

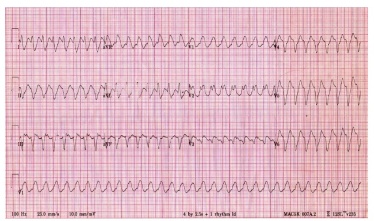
Ventricular tachycardia exhibits 4 or more ventricular ectopic beats at a HR of 150-200bpm.
It results from two possible mechanisms:
- A latent ventricular focus/ enhanced automaticity in a ventricular pacemaker

- A re-entry circuit around a fixed anatomical area of the ventricular myocardium
There exist a number of variances in VT:
- Rate
- Morphology
- Duration
- Frequency
- Regularity
VT can exist as:
- Sustained
- Period of VT lasting >30 seconds
- Non-sustained
- Period of VT lasting <30 seconds
Prognosis varies from few or no symptoms, to death.
VT can inhibit cardiac output, resulting in syncope, hypotension and acute cardiac failure. The uncoordinated nature of impulse activity gives a loss in atrial kick.
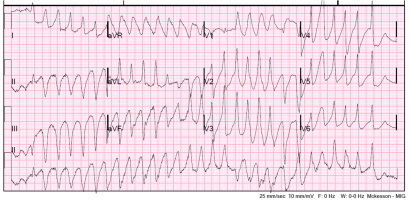
There are two primary types of VT:
- Monomorphic
- A run of fast ventricular ectopics with the same morphology present in each waveform
- Polymorphic
- A run of fast ventricular ectopics displaying a beat to beat variation in morphology
ECG characteristics:
- Rapid ventricular rate
- Vrate>Arate
- Wide complexes
- >140ms
- AV Dissociation
- The SA node still continues to generate impulses
- Due to the amplitude and duration of the ventricular impulses, P waves are often masked by their morphology
- Hence, both the atria and ventricles are paced independently

- Positive Concordance
- VT starts in left posterior wall
- Negative Concordance
- VT starts apically
- Monomorphic VT:
- Regular rhythm
- Uniform trace morphology
- Impulses arise from a single focus
- Polymorphic VT:
- Varying trace morphologies
- Multi-focal impulse generation
Capture Beats (2)
Occasionally, the timing of a SA node impulse will be such that it can be conducted to the ventricles via the AV node and activate them before the next independent impulse.
This results in a depolarisation that displays as normal on the ECG trace, and occurs slightly sooner than the next ventricular focused beat would be expected.
Fusion Beats (1)
These are similar to capture beats, however, the atrial impulse conducts to the ventricles later in the cardiac cycle, so the sinus impulse and that from the ventricular focus cause the ventricles to activate in unison. The resulting waveform resembles something in between normal and VT.

Causes of VT:
- Acute MI/ ischaemia
- Previous MI
- Dilated Cardiomyopathy
- Hypertrophic Cardiomyopathy
- Mitral Valve Prolapse
- Sarcoidosis
- Digoxin Toxicity
- Myocarditis
Clinical Details:
- Monomorphic VT can indicate heart disease, but can be normal
- VT can resemble other problems:
- Artefact
- Assume VT: assess the patient before the ECG
- SVT with aberrancy
- Artefact
VT vs SVT w/ Aberrancy
It is important to distinguish between the two when analysing the ECG. Features that suggest VT are as follows:
- History of heart disease
- Absence of BBB morphology
- Concordance
- Capture/Fusion beats
- Complexes >160ms
- AV dissociation
- Extreme axis deviation
- Brugada’s sign
- RSR’ complexes where RSR’ is taller than RSR‘
References:
http://www.hqmeded-ecg.blogspot.kr
Wagner, GS. Marriott’s Practical Electrocardiography (11th edition), Lippincott Williams & Wilkins 2007.
Hampton, JR. The ECG Made Easy (8th edition), Churchill Livingstone 2013.
Luthra, A. ECG Made Easy (3rd edition), Anshan 2007.

