Download presentation
Presentation is loading. Please wait.

1
Bronchiectasis Hassan Ghobadi MD. Assistant professor of Internal Medicine Ardabil University of Medical sciences

2
CONTENTS Definition Pathology Etiology Pathogenesis Clinical manifestations Diagnosis Treatment

3
BRONCHIECTASIS Definition : Abnormal and permanent dilation of bronchi. It may be focal or diffuse distribution

4
Pathology The bronchial dilatation of bronchiectasis is associated with destructive and inflammatory changes in the walls of airways. The normal structural components of the wall, including cartilage, muscle, and elastic tissue, are destroyed and may be replaced by fibrous tissue. The dilated airways frequently contain pools of thick, purulent material, while more peripheral airways are often occluded by secretions or obliterated and replaced by fibrous tissue.

5
Pathology Three different patterns of bronchiectasis have been described. 1- Cylindrical bronchiectasis, 2- Varicose bronchiectasis, 3- Saccular (cystic) bronchiectasis,
 bronchiectasis,.")
7
ETIOLOGY : IMPAIRED HOST DEFENCE Local causes: Endobronchial obstruction Generalized impairment: 1. Immunoglobulin deficiency 2. Primary ciliary disorders (PCD) 3. Cystic fibrosis
 3. Cystic fibrosis.")
8
Etiology: A. Impaired host defense Impaired host defense mechanisms are often involved in the predisposition to recurrent infections. Generalized impairment of pulmonary defense mechanisms occurs with immunoglobulin deficiency, primary ciliary disorders, or cystic fibrosis (CF). primary ciliary dyskinesia, are responsible for 5–10% of cases of bronchiectasis. Primary ciliary dyskinesia is inherited in an autosomal recessive fashion. In CF impaired bacterial clearance, resulting in colonization and infection with particularly P. aeruginosa & S. aureus, H. influenzae, Escherichia coli, and Burkholderia cepacia.
. primary ciliary dyskinesia, are responsible for 5–10% of cases of bronchiectasis. Primary ciliary dyskinesia is inherited in an autosomal recessive fashion. In CF impaired bacterial clearance, resulting in colonization and infection with particularly P. aeruginosa & S. aureus, H. influenzae, Escherichia coli, and Burkholderia cepacia..")
9
Etiology: B. Infections Causes Adeno & Influenza virus Measles and Pertussis Atypical mycobacteria Bacterial infection with virulent organisms: S.aureus, Klebsiella Anaerobes Bordetella pertussis Mycoplasma HIV Tuberculosis Fungi Mycobacterium avium complex

10
Etiology: C. Noninfectious Causes Exposure to a toxic substance An immune response in the airway (ABPA), Inflammatory diseases: ulcerative colitis, rheumatoid arthritis, Sjögren syndrome. Alpha 1- antitrypsin deficiency, Yellow nail syndrome,
, Inflammatory diseases: ulcerative colitis, rheumatoid arthritis, Sjögren syndrome. Alpha 1- antitrypsin deficiency, Yellow nail syndrome,.")
11
Bronchiectasis: Clinical Manifestation Cough (90 %) Daily sputum production (76%) Dyspnea (72%) Hemoptysis (56%) Recurrent pleurisy
 Daily sputum production (76%) Dyspnea (72%) Hemoptysis (56%) Recurrent pleurisy")
12
PHYSICAL EXAMINATION Any combination of, rhonchi, crepitus or wheezes Clubbing of digits, Chronic hypoxemia cor pulmonale Rt. heart failure Amiloidosis (rare)
.")
13
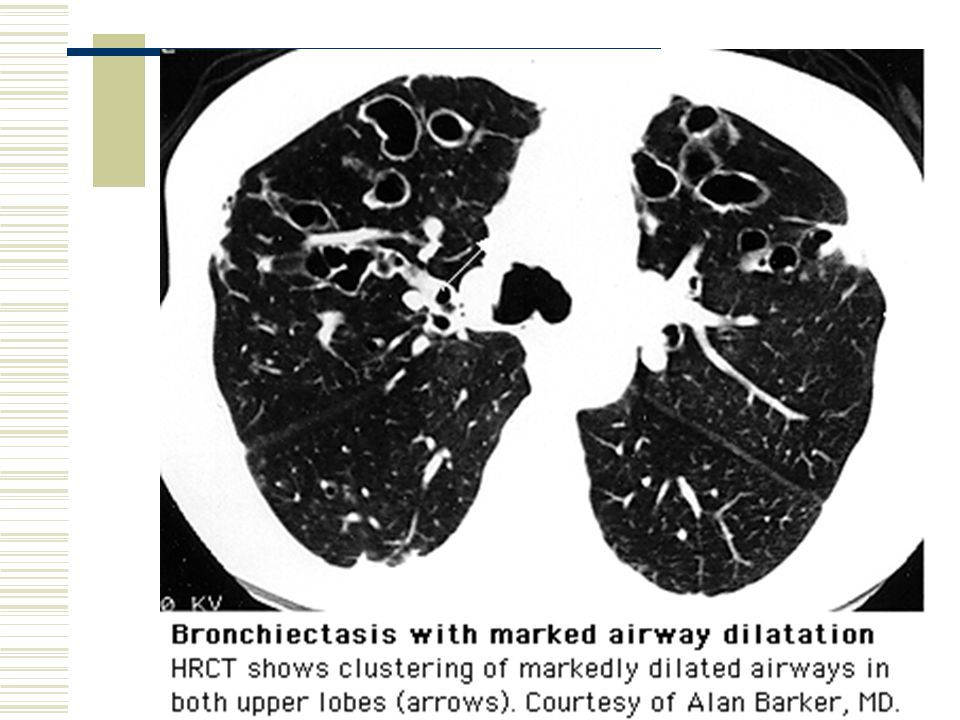
Bronchiectasis: Radiographic Findings CXR may be normal with mild disease. Patients with saccular bronchiectasis may have prominent cystic spaces, Other findings are due to dilated airways with thickened walls, which result from peribronchial inflammation as ("tram tracks“&"ring shadows“). HRCT provides an excellent view of dilated airways (standard technique for detecting or confirming the diagnosis of bronchiectasis).
. HRCT provides an excellent view of dilated airways (standard technique for detecting or confirming the diagnosis of bronchiectasis)..")
14
Bronchiectasis: Laboratory Findings Pulmonary function tests may demonstrate airflow obstruction. Upper lobe involvement may be suggestive of either tuberculosis or ABPA. With more widespread disease, measurement of sweat chloride levels for CF, Structural or functional assessment of nasal or bronchial cilia or sperm for primary ciliary dyskinesia.

15
Pathophysiology Infection: Bacterial, mycobacterial, esp. ABPA central airway bronchiectasis Airway obstruction: Intra luminal tumor, foreign body, lymph nodes, COPD Immunodeficiency: Ciliary dyskinesia, HIV, hypogammaglobulinemia, cystic fibrosis (obstruction and immunodeficiency.)
.")
16
Compares primary bronchiectasis with COPD

17
Exacerbation: Etiology Colonization/infection: Hemophilus Pseudomonas MAI Aspergillus Very difficult to distinguish colonization from acute infection with these bacteria.

18
Cystic air spaces

19
Ring shadow

22
DIAGNOSIS Lung function: Airflow obstruction – FEV1 decreased. Air trapping - RV increased Sweat test: Increased sodium and chloride in cystic fibrosis Bronchoscopy: Obstruction – foreign body, tumor. Immunoglobulin Cilia function and structure: Kartagener syndrome.

23
TREATMENT four Goals: 1. Eliminate cause 2. Improve tracheo bronchial clearance 3. Control infection 4. Reverse airflow obstruction

24
TREATMENT - 2 1. Immunoglobulin 2. Antituberculous drugs 3. Corticosteroids (ABPA) 4. Remove aspirated material Chest physical therapy Mucolytics agents Bronchodilators
 4. Remove aspirated material Chest physical therapy Mucolytics agents Bronchodilators.")
25
TREATMENT - 3 Antibiotics : short course, prolonged course, intermittent regular courses, inhalation. Initial empiric Rx: Ampicillin, Amoxicilin, Cefaclor, Septran Pseudomona aeruginosa = 3rd gen. Cephalosporin, Quinolone, Aminoglycoside, Pipracillin. Surgery Oxygen and diuretics Lung transplant

27
Lung Abscess Definition: A pulmonary parenchymal necrosis and cavitation resulting from infection. Aspiration is the most common cause. Risk Factors: E sophageal dysmotility, Seizure disorders, Neurologic conditions causing bulbar dysfunction. Periodontal disease and Alcoholism.

28
Microbiology Anaerobic bacteria are the most common causative organisms for lung abscess. Aerobic or facultative bacteria such as S. aureus, Klebsiella pneumoniae, Nocardia sp., and gram-negative organisms. Nonbacterial pathogens like fungi and parasites, may also cause abscess formation. In the immunocompromised host, aerobic bacteria and opportunistic pathogens may predominate.

29
Clinical Manifestations The symptoms may include cough, purulent sputum production, pleuritic chest pain, fever, and hemoptysis. In anaerobic infection, the clinical course may be chronic, and some patients may be asymptomatic. Physical examination : Rales or evidence of consolidation Fetid breath and poor dentition may be diagnostic clues. Clubbing or hypertrophic pulmonary osteoarthropathy may occur in chronic cases.

30
Clinical Manifestations The CXR classically reveals one or two thick-walled cavities in dependent areas of the lung. An air-fluid level is often present. Laboratory studies may reveal leukocytosis, anemia, and an elevated erythrocyte sedimentation rate. CT of the chest is helpful in defining the size and location of the abscess, as well as to evaluate for additional cavities and the presence of pleural disease. Cavitary lesions in nondependent regions like the right middle lobe or anterior segments of the upper lobes should raise the possibility of other etiologies, including malignancy.

31
Diagnosis The diagnosis of lung abscess is based on clinical symptoms, identification of predisposing conditions, and chest radiographic findings. Anaerobic bacteria are particularly difficult to isolate. Blood, sputum cultures, pleural fluid cultures should be obtained from patients with lung abscess. Bronchoscopy is perhaps most useful to rule out airway obstruction, mycobacterial infection, or malignancy.

32
CXR Finding

33
CT Finding

34
Differential diagnosis Mycobacterial infection, Pulmonary sequestration, Malignancy, Pulmonary infarction, Infected bulla.

35
Lung Abscess: Treatment Penicillin was the mainstay of empiric antibiotic therapy for lung abscess. Due to the emergence of beta-lactamase producing organisms, clindamycin (150 mg–300 mg every 6 h) is now standard therapy. Other agents, such as carbapenems and beta-lactam/ beta- lactamase inhibitor combinations, may be useful in selected cases. The duration of treatment for lung abscess is controversial. Four to six weeks of antibiotic therapy is typically employed. Treatment failure suggests the possibility of a noninfectious etiology.
 is now standard therapy. Other agents, such as carbapenems and beta-lactam/ beta- lactamase inhibitor combinations, may be useful in selected cases. The duration of treatment for lung abscess is controversial. Four to six weeks of antibiotic therapy is typically employed. Treatment failure suggests the possibility of a noninfectious etiology..")
36
Treatment : Surgery Refractory hemoptysis, Inadequate response to medical therapy, The need for a tissue diagnosis when there is concern for a noninfectious etiology.

37
الهی عاقبت محمود گردان به حق صالحان و نیک مردان

Similar presentations





Dr.Krock Dr.Vysetti Dr.Vysetti.>")









, and the parenchyma.>")






