrhosis Management of PBC Evaluation Interval Clinical visit 6-12 months Serum liver tests 3-6 months Sensitive TSH Yearly Lipid profile Yearly Bone density Diagnosis, 2 years Vitamin levels If total bilirubin elevated Slide 112 Management of PBC The recommended long-term management of PBC includes a clinical visit at least once a year with laboratory assessment of cholestasis and hepatic synthetic function. In patients with advanced liver disease should have serum liver enzyme tests more frequently (at least every 6 months). Bone mineral density testing at diagnosis and after 2 years if therapy is initiated is also recommended. Inpatients with jaundice (total bilirubin > 2 mg/dL), serum fat-soluble vitamin levels should be obtained with oral replacement of deficient states. Talwalkar JA, Lindor KD. Therapy of Dig Dis (in press)
. Bone mineral density testing at diagnosis and after 2 years if therapy is initiated is also recommended. Inpatients with jaundice (total bilirubin > 2 mg/dL), serum fat-soluble vitamin levels should be obtained with oral replacement of deficient states. Talwalkar JA, Lindor KD. Therapy of Dig Dis (in press)")
47
Medical Management Unsuccessful Questionable Useful
Primary Biliary Cirrhosis Medical Management Unsuccessful Questionable Useful penicillamine steroids UDCA cyclosporine colchicine azathioprine methotrexate thalidomide malotilate chlorambucil Slide 113 Medical Management A number of medical therapies to halt disease progression have been tested in PBC. The only medical therapy with proven efficacy to delay progression of disease as well as extend transplant-free survival is UDCA.

48
Actions of Ursodeoxycholic Acid
Primary Biliary Cirrhosis Actions of Ursodeoxycholic Acid Protects against cytotoxic effects of di-hydroxy bile acids Modulates expression of HLA Stabilizes bile canalicular membrane Choleretic effect Decreased apoptosis Decreased cytokine production Slide 114 Actions of Ursodeoxycholic Acid The mechanism of action for UDCA therapy in PBC is multifactorial. In addition to promoting endogenous bile acid secretion, there is evidence to suggest that UDCA is associated with membrane stabilization, reduced aberrant HLA type I expression on hepatocytes, and decreased cytokine production. The inhibition of apoptosis and mitochondrial dysfunction caused by exposure to hydrophobic bile acids are also prevented by UDCA. Lazaridis KN, Gores GJ, Lindor KD. Ursodeoxycholic acid mechanisms of action and clinical use in hepatobiliary disorders. J Hepatol 2001;35:

49
Comparison of Prognostic Models - PBC
Primary Biliary Cirrhosis Comparison of Prognostic Models Yale European Mayo Oslo Glasgow Australia Age Age Age Variceal Age Age bleeding Bilirubin Bilirubin Bilirubin Bilirubin Bilirubin Bilirubin Hepatomegaly Albumin Albumin Ascites Albumin Fibrosis Cirrhosis Prothrombin Variceal time bleeding Cirrhosis Cholestasis Edema Fibrosis Cholestasis Mallory bodies Slide 120 Comparison of Prognostic Models – PBC A number of prognostic mathematical models have been developed to predict the natural history of PBC among individual patients. The model which has been most often validated comes from the Mayo Clinic. In addition, the ability to predict survival without histological information obviates the need for liver biopsy which is not found in other models to date. Wiesner, Mayo Clin Proc 1998; 73(6):575
:575.")
50
Overview Definition Clinical picture Diagnosis Pathology Management
Overview – AIH Autoimmune Hepatitis Overview Definition Clinical picture Diagnosis Pathology Management Complications Transplantation Slide 123 Overview – AIH

51
Autoimmune Hepatitis Autoimmune Hepatitis Autoimmune Hepatitis Intermittently progressive inflammatory liver disease of presumed autoimmune etiology High gamma globulins, autoantibodies Predominately periportal hepatitis Usually responds favorably to corticosteroids Slide 124 Autoimmune Hepatitis Autoimmune hepatitis is an intermittently progressive liver disease characterized by hypergammaglobulinemia, autoantibodies, predominately periportal hepatitis and a usually favorable response to corticosteroid therapy. There is a marked portal inflammatory infiltrate that is not confined to the portal tract; interface activity (“piecemeal necrosis”) is present. Hepatitic rosettes are subtle.
 is present. Hepatitic rosettes are subtle.")
52
Clinical Features Autoimmune Hepatitis Clinical Features Middle-aged (or teenage) woman, non-drinker without viral hepatitis Fatigue, arthralgias/myalgias, oligomenorrhea, jaundice Increased ALT, AST, gamma globulins Positive ANA and SMA Interface hepatitis with lymphoplasmacytic infiltrate Responds to corticosteroids Slide 128 Clinical Features The typical patient with autoimmune hepatitis is a middle-aged or teen-aged woman without environmental risk factors for liver disease who presents with insidious onset of fatigue, arthralgias, myalgias, oligomenorrhea and then often develops jaundice. Laboratory testing reveals evidence of hepatocellular injury, hypergammaglobulinemia and usually the presence of both anti-nuclear and anti-smooth muscle antibodies. Liver histology is marked by the presence of interface hepatitis and a lymphoplasmacytic infiltrate and, when corticosteroid therapy is started, a gratifying, steady resolution of biochemical and histological abnormalities ensues.

53
Auto-Antibodies in AIH
Autoimmune Hepatitis Auto-Antibodies in AIH Antibody Target Antigens Prevalence Other Disease ANA Multiple nuclear % PBC, PSC, HCV, proteins NAFLD SMA Actin % HCV, NAFLD, Acute viral hepatitis pANCA Lactoferrin, Other % PSC, PBC unknown Ag LKM-1 CYP 2D6 ≈ 4% HCV SLA/LP UGA repressor % HCV tRNA-associated protein Slide 132 Auto-Antibodies in AIH 60-80% of patients with autoimmune hepatitis have autoantibodies directed against multiple nuclear proteins (ANA) and/or against actin (SMA). Such patients often also have perinuclear anti-neutrophil cytoplasmic (pANCA) antibodies and may have autoantibodies directed against the soluble liver antigen (SLA) UGA repressor tRNA-associated protein. A small subset of patients with autoimmune hepatitis only have autoantibodies directed against the liver kidney microsomal type 1 (LKM-1) antigen CYP 2D6. It is important to recognize that some patients with autoimmune hepatitis lack conventional ANA, SMA or LKM-1 autoantibodies. Supplemental testing for pANCA and SLA and/or use of more extensive AIH scoring criteria may be helpful in supporting a diagnosis of autoimmune hepatitis in such cases. Unfortunately, none of the autoantibody markers of autoimmune hepatitis are specific for this disease. Each of these autoantibodies has been found to be present in patients with other forms of liver disease.
 and/or against actin (SMA). Such patients often also have perinuclear anti-neutrophil cytoplasmic (pANCA) antibodies and may have autoantibodies directed against the soluble liver antigen (SLA) UGA repressor tRNA-associated protein. A small subset of patients with autoimmune hepatitis only have autoantibodies directed against the liver kidney microsomal type 1 (LKM-1) antigen CYP 2D6. It is important to recognize that some patients with autoimmune hepatitis lack conventional ANA, SMA or LKM-1 autoantibodies. Supplemental testing for pANCA and SLA and/or use of more extensive AIH scoring criteria may be helpful in supporting a diagnosis of autoimmune hepatitis in such cases. Unfortunately, none of the autoantibody markers of autoimmune hepatitis are specific for this disease. Each of these autoantibodies has been found to be present in patients with other forms of liver disease.")
54
Sub-Types of Autoimmune Hepatitis
Type 1 Type 2 Age at Presentation Any age Predominantly children Female:Male 4:1 8:1 Ig G Levels Elevated IgG Variable Ig G Ig A Levels Normal +/- Low IgA Auto-antibodies ANA, SMA LKM-1 Cirrhosis at 3 yrs ~ 40% ~ 80% Slide 133 Sub-Types of Autoimmune Hepatitis Sub-types of autoimmune hepatitis have been proposed based on differences in autoantibody markers and clinical features. The most common form is type 1 autoimmune hepatitis characterized by the presence of ANA and SMA. Less common is the type 2 form characterized by the presence of LKM-1 autoantibodies but absence of ANA, SMA or pANCA. This disease presents predominately in children, may be associated with low IgA levels with or without elevations of IgG and more commonly progressed to cirrhosis early in the course of the disease. A type 3 AIH characterized by the presence of SLA autoantibodies in the absence of ANA, SMA or LKM-1 autoantibodies has been proposed, but this syndrome appears indistinguishable from Type 1 AIH in all other clinical and laboratory features.

55
Portal Tract Inflammation Histology
Plasma cell cluster; occasional eosinophils Plasma cells Slide 134 Portal Tract Inflammation Histology Portal tract inflammation is mixed with mononuclear cells, occasional eosinophils, and an over-representation of plasma cells, often in clusters (blue arrow). The interface hepatitis of AIH is typically markedly active and includes numerous plasma cells (white arrows).
. The interface hepatitis of AIH is typically markedly active and includes numerous plasma cells (white arrows).")
56
Plasma cells in foci of spotty necrosis
Slide 135 Spotty Necrosis Clusters of plasma cells in the lobules, usually associated with “spotty necrosis” as shown in this photomicrograph, are characteristic of AIH.

57
Plasma Cell Interface Activity and Hepatitic Rosettes
Slide 136 Plasma Cell Interface Activity and Hepatitic Rosettes This photomicrograph of a biopsy showing AIH illustrates two often-discussed features of AIH: plasma cell interface activity (yellow arrow) and hepatitic rosettes. The latter are clusters of reactive appearing hepatocytes encircled by inflammatory cells. The presence of abundant rosettes, such as in this case, lend an appearance of “cobblestoning” to the hepatic parenchyma. One rosette is demarcated by yellow lines.
 and hepatitic rosettes. The latter are clusters of reactive appearing hepatocytes encircled by inflammatory cells. The presence of abundant rosettes, such as in this case, lend an appearance of cobblestoning to the hepatic parenchyma. One rosette is demarcated by yellow lines.")
58
Recognition and Diagnosis of AIH
Autoimmune Hepatitis Recognition and Diagnosis of AIH Should be considered in patient with elevated AST/ALT or cirrhosis of uncertain etiology ANA, SMA and other autoantibody tests are poor “screening tests” The diagnosis of AIH must be based on a constellation of findings A diagnosis of AIH is often a “work in progress” Slide 146 Recognition and Diagnosis of AIH The diagnosis of AIH should be considered in patients with hepatitis or cirrhosis of uncertain etiology. Because of their lack of specificity, ANA, SMA and LKM-1 autoantibody tests should not be used as “screening tests, but rather as markers supportive of the diagnosis of autoimmune liver disease in patients with the constellation of findings that define this disease. Because there are no pathognomonic markers for AIH, this diagnosis is often a “work in progress” in which the clinician must repeatedly reconsider factors that favor or argue against AIH as diagnostic evaluations and therapy progresses.

60
International Autoimmune Hepatitis Group Scoring System: Patient History
Favor AIH Favor other diagnosis (points) (points) Gender Female (+2) Male (0) Alcohol < 25 g/d (+2) > 60 g/d (–2) Hepatotoxic drugs None (+1) Present (-4) Other autoimmune Present (+2) None (0) diseases Slide 149 International Autoimmune Hepatitis Group Scoring System: Patient History The international autoimmune hepatitis group scoring system assigns positive points for historical features typical of AIH such as female gender, minimal levels of alcohol consumption, absence of hepatotoxic drug exposure and the presence of extrahepatic autoimmune disorders. Negative points are assigned for presence of excess alcohol consumption or for exposure to know hepatotoxins.
 (points) Gender Female (+2) Male (0) Alcohol < 25 g/d (+2) > 60 g/d (–2) Hepatotoxic drugs None (+1) Present (-4) Other autoimmune Present (+2) None (0) diseases. Slide 149. International Autoimmune Hepatitis Group Scoring System: Patient History. The international autoimmune hepatitis group scoring system assigns positive points for historical features typical of AIH such as female gender, minimal levels of alcohol consumption, absence of hepatotoxic drug exposure and the presence of extrahepatic autoimmune disorders. Negative points are assigned for presence of excess alcohol consumption or for exposure to know hepatotoxins.")
61
International Autoimmune Hepatitis Group Scoring System: Biochemistries
Favor AIH Favor other diagnosis (points) (points) Alkaline phosphatase < 1.5 (+2) > 3.0 (-2) elevation: ALT elevation Serum globulins, > 2 x normal (+3) Normal (0) g globulin or IgG >1.5-2 x normal (+2) > x normal (+1) Slide 150 International Autoimmune Hepatitis Group Scoring System: Biochemistries The international autoimmune hepatitis group scoring system assigns positive points for typical biochemical features of AIH including a ratio of alkaline phosphatase (or GGT in children) elevation to ALT elevation that is < 1.5 and elevation of total serum globulins, gamma globulins or IgG. In the revised scoring system, negative points are assigned if the ratio of alkaline phosphatase (or GGT in children) elevation to ALT elevation is > 3.0.
 (points) Alkaline phosphatase < 1.5 (+2) > 3.0 (-2) elevation: ALT elevation. Serum globulins, > 2 x normal (+3) Normal (0) g globulin or IgG >1.5-2 x normal (+2) > x normal (+1) Slide 150. International Autoimmune Hepatitis Group Scoring System: Biochemistries. The international autoimmune hepatitis group scoring system assigns positive points for typical biochemical features of AIH including a ratio of alkaline phosphatase (or GGT in children) elevation to ALT elevation that is < 1.5 and elevation of total serum globulins, gamma globulins or IgG. In the revised scoring system, negative points are assigned if the ratio of alkaline phosphatase (or GGT in children) elevation to ALT elevation is > 3.0.")
62
International Autoimmune Hepatitis Group Scoring System: Serologies
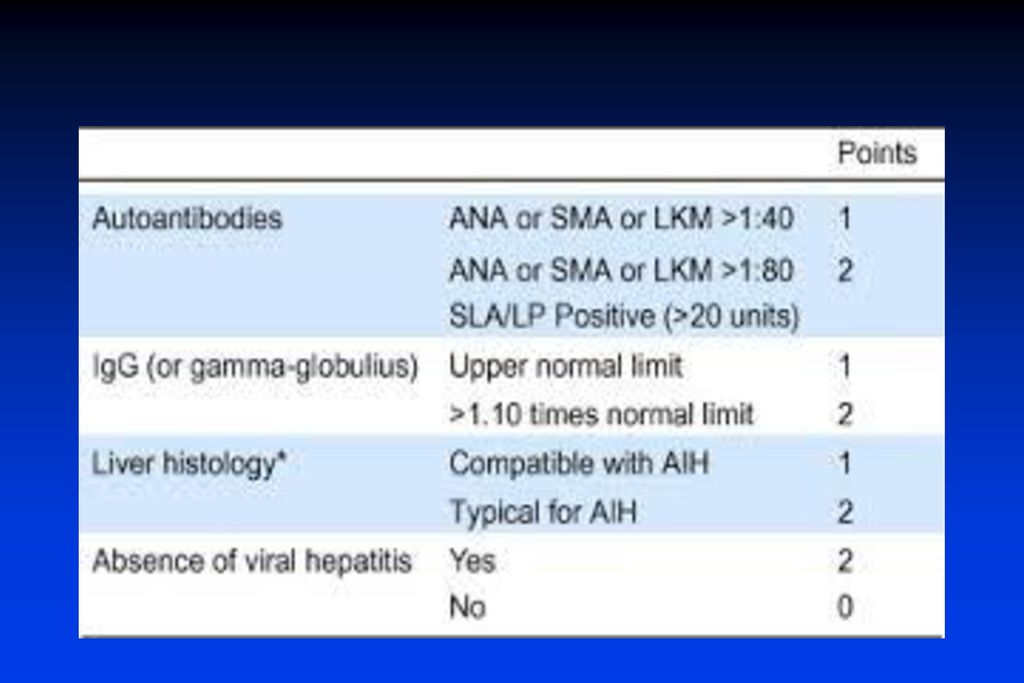
Favor AIH Favor other diagnosis (points) (points) ANA, SMA or LKM-1 > 1:80 (+3) < 1:40 (0) 1:80 (+2) 1:40 (+1) AMA Negative (0) Positive (-4) Hepatitis Markers Negative (+3) Positive (-3) Other autoantibodies Present (+2) Absent (0) HLA-DR3 or DR4 Present (+1) Absent (0) Slide 151 International Autoimmune Hepatitis Group Scoring System: Serologies The international autoimmune hepatitis group scoring system assigns positive points for typical serologic features of AIH such as the presence of conventional ANA, SMA or LKM-1 autoantibodies, the absence of hepatitis markers, the presence of other autoantibodies associated with AIH such as pANCA or SLA and the presence of HLA-DR3 or DR4. Negative points are assigned for the presence of AMA or markers of chronic viral hepatitis infection.
 (points) ANA, SMA or LKM-1 > 1:80 (+3) < 1:40 (0) 1:80 (+2) 1:40 (+1) AMA Negative (0) Positive (-4) Hepatitis Markers Negative (+3) Positive (-3) Other autoantibodies Present (+2) Absent (0) HLA-DR3 or DR4 Present (+1) Absent (0) Slide 151. International Autoimmune Hepatitis Group Scoring System: Serologies. The international autoimmune hepatitis group scoring system assigns positive points for typical serologic features of AIH such as the presence of conventional ANA, SMA or LKM-1 autoantibodies, the absence of hepatitis markers, the presence of other autoantibodies associated with AIH such as pANCA or SLA and the presence of HLA-DR3 or DR4. Negative points are assigned for the presence of AMA or markers of chronic viral hepatitis infection.")
63
International Autoimmune Hepatitis Group Scoring System: Histology
Favor AIH Favor other diagnosis (points) (points) Interface Hepatitis +3 Lymphoplasmacytic +1 Infiltrate Rosetting of liver cells +1 None of Above -5 Biliary Changes -3 Other changes -3 Slide 152 International Autoimmune Hepatitis Group Scoring System: Histology An essential component in the evaluation of patients for AIH is assessment of liver histology. The international autoimmune hepatitis group scoring system assigns positive points for typical histological features such as interface hepatitis, lymphoplasmacytic infiltrates and rosetting of liver cells. However, negative points are assigned for the absence of all of these AIH features or for the presence of biliary lesions or other changes such as granulomas or significant steatosis that are more typical of other types of inflammatory liver diseases.
 (points) Interface Hepatitis +3. Lymphoplasmacytic +1. Infiltrate. Rosetting of liver cells +1. None of Above -5. Biliary Changes -3. Other changes -3. Slide 152. International Autoimmune Hepatitis Group Scoring System: Histology. An essential component in the evaluation of patients for AIH is assessment of liver histology. The international autoimmune hepatitis group scoring system assigns positive points for typical histological features such as interface hepatitis, lymphoplasmacytic infiltrates and rosetting of liver cells. However, negative points are assigned for the absence of all of these AIH features or for the presence of biliary lesions or other changes such as granulomas or significant steatosis that are more typical of other types of inflammatory liver diseases.")
64
International Autoimmune Hepatitis Group Scoring System: Response to Therapy
Favor AIH (points) Complete Remission (normal ALT, IgG, +2 bilirubin within 12 mo and for >6 month duration or: all tests > 50% improved in 1 mo. and AST/ALT < 2x normal within 6 mos. or: liver biopsy with minimal activity) Remission with relapse (return of +3 symptoms, abnormal biopsy and /or > 2 x normal AST/ALT) Slide 153 International Autoimmune Hepatitis Group Scoring System: Response to Therapy Following institution of corticosteroid therapy, the international autoimmune hepatitis group scoring system assigns additional positive points for two typical features of this disease: a complete remission on therapy and a remission followed by relapse after discontinuation of therapy.
 Complete Remission (normal ALT, IgG, +2. bilirubin within 12 mo and for >6 month. duration or: all tests > 50% improved in. 1 mo. and AST/ALT < 2x normal within 6 mos. or: liver biopsy with minimal activity) Remission with relapse (return of +3. symptoms, abnormal biopsy and /or. > 2 x normal AST/ALT) Slide 153. International Autoimmune Hepatitis Group Scoring System: Response to Therapy. Following institution of corticosteroid therapy, the international autoimmune hepatitis group scoring system assigns additional positive points for two typical features of this disease: a complete remission on therapy and a remission followed by relapse after discontinuation of therapy.")
65
Interpretation of International Autoimmune Hepatitis Group Score
Autoimmune Hepatitis - Criteria Interpretation of International Autoimmune Hepatitis Group Score Score Interpretation Pre-therapy: >15 Definite AIH 10-15 Probable AIH Post-therapy: >17 Definite AIH 12-17 Probable AIH Slide 154 Interpretation of International Autoimmune Hepatitis Group Score Following complete historical, laboratory and histological evaluation, a score of > 15 indicates definite AIH whereas a score of indicates probable AIH. After responses to therapy are considered, a score of > 17 indicates definite AIH and a score of suggests probable AIH.

66
Indications for Treatment Based on the results of
Autoimmune Hepatitis Indications for Treatment Absolute Relative None AST 10x normal Symptoms No symptoms AST 5x normal AST < 5x normal Inactive and -globulin -globulin cirrhosis 2x normal < 2x normal Bridging necrosis Interface Portal hepatitis hepatitis Slide 155 Indications for Treatment Based on the results of randomized controlled trials of therapy in symptomatic patients and the assessment of the natural history of disease in AIH patients with different degrees of biochemical and/or histological abnormalities, there is a general consensus that symptomatic AIH patients with AST ≥ 10-fold elevated, AST ≥ 5-fold elevated and gamma globulins ≥ 2 fold elevated or bridging necrosis on liver biopsy should be treated whereas asymptomatic patients with only inactive cirrhosis or portal hepatitis (i.e. no interface hepatitis) on liver biopsy should not. In patients with intermediate indications for therapy, clinical judgment must be used in making therapeutic decisions. AASLD Practice Guidelines, Hepatology 2002, 36:479
 on liver biopsy should not. In patients with intermediate indications for therapy, clinical judgment must be used in making therapeutic decisions. AASLD Practice Guidelines, Hepatology 2002, 36:479.")
67
Therapy in Adults Combination Therapy Monotherapy
Autoimmune Hepatitis Therapy in Adults Combination Therapy Monotherapy Interval Prednisone Prednisone Azathrioprine mg/d mg/d mg/d Week Week Week Week Daily until endpoint Slide 158 Therapy in Adults The second standard regimen for initial therapy of AIH is a combination regimen using 50% of the dose of prednisone used in the monotherapy regiment in combination with 50 mg/d of azathioprine. AASLD Practice Guidelines, Hepatology 2002, 36:479

68
Reasons for Selecting Treatment Regimens
Autoimmune Hepatitis Reasons for Selecting Treatment Regimens Prednisone Monotherapy Severe cytopenia TPMT deficiency Prior Aza intolerance Pregnancy Malignancy Combination (Pred+Aza) Postmenopausal state Osteoporosis Brittle diabetes Obesity Acne Emotional lability Hypertension Slide 159 Reasons for Selecting Treatment Regimens Long term follow-up of patients receiving prednisone monotherapy versus prednisone and azathioprine combination therapy indicates that the two regimens achieve similar efficacy but are associated with different side effect profiles. Corticosteroid side effects are especially common in patients with AIH and for most patients and especially for patients already at risk for osteoporosis, diabetes, obesity and/or hypertension, the combination regimen is to be preferred because of the steroid sparing benefits of azathioprine. However, in patients with severe cytopenias, known thiopurine methyl transferase deficiency or azathioprine intolerance or with concerns about the teratogenic or oncogenic potential of azathioprine, prednisone monotherapy may be preferred. AASLD Practice Guidelines, Hepatology 2002, 36:479
 Postmenopausal state. Osteoporosis. Brittle diabetes. Obesity. Acne. Emotional lability. Hypertension. Slide 159. Reasons for Selecting Treatment Regimens. Long term follow-up of patients receiving prednisone monotherapy versus prednisone and azathioprine combination therapy indicates that the two regimens achieve similar efficacy but are associated with different side effect profiles. Corticosteroid side effects are especially common in patients with AIH and for most patients and especially for patients already at risk for osteoporosis, diabetes, obesity and/or hypertension, the combination regimen is to be preferred because of the steroid sparing benefits of azathioprine. However, in patients with severe cytopenias, known thiopurine methyl transferase deficiency or azathioprine intolerance or with concerns about the teratogenic or oncogenic potential of azathioprine, prednisone monotherapy may be preferred. AASLD Practice Guidelines, Hepatology 2002, 36:479.")
69
Liver Transplantation
Autoimmune Hepatitis Liver Transplantation Overall 5-year survival rates 80-90% Increased frequency of acute allograft rejection AIH recurrence in 30-40% Surveillance liver biopsies may be warranted Manage with corticosteroids Slide 166 Liver Transplantation Liver transplantation is effective for AIH patients who either fail to respond to therapy or deteriorate due to complications of cirrhosis that developed before or during initial therapy. There is a modestly increased incidence of acute allograft rejection and a 30-40% disease recurrence rate in these patients but if anticipated and treated appropriately these complications usually respond well to immunosuppressive therapy.

Similar presentations



 in 2000, at the age of 67, based on: diagnosis of primary biliary.>")
>")
 that progresses to cirrhosis Replacement of liver tissue.>")













