Download presentation
Presentation is loading. Please wait.

1
Acute complication of peptic ulcer disease
Bleeding peptic ulcer Acute complication of peptic ulcer disease

2
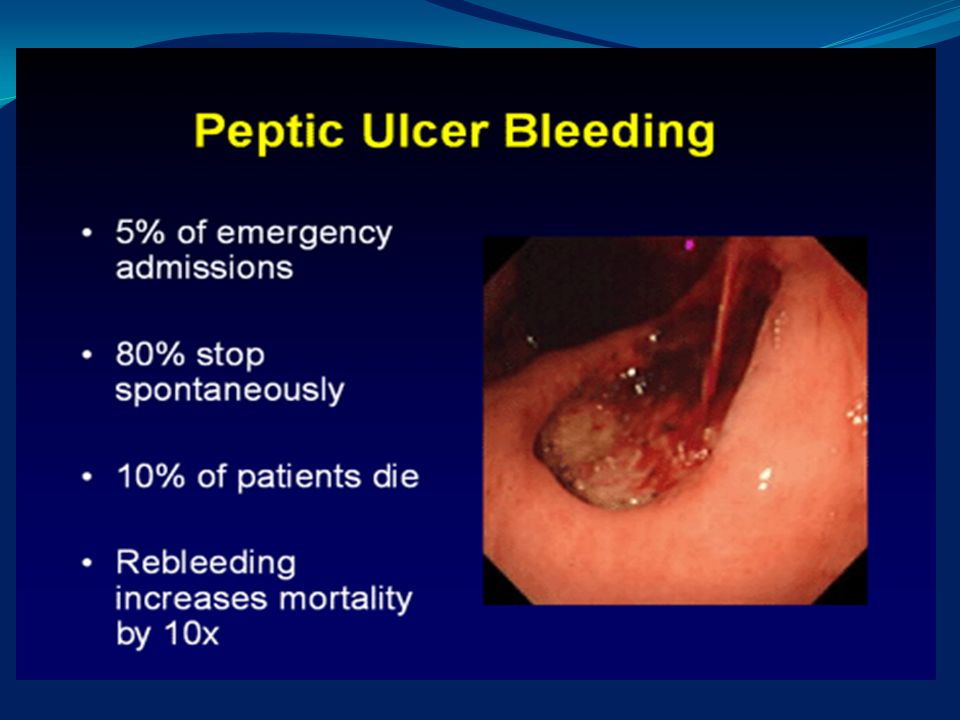
Bleeding peptic ulcer PU is the most common cause of acute hemorrhage in the UGI tract - 50% of cases. Although hospitalization and surgery for uncomplicated PU has decreased over the past 30 years, The number of hospital admissions for hemorrhage associated with PU has remained relatively unchanged.

3
Bleeding peptic ulcer Bleeding from ulcers ceases spontaneously in at least 80% of patients However, a subgroup of patients with bleeding ulcers does not fare as well. Overall mortality rate has remained around 6% for the past 30 years. .

5
Mortality rate Two possible explanations for this unchanging mortality rate: age and comorbidities. Patients with bleeding usually die not from exsanguination but from decompensation due to other diseases.

6
Histologic Features Histologic examination of a surgically resected gastric ulcer associated with bleeding reveals an artery eroded by the crater of the ulcer. In most cases the diameter of the bleeding artery is small (less than 2 mm.) A larger arterial size is probably associated with increased morbidity and mortality, as well as a decreased likelihood of success with endoscopic therapy.
 A larger arterial size is probably associated with increased morbidity and mortality, as well as a decreased likelihood of success with endoscopic therapy.")
7
Predisposing Factors High levels of acid secretion do not appear to account for the development of bleeding in patients with PU. Basal and stimulated acid output is similar in patients with bleeding duodenal ulcers and in those with nonbleeding ulcers. The prevalence of Helicobacter pylori in patients with bleeding ulcers may be 15 to 20 percent lower than in patients with nonbleeding ulcers.

8
Predisposing Factors The use of NSAIDs is reported to be an important risk factor for bleeding ulcers. A recent meta-analysis found that an age over 60 years and use of NSAIDs for less than one month were associated with higher risks of complications. Ingestion of NSAIDs may cause both gastric and duodenal ulcers.

9
Predisposing Factors Complications may occur soon after the initiation of NSAID therapy and appear to be more common during the first month of therapy. The risk of an ulcer due to use of aspirin or non-aspirin NSAIDs is dependent on the dose.

10
Predisposing Factors Recent evidence indicates that 10 mg of aspirin a day virtually obliterates the synthesis of platelet thromboxane B2 But does not significantly decrease the output of gastric prostaglandin E2 or increase gastric injury.

11
Predisposing Factors Steroids - double the NSAID-associated risk of serious gastrointestinal complications, Concomitant use of steroids and NSAIDs may be associated with a 10-fold increased risk. Although anticoagulation therapy would seem likely to increase the risk of bleeding in patients with PU, placebo-controlled trials with warfarin (which generally exclude patients with known ulcer disease) have not documented a significant increase in bleeding ulcers.
 have not documented a significant increase in bleeding ulcers.")
12
Clinical Presentation
20 % of patients who have bleeding ulcers present with melena, 30 % with hematemesis 50 % with both.

13
Clinical Presentation
Whether the rectal output is bright red ( hematochezia) or black (melena) is determined by the volume and rapidity of blood loss
 or black (melena) is determined by the volume and rapidity of blood loss.")
14
Clinical Presentation
Melena can result when as little as 50 to 100 ml of blood is experimentally introduced into the upper gastrointestinal tract, Whereas 1000 ml or more of blood always leads, at least initially, to hematochezia.

15
Clinical Prognostic Factors
Clinical markers that indicate severe bleeding or a high risk of further hemorrhage include: hemodynamic instability on presentation, bleeding manifested as repeated red hematemesis or hematochezia, failure of the gastric aspirate to clear with lavage.

16
Clinical Prognostic Factors
Advanced age (over 60 years) and the presence of serious underlying medical illness are important in predicting survival after an acute episode of bleeding. A study of 701 patients with bleeding peptic ulcers reported a mortality rate of 10 % among patients over the age of 60 years, 0.5 % among those 60 or younger
 and the presence of serious underlying medical illness are important in predicting survival after an acute episode of bleeding. A study of 701 patients with bleeding peptic ulcers reported a mortality rate of. 10 % among patients over the age of 60 years, 0.5 % among those 60 or younger.")
17
Prognostic Features at Endoscopy
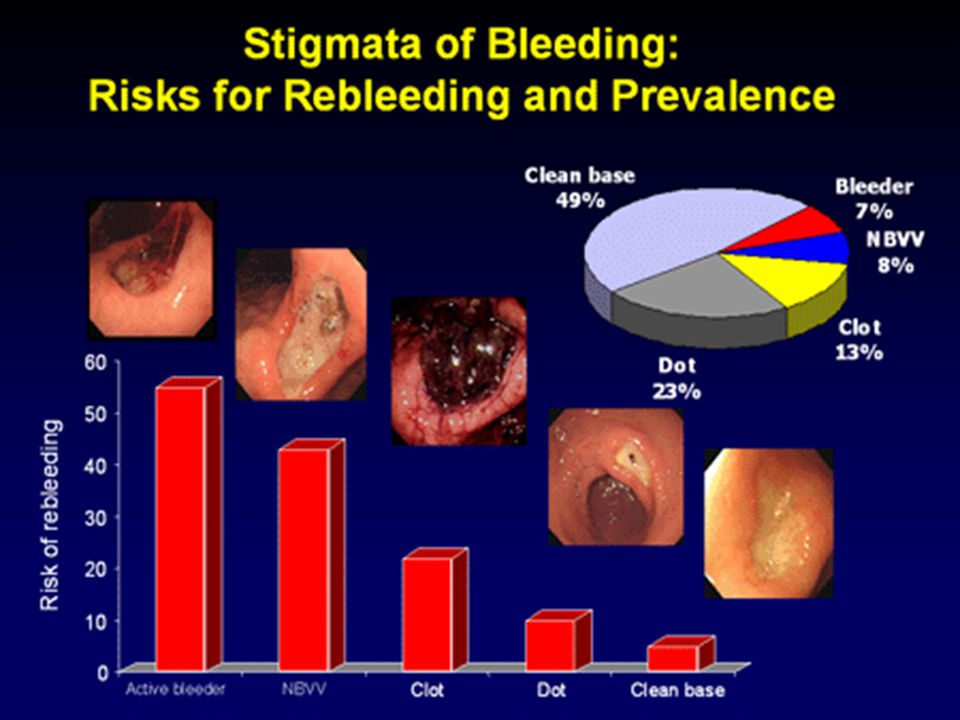
The endoscopic appearance of an ulcer may provide the most helpful prognostic information. The ulcer may have a clean base or have one of several stigmata of hemorrhage: a flat pigmented spot (red, purple, brown, or black), an adherent clot, a visible vessel (a smooth-surfaced protuberance or plug in the base of the ulcer), active bleeding (either oozing or spurting).
, an adherent clot, a visible vessel (a smooth-surfaced protuberance or plug in the base of the ulcer), active bleeding (either oozing or spurting).")
18
Prognostic Features at Endoscopy
The size of an ulcer is also a prognostic indicator. Patients with ulcers larger than 1 or 2 cm in diameter have increased rates of rebleeding and death, even after endoscopic hemostatic therapy. Large ulcers are more frequently found to have stigmata of recent hemorrhage than are small ulcers.

20
Doppler ultrasound A Doppler ultrasound probe passed through the biopsy channel of an endoscope has been used to identify evidence of blood flow beneath the surface of the ulcer. Rebleeding is rare in the absence of a Doppler signal from the base of the ulcer, but the clinical course in patients with Doppler-positive ulcers has not been well defined.

21
Initial Management Hemodynamic assessment (BP, PR, and postural changes) and, if necessary, institution of resuscitative measures are the first steps in the management of upper gastrointestinal bleeding. Clinical prognostic features and the initial response to resuscitation are used to decide whether a patient should be hospitalized and, if so, what level of care should be provided.
 and, if necessary, institution of resuscitative measures are the first steps in the management of upper gastrointestinal bleeding. Clinical prognostic features and the initial response to resuscitation are used to decide whether a patient should be hospitalized and, if so, what level of care should be provided.")
22
Initial Management Patients with clinical characteristics - high risk of further bleeding or death should be admitted to an ICU. Patients predicted to do well may be admitted to a regular ward or may even be kept in the emergency department until diagnostic endoscopy has been performed.

23
Initial Management Healthy, young patients presenting with clinically trivial bleeding may, in some cases, be discharged home without diagnostic evaluation but with arrangements for outpatient follow-up.

24
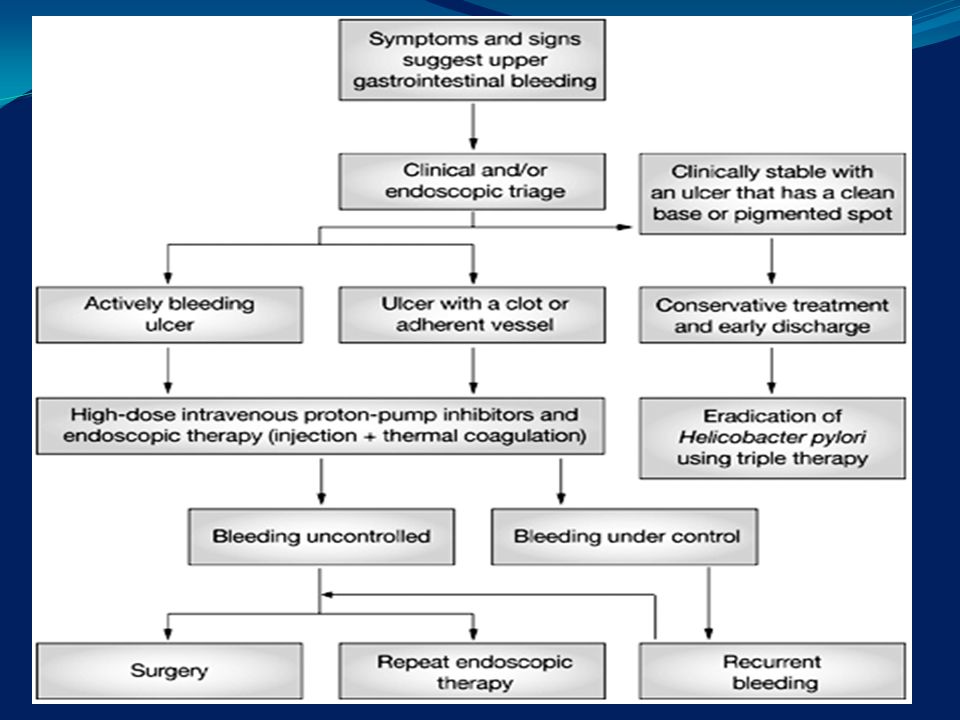
Endoscopy Endoscopic appearance of an ulcer provides an excellent complement to clinical factors in assessing the risk of further bleeding or death. Such information dictates management in terms of: therapy, level of hospital care, resumption of feeding, length of hospitalization.

25
Endoscopy Most patients with acute UGI bleeding should undergo endoscopic examination. Endoscopy should be performed as soon as safely possible in patients at high risk for further bleeding or death. Patients with minor bleeding who have been admitted to a medical ward can wait until the next day for endoscopy. Since the need for admission may be determined by the endoscopic findings, physicians should consider placing patients at low risk in a short-stay area while they await endoscopy.

26
Management Subsequent management of bleeding ulcers is determined by the results of endoscopy. Most studies indicate that among patients with clean-based ulcers, the rate of recurrent bleeding is 0%- 2%.

27
Management Patients with clean-based ulcers virtually never require urgent intervention for recurrent bleeding Assuming that there is no other reason for hospitalization, such patients are candidates for early discharge after resuscitation, stabilization, and institution of therapy. Patients whose condition is stabilized in the emergency department may be sent directly home.

28
Management Among patients with ulcers characterized by flat spots or adherent clots the incidence of rebleeding and urgent intervention is higher . Such patients require a longer period of hospitalization, although not in an intensive care unit.

29
Management Patients with actively bleeding ulcers or nonbleeding ulcers with visible vessels, who are at the highest risk for further bleeding and death, should spend at least one day in the ICU.

30
Management Since most episodes of recurrent bleeding occur within three days after the initial episode, we believe that patients who have an uncomplicated hospital course may be considered for discharge after three days. Such an approach has been corroborated by a recent study in which endoscopy was performed daily in 166 patients who had bleeding ulcers with clots or visible vessels at admission. The stigmata disappeared within three days in all the patients.

31
Management The period during which food is withheld from patients with bleeding ulcers varies widely. Many physicians routinely withhold food for the first one to three days after endoscopy.

32
Management Patients with endoscopic features indicating a low risk of further bleeding or death can therefore begin eating soon after the procedure. Patients with endoscopic findings suggesting a higher risk should receive nothing by mouth or only clear liquids for the first two days of hospitalization so that food in the stomach will not interfere with an urgent endoscopic or surgical procedure, which may be necessary if rebleeding ensues.

33
Treatment of Acute Bleeding Episodes
Dictated by the patient's clinical condition and the endoscopic findings. Medical Therapy There is no convincing evidence that gastric lavage with any fluid at any temperature will stop bleeding or prevent recurrent bleeding. If used to cleanse the stomach before endoscopy, lavage with room-temperature tap water minimizes the discomfort experienced by the patient.

34
Medical Therapy There is no convincing evidence that gastric lavage with any fluid at any temperature will stop bleeding or prevent recurrent bleeding. If used to cleanse the stomach before endoscopy, lavage with room-temperature tap water minimizes the discomfort experienced by the patient.

35
Medical therapy Pharmacologic agents that are vasoconstrictors or reduce gastric acidity or both, including vasopressin, secretin, prostaglandins, somatostatin, and H-receptor antagonists, have been used in an attempt to staunch the flow of blood from actively bleeding ulcers. In one double-blind trial 241 patients with endoscopic documentation of actively bleeding ulcers were randomly assigned to receive an intravenous infusion of somatostatin or placebo. Bleeding ceased in 88 percent of the patients treated with somatostatin and in 83 percent of those receiving placebo.

36
Medical therapy Reduction of gastric acidity.
Data from in vitro studies suggest that the dissolution of clots by proteolytic enzymes occurs more slowly at high pH levels. A recent double-blind trial compared the most potent antisecretory agent available, omeprazole (given intravenously during the first 24 hours, then orally for 3 more days), with placebo in 503 patients with bleeding ulcers. Bleeding recurred in 24 % of the patients receiving omeprazole and in 23 % of those receiving placebo.
, with placebo in 503 patients with bleeding ulcers. Bleeding recurred in 24 % of the patients receiving omeprazole and in 23 % of those receiving placebo.")
37
Medical therapy Another means of enhancing clot function is through the use of tranexamic acid, which inhibits fibrinolysis. A meta-analysis of six controlled trials showed no statistically significant reduction in recurrent bleeding or the need for surgery but did find, for reasons that are unclear, a 40 % reduction in mortality, which was significant.

38
Medical therapy Unfortunately, the applicability of these results to the management of bleeding ulcers is uncertain, because each of the trials included a substantial number of patients with bleeding from lesions other than peptic ulcers. Tranexamic acid is not approved by the Food and Drug Administration for the treatment of bleeding ulcers, and few U.S. physicians use it for this indication.

39
Medical therapy It is reasonable, however, to initiate therapy to promote healing. For most patients, in whom feeding is resumed shortly after endoscopy, such therapy will be in oral form. Intravenous administration of H2-receptor antagonists, which is more expensive than oral administration, can be reserved for those cases in which feeding is being delayed. The routine use of intravenous H2-receptor antagonists is neither necessary nor cost effective.

40
Endoscopic Therapy The lack of any clearly effective medical therapy for patients with bleeding ulcers has prompted a search for alternative forms of hemostatic therapy. The development of a variety of endoscopic therapies, has proved to be the most important advance in the treatment of bleeding ulcers over the past decade.

41
Endoscopic Therapy In the meta-analysis laser therapy did significantly reduce the rates of further bleeding, urgent surgery, and mortality. However, laser therapy may cause transmural injury and requires a high degree of technical expertise Laser units are very expensive, bulky, and usually impossible to transport. Laser therapy therefore cannot be recommended as the treatment of choice for bleeding ulcers.

42
Endoscopic Therapy Monopolar electrocoagulation, bipolar electrocoagulation, and heater-probe therapy use thermal contact - hemostasis . Monopolar electrocoagulation has been replaced by the other two methods primarily because of the concern that monopolar electrocoagulation causes a greater degree of tissue injury. In studies with animals, both bipolar electrocoagulation and heater probes are highly effective in stopping bleeding and coagulating mesenteric arteries up to 2 mm in diameter.

43
Endoscopic therapy Heat generated by electrical energy (with bipolar electrocoagulation) or thermal energy (with the heater probe) leads to coagulation and hemostasis. Maximal temperatures are 100 °C with bipolar electrocoagulation and 250 °C with the heater probe. Prospective, randomized trials have demonstrated that these approaches result in a significant reduction in further bleeding, blood transfusions, the length of the hospital stay, and the need for urgent surgery in patients with clinical evidence of major bleeding and endoscopic evidence of actively bleeding ulcers or nonbleeding ulcers with visible vessels.
 or thermal energy (with the heater probe) leads to coagulation and hemostasis. Maximal temperatures are 100 °C with bipolar electrocoagulation and 250 °C with the heater probe. Prospective, randomized trials have demonstrated that these approaches result in a significant reduction in further bleeding, blood transfusions, the length of the hospital stay, and the need for urgent surgery in patients with clinical evidence of major bleeding and endoscopic evidence of actively bleeding ulcers or nonbleeding ulcers with visible vessels.")
44
Injection therapy Injection therapy is a nonthermal method of achieving hemostasis. One of a variety of solutions is injected into the base of the ulcer with a catheter that has a retractable needle (the type of catheter used for esophageal variceal sclerotherapy). Solutions documented in controlled trials to provide effective hemostasis include absolute ethanol, epinephrine (at a dilution of 1:10,000), polidocanol (a sclerosing agent usually injected immediately after the injection of epinephrine), and even normal saline. The fact that normal saline is effective suggests that at least one mechanism of hemostasis is simply local compression of the blood vessel by the injected solution.
. Solutions documented in controlled trials to provide effective hemostasis include absolute ethanol, epinephrine (at a dilution of 1:10,000), polidocanol (a sclerosing agent usually injected immediately after the injection of epinephrine), and even normal saline. The fact that normal saline is effective suggests that at least one mechanism of hemostasis is simply local compression of the blood vessel by the injected solution.")
45
Endoscopic therapy Prospective clinical studies comparing injection therapy, bipolar electrocoagulation, and heater-probe therapy suggest that the three approaches are comparable in safety and efficacy.

46
Endoscopic therapy The two major complications of endoscopic therapy, perforation and induction of uncontrollable bleeding, are rare. A compilation of data from prospective controlled trials of bipolar electrocoagulation, heater-probe therapy, and injection therapy reveals induction of bleeding requiring surgery in 0.3% and perforation in 0.5%.

47
Endoscopic therapy Endoscopic therapy is not required in most patients with bleeding ulcers, only in those with clinical evidence of substantial bleeding (hemodynamic instability with tachycardia, hypotension, or postural changes in blood pressure or pulse, a dropping hematocrit or the need for transfusions) and endoscopic evidence of active bleeding or a nonbleeding visible vessel. In ulcers with a flat spot, adherent clot, or clean base, bleeding recurs much less commonly; such ulcers are not benefited by endoscopic therapy.
 and endoscopic evidence of active bleeding or a nonbleeding visible vessel. In ulcers with a flat spot, adherent clot, or clean base, bleeding recurs much less commonly; such ulcers are not benefited by endoscopic therapy.")
48
Endoscopic therapy Just over 10 percent of patients require urgent surgery for bleeding despite endoscopic therapy.

49
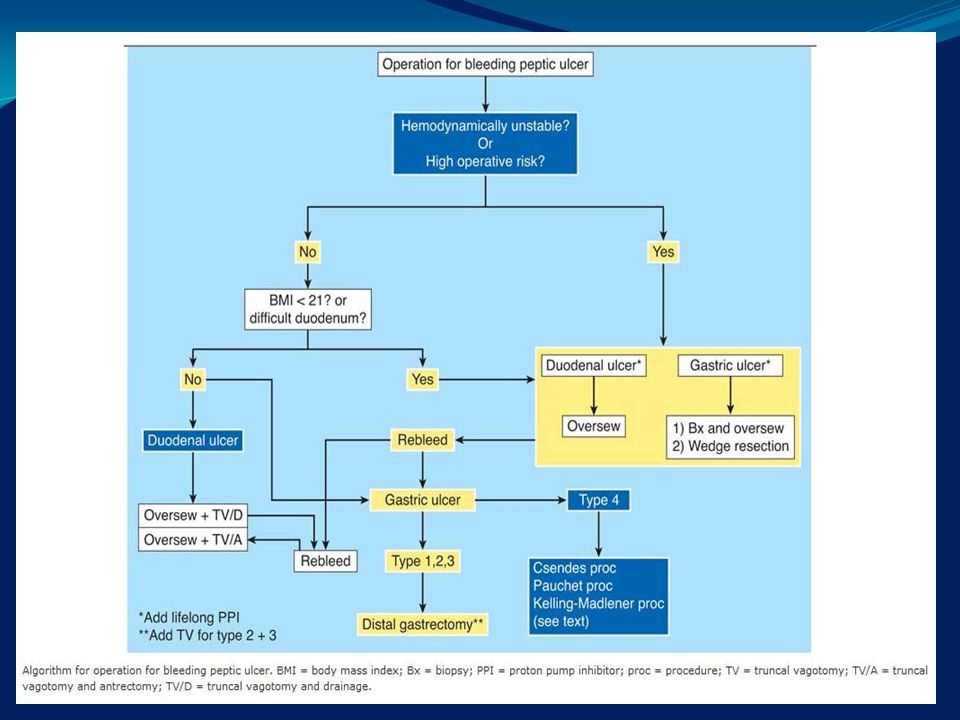
Surgical Therapy Surgery is generally performed if endoscopic therapy has failed or is unavailable. The same clinical and endoscopic criteria used to determine whether a patient requires urgent endoscopic therapy (features associated with a high risk of further bleeding and death) are used to determine whether a patient should have urgent surgery.
 are used to determine whether a patient should have urgent surgery.")
50
Surgical Therapy A prospective, randomized trial compared early surgery, which was performed on the basis of minimal criteria, such as the presence of any stigmata of hemorrhage or a history of prior bleeding, with delayed surgery, which was performed only if there was clinical evidence of severe persistent or recurrent bleeding. In the early-surgery group 4% died, In the delayed-surgery group 10 % died. All the patients who died were over 60 years of age. Thus, the more recent trial does suggest the possibility of a benefit with early surgery, primarily for patients over 60 years old.

51
SURGICAL TREATMENT: There are 2 types of operations 1. Gastrectomy: which could be total or partial, partial procedures where used using Billroth 1 or Billroth 2 techniques. 2. Vagotomy: division of the vagus nerve which stimulate acid secretion, this could be (a) truncal (b) Selective (c) highly selective. Long term complications of surgery: * Recurrent ulcer. * Dumping effect. * Diarrhea. * Blind loop syndrome. * Nutritional complications ( iron-deficiency anemia, megaloblastic anemia, osteomalacia
 truncal (b) Selective (c) highly selective. Long term complications of surgery: * Recurrent ulcer. * Dumping effect. * Diarrhea. * Blind loop syndrome. * Nutritional complications ( iron-deficiency anemia, megaloblastic anemia, osteomalacia.")
52
Vagotomies

53
PYLOROPLASTY

54
OMENTOPLASTY

55
SUTURE

56
Partial gastrerctomy

58
Angiographic Therapy Angiographic therapy is rarely used to treat patients with bleeding ulcers and should be considered only for severe, persistent bleeding if surgery poses an extremely high risk and endoscopic therapy has been unsuccessful or is unavailable. Ulcers may stop bleeding with an intraarterial infusion of vasopressin in up to 50 %. Uncontrolled studies suggest that arterial embolization with an absorbable gelatin sponge (Gelfoam), an autologous clot, tissue adhesives, or mechanical occlusion devices may control bleeding identified angiographically in approximately 75 to 80% of cases, although recurrent bleeding may occur in over half these cases. Complications of embolization include ischemia with stenosis, infarction, perforation, or abscess formation in target and nontarget organs.
, an autologous clot, tissue adhesives, or mechanical occlusion devices may control bleeding identified angiographically in approximately 75 to 80% of cases, although recurrent bleeding may occur in over half these cases. Complications of embolization include ischemia with stenosis, infarction, perforation, or abscess formation in target and nontarget organs.")
59
Prevention of Recurrent Bleeding
The first goal in preventing recurrent bleeding is successful healing of the ulcer. Bleeding and nonbleeding ulcers have similar rates of healing with standard therapy. Follow-up endoscopy may be warranted to document healing and rule out cancer in patients with bleeding from gastric ulcers. We believe that for most patients with duodenal ulcers, follow-up endoscopy to document healing is neither necessary nor cost effective. Antisecretory therapy 20 mg of omeprazole daily for six to eight weeks or longer- H2-receptor antagonist for three months. Such an approach is still far less expensive than repeated endoscopy.

60
Most patients with peptic ulcer disease have a recurrence.
Patients who have had one episode of bleeding from an ulcer may have another episode. It is therefore important to develop a long-term strategy to prevent recurrent bleeding. This is accomplished by eliminating as many risk factors for recurrence as possible for an individual patient. These risk factors, which are generally the same for gastric and duodenal ulcers, include the use of NSAIDs, infection with H. pylori, and gastric acid.

61
Medical Therapy Our approach to the long-term care of patients who have had bleeding from peptic ulcers is based on whether NSAIDs were used before the bleeding occurred and whether they must be continued. Gastric acid and H. pylori infection are the two factors that must be considered among patients who were not using NSAIDs when the bleeding occurred. Maintenance therapy with H2-receptor antagonists is widely used to prevent recurrent peptic ulceration.

62
Medical therapy It appears reasonable to attempt to eradicate H. pylori in infected patients and thereby remove an important risk factor for recurrent bleeding. This is best accomplished with combination therapy, such as a two-week course of bismuth subsalicylate (two tablets four times daily) plus metronidazole (250 mg four times daily) and tetracycline (500 mg four times daily).
 plus metronidazole (250 mg four times daily) and tetracycline (500 mg four times daily).")
63
Medical therapy Among patients who have bleeding ulcers associated with the ingestion of NSAIDs, the most important intervention is discontinuation of the drugs. If this is possible, ulcers should heal with standard therapy.

64
Medical therapy Bleeding ulcers in patients who must continue to take NSAIDs or aspirin represent a difficult management problem. Misoprostol significantly decreases the development of new gastric and duodenal ulcers in patients taking non-aspirin NSAIDs. H2-receptor antagonists, on the other hand, are effective in preventing duodenal, but not gastric, ulcers. Although the evidence is sparse, potent antisecretory therapy with proton-pump inhibitors such as omeprazole may also prevent both gastric and duodenal ulceration caused by NSAIDs.

65
Surgical Therapy Patients who have recurrences of bleeding from ulcers despite medical therapy are candidates for surgical therapy

66
Elective Surgical Therapy
Surgery is often an important part of the care of patients with the Zollinger-Ellison syndrome, although the advent of proton-pump inhibitors has changed the primary purpose of surgery from control of acid secretion to resection of tumors.

Similar presentations









>")

 682-3793; (p) 413-3222.>")







