Download presentation
Presentation is loading. Please wait.

1
RICKETTSIAL INFECTION: DIVERSITIES, DILEMMA AND CHALLENGES
Dr. Moniruzzaman Ahmed Associate Professor, Dept of Medicine MAG Osmani Medical College, Sylhet

2
Rickettsial diseases - 4 distinct genera:
Rickettsia, Orientia, Ehrlichia (Ehrlichia chaffeensis, the agent of human monocytic ecrlichiosis) and Anaplasma (Anaplasma phagocytophilium, the agent of human granulocytic anaplasmosis) Diseases caused by Rickettsia and Orientia species often reffered to as rickettsioses Coxiella burnetii, the agent of Q fever and Bartonella spp. were recently removed from the order Rickettsiales Parola P, Paddock CD, Raoult D. Tick-borne rickettsioses around the world: emerging diseases challenging old concepts. Clin Microbiol Rev. 2005;18:719–56
 and Anaplasma (Anaplasma phagocytophilium, the agent of human granulocytic anaplasmosis) Diseases caused by Rickettsia and Orientia species often reffered to as rickettsioses. Coxiella burnetii, the agent of Q fever and Bartonella spp. were recently removed from the order Rickettsiales. Parola P, Paddock CD, Raoult D. Tick-borne rickettsioses around the world: emerging diseases challenging old concepts. Clin Microbiol Rev. 2005;18:719–56.")
3
RICKETTSIAL SPECIES-BIOVARS
SPOTTED FEVER GROUP RICKETTSIOSES (SFGR) / TICK BORN RICKETTSIAL DISEASE (TBRD) TYPHUS GROUP (TG) SCRUB TYPHUS GROUP
 / TICK BORN RICKETTSIAL DISEASE (TBRD) TYPHUS GROUP (TG) SCRUB TYPHUS GROUP.")
4
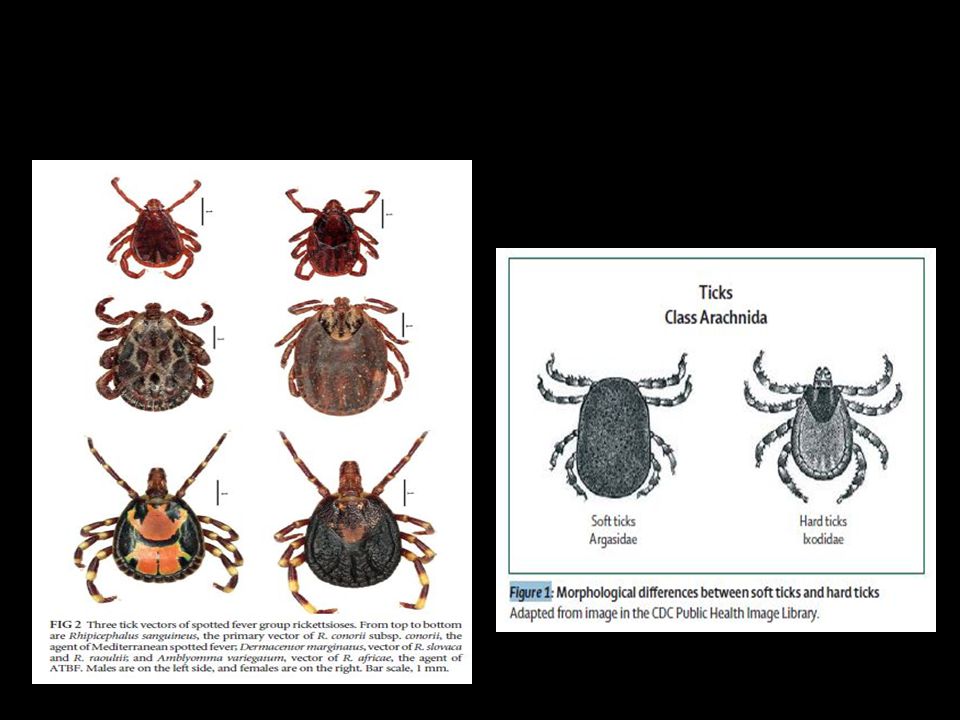
RICKETTSIA- BIOLOGY Small obligate intracellular parasites
Gram-negative bacteria Stain poorly with Gram stain (Giemsa) “Energy parasites” but not obligate, have capacity to make ATP Parasite of arthropods – fleas, lice, ticks and mites Reservoirs - animals, insects and humans
 Energy parasites but not obligate, have capacity to make ATP. Parasite of arthropods – fleas, lice, ticks and mites. Reservoirs - animals, insects and humans.")
5
The genus Rickettsia is named after Howard Taylor Ricketts (1871–1910), who studied Rocky Mountain spotted fever in the Bitterroot Valley From 1906 to 1910, Howard T Ricketts isolated the pathogen and showed that it circulated among ticks and mammals in the wild. Tragically, this talented rickettsiologist was affected by epidemic typhus and died in 1910, at the age of 39 years.

6
TRANSMISSION, PATHOGENESIS & PATHOPHYSIOLOGY

7
SPOTTED FEVER GROUP RICKETTSIOSES (SFGR)/ TICK BORN RICKETTSIAL DISEASE(TBRD)
/ TICK BORN RICKETTSIAL DISEASE(TBRD)")
8
PROTYPICAL DISEASES (SFGR)/(TBRD) ORGANISM DISEASE DISTRIBUTION
R.Rickettsii Rocky Mountain spotted fever Western hemisphere R. akari Rickettsialpox USA, former Soviet Union R. conorii Boutonneuse fever, Kenya tick typhus, Israeli tick typhus, Mediterranean spotted fever(MSF), Indian tick typhus, Astrakhan tick typhus, Marseilles fever Mediterranean countries, Africa, India, Southwest Asia R. sibirica Siberian tick typhus Siberia, Mongolia, northern China R. australia Australian tick typhus Australia R. japonica Oriental spotted fever Japan
, Indian tick typhus, Astrakhan tick typhus, Marseilles fever. Mediterranean countries, Africa, India, Southwest Asia. R. sibirica. Siberian tick typhus. Siberia, Mongolia, northern China. R. australia. Australian tick typhus. Australia. R. japonica. Oriental spotted fever. Japan.")
9
GEOGRAPHICAL DISTRIBUTION
Update on Tick-Borne Rickettsioses around the World: a Geographic Approach Philippe Parola,a Christopher D. Paddock,b Cristina Socolovschi,a Marcelo B. Labruna,c Oleg Mediannikov,a Tahar Kernif,d Mohammad Yazid Abdad,e* John Stenos,e Idir Bitam,f Pierre-Edouard Fournier,a Didier Raoulta October 2013 Volume 26 Number 4 Clinical Microbiology Reviews p. 657–702

10
GEOGRAPHICAL DISTRIBUTION (South America)
Update on Tick-Borne Rickettsioses around the World: a Geographic Approach Philippe Parola,a Christopher D. Paddock,b Cristina Socolovschi,a Marcelo B. Labruna,c Oleg Mediannikov,a Tahar Kernif,d Mohammad Yazid Abdad,e* John Stenos,e Idir Bitam,f Pierre-Edouard Fournier,a Didier Raoulta October 2013 Volume 26 Number 4 Clinical Microbiology Reviews p. 657–7

11
GEOGRAPHICAL DISTRIBUTION (EUROPE)
Update on Tick-Borne Rickettsioses around the World: a Geographic Approach Philippe Parola,a Christopher D. Paddock,b Cristina Socolovschi,a Marcelo B. Labruna,c Oleg Mediannikov,a Tahar Kernif,d Mohammad Yazid Abdad,e* John Stenos,e Idir Bitam,f Pierre-Edouard Fournier,a Didier Raoulta October 2013 Volume 26 Number 4 Clinical Microbiology Reviews p. 657–7

12
GEOGRAPHICAL DISTRIBUTION
Update on Tick-Borne Rickettsioses around the World: a Geographic Approach Philippe Parola,a Christopher D. Paddock,b Cristina Socolovschi,a Marcelo B. Labruna,c Oleg Mediannikov,a Tahar Kernif,d Mohammad Yazid Abdad,e* John Stenos,e Idir Bitam,f Pierre-Edouard Fournier,a Didier Raoulta October 2013 Volume 26 Number 4 Clinical Microbiology Reviews p. 657–7

13
GEOGRAPHICAL DISTRIBUTION
Update on Tick-Borne Rickettsioses around the World: a Geographic Approach Philippe Parola,a Christopher D. Paddock,b Cristina Socolovschi,a Marcelo B. Labruna,c Oleg Mediannikov,a Tahar Kernif,d Mohammad Yazid Abdad,e* John Stenos,e Idir Bitam,f Pierre-Edouard Fournier,a Didier Raoulta October 2013 Volume 26 Number 4 Clinical Microbiology Reviews p. 657–7

14
GEOGRAPHIC DISTRIBUTION
Geographic and temporal distribution of rickettsioses is largely determined by their vectors “One continent, one pathogenic tick-born rickettsia” an anachronism Prevalent throughout the world except Antarctica

15
Summary of prevalent Rickettsiae in Southeast Asia,their reservoirs and vectors for disease transmission Rickettsiae Main reservoirs Main vectors Typhus group Murine typhus (R.typhi) Rats(Rattus rattus, Rattus norvegicus, other Rattus sp.) Xenopsylla cheopis Scrub typhus (O. tsutsugamushi) Rats (Rattus sp. and Bandicota sp.) Trombiculid mites (Larval stage ) Spotted fever group R.Honei Rats ( Rattus sp. And Bandicota indica.) Ixodes granulatus, Ixodes sp., Rhipicephalus sp. R. felis Rats(Rattus sp) and shrews (Suncus murinus) Domestic cats, dogs, cows and pigs. Ctenocephalides orientis, C. felis felis, X. cheopis R. Conorii subsp. indica Rats ( Rattus sp.) R. sanguineus R. helvetica Unknown Ixodes spp R. japonica Rats ( Rattus sp. And B. indica.) Various species of animal ticks. Am. J. Trop. Med. Hyg., 91(3), 2014, pp. 451–460 Review Article: Rickettsial Infections in Southeast Asia: Implications for Local Populace and Febrile Returned Travelers Ar Kar Aung,* Denis W. Spelman, Ronan J. Murray, and Stephen Graves
 Rats(Rattus rattus, Rattus norvegicus, other Rattus sp.) Xenopsylla cheopis. Scrub typhus (O. tsutsugamushi) Rats (Rattus sp. and Bandicota sp.) Trombiculid mites (Larval stage ) Spotted fever group. R.Honei. Rats ( Rattus sp. And Bandicota indica.) Ixodes granulatus, Ixodes sp., Rhipicephalus sp. R. felis. Rats(Rattus sp) and shrews (Suncus murinus) Domestic cats, dogs, cows and pigs. Ctenocephalides orientis, C. felis felis, X. cheopis. R. Conorii subsp. indica. Rats ( Rattus sp.) R. sanguineus. R. helvetica. Unknown. Ixodes spp. R. japonica. Rats ( Rattus sp. And B. indica.) Various species of animal ticks. Am. J. Trop. Med. Hyg., 91(3), 2014, pp. 451–460 Review Article: Rickettsial Infections in Southeast Asia: Implications for Local Populace and Febrile Returned Travelers Ar Kar Aung,* Denis W. Spelman, Ronan J. Murray, and Stephen Graves.")
16
Short Report: Serosurveillance of Orientia tsutsugamushi and Rickettsia typhi in Bangladesh
Rapeephan R. Maude,* Richard J. Maude, Aniruddha Ghose, M. Robed Amin, M. Belalul Islam, Mohammad Ali, M. Shafiqul Bari, M. Ishaque Majumder, Ampai Tanganuchitcharnchai, Arjen M. Dondorp, Daniel H. Paris, Robin L. Bailey, M. Abul Faiz, Stuart D. Blacksell, and Nicholas P. J. Day Am. J. Trop. Med. Hyg., 91(3), 2014, pp. 580–583
, 2014, pp. 580–583.")
17
An ongoing study in Mymensingh Medical College
A total of 155 clinically suspected febrile patients were enrolled in the study. Out of them, 136 (88%), 31 (23%) and 61 (43%) were positive by Weil-Felix test, ELISA and PCR respectively. Out of the 61 PCR positive products, 16 were sequenced in Sapporo Medical University, Japan where 13 were found to be 99.9% consistent with Rickettsia felis. An ongoing study in Mymensingh Medical College A case series of 40 rickettsial infection in MMCH found 60% positive for scrub typhus by using Weil-Felix test (Miah MT, Rahman S, Sarker CN, Khan GK, Barman TK, Study on 40 cases of Rickettsia. Mymensingh Med J 16: 85–88)
, 31 (23%) and 61 (43%) were positive by Weil-Felix test, ELISA and PCR respectively. Out of the 61 PCR positive products, 16 were sequenced in Sapporo Medical University, Japan where 13 were found to be 99.9% consistent with Rickettsia felis. An ongoing study in Mymensingh Medical College. A case series of 40 rickettsial infection in MMCH found 60% positive for scrub typhus by using Weil-Felix test. (Miah MT, Rahman S, Sarker CN, Khan GK, Barman TK, Study on 40 cases of Rickettsia. Mymensingh Med J 16: 85–88)")
18
Association of tick genera and rickettsial species

21
CLINICAL MANIFESTATIONS
Clinical symptoms of tick-borne SFG rickettsioses begin 4 to 10 days after a bite and typically include fever, headache, muscle pain, rash, local lymphadenopathy, and, for most of these diseases, a characteristic inoculation eschar at the bite site Life-threatening manifestations : prolonged fever, renal failure, myocarditis, meningoencephalitis, hypotension, ARDS, multiple organ failure

22
ESCHAR (TACHE NOIRE) A crusty necrotic lesion with or without a surrounding erythematous halo which suggests the location of the vector bite
 A crusty necrotic lesion with or without a surrounding erythematous halo which suggests the location of the vector bite.")
25
LAR Lymphangitis may be present in several rickettsioses
Half of the cases of R. sibirica subsp. mongolitimonae infection present this sign (rope-like lymphangitis between the inoculation eschar and lymphadenitis) the infection being termed lymphangitis-associated rick-ettsiosis (LAR) also present in infections caused by R. heilongjiangensis and R. africae
 the infection being termed lymphangitis-associated rick-ettsiosis (LAR) also present in infections caused by R. heilongjiangensis and R. africae.")
26
DEBONEL / TIBOLA /SENLAT
Two dominant signs characterize this syndrome: an inoculation eschar and regional lymphadenopathy The occurrence of fever and rash is rare. DEBONEL/TIBOLA (Dermacentor-borne necrosis erythema lymphadenopathy/tick-borne lymphadenopathy), also called SENLAT (scalp eschar and neck lymphadenopathy after tick bite) when the tick bite affects only the scalp Produced by different species of Rickettsia. The main etiological agent is Rickettsia slovaca
, also called SENLAT (scalp eschar and neck lymphadenopathy after tick bite) when the tick bite affects only the scalp. Produced by different species of Rickettsia. The main etiological agent is Rickettsia slovaca.")
27
TYPHUS GROUP

28
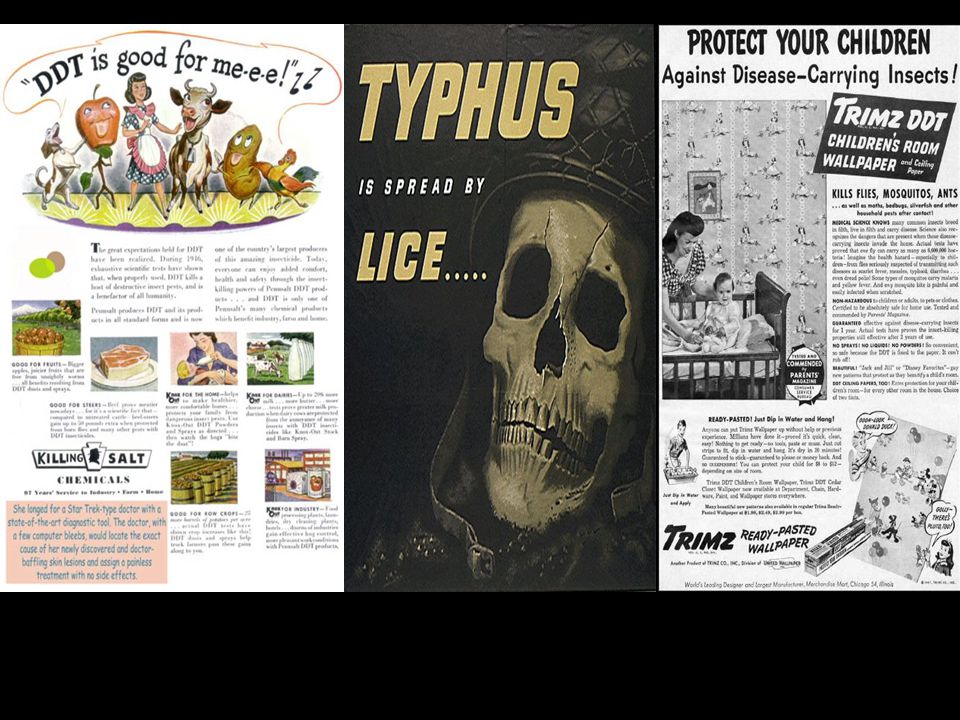
HISTORY AND HISTORICAL IMPACT OF TYPHUS
Europian history has been affected by Typhus epidemics from the the 15th through the 20th centuries, Pediculus humanus corporis as having a more profound effect on human history than any other animal Rickettsia prowazeki is isolated and identified by Da Rocha-Lima in Named in honor of H. T. Ricketts and L. von Prowazek, both of whom contracted typhus in the course of their investigations and died In 1829, the French clinician Louis clearly differentiated Typhus Fever from Typhoid Fever (Wolback et al., 1922) Transmission of Epidemic Typhus by the body louse was first demonstrated experimentally by Nicolle and others (1909) Early History. The first pestilence attributed to louse-borne typhus was the Athenian Plague of 430 B.C. The Fifteen Century. An epidemic of louse-borne typhus struck the besieging army of Spanish and within a month had killed 17,000 of the original 25,000 soldiers. The Sixteen Century. Western civilizations at that time regarded their God as a somewhat capricious tyrant, who either gave life or took it. Having no recourse to medicine as a means of explaining their devastations, medieval man turned to spiritual and metaphysical sources. A number of so-called "Assize Epidemics" occurred in England at this time, most notably at Oxford in 1577 and Exeter in The Oxford epidemic was of such import that the University there was closed for 30 years afterward. The Seventeenth Century. In the Thirty Years War of along with Plague and starvation, typhus was responsible for the loss of 10,000,000 people in which only 350,000 men died in combat . The Eighteenth Century. The 18th century was marred by many small epidemics of typhus The Nineteenth Century. Napoleon Bonaparte's campaign against the Russians in 1812 Napoleon had organized his "Grande Armee", numbering 600,000 well-seasoned troops -Only 90,000 French soldiers reached Moscow out of the original army of 600,000. The great majority, possibly as high as 300,000, had died of Epidemic Typhus and dysentery. Epidemic Typhus had helped defeat Napoleon and end his dreams of a French-ruled world. Typhus was endemic in Russia with some 82,000 cases a year recorded before 1914 ‘Either socialism will defeat the louse’, ‘or the louse will defeat socialism’; ‘All attention to this problem comrades!’ Lenin observed The Twentieth Century. Nicolle's proof of the transmission of typhus by body lice in 1910 Insurance Company as saying that as many as twenty-five million cases of typhus occurred during the years with upwards of three million deaths. To dehumanise the Jews the Nazi Propaganda Minister Joseph Goebbels declared: ‘These are no longer people…The task is not humanitarian but surgical. Steps have to be taken here, and really radical ones tool. Otherwise Europe will perish from the Jewish disease.’
 Transmission of Epidemic Typhus by the body louse was first demonstrated experimentally by Nicolle and others (1909) Early History. The first pestilence attributed to louse-borne typhus was the Athenian Plague of 430 B.C. The Fifteen Century. An epidemic of louse-borne typhus struck the besieging army of Spanish and within a month had killed 17,000 of the original 25,000 soldiers. The Sixteen Century. Western civilizations at that time regarded their God as a somewhat capricious tyrant, who either gave life or took it. Having no recourse to medicine as a means of explaining their devastations, medieval man turned to spiritual and metaphysical sources. A number of so-called Assize Epidemics occurred in England at this time, most notably at Oxford in 1577 and Exeter in The Oxford epidemic was of such import that the University there was closed for 30 years afterward. The Seventeenth Century. In the Thirty Years War of along with Plague and starvation, typhus was responsible for the loss of 10,000,000 people in which only 350,000 men died in combat . The Eighteenth Century. The 18th century was marred by many small epidemics of typhus. The Nineteenth Century. Napoleon Bonaparte s campaign against the Russians in 1812 Napoleon had organized his Grande Armee , numbering 600,000 well-seasoned troops -Only 90,000 French soldiers reached Moscow out of the original army of 600,000. The great majority, possibly as high as 300,000, had died of Epidemic Typhus and dysentery. Epidemic Typhus had helped defeat Napoleon and end his dreams of a French-ruled world. Typhus was endemic in Russia with some 82,000 cases a year recorded before ‘Either socialism will defeat the louse’, ‘or the louse will defeat socialism’; ‘All attention to this problem comrades!’ Lenin observed. The Twentieth Century. Nicolle s proof of the transmission of typhus by body lice in Insurance Company as saying that as many as twenty-five million cases of typhus occurred during the years with upwards of three million deaths. To dehumanise the Jews the Nazi Propaganda Minister Joseph Goebbels declared: ‘These are no longer people…The task is not humanitarian but surgical. Steps have to be taken here, and really radical ones tool. Otherwise Europe will perish from the Jewish disease.’")
29
HISTORY AND HISTORICAL IMPACT OF TYPHUS
Rickettsia prowazeki is isolated and identified by Da Rocha-Lima in Named in honor of H. T. Ricketts and L. von Prowazek, both of whom contracted typhus in the course of their investigations and died In 1829, the French clinician Louis clearly differentiated Typhus Fever from Typhoid Fever (Wolback et al., 1922) Transmission of Epidemic Typhus by the body louse was first demonstrated experimentally by Nicolle and others (1909). Nicolle received the Nobel Prize for his work on typhus in 1928.
 Transmission of Epidemic Typhus by the body louse was first demonstrated experimentally by Nicolle and others (1909). Nicolle received the Nobel Prize for his work on typhus in")
30
Henrique da Rocha Lima and Stanislas von Prowazeck

31
Charles Jules Henri Nicolle

32
HISTORY AND HISTORICAL IMPACT OF TYPHUS
15th-19th century Epidemics in Europe as a result of war, disaster, or in prisoners The Sixteen Century The Oxford was closed for 30 years The Seventeenth Century. In the Thirty Years War of along with Plague and starvation, typhus was responsible for the loss of 10,000,000 people in which only 350,000 men died in combat The Nineteenth Century. Only 90,000 French soldiers reached Moscow out of the original army of 600,000. Epidemic Typhus had helped defeat Napoleon and end his dreams of a French-ruled world

33
HISTORY AND HISTORICAL IMPACT OF TYPHUS
‘Either socialism will defeat the louse’, ‘or the louse will defeat socialism’; ‘All attention to this problem comrades!’ Lenin observed To dehumanise the Jews the Nazi Propaganda Minister Joseph Goebbels declared: ‘These are no longer Steps have to be taken here, and really radical ones tool. Otherwise Europe will perish from the Jewish disease.’ End of WWII, DDT for control Discovery of Tetracycline and Chloramphenicol in late 1940

34
Delousing and Disinfection

35
In German soilders had to show delousing certificates when on leave

38
Neither the queens nor the kings, the lice shaped the history of Europe

39
TYPHUS Disease Group Agent Vector Animal Reservoir
Geographical Distribution Typhus Group Epidemic Typhus Sylvatic typhus R. prowazekii Human body louse Flea Humans, Fleas, flying squirells Mountainous regions of Africa, Asia, and Central, north and South America. Murine typhus R. typhi Rat flea (Xenopsylla cheopis) Rats, cat, mice Tropical and subtropical areas Worldwide
 Rats, cat, mice. Tropical and subtropical areas. Worldwide.")
40
Brill-Zinsser Disease EPIDEMIC TYPHUS
The rickettsia can remain latent and reactivate months or years later, with symptoms similar to or even identical to the original attack of typhus, including a maculopapular rash Mild illness and low mortality rate. Rash is rare EPIDEMIC TYPHUS Incubation period approximately 1 week Sudden onset of fever, chills, headache and myalgia Rash after one week Maculopapular progressing to petechial or hemorrhagic First on trunk and spreads to extremities (centrifugal spread) Complications Myocarditis, stupor, delirium (Greek “typhos” = smoke) Recovery may take months, debilitating Mortality rate can be high (60-70%) but this may be because of the situation, such as famine
 Complications. Myocarditis, stupor, delirium (Greek typhos = smoke) Recovery may take months, debilitating. Mortality rate can be high (60-70%) but this may be because of the situation, such as famine.")
41
Rickettsia typhi - Murine or endemic typhus
Occurs worldwide Vector - rat flea Bacteria in feces Reservoir - rats No transovarian transmission Normal cycle - rat to flea to rat Humans accidentally infected Incubation period weeks Sudden onset of fever, chills, headache and myalgia Rash in most cases begins on trunk and spreads to extremities (centrifugal spread) Mild disease - resolves even if untreated
 Mild disease - resolves even if untreated.")
42
SCRUB TYPHUS

43
SCRUB TYPHUS GROUP Antigenic group Disease Species Vector
Animal reservoir Geographic distribution Scrub typhus Orientiatsutsugamushi Larval mite(chigger) Rodents Asia-Pacific region from maritime Russia and China to Indonesia and North Australia to Afghanistan Scrub Typhus Orientia chuta Unknown Dubai
 Rodents. Asia-Pacific region from maritime Russia and China to Indonesia and North Australia to Afghanistan. Scrub Typhus. Orientia chuta. Unknown. Dubai.")
44
Isolation of a Novel Orientia Species (O. chuto sp. nov.)
from a Patient Infected in Dubai Leonard Izzard,1,2 Andrew Fuller,3 Stuart D. Blacksell,4,5 Daniel H. Paris,4,5 Allen L. Richards,4,6,7 Nuntipa Aukkanit,4,5 Chelsea Nguyen,1 Ju Jiang,6 Stan Fenwick,2 Nicholas P. J. Day,4 Stephen Graves,1 and John Stenos1,2* JOURNAL OF CLINICAL MICROBIOLOGY, Dec. 2010, p. 4404–4409 Vol. 48, No. 12 Regional map showing the distribution of scrub typhus and the location of Dubai within the UAE. (Modified from a map by Lokal Profil that is freely available on Wikipedia.)
")
45
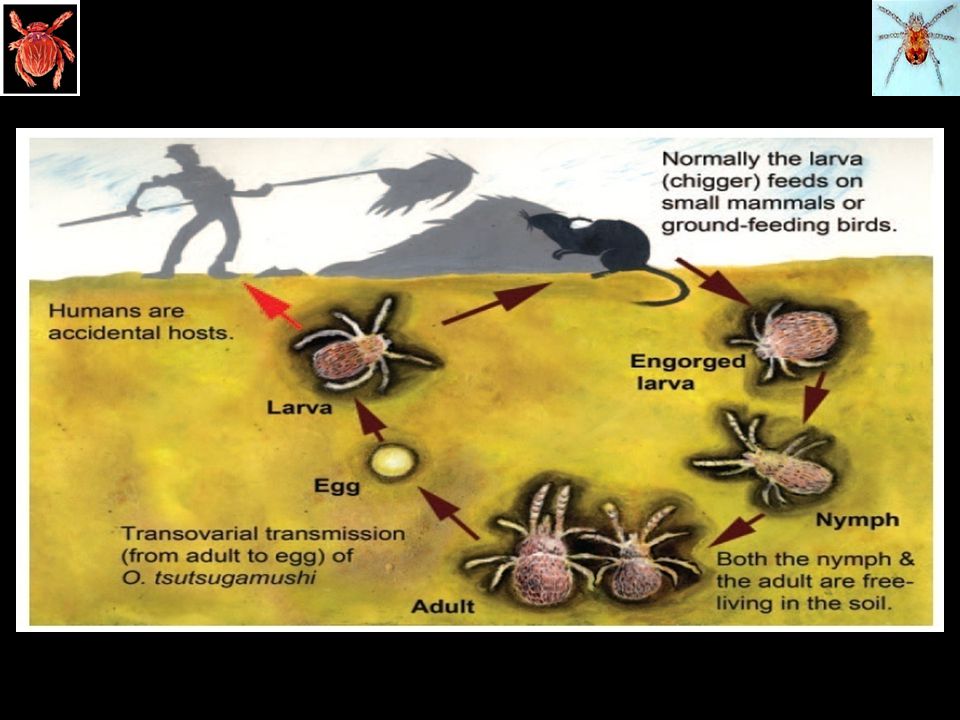
Scrub typhus Orientia tsutsugamushi is the causative agent & transmitted to humans through the bite of thrombiculid mites. The chigger (larval) phase is the only stage that is parasitic on animals or humans. First described in china 318 AD, isolated in Japan in 1930 Disease of rural villages and suburban areas. Term scrub is used because of the vegetation (terrain between woods and clearing) that harbours the vector. Scrub typhus is endemic in tsutsugamushi triangle which extends from northern Japan, far eastern Russia in the north to the Northern Australia in the south and pakistan in the west. Estimated 1 billion people are at risk of scrub typhus and estimated 1 million cases occur annually.
 phase is the only stage that is parasitic on animals or humans. First described in china 318 AD, isolated in Japan in Disease of rural villages and suburban areas. Term scrub is used because of the vegetation (terrain between woods and clearing) that harbours the vector. Scrub typhus is endemic in tsutsugamushi triangle which extends from northern Japan, far eastern Russia in the north to the Northern Australia in the south and pakistan in the west. Estimated 1 billion people are at risk of scrub typhus and estimated 1 million cases occur annually.")
46
TSUTSUGAMUSHI TRIANGLE

48
Clinical features-Scrub typhus
Incubation period - 1 to 3 weeks Sudden onset of fever, chills, headache and myalgia Maculopapular rash (spots and bumps) Begins on trunk and spreads to extremities (centrifugal spread) Commonest symptom high grade fever ,headache muscle pain ,cough, and GI symptoms Severe disease in 2ND week. Meningitis , meningo-encephalitis , deafness, pneumonia, ARDS, MODS & myocarditis. Reinfection & Relapses are seen due to variable immunity to different strains Mortality rates variable (1-15%)
 Begins on trunk and spreads to extremities (centrifugal spread) Commonest symptom high grade fever ,headache muscle pain ,cough, and GI symptoms. Severe disease in 2ND week. Meningitis , meningo-encephalitis , deafness, pneumonia, ARDS, MODS & myocarditis. Reinfection & Relapses are seen due to variable immunity to different strains. Mortality rates variable (1-15%)")
49
ESCHAR

51
SYNDROMIC CLASSIFICATION OF RICKETTSIOSES
Syndromic classification of rickettsioses: an approach for clinical Practice´l varo A. Faccini-Marti´nez a, Lara Garci´a-A´ lvarez b, Marylin Hidalgo a, Jose´ A. Oteo b,* International Journal of Infectious Diseases 28 (2014) e126–e139
 e126–e139.")
52
SYNDROMIC CLASSIFICATION OF RICKETTSIOSES
Syndromic classification of rickettsioses: an approach for clinical Practice´ lvaro A. Faccini-Marti´nez a, Lara Garci´a-A´ lvarez b, Marylin Hidalgo a, JoseInfectious Diseases 28 (2014) e126–e139
 e126–e139.")
53
Laboratory Diagnosis Serologic assays (eg, indirect immunofluorescence, complement fixation, indirect hemagglutination, latex fixation, enzyme immunoassay, microagglutination) are preferable to the nonspecific and insensitive Weil-Felix test based on the cross-reactive antigens of Proteus vulgaris strains Immunofluorescence assay (IFA) is currently considered to be the reference serological method.
 are preferable to the nonspecific and insensitive Weil-Felix test based on the cross-reactive antigens of Proteus vulgaris strains. Immunofluorescence assay (IFA) is currently considered to be the reference serological method.")
54
Polymerase chain reaction (PCR) to detect rickettsiae in blood or tissue provides promise for early diagnosis. PCR testing and immunohistochemical staining of skin specimen obtained by performing a biopsy may help confirm the clinical diagnosis in patients with rash. The swabs of eschars may be used for molecular detection of rickettsial infections when biopsies are difficult to perform.

56
DILEMMA & CHALLENGES

57
DIAGNOSIS A thorough history and knowledge of the distribution of rickettsial agents and their vectors evidence of exposure to vector clinical features like fever, rash, eschar, headache and myalgia high index of suspicion are crucial factors

58
TREATMENT Treatment Antibiotic Indication Dosage
Doxycycline (standard treatment of rickettsosis) Severe rickettsioses (including pregnant women and children) Ideally intravenous Adults or children>45kg Adults or children>45kg;100 mg twice a day pregnant women(last trimester):100 mg twice a day Children<45kg;22 mg twice a day Continued for 3 days after symptoms has resolved Macrolides(josamycin, clarythromycin and azithrothromycin Option for not severe rickettsioses in children and pregnant women Josamycin:children 50 mg/kg twice a day, pregnant women 1g/8hrly Clarithromycin for children :15mg/kg twice a day Josamycin 5 days Clarithromycin 7 days and Azithromycin 3 days Chloramphenicol Alternative option in severe rickettsioses Azithromycin in children :10 mg /kg/day in 1 dose Adults and pregnant (first and second trimester); mg/kg in4 divided doses Children12-25 mg/kg every 6 hourly 5-10 days Syndromic classification of rickettsioses: an approach for clinical Practice´ lvaro A. Faccini-Marti´nez a, Lara Garci´a-A´ lvarez b, Marylin Hidalgo a, JoseInfectious Diseases 28 (2014) e126–e139
 Severe rickettsioses (including pregnant women and children) Ideally intravenous. Adults or children>45kg. Adults or children>45kg;100 mg twice a day pregnant women(last trimester):100 mg twice a day. Children<45kg;22 mg twice a day. Continued for 3 days after symptoms has resolved. Macrolides(josamycin, clarythromycin and azithrothromycin. Option for not severe rickettsioses in children and pregnant women. Josamycin:children 50 mg/kg twice a day, pregnant women 1g/8hrly. Clarithromycin for children :15mg/kg twice a day. Josamycin 5 days. Clarithromycin 7 days and Azithromycin 3 days. Chloramphenicol. Alternative option in severe rickettsioses. Azithromycin in children :10 mg /kg/day in 1 dose. Adults and pregnant (first and second trimester); mg/kg in4 divided doses. Children12-25 mg/kg every 6 hourly days. Syndromic classification of rickettsioses: an approach for clinical. Practice´ lvaro A. Faccini-Marti´nez a, Lara Garci´a-A´ lvarez b, Marylin Hidalgo a, JoseInfectious Diseases 28 (2014) e126–e139.")
60
But however secure and well-regulated civilized life may become; bacteria, protozoa, viruses, infected fleas, lice, ticks, mosquitoes, and bedbugs will always lurk in the shadows ready to pounce when neglect, poverty, famine, or war lets down the defenses. Hans Zinsser Rats, Lice and History (1934), 13-4.
,")
Similar presentations





















 are viruses that can be transmitted to man by arthropod vectors. Arboviruses belong to three.>")


