Download presentation
Presentation is loading. Please wait.

2
Diabetic Neuropathy

3
Diabetic neuropathy is the most common type of neuropathy.
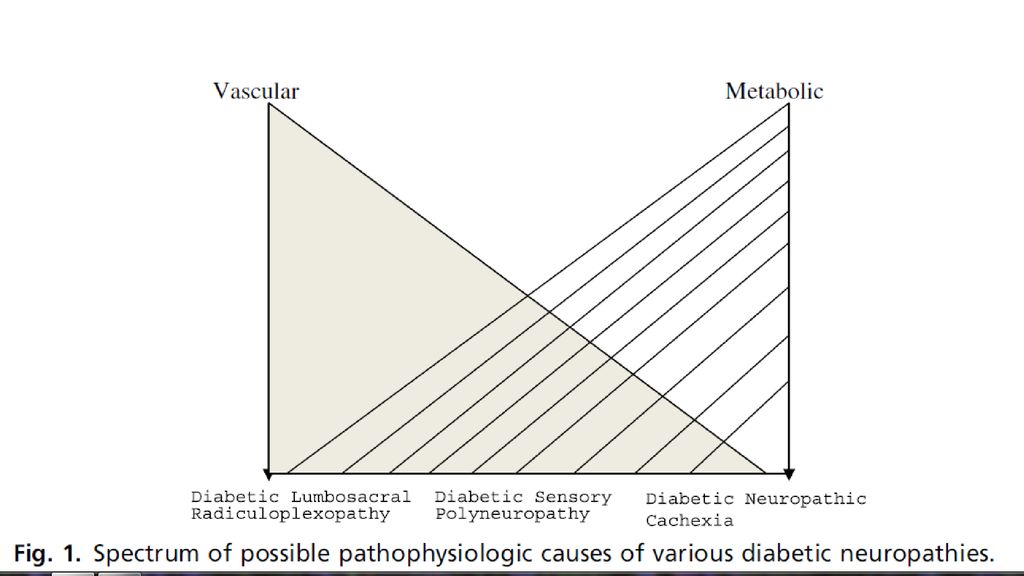
Various types of neuropathies are associated with diabetes mellitus. Metabolic, vascular, inflammatory, and immune theories have been suggested for pathogenesis. Axonal and demyelination can be seen on electrophysiology and pathology. Treatment is mainly aimed at glycemic control and neuropathic pain management.

4
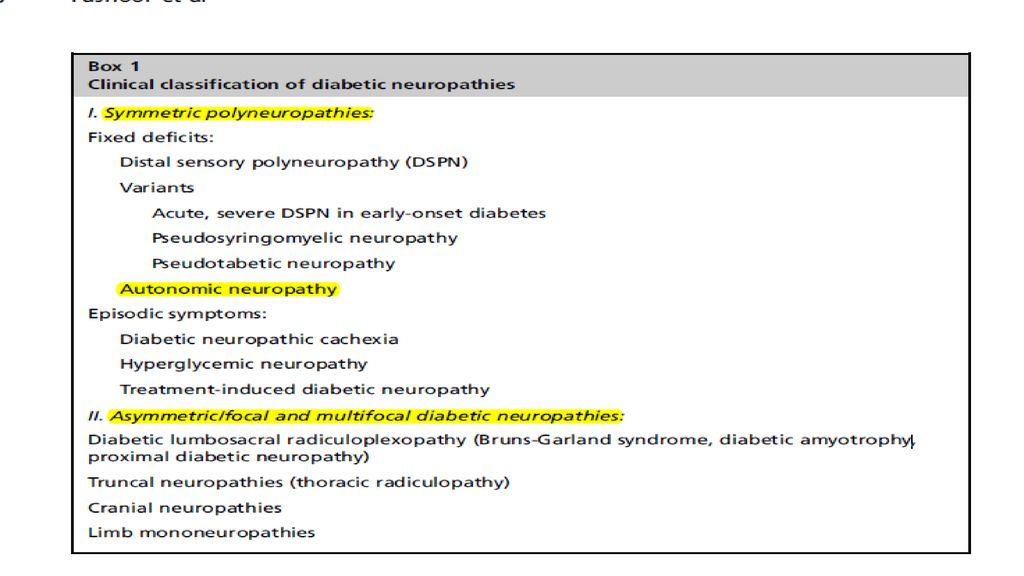
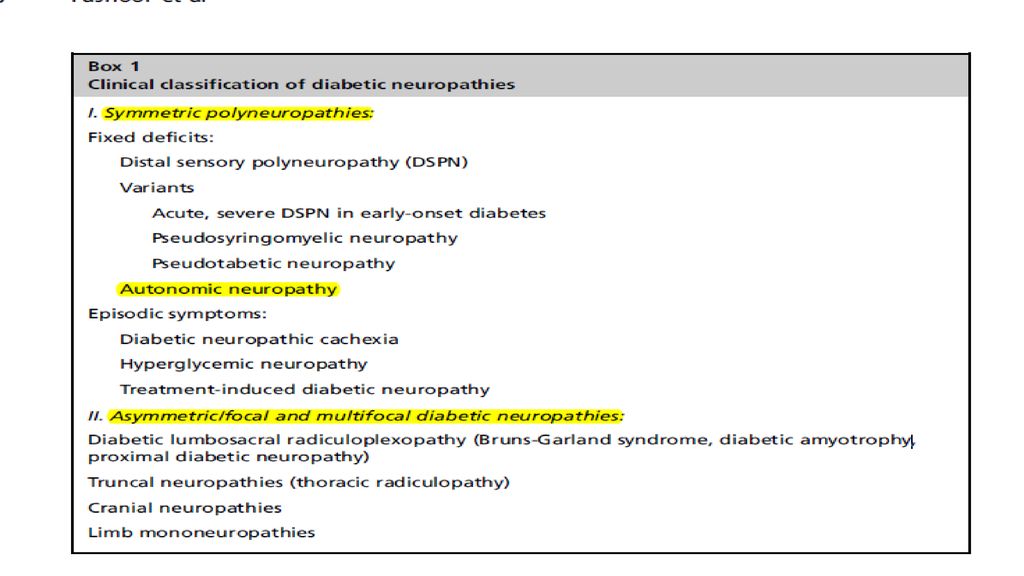
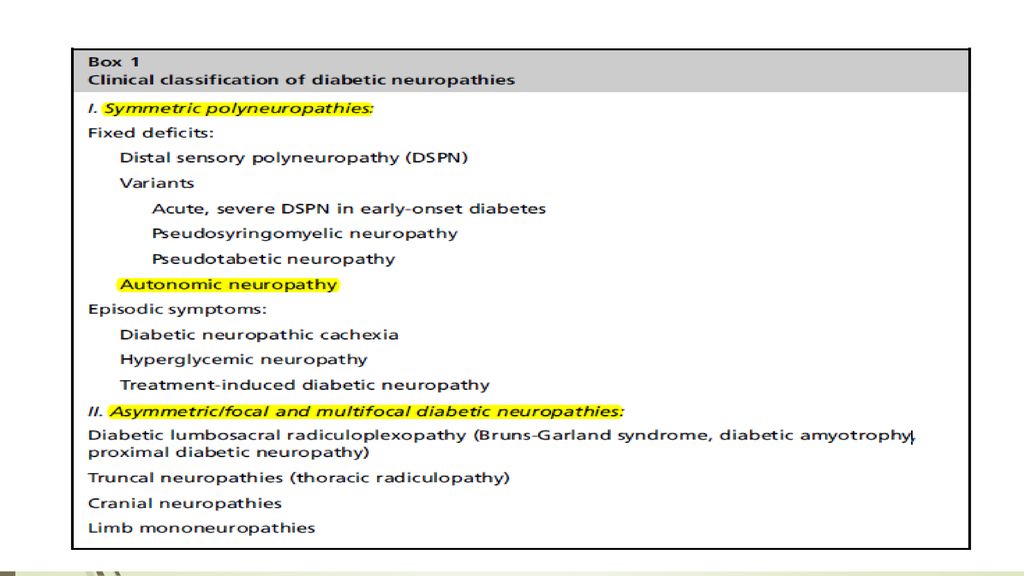
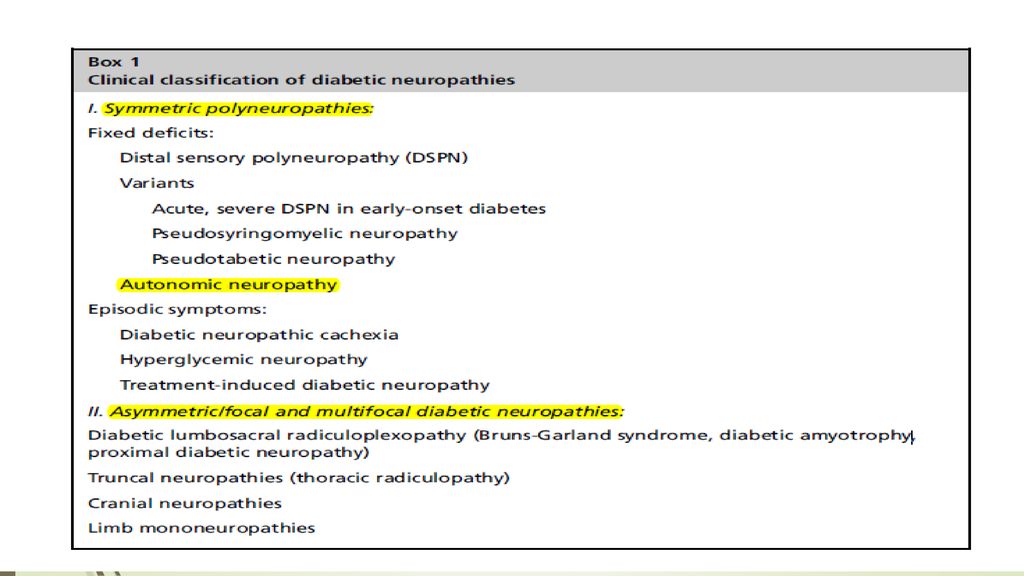
Diabetes mellitus (DM) has 4 major complications: neuropathy, retinopathy, nephropathy, and vasculopathy. The various neuropathies associated with DM can clinically be divided into symmetric and asymmetric (focal and multifocal) forms In addition, clinicians need to be aware of diabetic muscle infarction, a muscle disorder that can occur in diabetic patients.
 forms. In addition, clinicians need to be aware of diabetic muscle infarction, a muscle disorder that can occur in diabetic patients.")
5
EPIDEMIOLOGY The estimated prevalence of DM in the United States in individuals 40 to 74 years old is 12% if only fasting blood sugar (FBS) criteria are used, but 14% if both FBS and glucose tolerance testing (GTT) criteria are used. It is estimated that about half the adults with diabetes in the United States are undiagnosed If the population considered, including children, DM has been reported to occur in 1% to 4%.
 criteria are used, but 14% if both FBS and glucose tolerance testing (GTT) criteria are used. It is estimated that about half the adults with diabetes in the United States are undiagnosed. If the population considered, including children, DM has been reported to occur in 1% to 4%.")
6
Approximately two-thirds of patients with insulin-dependent DM (IDDM) and non- IDDM (NIDDM) had subclinical or clinical evidence of a peripheral neuropathy Roughly half of the diabetics had a symmetric polyneuropathy a quarter had carpal tunnel syndrome about 5% had autonomic neuropathy and 1% had asymmetric proximal neuropathy. The occurrence of neuropathy correlates with the duration of DM, poor glycemic control, and with the presence of retinopathy and nephropathy

7
In the study by Picart, 7.5% of patients had neuropathy at the time of diagnosis, and, after 20 years of DM, 50% had neuropathy. Partanen and colleagues showed that after 10 years of follow- up the percentage of diabetics with neuropathy increased from 8% at baseline to 42%.

8
Pathogenesis of Diabetic Neuropathy

10
Metabolic pathogenesis
Experimental models of acute, severe hyperglycemia can produce reduction in nerve conduction velocity and axonal shrinkage. Glucose and myoinositol share a structural similarity and hyperglycemia may reduce myoinositol uptake in diabetic nerves.

11
This reduction secondarily impairs the function of membrane-bound sodium/potassium ATPase, which can cause axoglial changes and alterations of conduction velocity. However, in nerves from diabetic patients, endoneurial myoinositol was not decreased in 2 clinical trials, there was no benefit to patients from myoinositol supplementation.

12
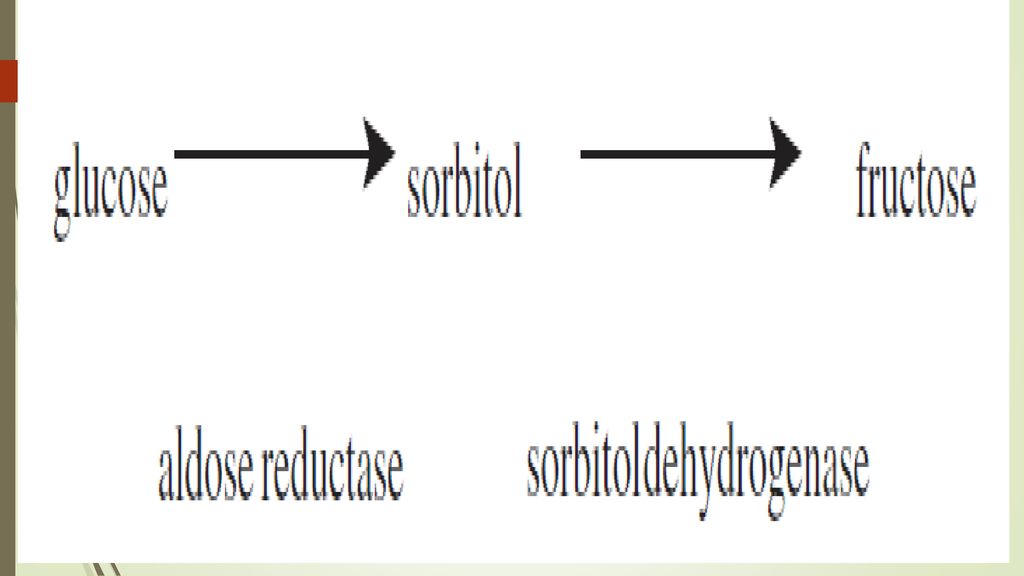
Another popular mechanism is an alteration of polyol metabolism
Another popular mechanism is an alteration of polyol metabolism. Persistent hyperglycemia activates the enzyme aldose reductase, thereby converting glucose to the polyol, sorbitol, and ultimately to fructose. Sorbitol, a compound with a degree of impermeability, accumulates in the nerve creating a hypertonic condition and subsequent water accumulation

14
The accumulation of sorbitol and fructose increases the distance between capillaries, producing endoneurial hypoxia and oxidative stress. Aldose reductase inhibitors in animal models decrease sorbitol concentration in the sciatic nerve and restore conduction velocities to normal.

15
In addition, protection from sorbitol increase in experimental diabetes using aldose reductase inhibitors prevents the loss of myoinositol from the nerve, which may connect 2 possible pathogenic mechanisms.

16
Alterations of fatty acid metabolism can result from chronic hyperglycemia.
In experimental diabetes there is a deficiency of gamma-linolenic acid that could lead to abnormalities in endoneurial blood flow through secondary deficiencies in arachidonic acid and prostaglandins. This finding has led to clinical trials of diets enriched in linolenic acid.

17
Chronic hyperglycemia increases glycosylation of proteins.
Glycation products can accumulate in tissues, producing microvascular disease by direct deposition on endothelial cell membranes or the generation of reactive oxygen species, which adds to oxidative stress. Aminoguanidine, an inhibitor of advanced glycation, has been used in experimental animal models of diabetes and is currently being studied in humans.

18
Vascular pathogenesis

19
It has been postulated that hypoxia or ischemia is involved in diabetic polyneuropathy.
The ultrastructural studies of Dyck and colleagues have shown that the increase in basement membrane area and endothelial cell degeneration is associated with severity of polyneuropathy

20
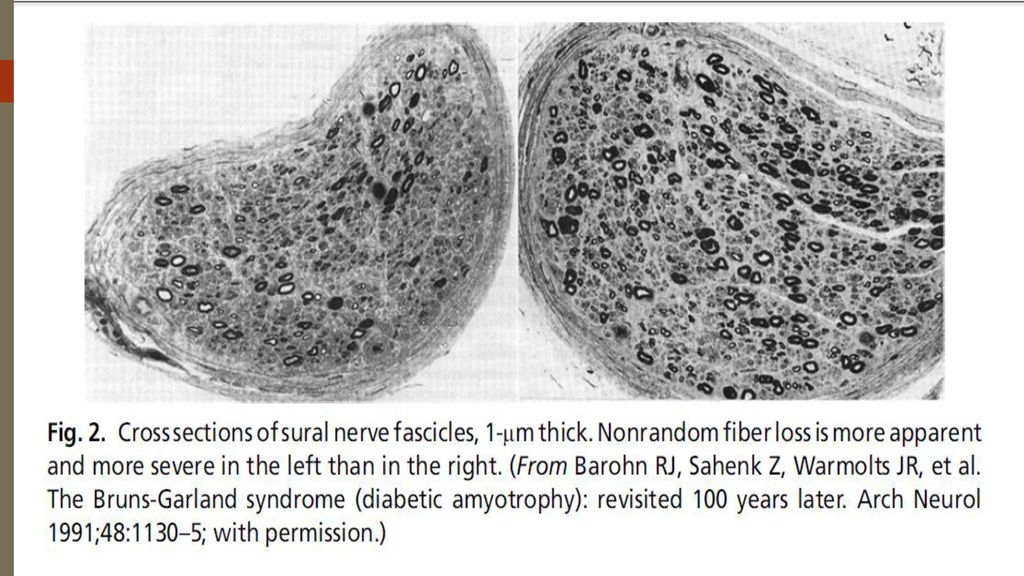
On a more macroscopic level, the study of the distribution of fiber loss in diabetic nerves also suggests a vascular disorder..

21
Johnson and colleagues20 identified changes in the perineurium and surrounding epineurium that resembled those seen in peripheral nerve vasculitis.

22
Autopsy material from patients with diabetic cranial third nerve palsy reveals central fascicular injury suggesting ischemia. An autopsy study in diabetic asymmetric proximal lower extremity neuropathy by Raff and colleagues showed ischemic infarcts of the proximal major nerve trunks of the leg and lumbosacral plexus with multiple areas of decreased myelinated fiber density at these levels

23
In the Mayo Clinic series of Pascoe and colleagues in 6 biopsied patients with diabetic proximal neuropathy, a multifocal distribution of fiber loss was noted in 3 sural nerve specimens. In a recent Mayo Clinic series, changes suggesting ischemia were found in the most of 33 nerve biopsies with diabetic radiculoplexus neuropathy

24
Immunologic/inflammatory pathogenesis

25
An immune-mediated pathogenesis has recently been advocated in some cases of diabetic neuropathy.
In a study of proximal asymmetric neuropathy that showed asymmetric nerve fiber loss, an additional feature was lymphocytic epineurial inflammation resembling vasculitis.

26
Krendel and colleagues found similar perivascular inflammation in 7 of 10 patients with asymmetric lumbosacral neuropathy. In a Mayo Clinic study of diabetic proximal neuropathy, 2 out of 6 sural nerve biopsies showed perivascular mononuclear inflammatory infiltrates.

27
Pathology and Pathophysiology

28
Axonal degeneration or segmental demyelination
There has been some debate regarding whether the primary lesion in diabetic neuropathy is the axon or Schwann cell/myelin. Ballin and Thomas identified onion bulbs and teased nerve fiber, suggesting recurrent demyelination and Vital reported both segmental demyelination and axonal degeneration

29
of the sural nerves of patients with prominent small-fiber sensory loss found pathologic evidence for axonal degeneration, as well as both primary and secondary segmental demyelination.

30
The electrophysiologic studies can similarly show evidence of axonal degeneration and demyelination.
An early and characteristic feature of diabetic neuropathy is prolonged distal latencies and F waves, slow conduction velocity, and reduced amplitude of potentials.

31
Electrophysiologic changes of demyelination in a diabetic patient with a symmetric distal or an asymmetric proximal neuropathy may not necessarily imply an immune-mediated neuropathy that will respond to immunosuppressive therapy.

32
TYPES OF DIABETIC NEUROPATHIES
Symmetric Neuropathies

34
Symmetric neuropathies with fixed deficits

35
DSPN is the most common form of diabetic neuropathy
DSPN is the most common form of diabetic neuropathy. This is primarily a length- dependent sensory neuropathy, and significant distal weakness is uncommon.

36
However, because diabetic patients are often monitored closely before they develop symptoms of neuropathy, the earliest signs of neuropathy may be decreased distal vibration, touch, and pin sensation and ankle reflex loss on examination. The first symptoms are usually decreased feeling or tingling in the toes.

37
Although there may be atrophy and weakness of the toe extensor and flexor muscles, significant distal ankle weakness is uncommon. If profound distal upper and lower extremity weakness is present in a diabetic patient, an evaluation for other causes of neuropathy is warranted

38
Progression of DSPN is usually slow.
In the Rochester Diabetic Neuropathy Study, none of the 380 diabetic patients had polyneuropathy that was disabling even when followed for many years. An exception to this rule is the unusual cases of severe sensory and autonomic neuropathy that can occur in the first several after the onset of type 1 diabetes. It is not known why some patients develop this unusually severe form of neuropathy in the early stages of the disease and there is no relationship between the neuropathy and hyperglycemia or the initiation of insulin therapy.

39
Depending on the clinical context, it may be appropriate to perform screening blood tests for other causes of neuropathy (complete blood count, chem 20, vitamin B12 level, Venereal Disease Research Laboratory test, serum immunofixation). Skin biopsies have become a tool to diagnose small-fiber neuropathy in patients with normal electrodiagnostic testing.

40
There is a selective loss of pain fibers resulting in impaired cutaneous and deep pain and temperature sensation. Severe proprioceptive loss is uncommon, but occasionally this can occur when there is prominent large-fiber involvement. These patients develop sensory ataxia and autonomic manifestations with impotence, bladder atony, and pupillary changes and thus have been called the pseudotabetic form of diabetic neuropathy

41
However, severe proprioception deficits and ataxia are uncommon in diabetes, and when present should lead to a search for other potential causes (syphilis, vitamin B12 deficiency, paraneoplastic or Sjogren syndrome sensory neuronopathy, CIDP)
")
42
However, we think that the pseudosyringomyelic, pseudotabetic, and the early-onset neuropathy described by Said and colleagues are all severe variants of diabetic DSPN and probably not distinct forms of neuropathy.

43
Treatment of DSPN Glucose control In general, patients with strict control of blood glucose have fewer diabetic neuropathy complications. Several studies have shown that tight glucose control with aggressive insulin therapy can reduce the risk for development of neuropathy.

44
The DCCT trial convincingly showed that intensive insulin therapy with an insulin pump or 3 or more daily injections is more effective than conventional therapy in reducing neuropathy. Neuropathy occurred in only 5% of intensively treated patients compared with 13% of those conventionally treated.

45
Other experimental approaches
Many different approaches to treat diabetic neuropathy and the other complications of diabetes have been attempted, but in general there has been little success.

46
In streptozotocin-induced diabetic rats, treatment with alpha-lipoic acid improved nerve blood flow and improved conduction velocity. Alpha-lipoic acid (also known as thioctic acid) may act as an antioxidant free-radical scavenger, and it may inhibit nonenzymatic glycation.
 may act as an antioxidant free-radical scavenger, and it may inhibit nonenzymatic glycation.")
47
A placebo-controlled trial using intravenous alpha-lipoic acid reduced neuropathic symptoms in diabetic patients. In a 5-week randomized controlled trial of oral alpha-lipoic acid 600, 1200, or 1800 mg daily, there was a 50% pain reduction as measured by the Total Symptom Score, including stabbing and burning pain, across all doses, which was statistically significant compared with the placebo response (32%, P<.05).
.")
48
A more recent study suggested that 4-year treatment with oral alpha-lipoic acid 600 mg once daily in mild to moderate distal symmetric neuropathy did not influence the primary composite end point of Neuropathy Impairment Score of the Lower Limbs and 7 neurophysiologic tests.

49
There has recently been interest in nerve growth factor (NGF) therapy as a treatment of diabetic neuropathy. In experimental animal models of diabetes, there is some evidence for decreased NGF expression in various target tissues, and NGF treatment in these models prevented the manifestations of neuropathyIn humans with diabetic neuropathy, NGF levels are reduced in skin biopsy specimens.

50
In a phase II placebo-controlled trial of subcutaneous NGF in 250 patients with diabetic neuropathy, the only end point that reached statistical significance was the patient’s overall global symptom assessment that they felt improved. However, in the larger phase III trial, there was no benefit in the NGF group on any end point

51
Symptomatic treatment

52
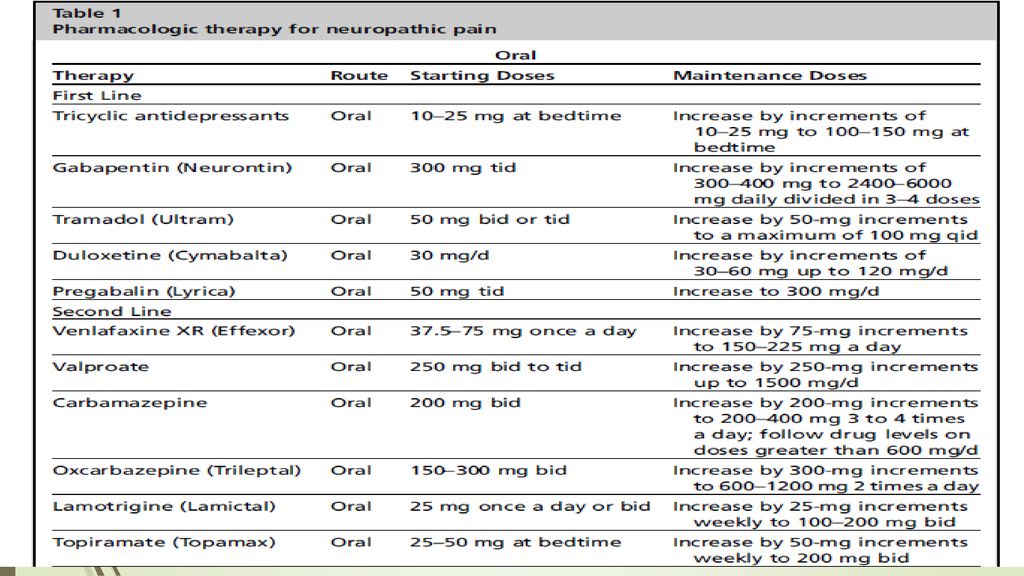
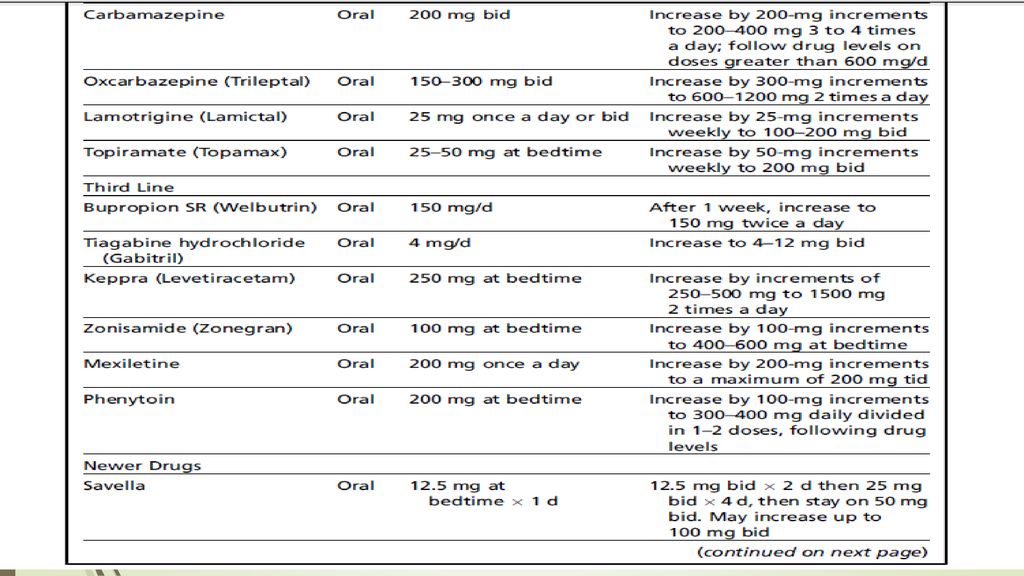
If a patient’s with diabetic neuropathy does not complain of pain, symptomatic treatment is of no value and is not necessary. Symptoms of numbness and tingling should not be treated The most frequently used oral drugs for the symptomatic treatment of diabetic and nondiabetic painful neuropathy are the tricyclic antidepressants, carbamazepine, gabapentin,mexiletene, and, more recently, pregabalin and cymbalta

53
Recent evidencebased guidelines for treatment of pain in diabetic neuropathy were published by the American Academy of Neurology. According to this, pregabalin is established as effective and should be offered for relief of Diabetic Polyneuropathy (DPN). Venlafaxine, duloxetine, amitriptyline, gabapentin, valproate, opioids (morphine sulfate, tramadol, and oxycodone controlled release), and capsaicin are probably effective and should be considered for treatment of PDN.
. Venlafaxine, duloxetine, amitriptyline, gabapentin, valproate, opioids (morphine sulfate, tramadol, and oxycodone controlled release), and capsaicin are probably effective and should be considered for treatment of PDN.")
54
Topical therapy with capsaicin and lidocaine creams can be tried.
In our experience, few patients respond to these modalities and the creams are difficult to use because they need to be applied several times a day. Lidoderm patches may be effective, but they are expensive and cumbersome to apply to the soles of both feet. Transcutaneous nerve stimulation is occasionally helpful. An unusual alternative medicine approach to painful neuropathies with magnetic inserts has received some attention.

55
larger multicenter study of repetitive and cumulative exposure to low frequency pulsed electromagnetic fields in 225 subjects with painful diabetic neuropathy did not show any effect on pain reduction. Exercise therapy is being investigated as another treatment modality. A small pilot study reported improvements in neuropathic pain.

59
Autonomic neuropathy

60
Autonomic manifestations can affect cardiovascular, genitourinary, or gastrointestinal organ systems so that patients develop orthostasis, tachycardia/ tachyarrhythmias, gastroparesis,, bladder atony, or impotence. Other autonomic manifestations include profuse nocturnal or postprandial sweating and abnormal pupillary light responses.

61
Diabetic diarrhea and incontinence are rare but can be disabling
Diabetic diarrhea and incontinence are rare but can be disabling. Gastrointestinal autonomic dysfunction is assessed with various radiographic techniques, but the easiest is to show the abnormally slow passage of barium through the gut. Impotence is the most common clinical manifestation of autonomic neuropathy, affecting more than 50% of men with diabetes.

62
Midodrine (ProAmatine) is an alpha-adrenoreceptor agonist that increases blood pressure by producing arterial and venous constriction. The recommended dose is 10 mg 3 times daily. Pharmacotherapy can be tried for delayed gastric emptying (metoclopramide; erythromycin) and diarrhea (clonidine). Impotence can be treated with oral phosphodieterase-5inhibitors such as sildenafil (Viagra) and, less commonly, with injectable (phentolamine/ papervine) drug therapy or penile prosthesis.
 and diarrhea (clonidine). Impotence can be treated with oral phosphodieterase-5inhibitors such as sildenafil (Viagra) and, less commonly, with injectable (phentolamine/ papervine) drug therapy or penile prosthesis.")
63
Symmetric neuropathies with episodic symptoms

64
Diabetic neuropathic cachexia is an uncommon syndrome initially described by Ellenberg144 in 1974 in which patients develop profound weight loss, a symmetric sensory peripheral neuropathy, and painful dysesthesias over the limbs and trunk, without associated weakness.

65
Unlike other symmetric neuropathies caused by diabetes, diabetic neuropathic cachexia is reversible over a period of weeks to months. Most reported patients have been men, usually in the sixth or seventh decades of life, but there have been 2 cases described in women. All cases initially show a precipitous weight loss of up to 60% of total body weight, leading at times to an incorrect suspicion of an underlying cancer. Patients may experience intense contact hypersensitivity and may also describe intermittent stabbing or shooting pains.

66
The pain tends to be worse at night or during periods of relaxation
The pain tends to be worse at night or during periods of relaxation. The presence of proximal or truncal symmetric dysesthesias associated with profound weight loss should be clinical clues that support the diagnosis of diabetic neuropathic cachexia rather than the more common DSPN of diabetes.

67
Patients may also experience depression, anorexia, and impotence.
Sensory impairment associated with diabetic neuropathic cachexia is generally minimal, by contrast with the severity of the patient’s complaints of pain, and in some cases may not be clinically detectable. Some reports describe associated muscle atrophy and weakness, whereas others have reported normal strength.

68
Diabetic neuropathic cachexia can occur in patients with both type 1 and type 2 diabetes. There is a lack of correlation with other microvascular complications of diabetes such as nephropathy or retinopathy. Most cases are associated with poor glucose control. Some of these cases have been associated with malabsorption.

69
Treatment of diabetic neuropathic cachexia can be difficult and strict diabetic control is usually necessary. The usual drugs to treat neuropathic pain can be tried, but they are often unsuccessful and the temporary use of narcotics is often needed. The prognosis is usually good, and patients typically recover their baseline weight with resolution of the painful sensory symptoms within 1 year. A residual sensorimotor neuropathy is common.

70
Other possible transient symmetric sensory neuropathies

71
Other cases of transient distal sensory paresthesias and pain have been alleged to be caused by hyperglycemia (hyperglycemic neuropathy) or insulin neuritis following the institution of insulin. The insulin neuritis is usually characterized by acute severe pain, peripheral nerve degeneration, and autonomic dysfunction after intensive glycemic control, which often parallels worsening retinopathy and resolves in weeks or months.

73
Proximal and Asymmetric Phenotypes

74
Diabetic neuropathy presents with varied manifestations, including proximal and asymmetric types.
Except for entrapments, diabetic amyotrophy is the most common form of asymmetric diabetic neuropathy. Diabetic amyotrophy can present asymmetrically or symmetrically, with a rapid or insidious onset.

75
Symmetric form of diabetic amyotrophy can be indistinguishable from chronic inflammatory demyelinating polyneuropathy. Treatment of diabetic amyotrophy with intravenous immunoglobulin or immunosuppressive drugs is controversial.

76
diabetic amyotrophy because of the muscle atrophy in the thighs
diabetic amyotrophy because of the muscle atrophy in the thighs. But this term can falsely imply that the primary lesion is on the muscle and therefore we use the term DLSRP.

77
Clinical presentation
DLSRP syndrome affects an older group of diabetic individuals, more frequently men, usually older than 50, but occasionally we have seen the syndrome in middle-aged diabetic individuals. Most patients have type 2 diabetes mellitus; however, this can occur even in individuals with type 1 diabetes.

78
The development of this neuropathy is often unrelated to glucose control or the duration of glucose intolerance. DLSRP can be the presenting manifestation leading to the initial diagnosis of diabetes

79
This neuropathy begins with severe unilateral pain in the back, hip, or thigh, which subsequently spreads to the other side within weeks to months. Patients are frequently misdiagnosed as having a compressive lumbosacral radiculopathy. Some patients undergo unnecessary lumbar surgery despite minor changes on lumbar magnetic resonance imaging (MRI) scan
 scan.")
80
Given the associated weight loss, patients are often suspected to have a pelvic tumor. Within days to weeks of the pain onset, patients develop weakness in typically proximal and, to a lesser extent, distal leg muscles. On examination, there is weakness of hip flexors, adductors and extensors, knee flexors and extensors, and ankle dorsi flexors and plantar flexors of varying degree. Profound atrophy of the thigh and at times distal lower extremity muscles develops.

81
On examination, there is weakness of hip flexors, adductors and extensors, knee flexors and extensors, and ankle dorsiflexors and plantar flexors of varying degree. Profound atrophy of the thigh and at times distal lower extremity muscles develops. Weakness usually encompasses multiple root or plexus levels and is rarely isolated to an individual root or peripheral nerve.

82
Thus, in cases in which knee extension weakness is prominent and the possibility of a diabetic “femoral neuropathy” is considered, if one looks closely at other L2–L4 muscles either on the neurologic examination or with needle electromyography (EMG), the disease process can usually be found in these adjacent areas.
, the disease process can usually be found in these adjacent areas.")
83
Similarly, if there is a significant foot drop, there is also usually evidence of involvement in tibial or other L5 innervated muscles, and the process is actually to the peroneal nerve. There is usually distal sensory loss, but this is often indistinguishable from the sensory abnormalities of distal symmetric polyneuropathy (DSPN), which often is present before the development of the radiculoplexopathy. Loss of knee and ankle reflexes is common.
, which often is present before the development of the radiculoplexopathy. Loss of knee and ankle reflexes is common..")
84
Although the condition usually begins in one leg, spread to the other leg within weeks or months is rather frequent. The disorder worsens in a gradually progressive or stepwise manner. Cases have been documented in which there is worsening for 18 months. Eventually, the process stabilizes and gradually improves, although the recovery may take many months. In many cases, some degree of permanent weakness may persist.

85
about one-third of the cases, weakness spreads to proximal arm muscles and is attributed to cervicobrachial radiculoplexopathy. Approximately 12% of patients develop thoracic radiculopathy, leading to radiating pain in the chest or abdomen and intercostal muscle weakness. Respiratory weakness has also been described with this neuropathy.

86
Diagnostic workup

87
Electrophysiologically, nerve conduction study findings may not differentiate DLSRP neuropathy from DSPN, except for an asymmetric reduction of the femoral compound muscle action potential amplitudes in unilateral cases. However, the needle EMG reveals abundant fibrillation potentials in weak proximal and distal leg muscles, as well as in the lumbosacral para spinous muscles.

88
The cerebrospinal fluid (CSF) protein is often elevated, usually between 60 and 100 mg/dL, but occasionally as high as 400 mg/dL. The erythrocyte sedimentation rate may be elevated as well, but is usually less than 50 mm/h. MRI with gadolinium may show nerve root enhancement.

89
Sural nerve biopsy is not essential to the diagnosis of DLSRP syndrome
Sural nerve biopsy is not essential to the diagnosis of DLSRP syndrome. When done to exclude mimics, it shows significant fiber loss, often in an asymmetric fashion within and between fascicles, resembling focal ischemia . An ischemic pathogenesis was documented by Raff and colleagues in an autopsy study showing infarcts of proximal nerve trunks of the leg and lumbosacral plexus.

90
Asymmetric fiber loss in sural nerve may support this theory; however, it should be remembered that even patients with typical DSPN may show this multifocal pattern at times. The presence of occasional thinly myelinated fibers on plastic- embedded sections or short, thin segments on teased nerve fiber preparations should not lead the physician to diagnose a demyelinating neuropathy, as these findings can be seen in DSPN as well.

91
However, it should be emphasized that the electrophysiologic, biopsy, and laboratory features are often not particularly helpful, and the diagnoses of DLSRP is primarily clinically based on the history and neurologic examination.

92
There is probably a small subset of diabetic patients with amyotrophy who develop a painless, symmetric proximal neuropathy involving the lower extremities. Asburyfavoring the term proximal diabetic neuropathy, considered that there was a spectrum ranging from asymmetrical cases with a rapid onset to patients with symmetric proximal weakness of insidious onset.

93
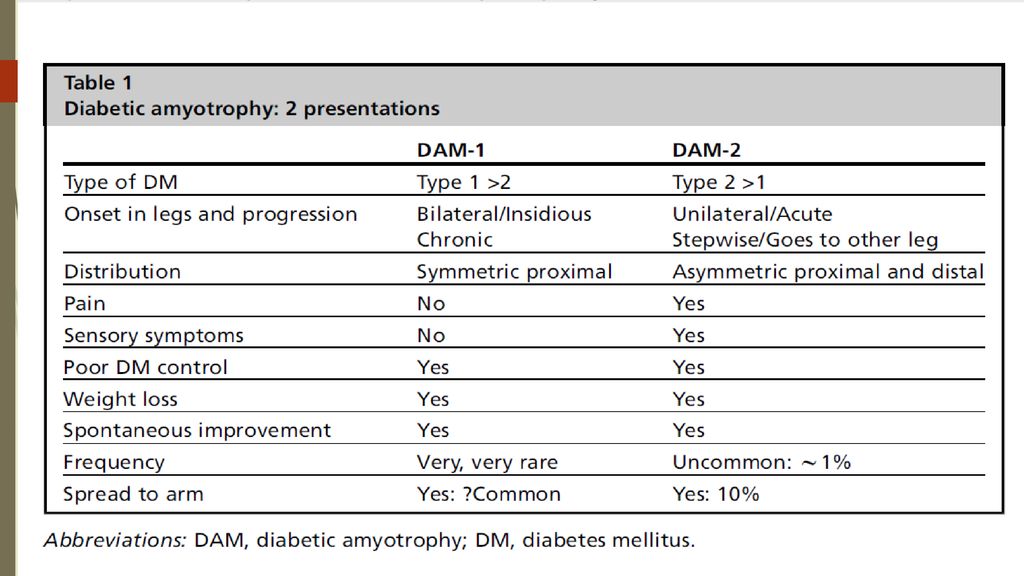
However, the symmetric presentation seems to be uncommon and tends to occur more often in young type 1 diabetic individuals who are having poor glycemic control. Therefore, we have divided the proximal diabetic amyotrophies (DAM) into 2 forms: DAM-1 and DAM-2
 into 2 forms: DAM-1 and DAM-2.")
94
If asymmetric diabetic neuropathies occur in only about 1% of the diabetic population, we think the painless, symmetric form of diabetic amyotrophy (DAM-1) is even more uncommon. This form superficially resembles idiopathic CIDP. We believe that for every 10 to 20 patients with asymmetric/painful amyotrophy (DAM- 2) seen at a tertiary care neuromuscular centers, only one DAM-1 patient will be seen. Whetheror not the pathogenesis of DAM-1 is different from DAM-2 and is more in line with metabolic dysfunction is unknown.
 seen at a tertiary care neuromuscular centers, only one DAM-1 patient will be seen. Whetheror not the pathogenesis of DAM-1 is different from DAM-2 and is more in line with metabolic dysfunction is unknown..")
97
Management

98
Treatment is centered around pain control and strict glycemic control
Treatment is centered around pain control and strict glycemic control. Both groups spontaneously improve over a period of months. Physical therapy can assist in improving functional mobility. Controversy involving DLSRP is whether or not there is an immune-mediated pathogenesis component and if patients respond favorably to immunomodulating therapy.

99
This concept was first introduced by Bradley and colleagues29 in in their report of 6 patients with a painful lumbosacral plexopathy, elevated sedimentation rate, mild perivascular inflammation on sural nerve biopsy, and asymmetric nerve fiber loss. Five were treated with immunosuppressive drugs (prednisone alone or prednisone and cyclophosphamide) and 4 improved or stopped progressing.
 and 4 improved or stopped progressing..")
100
In the Mayo Clinic group series by Pascoe and colleagues, 3 of 9 patients undergoing sural nerve biopsy had a multifocal distribution of fiber loss, and 2 had perivascular mononuclear inflammatory infiltrates. Twelve were treated with IVIG, and 9 improved. Of the 29 untreated patients, 17 spontaneously improved.

101
They concluded that the “efficacy of immunotherapy is unproven but such intervention may be considered in the severe progressive cases or ones associated with severe neuropathic pain.

102
The experience of the French group led by Gerard Said is important to note. In an article published in 1994, they reported inflammatory and ischemic lesions in nerve biopsy specimens of the intermediate cutaneous nerve of the thigh in patients with DLSRP. Three patients with “severe and prolonged painful disability” improved dramatically with corticosteroid treatment..

103
In a subsequent report in 1997 of 4 patients with DLSRP, Said and colleagues10 described patients who had symptoms for 4, 6, 12, and 18 months before biopsy ,Although all patients showed perivascular inflammation on nerve biopsy, to the investigators’ surprise, all became pain free with subsequent improvement of their weakness shortly following the biopsy. They concluded that despite the treatment with prednisone they used in their initial article, that DLSP “is self-limited and does not require the use of corticosteroids or immunomodulators.”

104
In a series by Dyck and colleagues, all 33 patients with DLSRP had some evidence of microvasculitis on nerve biopsy, and nearly all improved spontaneously. A report by the group from Houston found 18 of 19 patients with DLSRP had substantial improvement without immunomodulating therapy.

105
Despite many months of persistent symptoms or progression in some patients with DLSRP, eventually all patients spontaneously have resolution of pain and slow improvement of weakness . Treatment with IVIG or other immunosuppressive drugs is controversial. In a prospective case series, 5 patients with severe pain received IVIG after having no response to symptomatic therapy for pain and corticosteroids. Four had a decrease in pain

106
In contrast, Zochodne and colleagues in 2003 reported a patient who developed DLSRP while on immunosuppressive regimen consisting of cyclosporine and myophenolate mofetil for an allograft cardiac transplant and 2 patients with DLSRP who did not respond to IVIG treatment, arguing that immunosuppressive therapy did not prevent onset of DLSRP. In our opinion, we do not believe IVIG should be used in patients with DLSRP. At this time, we are not convinced that this form of immunomodulating therapy is indicated

107
Perhaps this question can be resolved with a controlled trial, but such a trial will be difficult, as each center sees a handful of patients annually and it will be difficult to get the pharmaceutical industry and the Food and Drug Administration to support a large multicenter IVIG trial in this rare disorder.

108
On the other hand, the experience of Said and Bradley with the improvement of pain with prednisone should not be ignored. According to a recent Cochrane review of immunotherapy for diabetic amyotrophy (DA) only one completed controlled trial using IV methyprednisolone in DA was found.
 only one completed controlled trial using IV methyprednisolone in DA was found.")
109
High doses of corticosteroids may lead to improvement of severe pain in some patients with DLSRP, and this may be analogous to the improvement of neuropathic pain in patients who are believed to have reflex sympathetic dystrophy. Perhaps breaking the pain syndrome in this manner may subsequently allow patients to begin moving their weak extremities easier. Presently, there is no convincing evidence from randomized trial to support any recommendation on the use of any immunotherapy treatment in DLSRP.

110
We believe one should be cautious about jumping to the conclusion that finding mild perivascular inflammation on biopsy, or demyelination features on either electrophysiology or pathology suggest that DLSRP is a disease that is primarily immune-mediated and will respond to immunomodulating therapy.

111
We cautioned previously about the danger of heavily relying on electrophysiologic evidence of demyelination on nerve conduction studies (NCS) of diabetic patients, as some will fulfill research electrophysiologic criteria for CIDP even though the clinica pattern does not correspond to CIDP, but actually is that of DLSRP. Similar caution should be used with data from nerve biopsies of patients with DLSRP in concluding these patients have either vasculitis or a demyelinating neuropathy.

112
In routine clinical practice, we do not recommend either nerve biopsy or immunomodulating therapy in patients with typical DLSRP. Finally, we would also caution clinicians about splitting patients with otherwise typical DLSRP because of nerve root enhancement on lumbar MRI scan. If other etiologies are excluded by CSF analysis, the mere finding of root enhancement on MRI in DLSRP should not necessarily lead to the initiation of immunomodulating therapy.

113
Other DLSRP caveats

115
Cervical brachial radiculoplexopathy

116
Cervical brachial radiculoplexopathy Although cervical/brachial plexus involvement is uncommon, it does occur. In the classic early Mayo Clinic series of “diabeticpolyradiculopathy” reported by Bastron and Thomas in 1981 of 105 patients, 81 had lower extremity involvement, 15 had upper extremity involvement, and 12 had thoracic/abdominal involvement.

117
Obviously, a few patients had involvement of more than one region
Obviously, a few patients had involvement of more than one region. As mentioned previously, in the Mayo Clinic series of Pascoe and colleagues,11 all 44 patients had (by definition) leg weakness, and 12 of these also ad arm weakness (7 bilateral, 5 unilateral). Occasionally, patients with DLSRP develop arm pain and weakness days to weeks after the initial leg symptoms.
 leg weakness, and 12 of these also ad arm weakness (7 bilateral, 5 unilateral). Occasionally, patients with DLSRP develop arm pain and weakness days to weeks after the initial leg symptoms.")
118
The arm involvement is usually proximal and distal, similar to the pattern of weakness seen in the legs. Interestingly, the arm symptoms can begin or continue to progress after the leg symptoms have plateaued or begun to improve. Thus, whereas cervical/brachial root and plexus involvement

119
Thus, whereas cervical/brachial root and plexus involvement has not been emphasized a great deal in diabetic radiculoplexopathy, the clinician should be aware of this possibility. We do believe that in this setting, a more extensive workup probably is to exclude other disease entities. All of these patients should have a CSF examination for infectious and neoplastic diseases, and nerve biopsy is probably warranted to exclude true vasculitic neuropathy.

120
CIDP in diabetic patients

121
CIDP in diabetic patients
Diabetic patients can develop typical CIDP but, as mentioned previously, there is no increased risk of CIDP in diabetic patients. The clinical features of gradually progressive, usually painless, proximal and distal symmetric weakness and numbness in the arms and legs should be sufficient to distinguish CIDP from the typical symmetric and asymmetric diabetic neuropathies; however, the laboratory results in this setting may not be particularly helpful, especially the CSF protein.

122
if there is an underlying diabetic DSPN on NCS and needle EMG, electrophysiologic results can also be relatively unhelpful unless clear-cut and ample features of an acquired, markedly demyelinating neuropathy are present. In addition, nerve biopsy in many diabetic neuropathies can show thinly myelinated fibers, and therefore we usually do not pursue nerve biopsy in this setting. Diagnosis is usually based on the clinical presentation and it is reasonable to proceed with immunomodulating therapy when CIDP is strongly suspected.

123
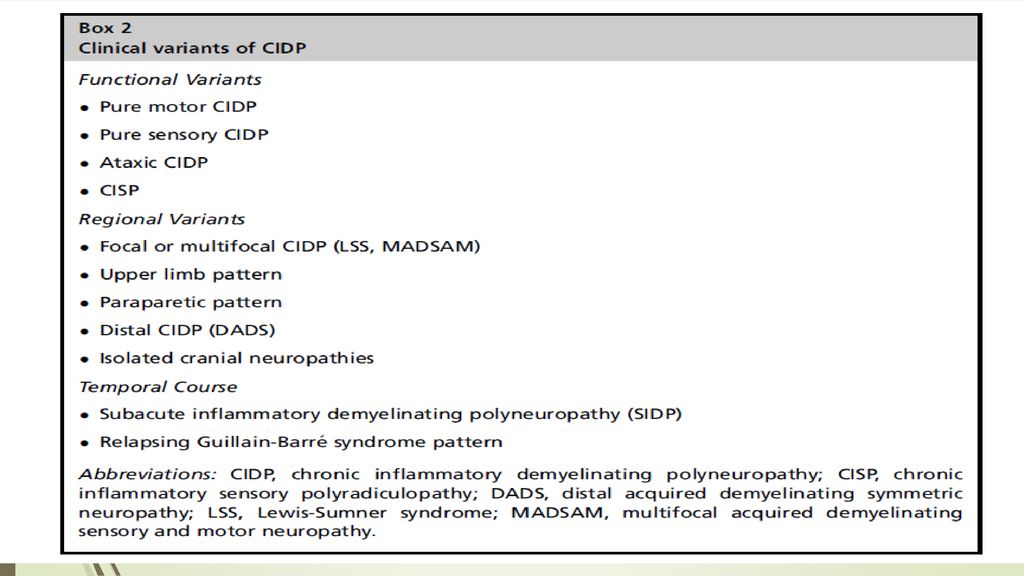
The classic description of CIDP includes
(1) progressive limb weakness involving proximal and distal muscles, sensory loss, and areflexia, and a relapsing or progressive course; (2) electrophysiological features of segmental demyelination, including prolonged distal motor and F-wave latencies, reduced conduction velocities, conduction block, and temporal dispersion; (3) albumino-cytologic dissociation in the cerebrospinal fluid (CSF) (4) inflammation, demyelination, and remyelination on nerve biopsy
 progressive limb weakness involving proximal and distal muscles, sensory loss, and areflexia, and a relapsing or progressive course; (2) electrophysiological features of segmental demyelination, including prolonged distal motor and F-wave latencies, reduced conduction velocities, conduction block, and temporal dispersion; (3) albumino-cytologic dissociation in the cerebrospinal fluid (CSF) (4) inflammation, demyelination, and remyelination on nerve biopsy.")
125
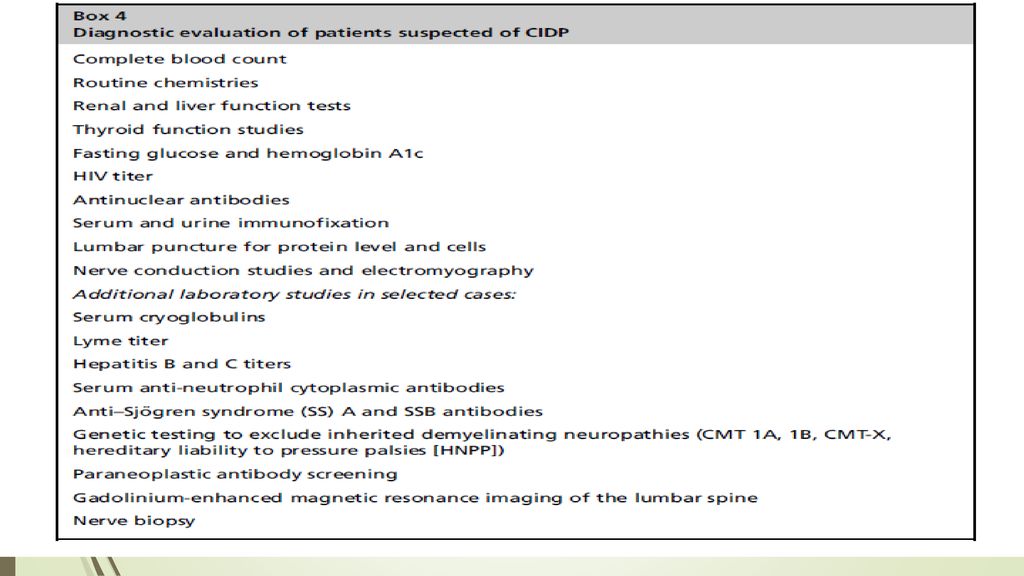
A lumbar puncture is indicated in most patients suspected of having CIDP. An elevated CSF protein level (>45 mg/dL) is detected in at least 80% of patients. The diagnosis of CIDP cannot be excluded based on a normal CSF protein concentration only. The cell count is usually normal, although as many 10% of patients have greater than 5 lymphocytes/mm3. The American Academy of Neurology (AAN) criteria has suggested that there should be fewer than 10 white blood cells in the spinal fluid, and fewer than 50 cells in patients with HIV infection
 criteria has suggested that there should be fewer than 10 white blood cells in the spinal fluid, and fewer than 50 cells in patients with HIV infection.")
127
ELECTRODIAGNOSTIC CRITERIA
(1) reduced conduction velocities (eg, <80% of the lower limit of normal [LLN] if the distal motor amplitude is normal, and <70% of LLN if the amplitude is substantially reduced); (2) prolonged distal motor latencies, (3) prolonged F-wave latencies (eg, >125% of the upper limit of normal [ULN] if the distal motor amplitude is normal, and >150% of ULN if the amplitude is reduced for distal latencies and F-waves); and, (4) conduction block/temporal dispersion (eg, conduction block is >50% reduction of proximal/distal [p/d] amplitude and abnormal temporal dispersion is >130% increase of p/d duration).
 reduced conduction velocities (eg, <80% of the lower limit of normal [LLN] if the distal motor amplitude is normal, and <70% of LLN if the amplitude is substantially reduced); (2) prolonged distal motor latencies, (3) prolonged F-wave latencies (eg, >125% of the upper limit of normal [ULN] if the distal motor amplitude is normal, and >150% of ULN if the amplitude is reduced for distal latencies and F-waves); and, (4) conduction block/temporal dispersion (eg, conduction block is >50% reduction of proximal/distal [p/d] amplitude and abnormal temporal dispersion is >130% increase of p/d duration).")
129
True mononeuritis multiplex in diabetes: does it exist?

130
Finally, a comment should be made regarding “mononeuritis multiplex” in diabetic patients. We suspect that most of these patients have diabetic radiculoplexopathy, usually lumbosacral, but rarely cervical-brachial.

131
It is uncommon for diabetic patients to develop a true mononeuritis multiplex in which individual distal peripheral nerves (eg, femoral, peroneal, tibial, ulnar, median or radial) are “picked-off” in a subacute or acute fashion. It is difficult to find good documentation of this in the literature. Although the early articles by Raff and colleagues use the term “mononeuropathy multiplex,” if one reads of clinical description of their 7 cases, they all had typical DLSRP with proximal and distal involvement not confined to an individual nerve.

132
If a diabetic patient develops a true mononeuritis multiplex, the usual causes need to be pursued (vasculitis, infectious, and hereditary). We believe that if one wants to include diabetes mellitus in the differential diagnosis of true mononeuritis multiplex, it should be at the bottom of such a list.

133
OTHER ASYMMETRIC NEUROPATHIES Truncal Radiculopathy

134
Clinical presentation
Patients develop abrupt pain over days to weeks with severe dysesthesias in a dermatomal pattern. In some patients, the pain may not radiate entirely around the trunk in a full radicular pattern, but the symptoms and signs may occur in smaller, restricted regions that imply damage of the dorsal or ventral rami or their medial or lateral branches.

135
Patients can occasionally develop weakness of the rectus abdominus muscles. Some patients may present with pseudohernia caused by weakening of the abdominal musculature. On the other hand, although most patients do not demonstrate obvious motor involvement, needle EMG can reveal abnormalities in the paraspinous or abdominal wall muscles.

136
Diagnostic workup Nerve conductions may reveal abnormalities related to distal symmetric polyneuropathy.Needle EMG findings include fibrillations in the paraspinous or abdominal wall muscles.

137
Management Treatment is directed at symptomatic pain management.
Truncal radiculopathy should be distinguished from the wedge- shaped midline area of symmetric truncal sensory loss that can occur in advanced DSPN and from rare discogenic thoracic radiculopathy.

138
Prognosis The natural history is similar to DLSRP, with persistence of sensory symptoms for weeks to months, with gradual resolution.

139
Cranial Neuropathies Diabetic patients can suddenly develop a unilateral third, fourth, sixth, or seventh cranial nerve palsy. The oculomotor nerve was found to be most frequently affected in one study by Greco and colleagues looking at 61 patients with diabetic cranial nerve palsies. The hallmark of diabetic third nerve palsy is pupillary sparing in most cases.

140
Retro-orbital pain accompanies about half of the cases
Retro-orbital pain accompanies about half of the cases. Sparing of the pupil in diabetic third nerve palsies is due to sparing of axons at the periphery of the nerve involved in pupillary function. Pathologic evidence supports the concept that the process is probably attributable to an ischemic watershed phenomenon in the central part of the nerve.

141
It has been suggested that patients with diabetes are more likely to develop a seventh cranial nerve palsy. However, Bell palsy is a common event and it is difficult to substantiate if it is indeed more prevalent in diabetes. It is interesting to note that in the Rochester Diabetic Neuropathy Study, neither cranial mononeuropathies nor truncal radiculopathies were more common in diabetic patients compared with control subjects.

142
Diagnostic workup Imaging studies may be necessary to rule out stroke in some cases; however, history alone without additional testing is sufficient in most of these patients.

143
Management and prognosis
The main risk factors for the development of cranial neuropathies are duration of diabetes and the patient’s age. Treatment should be mainly focused on management of diabetes. Most patients make a full recovery, with some early evidence of improvement within 2 to 3 months.

144
Isolated Mononeuropathies

145
Isolated Mononeuropathies
It is generally believed and established in studies that diabetic individuals are more susceptible to compression injuries compared with non diabetic individuals. This would include the median nerve at the carpal tunnel, ulnar nerve at the elbow, the peroneal (fibular) nerve at the fibular head, and perhaps the lateral cutaneous femoral nerve (meralgia paresthetica) at the hip.
 nerve at the fibular head, and perhaps the lateral cutaneous femoral nerve (meralgia paresthetica) at the hip.")
146
In the early study by Mulder and colleagues in 103 cases of diabetes, 16 had mononeuropathies affecting 29 nerves as follows: common peroneal, 13; median nerve (carpal tunnel), 9; ulnar nerve, 5; lateral femoral cutaneous nerve, 1; and femoral nerve, 1, the latter being likely due to DLSRP. Meralgia paresthetica (mononeuropathy of the lateral femoral cutaneous nerve) is associated with diabetes mellitus irrespective of obesity and advanced age
 is associated with diabetes mellitus irrespective of obesity and advanced age.")
147
In a study from Rochester, Minnesota, there was evidence that carpal tunnel syndrome is more common in diabetes mellitus than in the general population. In another Rochester Diabetic Neuropathy Study, approximately one-quarter of patients had subclinical carpal tunnel syndrome on NCS, but only 7.7% were symptomatic.

148
Diagnostic workup Diagnosis is usually established with electrophysiologic testing; however, electrophysiologic diagnosis of carpal tunnel or other mononeuropathies is sometimes difficult in individuals with diabetic polyneuropathy.

149
DIABETIC MUSCLE INFARCTION

150
DIABETIC MUSCLE INFARCTION
In the context of discussing the various diabetic neuropathies, it is relevant to review another neuromuscular complication of diabetes in which the muscle itself is the target organ rather than the nerve. It is an underdiagnosed complication of long-standing diabetes.

151
Clinical Presentation
Diabetic muscle infarction (DMI) begins with the abrupt onset of thigh pain, tenderness, and swelling. Over a period of days, a firm mass develops in nearly half of cases. The muscles most frequently involved are the vastus lateralis and medialis, thigh adductors, and biceps femoris. Calf involvement is reported in up to 20% of cases and bilateral involvement in 8% of cases.
 begins with the abrupt onset of thigh pain, tenderness, and swelling. Over a period of days, a firm mass develops in nearly half of cases. The muscles most frequently involved are the vastus lateralis and medialis, thigh adductors, and biceps femoris. Calf involvement is reported in up to 20% of cases and bilateral involvement in 8% of cases.")
152
Compared with 130 cases, there are 5 case reports of DMI affecting muscles of the upper limb of patients, particularly in patients with type 2 diabetes with end-stage renal disease

153
Edema from the swelling can extend to the knee and mimic a joint effusion.
DMI tends to occur in younger, poorly controlled diabetic patients with other end-organ complications. There are no associated systemic symptoms or signs indicative of infection and no skin discoloration suggesting cellulitis or thrombophlebitis.

154
The painful mass persists for weeks, occasionally with exacerbation of symptoms, and then spontaneously resolves over weeks to several months. Contralateral involvement of the other thigh can occur, even after the initial episode resolves. Up to 50% of cases will recur, mostly involving previously unaffected muscle groups

155
Diagnostic Workup Creatine kinase can be normal or modestly elevated. Needle EMG demonstrates fibrillation potentials in the involved muscles with a loss of voluntary motor unit potentials in the most affected areas. Remaining motor unit potentials may be brief and short, reflecting fragmentation of the motor unit.

156
MRI scan of the limb muscle reveals increased signal on T2-weighted images in the involved thigh muscles, indicative of marked muscle edema extending into the perifascicular and subcutaneous tissues . Gadolinium contrast administration is contraindicated in those with renal impairment. Radionuclide imaging with Technetium-99 demonstrates radiopharmaceutical accumulation and muscle ultrasound shows hyperechoic signal in the mass.

157
Biopsy of the region consists of large confluent areas of muscle necrosis and edema, with loss of the normal architectural pattern. A muscle biopsy is often not needed because it may prolong recovery and is indicated only when the presentation is atypical, response is poor, or diagnosis is uncertain. Biopsy, when performed,

159
Although there are obvious differences between DMI and DLSRP ,the abrupt onset of both syndromes, and pathologic evidence for probable focal ischemia in the muscle (DMI) and nerve (DLSRP) supports the theory that both entities have a primary vascular microangiopathic etiology.
 and nerve (DLSRP) supports the theory that both entities have a primary vascular microangiopathic etiology.")
160
Management and Prognosis
The treatment of DMI is supportive. No evidence-based recommendations are available on management of this condition; however, a retrospective analysis supports conservative management with bed rest, leg elevation, and adequate analgesia. Activities should be avoided to avoid increasing the pain. There is no evidence to support the use of corticosteroids or surgery. Short-term prognosis is good, but the recurrence rate is high (40%), and recurrences may not affect the same muscle group.
, and recurrences may not affect the same muscle group.")
Similar presentations















 Embolism Trauma Crush injuries.>")




>")
>")
