Download presentation
Presentation is loading. Please wait.

1
WATER, WATER METABOLISM ELECTROLYTE BALANCE
Prof. Dr.Yıldız DİNÇER

2
WATER

3
Life is inconceivable without water.
Water constitutes 45%-75% of total human body weight. It is distributed in intracellular and extracellular compartments and provides a continious solvent phase between body compartments. As the biological solvent, water plays a major role in all aspects of metabolism:

4
Absorption, transport, digestion, excretion as well as maintenance of body temperature.
Water is not just the solvent in biological reactions. Water is a good nucleofile and it is very often a direct participant in reactions such as hydrolysis and condensation The unique properties of water are derived from its structure.

5
Structure of water H2O Water is a hydride of oxygen in which the highly electronegative oxygen atom attracts the bonding electrons from two hydrogen atoms. This leads to polar H-O bonds in which the hydrogen atoms have a slight positive charge and the oxygen atom has a slight negative charge.

6
Therefore a water molecule has a dipol structure

7
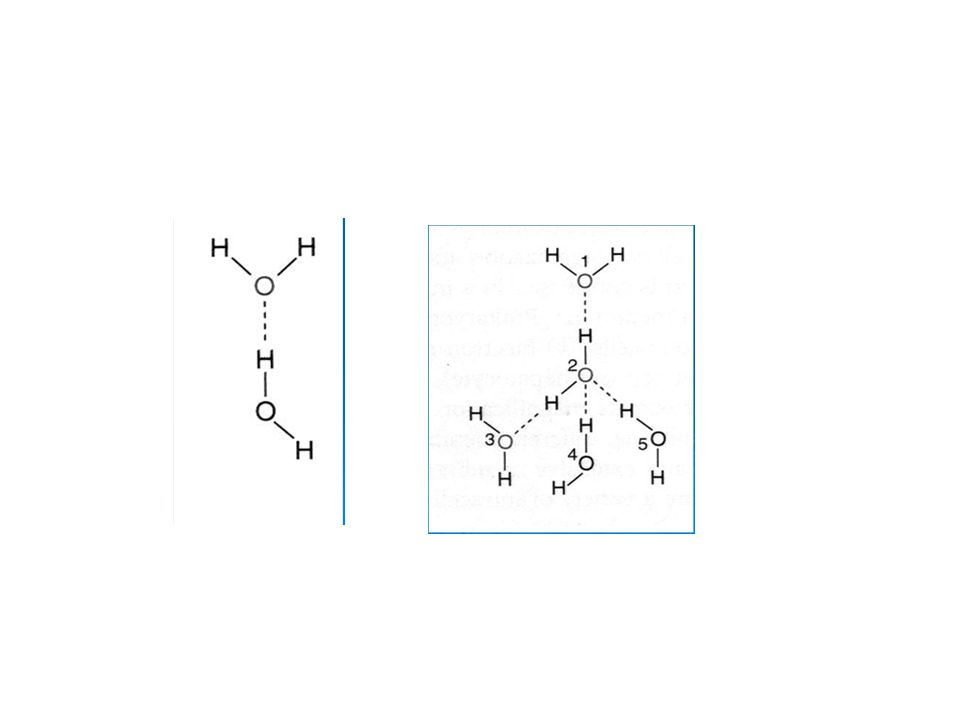
Neighboring liquid water molecules interact with one another.
The intermolecular bonding between water molecules arises from the attraction between the partial negative charge on the oxygen atom and the partial positive charge on the hydrogen atom of adjacent water molecules. This type of attraction involving a hydrogen atom is known as hydrogen bond

8
Hydrogen bonds contain a hydrogen atom between two electronegative atoms (e.g., O and N).
Hydrogen bonds are weaker than covalent bonds. However the cumulative effect of many hydrogen bonds is equivalent to the stabilizing effect of covalent bonds. In proteins, nucleic acids and water, hydrogen bonds are essential to stabilize overall structure.

10
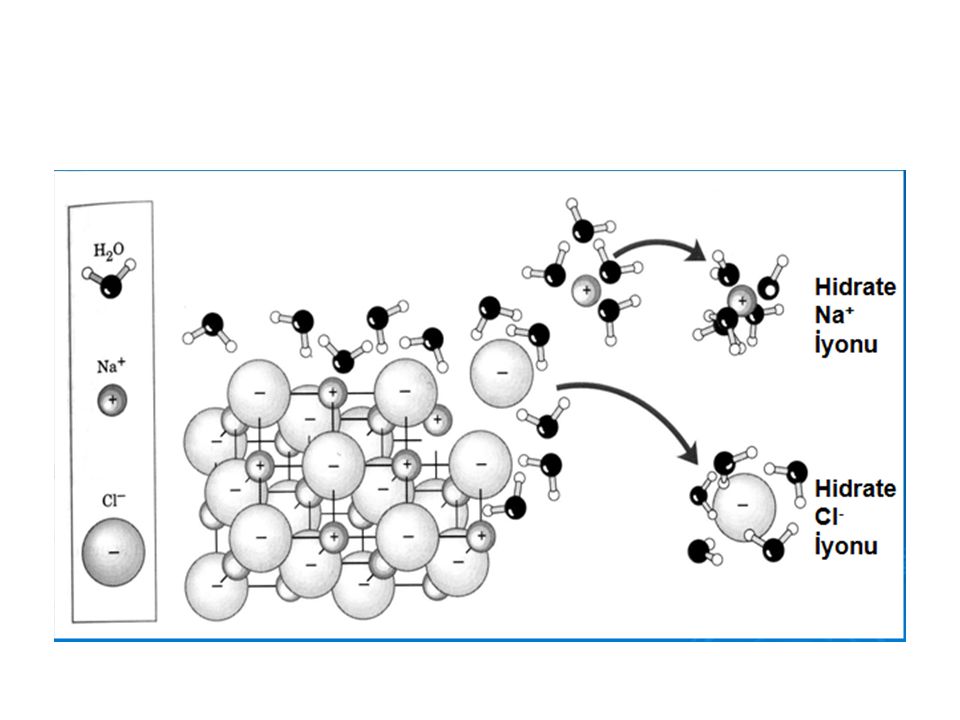
Water is an excellent solvent for both ionic compounds and low-molecular weight nonionic polar compounds such as sugars, urea and alcohols. Ionic compounds are soluble because water can overcome the electrostatic attraction between ions through solvation of the ions. Non-ionic polar compounds are soluble because water molecules can form hydrogen bonds to polar groups.

12
Amphipathic compounds
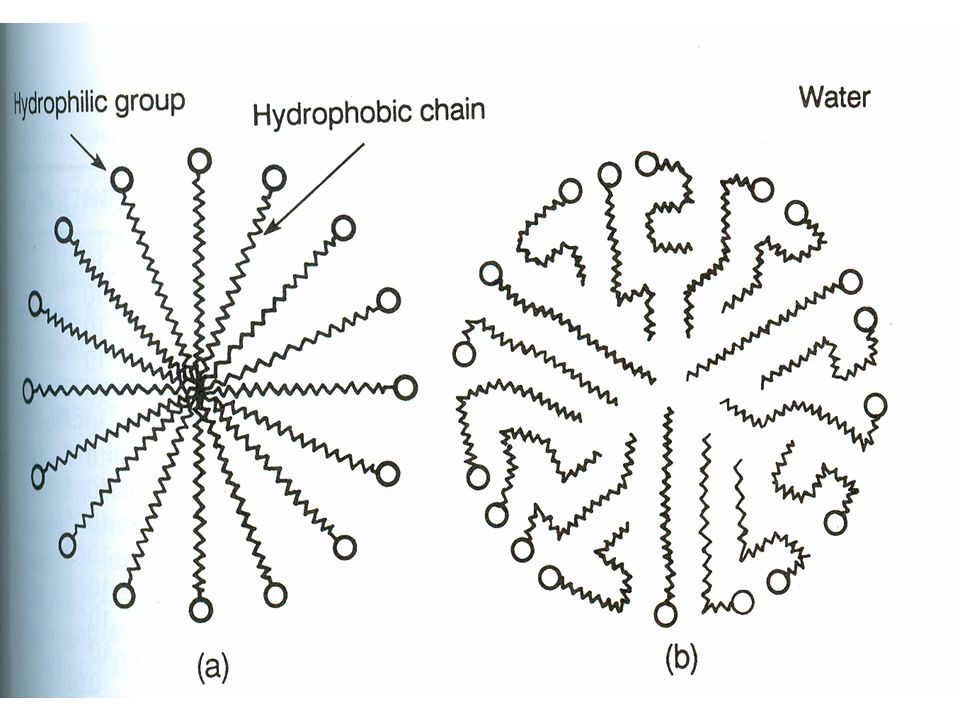
Amphipathic compounds are the molecules which contain both hydrophobic groups (large nonpolar hydrocarbon chains) and polar or ionic groups (hydrophilic groups). They don’t dissolve in water as individual molecules. When they reach at a definite concentration (critic micelle concentration) in water, they associate with each other in submicroscopic aggregations of molecules called micelles.
 and polar or ionic groups (hydrophilic groups). They don’t dissolve in water as individual molecules. When they reach at a definite concentration (critic micelle concentration) in water, they associate with each other in submicroscopic aggregations of molecules called micelles.")
13
Micelles have hydrophilic groups on their exterior (bonding with solvent water), and hydrophobic groups clustered in their interior. They occur in spherical shapes. Micelle structures are stabilized by hydrogen bonding with water, by van der Waals attractive forces between hydrocarbon groups in the interior, and by energy of hydrophobic interactions.

15
Hydrophobic interactions are also weaker than covalent bonds
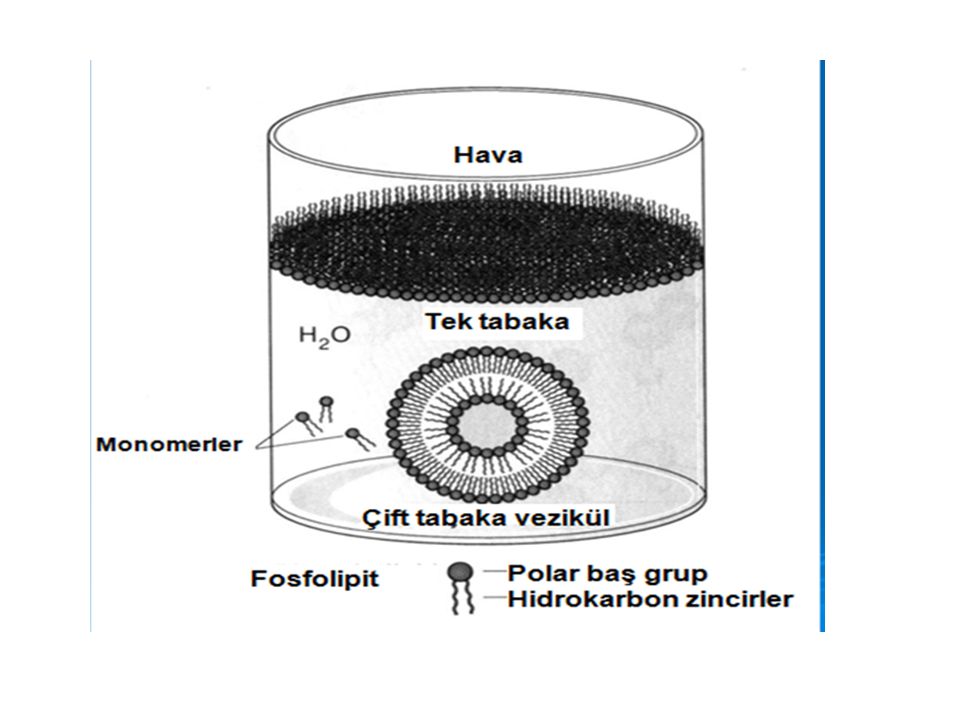
Hydrophobic interactions are also weaker than covalent bonds. However, many such interactions result in large, stable structures. When amphipathic compounds are available at a considerably higher concentration than critic micelle concentration, they form liposome vesicles after the sonication. Liposome vesicles are two-bilayer lipid spheres.

17
Liposomes have potential applications in medicine.
Drugs and some macromolecules encapsulated in liposome systems can be targeted to a particular cell population or organ

18
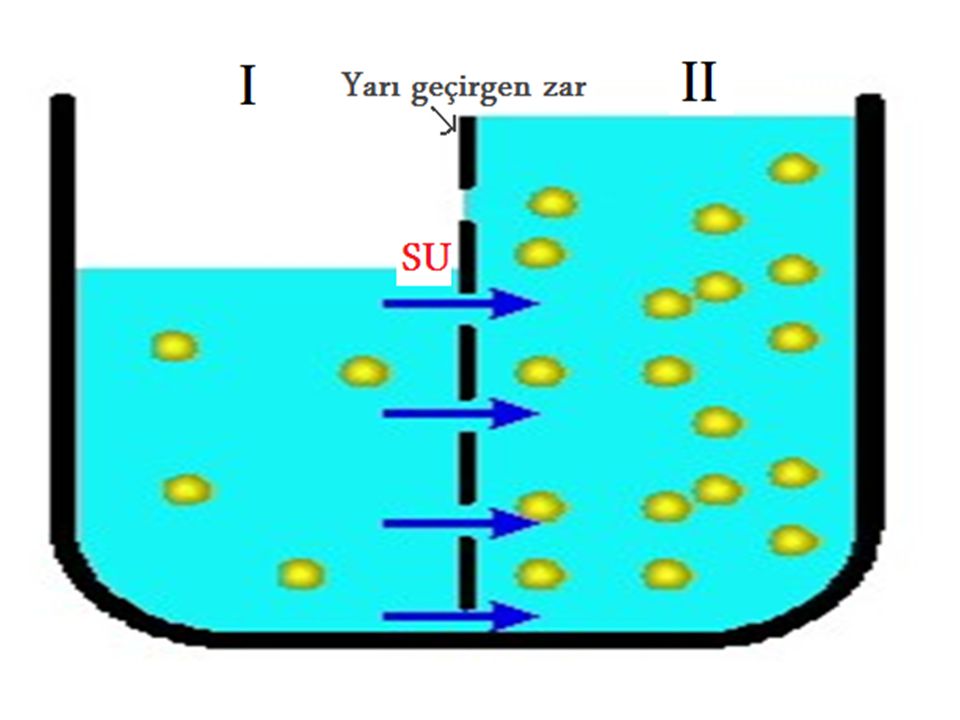
Osmotic pressure Osmotic pressure is a measure of the tendency of water molecules to migrate from a diluted solution to a concentrated solution through a semipermeable membrane. This migration of water molecules is termed osmosis. A solution containing 1 mol of solute particles in 1 kg of water is a one-osmolal solution.

19
A solution containing 1 mol of solute particles in 1 L of water is a one-osmolar solution.
When 1 mol of a solute (such as NaCl) that dissociates into two ions (Na+ and Cl-) is dissolved in 1 L of water, the solution is two osmolar.
 that dissociates into two ions (Na+ and Cl-) is dissolved in 1 L of water, the solution is two osmolar.")
21
In blood plasma, the normal total concentration of solutes is remarkably constant ( mosmolal) This constant osmolalite changes under some pathological conditions such as dehydration, renal failure, diabetes insipidus, hypo and hypernatremia, hyperglycemia.

22
WATER DISTRIBUTION IN BODY AND REGULATION OF WATER METABOLISM

23
All chemical reactions take place in aqueous medium in body, and all reactives are dissolved in body fluids. Water participates to many biochemical reactions, actively. Water plays an important role in absorption, transport, digestion, excretion and maintenance of body temperature.

24
Two thirds of total body water is distributed into the intracellular fluid (ICF) compartment, and one-third exists in the extracellular fluid (ECF) compartment. The ICF and ECF compartments are physically separated by the cellular plasma membrane. ECF may be further subdivided into two compartments:

25
1. Intravascular fluid compartment (25% of ECF)
2. Interstitial fluid compartment Transcellular fluids consists of GIS fluids, intraoccular fluid, cerebrospinal fluid and all connective tissue fluids. They are included by interstitial fluid compartment Water can easily pass through the different compartments when it is necessary.

26
% Body weight %Total body water
Extracellular fluid Vascular fluid Interstitial fluid Intracellular fluid

27
Water movement between compartments
Detainment of water in a compartment is depend on osmotic pressure which is constituted by dissolved ions and molecules in water. Osmotic pressure difference between two compartments enforces the water movement from diluted compartment to concentrated compartment, and this phenomenon is termed as osmosis.

28
Plasma osmotic pressure is mainly constituted by sodium ions dissolved in plasma and proteins.
Urea and glucose present in plasma also provide a contribution to osmotic pressure. Plasma osmotic pressure derived from plasma proteins termed as oncotic pressure.

29
Proteins are not able to pass through biological membranes because of their large molecular structure and electrical charges. Proteins have a major role for the maintenance of fluid equilibrium between vascular fluids and interstitial fluids. All solutions have the same osmolarity with plasma are determined as isotonic.

30
Another type of water movement between compartments is filtration.
Filtration is the movement of vascular fluid from vascular area to interstitial compartment against the oncotic pressure of plasma proteins. Renal glomerular filtrate is produced by this way. Arterial hydrostatic pressure leads the transition of vascular fluid and all soluted molecules (other than proteins) across the glomerular membrane.
 across the glomerular membrane.")
31
Intracellular osmotic pressure is regulated by cellular metabolism under physiological conditions.
Distribution of water between intracellular and interstitial compartments is determined by the osmotic pressure of interstitial fluid. An increase in osmolarity of interstitial fluid leads to movement of water from inside to interstitial area, a decrease in osmolarity of interstitial fluid causes water movement into cell.

32
In some tissues, cells establish an adaptive response to increased extravascular fluid osmolarity. They increase intracellular osmolarity to protection from osmotic stress. In the case of increased extravascular fluid osmolarity; Brain cells protect themselves by increasing amino acid concentrations Kidney cells protect themselves by increasing sorbitol concentration

33
Interstitial fluid which also includes lypmhatic fluid is generally in the gel form because of its proteoglycan content Proteoglycans have a high capacity of water retention because of a great number of OH groups in their structure. This is the answer why interstitial fluid does not accumulate in lower extremities because of gravity forming edema.

34
AQUAPORINS Aquaporins are integral membrane proteins which are provide transmembrane channels for rapid movement of water molecules across all plasma membranes. Ten aquaporins are known in humans. Each has a specialized role. Aquaporins are available in the nephrons (in the plasma membrane of proximal renal tubule cells and renal collecting duct), salivary glands, eye, central nervous system, lung, liver, pancreas and colon.
, salivary glands, eye, central nervous system, lung, liver, pancreas and colon.")
35
ELECTROLYT BALANCE Many compounds are carried into the cell by special carring systems because of limited permeability of cellular membranes Although their cellular and extracellular concentrations are different, these concentrations have a constant range Cellular membranes are permeable to water and hydrophobic molecules but not permeable for ions and hydrophilic neutral molecules.

36
These molecules are carried into cell by special carrier systems and pumps.
The most effective pump in the cell membranes is Na+/K+ ATPase Na+/K+ ATPase is responsible for setting and maintaining the intracellular concentrations of Na+and K+,and for generation of transmembrane electrical potential. Na+/K+ ATPase moves 3Na+out of the cell for every 2K+ moves in.

37
The electrical potential is central for electrical signaling in neurons and the gradient of Na+is used to drive uphill cotransport of various solutes such as glucose, amino acids in a variety of cell types.

38
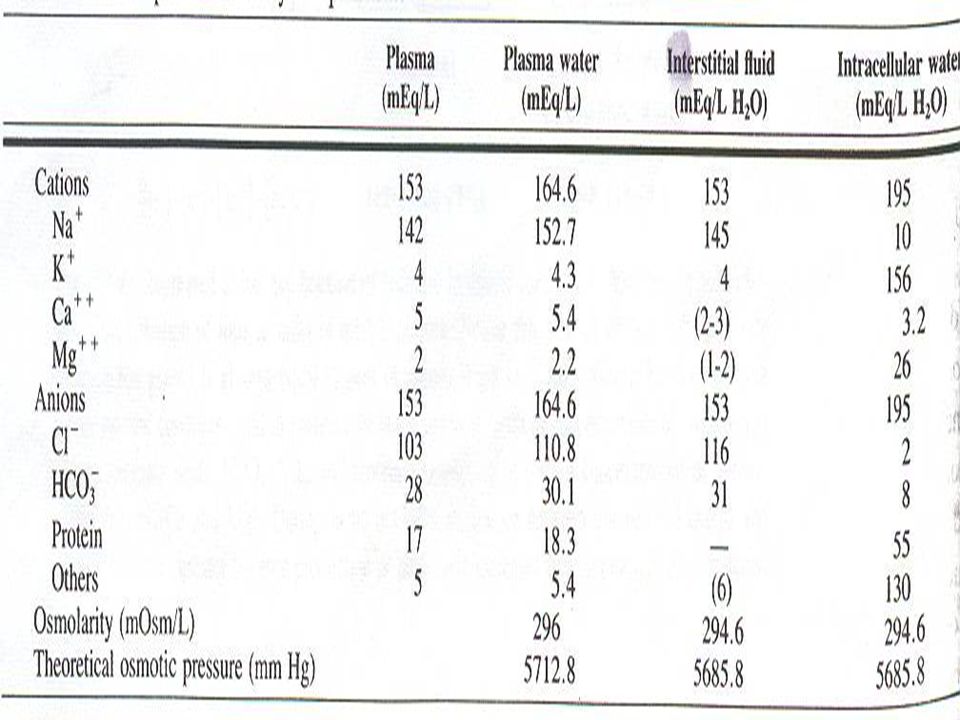
Major cations of the intracellular medium:
K+and Mg++ Major anions of the intracellular medium: Organic acids,proteins, HCO3- and Cl- Major cations of the plasma: Na+, Ca++, Mg++,K+ Major anions of the plasma: Cl- and HCO3-

40
The sum of all the (+) charges must be equal to the sum of all the (-) charges to maintain electrical neutrality in the plasma Most often, plasma concentrations only of Na+,K+,Cl- ve HCO3- are measured in clinical laboratories. The sum of these measured cations exceeds that of the measured anions. Therefore sum of unmeasured plasma anions must be greater than that of the unmeasured cations.

41
The difference between the sum of unmeasured cations and unmeasured anions is known as the anion gap and is calculated as Anion gap = Na+ + K+ Cl- HCO3- Anion gap is constant as 124 mEq/L under phsiological conditions. It increases some pathological conditions such as lactic acidosis, and renal failure.

42
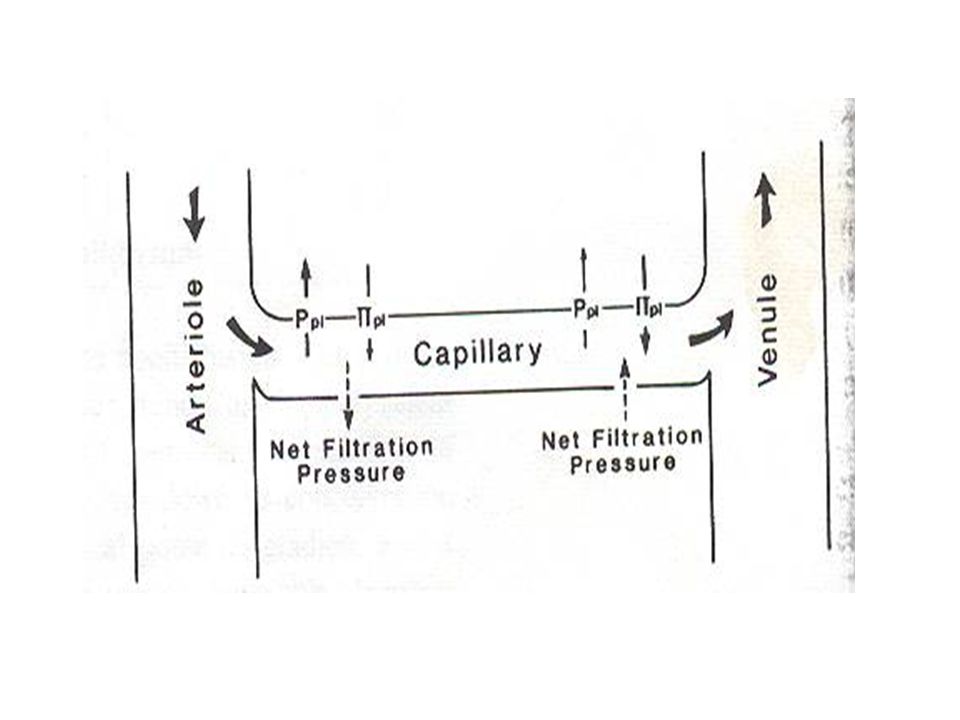
Movement of extracellular water between intravascular and interstitial areas
The movement of extracellular water between intravascular and interstitial areas is regulated by osmotic, hydrostatic and electrostatic forces İntravascular fluid is isolated from extracellular fluid by capillary wall that is permeable to water and ions but not permeable to proteins The major filtration force is plasma hydrostatic pressure in the capillary

43
The major reabsorption force is the osmotic pressure exerted across the capillary endothelium by plasma proteins Plasma hydrostatic pressure tends to drive water out of the capillary, colloid osmotic pressure tends to drive water into capillary Plasma hydrostatic pressure exceeds plasma colloid osmotic pressure at he arteriolar end of the capillary so that net filtration occurs.

44
As plasma moves along the capillary and filtration occurs, plasma hydrostatic pressure decreases and protein concentration increases along the course of capillary so that net reabsorption occurs toward the venous end of the capillary Overall filtration exceeds the reabsorption Therefore water must be returned to the plasma from interstitital area by the way of lymphatic system to prevent edema

46
WATER BALANCE IN THE BODY
Extracellular water osmolarity is maintained constant at mOsm/L as a consequence of the dynamic balance between water intake and water excretion. Under normal conditions approximately one half to two thirds of water intake is in the form of oral fluid intake, and approximately one half to two thirds of water intake is in the form of oral intake of water in food. A small amount of water is produced by oxidative metabolism ( ml/day)
")
47
Water is excreted by urine, sweating, respiration and gastrointestinal water loss
Average daily water turnover in the adult approximately is 2,5 L, but the range of water turnover is great and depends on intake, environment and physical activity Volume and composition of the body fluids are regulated by neuro-hormonal system Hypothalamus, kidneys, antidiuretic hormone (ADH), renin-angiotensin-aldosterone system and natriuretic factors take place in this regulation
, renin-angiotensin-aldosterone system and natriuretic factors take place in this regulation.")
48
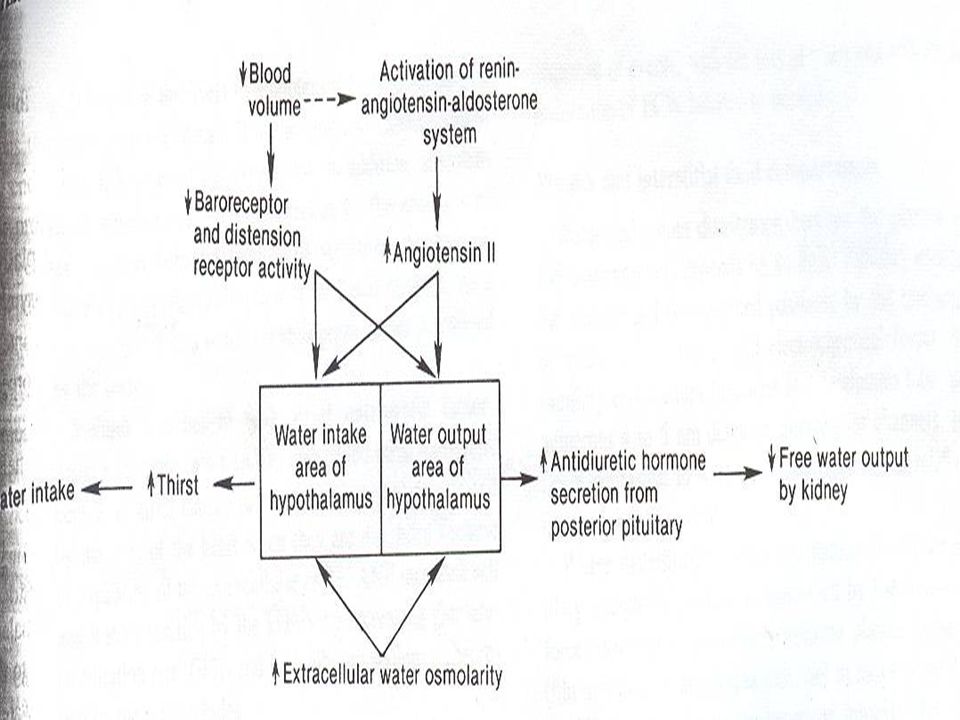
Hypothalamus and ADH The regulatory centers for water intake and water output are located in separate areas of the hypothalamus. Neurons in each of these areas respond to increases in extracellular water osmolarity, to decreases in intravascular volume, and to angiotensin II. Increased extracellular water osmolarity stimulates the neurons directly by causing them to shrink

49
A decrease in intravascular volume causes a reduction in activity of distension receptors located in the atria of the heart, the inferior vena cava, and the pulmonary veins and a reduction in activity of blood pressure receptors in the aorta and the carotid arteries. Relay of this information to the central nervous system stimulates neurons in the water-intake and water-output areas of the hypothalamus.

50
Stimulation of neurons located in the water-intake area produces a sensation of thirst and thereby stimulates water intake. Stimulation of neurons located in the water-output area results in the release of ADH from the posterior pituitary gland. ADH stimulates water reabsorption in the collecting ducts of the kidney which results the formation of hypertonic urine and decreased output of water. The integration of those mechanisms ensures maintenance of appropriate water balance.

52
Renin-angiotensin-aldosterone system (RAA)
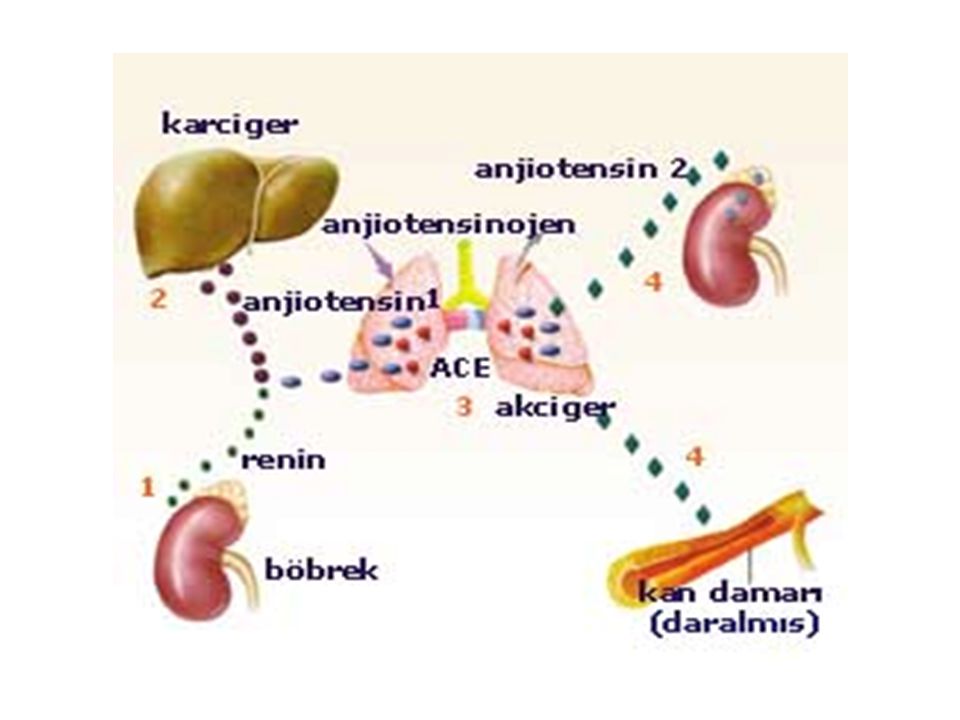
RAA system functions as a neurohormonal regulating mechanism for body sodium and water content, arterial blood pressure, and potassium balance. Renin is a proteolytic enzyme synthesized, stored and secreted by cells in the juxtaglomerular bodies of kidney.

53
Renin secretion is increased by decreased renal perfusion pressure, stimulation of sympathetic nerves to the kidneys and decreased sodium concentration in the fluid of the distal tubule. Renin converts angiotensinogen, a polypeptide synthesized in liver, to angiotensin I. Angiotensin I is converted to angiotensin II in the lung and kidney by the angiotensin converting enzyme.

54
Angiotensin II is a potent vasoconstructor
Angiotensin II is a potent vasoconstructor. In addition, it stimulates aldosterone secretion by the adrenal cortex, thirsty behavior and ADH secretion. Aldosterone stimulates sodium reabsorption in the distal nephron. As a consequence of this sodium reabsorption, water is retained by the body.

56
Natriuretic factors They contribute the maintenance of sodium balance in body. The best known is atrial natriuretic factor (ANF) which is a peptide released by the atria of the heart when they are distended because of expansion of the extracellular space ANF increases salt and water excretion by the kidney by increasing glomerulary filtration rate and by inhibiting sodium reabsorbsion by RAA system
 which is a peptide released by the atria of the heart when they are distended because of expansion of the extracellular space. ANF increases salt and water excretion by the kidney by increasing glomerulary filtration rate and by inhibiting sodium reabsorbsion by RAA system.")
57
The action of ANF is moderate under phsiological conditions but it is more effective under some pathological conditions such as congestive heart failure.

58
DISORDERS OF WATER METABOLISM
Disorders in water metabolism generally derived from imbalance between water intake and water output Disorders in water metabolism appear as dehydration and edema rather than overhydration. Na+ retention or excretion along with water is also important in the homeostasis of water.

59
Dehydration Deficient of water (Simple dehydration):
It is defined as a decrease in total body water with relatively normal total body sodium It may result from failure to replace obligatory water losses or failure of the regulatory of effector mechanisms that promote conservation of water by the kidney

60
Simple dehydration is defined with hypernatremia and hyperosmolarity
Simple dehydration is defined with hypernatremia and hyperosmolarity. Because water balance is negative, sodium balance is normal Deficient water and sodium: More often dehydration results from a negative balance of both water and sodium. In this case;

61
a) water balance may be more negative than sodium balance (hypernatremic and hyperosmolar dehydration) b) water balance may be equal to sodium balance (normonatremic and isomolar dehydration) c) water balance may be more positive than sodium balance (hyponatremic and hypoosmolar dehydration)
 water balance may be equal to sodium balance (normonatremic and isomolar dehydration) c) water balance may be more positive than sodium balance (hyponatremic and hypoosmolar dehydration)")
62
Causes of dehydration Hypernatremic dehydration
Water and food deprivation Excessive sweating (if water intake is inadequate) Osmotic diuresis (with glucosuria) Diuretic therapy(if water intake is inadequate)
 Osmotic diuresis (with glucosuria) Diuretic therapy(if water intake is inadequate)")
63
Normonatremic dehydration
Vomiting, diarrhea Replacement of losses in the above conditions with low-sodium liquids Hyponatremic dehydration Diuretic therapy (if water intake is excessive) Excessive sweating Salt wasting renal diseases Adrenocortical insufficiency
 Excessive sweating. Salt wasting renal diseases. Adrenocortical insufficiency.")
64
EDEMA Plasma fluid across the vascular area as a result of increased hydrostatitic pressure, increased capillary permeability or decreased oncotic pressure. This plasma fluid can accumulate in the interstitial area and form edema in the case of decreased lymphatic drainage derived by a pathological circumstance.

65
Edema appears in the; Acute inflammation
Venous and/or lymphatic obstructions Renal failure Heart failure Liver failure It may be local or systemic

66
Overhydration Excessive water: Water intoxication is defined as an increase in total body water with normal total body sodium, It rarely results from excessive water consumption. More often water intoxication results from impaired renal free water excretion as a result of inappropriate ADH secretion that required to maintain normal ECW osmolarity Hyponatremia appears

67
Excessive water and sodium: Expansion of the EC compartment usually results from sodium and water retension. This occurs with oliguric renal failure, nephrotic syndrome, congestive heart failure, cirrhosis and primary hyperaldosteronism In these conditions total body water excess is associated with normal or low serum sodium and osmolarity Hypernatremia is rare with water excess

68
ACID-BASE BALANCE AND BUFFERING SYSTEMS

69
pH is the (-) logarithm of [H+]
pOH is the (-) logarithm of [OH-] Keq=1.8x10-16 for water (a result of measurement of conductivity of water) [H+]=[OH-]=10-7M, pH=7 and pH+pOH=14 (calculated)
![pH is the (-) logarithm of [H+]](http://slideplayer.com/slide/4572195/15/images/69/pH+is+the+%28-%29+logarithm+of+%5BH%2B%5D.jpg "pOH is the (-) logarithm of [OH-] Keq=1.8x10-16 for water (a result of measurement of conductivity of water) [H+]=[OH-]=10-7M, pH=7 and pH+pOH=14 (calculated)")
70
A solution has a lower pH value than 7 is a acid.
Acids are [H+] donors. A solution has a higher pH value than 7 is a base. Bases are [H+] acceptors. HCl and H2SO4 are strong acids acids and are complately ionized in aqueous solutions. HCl H+ + Cl-

71
NaOH and KOH are strong bases and are also complately ionized.
Some acids such as acetic acid, lactic acid, carbonic acids are partly ionized and termed as weak acids. HA H+ + A- Acids and bases in living organisms are weak acids, other than gastric acid.

72
pH for strong acids is equal to -log H+.
However pH for weak acids is can be calculated by Henderson-Hasselbach equation. Equilibrium constant of a weak acid can be shown as below: [H+] [A-] Ka= [HA]

73
Ka [HA] [H+] = [A-] -log [H+] = -log Ka - log[HA] + log[A-] If -log [H+] is replaced with pH, and -log Ka is replaced with pKa Henderson-Hasselbach equation is found:
![Ka [HA] [H+] = [A-] -log [H+] = -log Ka - log[HA] + log[A-]](http://slideplayer.com/slide/4572195/15/images/73/Ka+%5BHA%5D+%5BH%2B%5D+%3D+%EF%82%BE%EF%82%BE%EF%82%BE%EF%82%BE%EF%82%BE%EF%82%BE%EF%82%BE%EF%82%BE+%5BA-%5D+-log+%5BH%2B%5D+%3D+-log+Ka+-+log%5BHA%5D+%2B+log%5BA-%5D.jpg "If -log [H+] is replaced with pH, and -log Ka is replaced with pKa Henderson-Hasselbach equation is found:")
74
A- pH= pKa+ log HA A- is conjugate base of weak acid.

75
Buffering Systems Buffers are aqueous systems that tend to resist changes in pH when small amounts of strong acid [H+] or strong base [OH-] are added. A buffer system consists of a weak acid (the proton donor) and its conjugate base (the proton acceptor). A mixture of equal concentrations of acetic acid and acetate ion is a buffer system.
 and its conjugate base (the proton acceptor). A mixture of equal concentrations of acetic acid and acetate ion is a buffer system.")
76
When a strong acid (HCl) is added:
CH3COO- + HCl CH3COOH + Cl- When a strong base (NaOH) is added: CH3COOH +NaOH CH3COO- +H2O + Na+ Buffering mechanism for weak base and its conjugate acid is also same.
 is added: CH3COOH +NaOH CH3COO- +H2O + Na+ Buffering mechanism for weak base and its conjugate acid is also same.")
77
pH of the buffers is calculated by the equation of Henderson-Hasselbach.
Conjugate base pH= pKa+ log Weak acid When the conjugate base and weak acid at equal concentrations, the buffer has the maximum buffering capacity and pH= pKa.

78
Buffering has the most effectivity at the point of
Conjugate base / weak acid= 0,1 – 10.0 A buffer system is maximally effective at a pH close to its pKa.

79
ACID-BASE BALANCE The end-products of the catabolism of carbonhydrates, lipids and proteins are generally acidic molecules in living organisms. In metabolic reactions, mEq acid (organic acids, inorganic acids and CO2) is produced per day. H+ is a direct participant for many reactions, and enzymes and many molecules contain ionizable groups with characteristic pKa values.
 is produced per day. H+ is a direct participant for many reactions, and enzymes and many molecules contain ionizable groups with characteristic pKa values.")
80
An increase of H+ concentration can easily alter the charges and functions of proteins, enzymes, nucleic acids, some hormones and membranes. Normal blood pH is 7,35-7,45. Values below 6,8 or above 7,70 are seldom compatible with life. In living organisms, pH of the body fluids are tightly regulated by biological buffers and some organs (lungs and kidneys).
.")
81
Biological Buffering Systems
1. Bicarbonate/carbonic acid buffer system 2. Protein buffer system 3. Hemoglobin buffer system 4. Phosphate buffer system

82
Bicarbonate/carbonic acid buffer system
The most important buffer of the plasma is the bicarbonate/carbonic acid buffer system The ratio of base to acid (HCO3-/H2CO3) is nearly 20/1 in plasma under physiological conditions This buffer system is more complex than others, because carbonic acid (H2CO3) is formed from dissolved CO2 which produced in tissues and diffused to plasma).
 is nearly 20/1 in plasma under physiological conditions. This buffer system is more complex than others, because carbonic acid (H2CO3) is formed from dissolved CO2 which produced in tissues and diffused to plasma).")
83
CO2 + H2O H2CO HCO3- + H+ This reaction is slow in plasma but in erythrocytes, carbonic anhydrase increases the rate of this reaction. HCO3-/H2CO3 = 20/1 when plasma pH=7,4 When hydrogen ion concentration increases in plasma, HCO3- ions bind H+ forming H2CO3. H2CO3 is converted to CO2 + H2O CO2 is released to atmosphere by lungs

84
Protein buffer system In proteins, ionizable R groups (COOH groups of aspartate and glutamate, NH2 groups of lysine, arginine and histidine) and N-terminale -NH2 groups of some amino acids are responsible for buffering. Proteins, especially albumin, account for the %95 of the non-bicarbonate buffer value of the plasma. Buffering effect of proteins is low in plasma Proteins are much more effective buffers in intracellular medium.
 and N-terminale -NH2 groups of some amino acids are responsible for buffering. Proteins, especially albumin, account for the %95 of the non-bicarbonate buffer value of the plasma. Buffering effect of proteins is low in plasma. Proteins are much more effective buffers in intracellular medium.")
85
The most important buffer groups of proteins in the physiological pH range are the imidazole groups of histidine which has a pKa value of 6.5 Each albumin molecule contains 16 histidines

86
Hemoglobin buffer system
Hemoglobin (Hb) is a protein which carries O2 to tissues and CO2 from tissues to lungs and is an effective buffer. The most important buffer groups of Hb are histidines. Each globin chain contains 9 histidine. %95 of CO2which is released from tissues to plasma is diffused into erythrocytes.
 is a protein which carries O2 to tissues and CO2 from tissues to lungs and is an effective buffer. The most important buffer groups of Hb are histidines. Each globin chain contains 9 histidine. %95 of CO2which is released from tissues to plasma is diffused into erythrocytes.")
87
In erythrocytes, carbonic anhydrase constitutes H2CO3 from CO2 and H2O and then HCO3- and H+ are released by the ionization of H2CO3. Carbonic anhydrase CO2 + H2O H2CO HCO3- + H+ Released protons take part in the formation of salt bridges between globin chains of Hb, and lead the change in the conformation of Hb molecule in tissue capillaries.

88
The binding of proton and CO2 is conversly related to binding of oxygen.
In tissue capillaries proton and CO2 binding decreases the oxygen binding capacity of Hb so that oxygen is released by Hb. This effect of pH and CO2 concentration on the binding and release of oxygen by Hb is called the Bohr Effect. Because of the accumulation of HCO3- formed by ionization of H2CO3 within erythrocytes, there is a concentration gradient for HCO3- between plasma and erythrocytes.

89
In that case, HCO3- ions rapidly move from erythrocytes to plasma, and Cl- ions move from plasma to erythrocytes to provide electrochemical balance. This shift of Cl- is referred to as the chloride shift. All those phenomenons occur in capillaries of peripheral erythrocytes conversely change in capillaries of lungs.

90
When Hb reaches the lungs, the high oxygen concentration promotes binding of oxygen and release of protons from broken salt bridges.Protons associate with HCO3- and H2CO3 forms. H2O and CO2 form by the reaction catalyzed by carbonic anhydrase Carbonic anhydrase H2CO CO2 + H2O This phenomenon is referred as Haldane Effect. H2O and CO2 are excreted to atmosphere by respiration.

91
Phosphate buffer system
Phosphate buffer system is most effective in intracellular medium, especially in kidneys. Phosphoric acid has 3 ionization steps: H3PO H2PO H pK1= 1.9 H2PO HPO H pK2= 6.8 HPO PO H pK3= 12.4

92
Among the 3 ionization steps, H2PO4-/ HPO42- is a good buffer because of its pKa value (6,8) which is close to physiological pH (7,4). HPO42- / H2PO4- = 4 at the pH (7,4). Phosphate buffer system is not effective in plasma, because phosphate ion concentrations are low. However it is important in the excretion of acids in the urine.
. Phosphate buffer system is not effective in plasma, because phosphate ion concentrations are low. However it is important in the excretion of acids in the urine.")
93
H+ secrected into the tubular lumen by the Na+–K+ exchanger react with HPO42- to form H2PO4-.
Some organic phosphates (2,3 diphosphoglycerate in erythrocytes) has also buffering capacity.
 has also buffering capacity.")
94
REGULATION OF ACID-BASE BALANCE
Lungs and kidneys have an important role for regulation of acid-base balance. Lungs: Lungs provide O2/CO2 exchange between blood and atmosphere. O2 and CO2 are transported between lungs and peripheral tissues by Hb within erythrocytes. CO2 carried with either carbaminoHb form or H+ form in the salt bridges between globin chains is excreted by respiration.

95
Respiratory center senses and responds to the pH of blood and the source of pulmonary control. Both O2 and CO2 partial pressures influence the center. A decrease in pH results in an increased respiratory rate and deeper breathing. A decrease in respiratory rate leads to accumulation of CO2 and decrease in pH. Pulmonary response is rapid (max. at 3-6 h) while renal compensation is relatively slower.
 while renal compensation is relatively slower.")
96
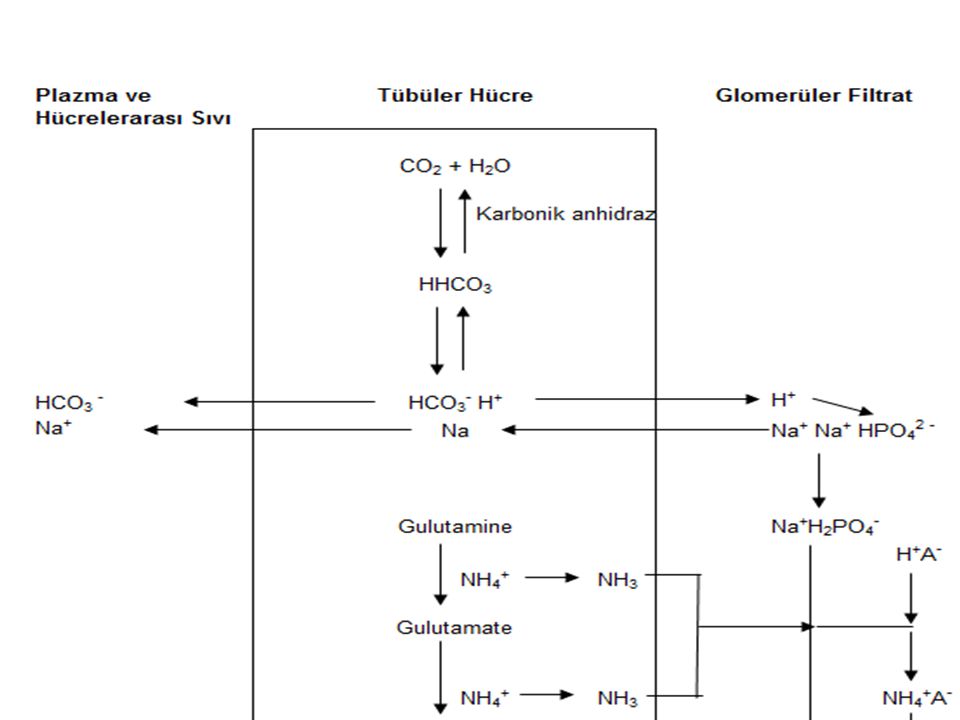
Kidneys: The kidneys secrete protons through 3 mechanisms: 1. Reabsorbsion of HCO3- 2. Na+/H+ exchange 3. Production of ammonia and excretion of NH4+

97
1. Reabsorbsion of HCO3- The proximal tubule is responsible for reabsorbsion of HCO3- filtered through glomeruli. In tubuler cells CO2 reacts with H2O to form H2CO3 HCO3- derived from dissociation of H2CO3 is reabsorbed to plasma

98
2. Na+/H+ exchange H+ secreted into the tubules in exchange for Na+ from the tubular fluid by Na+/H+-ATPase combines with HCO3- to form CO2 and water. The CO2 diffuses into the tubular cells where it is rehydrated to H2CO3 by carbonic anhdydrase. H2CO3 dissociates to HCO3- and H+.The HCO3- is reabsorbed and diffuses into the blood stream.

99
K+ ions compete with H+ for Na+/H+ exchange
K+ ions compete with H+ for Na+/H+ exchange. When K+ ions excretion increase in urine, excretion of H+ ions decreases. Na+/H+ exchange may also be coupled to formation of H2PO4- from HPO42- in the lumen.

100
3. Production of ammonia and excretion of NH4+
Glutaminase Glutamine + H Glutamate- + NH3 Glutamate dehidrogenase Glutamate- + NAD α-ketoglutarate+ NADH + H+ + NH3

101
NH3 is a toxic gase and readily diffuses to tubular lumen, combines with H+ to form NH4+. NH4+ is excreted by urine as NH4+ salts. Renal compensation is low (5-7 days).
.")
103
DISORDERS OF ACID-BASE BALANCE
These disorders are classified according to their cause: 1. Metabolic acidosis 2. Respiratory acidosis 3. Metabolic alkalosis 4. Respiratory alkalosis pH is lower than 7.37 in acidosis, higher than 7.44 in alkalosis.

104
1. Metabolic acidosis It is detected by decreased plasma bicarbonate. Causes: 1. Production of organic acid that exceeds the rate of elimination (e.g.,lactic acid acidosis) 2. Reduced excretion of acids resulting an accumulation of acid that consumes bicarbonate (e.g., renal failure, some renal tubular acidosis) 3.Excessive loss of bicarbonate due to increased renal excretion or excessive loss of duodenal fluid
 2. Reduced excretion of acids resulting an accumulation of acid that consumes bicarbonate (e.g., renal failure, some renal tubular acidosis) 3.Excessive loss of bicarbonate due to increased renal excretion or excessive loss of duodenal fluid.")
105
Total anions in plasma must equal total cations
Anion gap:It is unmeasured anions (phosphate, sulfate, proteins) in plasma and it is calculated as the difference between measured cations and measured anions. Anion gap= Na+ + K+ Cl- HCO3- It is equal 124 mEq/L under physiological conditions. Anion gap is generally high in metabolic acidosis.
 in plasma and it is calculated as the difference between measured cations and measured anions. Anion gap= Na+ + K+ Cl- HCO3- It is equal 124 mEq/L under physiological conditions. Anion gap is generally high in metabolic acidosis.")
106
Causes of metabolic acidosis
Renal failure Renal tubular acidosis Diabetic ketoacidosis Lactic acidosis Hypoxia Increased acid intake Hyperthyroidism Hyperparathyroidism Carbonic anhydrase inhibitors Salicylate overdose

107
Respiratory and renal compensations occur in metabolic acidoses.

108
2. Respiratory acidosis Respiratory acidosis is characterized by accumulation of CO2, rise in pCO2, decreases in bicarbonate concentration and pH. It may result from central depression of respiration or from pulmonary disease Plasma K+ concentration may increase because of its competition with H+ for Na+/H+ exchange.

109
Plasma Cl- concentration may decrease because of chloride shift (Cl- also accompanies the renal excretion of NH4+). Urine is much more acidic than usual. Acute respiratory acidosis is compensated by kidneys. However renal compensation is not enough in the case of chronic respiratory acidosis. The primary goal of treatment is to remove the cause of the distributed ventilation.

110
Causes of respiratory acidosis
Narcotic or barbiturate overdose Trauma Infection Cerebrovascular accident Asthma, obstructive lung diseases

111
3. Metabolic alkalosis Metabolic alkalosis is characterized by elevated plasma bicarbonate level. It may result from administration of excessive amount of alkali or vomiting which causes loss of H+ and Cl-. Plasma level of bicarbonate is high, K+ and Cl- are low, urine is much more alkaline than usual.

112
When pH> 7.55 many of anions bind the Ca2+ ions so that ionized Ca2+ concentration decreases in plasma. This leads the cramps and convulsions. Metabolic alkalosis is compensated by lungs and kidneys. Respiratory rate is decreased by lungs as a result of depression of respiratory center by high pH, therefore CO2 is kept . Renal compensation involves decreased reabsorbtion of bicarbonate, Na+/H+ exchange and NH4+ formation which lead formation of alkaline urine.

113
Causes of metabolic alkalosis
Loss of hidrogen ions from GIS K+ deficiency Hyperaldosteronism Cushing syndrome Antiacids, diüretics, corticosteroids

114
4. Respiratory alkalosis
Respiratory alkalosis occurs when the respiratory rate increases abnormally and leads to decrease in PCO2 and rise in blood pH. Hyperventilation occurs in hysteria, pulmonary irritation and head injury with damage to respiratory center. The increase in blood pH is buffered by plasma bicarbonate buffer system. Renal compensation seldom occurs because this type of alkalosis is usually transitory.

115
The increase in blood pH is buffered by plasma bicarbonate buffer system.

Similar presentations










 Newborn (77%) Adult male (60%) Adult female (54%) Elderly (45%) Adipose.>")

![1. pH = - log [H + ] H + is really a proton Range is from 0 - 14 If [H + ] is high, the solution is acidic; pH < 7 If [H + ] is low, the solution.](/15/4651316/big_thumb.jpg "1. pH = - log [H + ] H + is really a proton Range is from 0 - 14 If [H + ] is high, the solution is acidic; pH < 7 If [H + ] is low, the solution.>")






