
25 Chapter 25 The Urinary System
By Ganesan Kamatchi
Motivation.

Hemodialysis, also spelled haemodialysis, or simply dialysis, is a process of purifying the blood of a person whose kidneys are not working normally. This type of dialysis achieves the extracorporeal removal of waste products such as creatinine and urea and free water from the blood when the kidneys are in a state of failure. Hemodialysis is one of three renal replacement therapies (the other two being kidney transplant and peritoneal dialysis). An alternative method for extracorporeal separation of blood components such as plasma or cells is apheresis. Hemodialysis can be an outpatient or inpatient therapy. Routine hemodialysis is conducted in a dialysis outpatient facility, either a purpose built room in a hospital or a dedicated, stand-alone clinic. Less frequently hemodialysis is done at home. Dialysis treatments in a clinic are initiated and managed by specialized staff made up of nurses and technicians; dialysis treatments at home can be self-initiated and managed or done jointly with the assistance of a trained helper who is usually a family member.
Learning Objectives
Upon completion of the work in this chapter students should be able to:
- Describe the external structure of the kidney, including its location, support structures, and covering
- Identify the major internal divisions and structures of the kidney
- Identify the major blood vessels associated with the kidney and trace the path of blood through the kidney
- Provide specific examples to demonstrate how the urinary system responds to maintain homeostasis in the body in relation with other systems
Background.
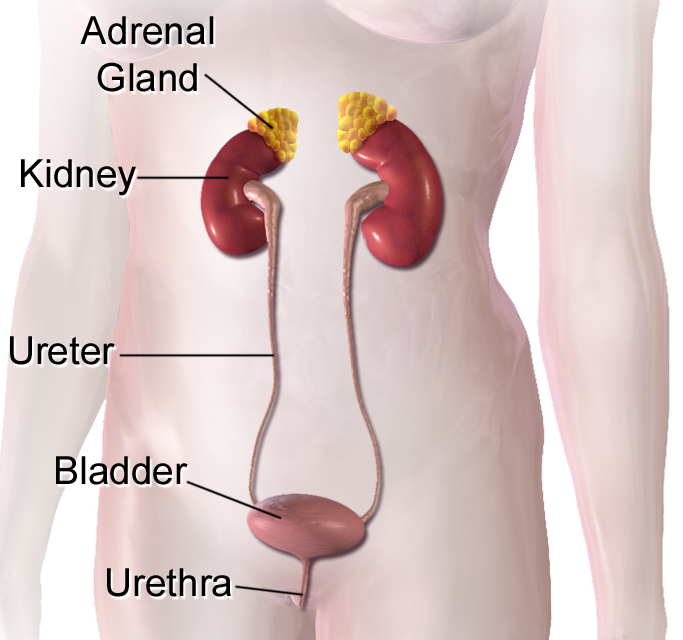
The urinary system consists of two kidneys, two ureters, a single urinary bladder, and a single urethra (Figure 25.2). This system has roles that you may already be aware of, such as cleansing the blood and ridding the body of wastes. However, there are additional, equally important functions played by the system. Take for example, regulation of pH, a function shared with the lungs and the buffers within the blood. Additionally, the regulation of blood pressure is a role shared with the heart and blood vessels. What about regulating the concentration of solutes in the blood? Did you know that the kidney is important in determining the concentration of red blood cells?
Most importantly, the urinary system works to remove the dissolved materials from the blood through the process of filtration. Filtration occurs when one or more substances pass through a selectively permeable membrane, while others are retained. Within the kidneys, filtration involves both metabolic waste products, such as urea or toxins, as well as materials that are beneficial to the body. Any filtered material that is not desirable though will be excreted from the body. If the kidneys fail, these functions are compromised or lost altogether, with devastating effects on the homeostasis. Affected individuals may experience weakness, lethargy, shortness of breath, anemia, widespread edema (swelling), metabolic acidosis, rising potassium levels, heart arrhythmias, and more. Each of these functions is vital to your well-being and survival.
The Kidney
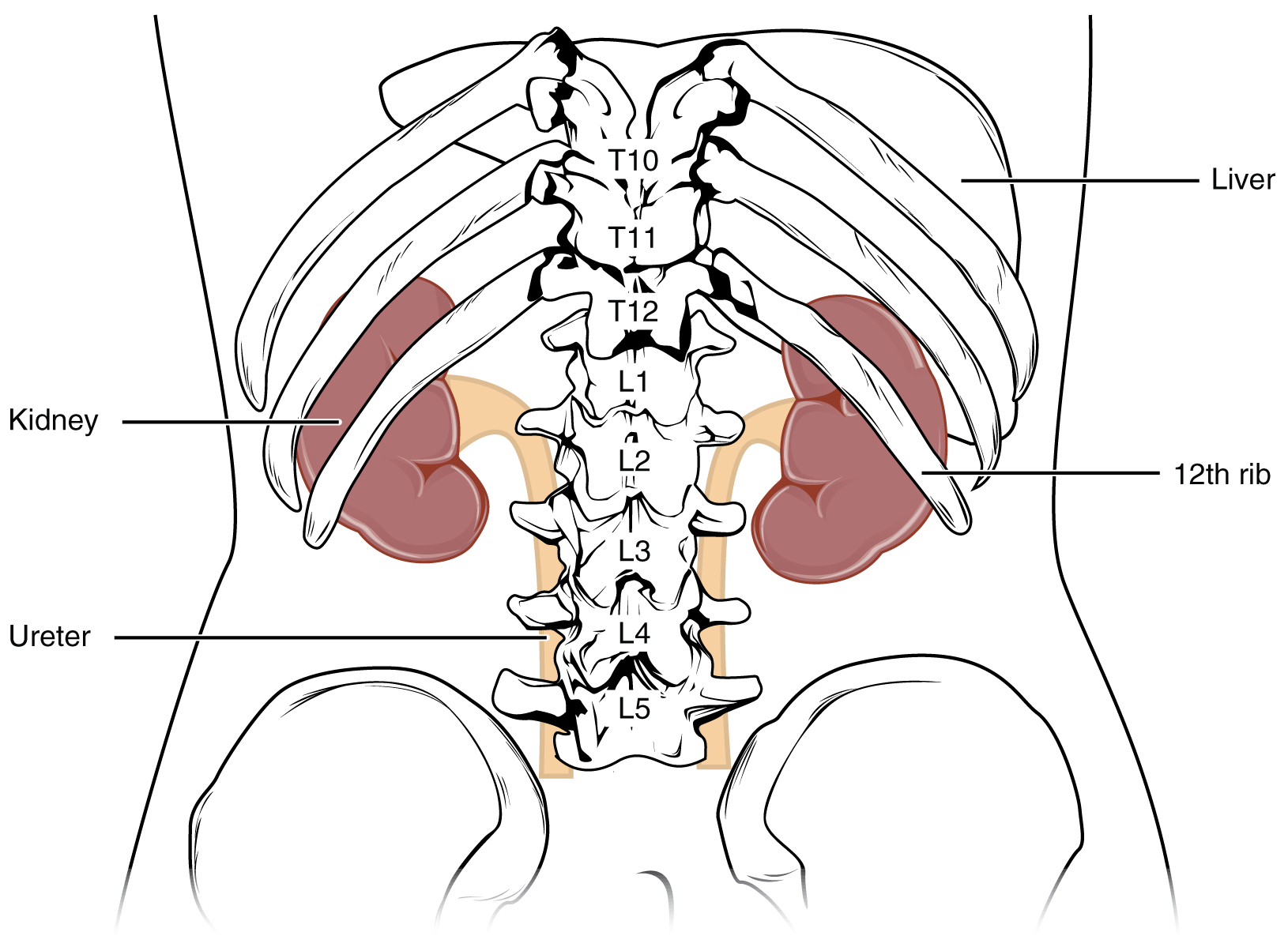
The kidneys lie on either side of the spine in the retroperitoneal space between the parietal peritoneum and the posterior abdominal wall, well protected by muscle, fat, and ribs (Figure 25.3). They are roughly the size of your fist, and the male kidney is typically a bit larger than the female kidney.
In this laboratory, you will use models, diagrams and histological samples to study the anatomy of the urinary system. Specifically, you will examine the gross and microscopic anatomy of the system as it is represented in humans. As you study the anatomy, keep in mind that the urinary system functions to remove the dissolved materials from the blood, regulate electrolytes and fluid volume, concentrate and release waste products, and reabsorb metabolically important substances.
Blood Supply to the Kidney
The kidneys are well vascularized, receiving about 25 percent of the cardiac output at rest. The kidney filters metabolic products from the blood and returns important components such as water, glucose, and ions back into the blood. To ensure this, blood flow into and out of the kidneys is essential (Figure 25.4).
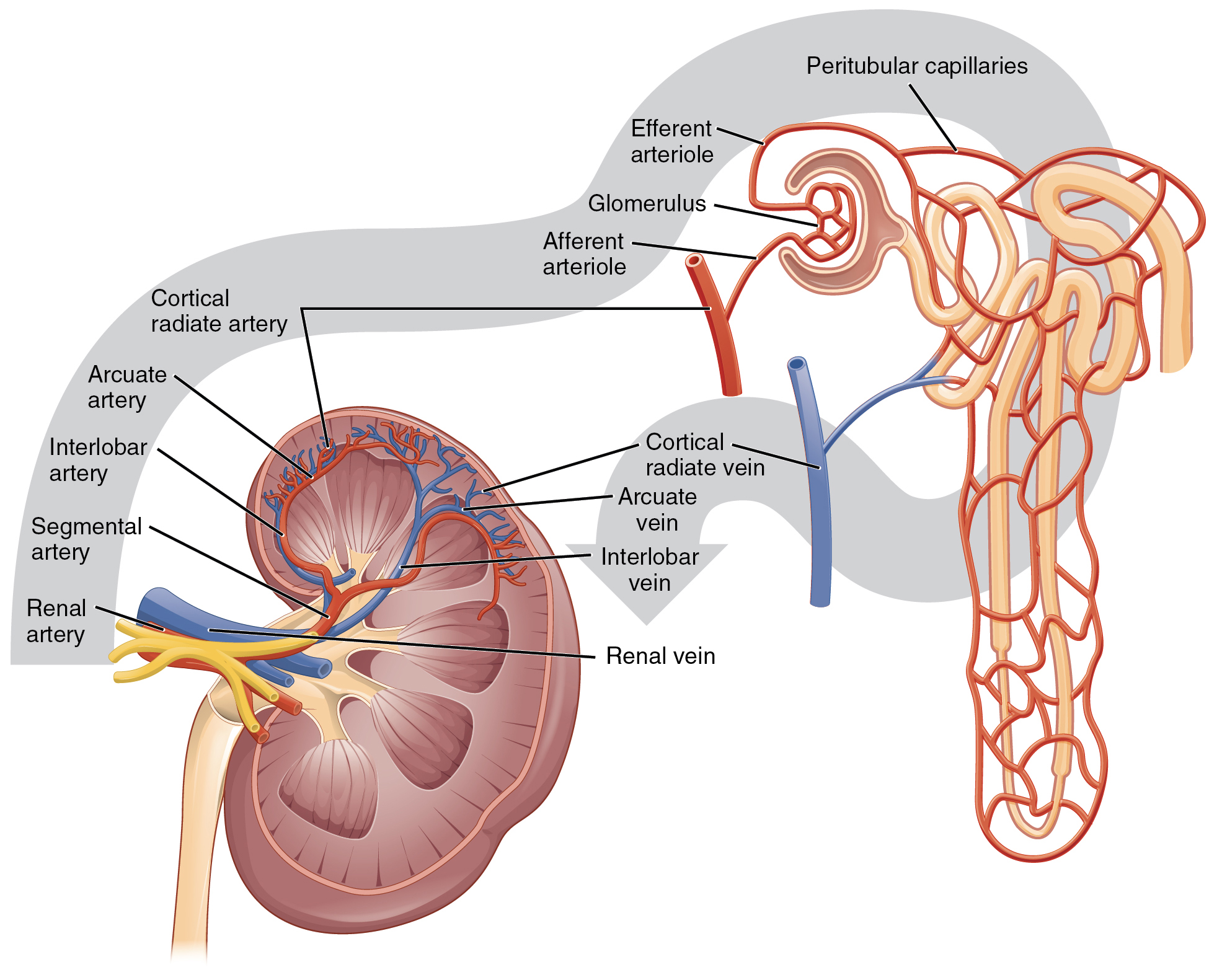
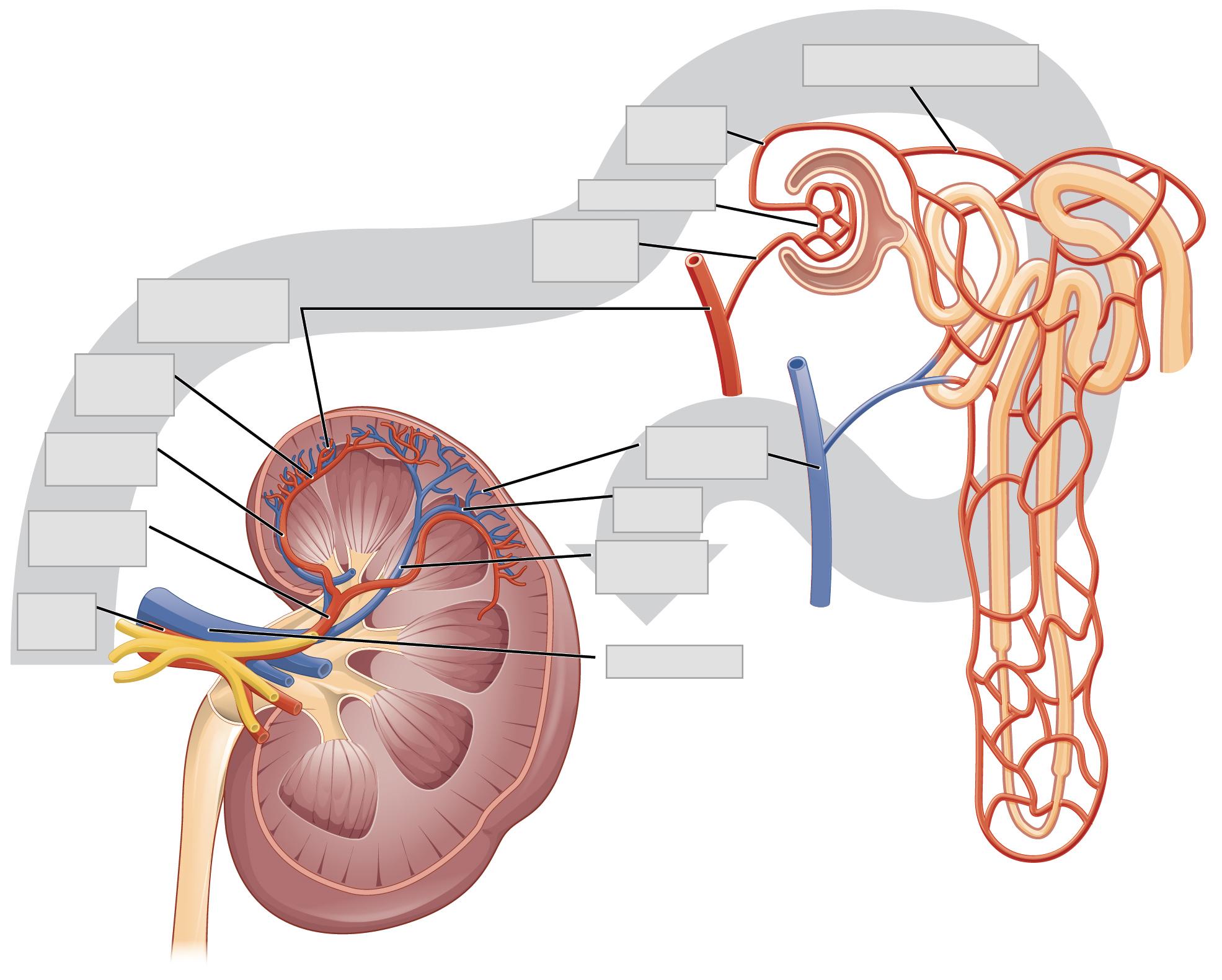
The first vessel to enter the kidney comes from the abdominal aorta, and this vessel is the renal artery. Once in the kidney, the renal artery first divides into segmental arteries, which are located within the renal sinus. As the segmental arteries continue to branch, blood flows into the interlobar arteries, which pass through the renal columns and extend to the cortex. Once the interlobar arteries reach the cortex, they bend abruptly and branch to form the arcuate arteries. These vessels are named so because they form an arc located between the medulla and cortex of the kidney. From here, the arteries become the cortical radiate (interlobular) arteries, which enter into the cortex.
The cortical radiate arteries then branch to form the afferent arterioles. The afferent arterioles will take blood to the glomerulus, a cluster of capillaries where filtration occurs. Blood then travels through the efferent arterioles and into the peritubular capillaries. It is within the peritubular capillaries that reabsorption and secretion will take place. In some regions of the cortex, the efferent arterioles may also branch to give rise to the vasa recta. These vessels only represent a small number of capillaries within the kidney, but they are important for producing concentrated urine.
Whereas the renal arteries form directly from the descending aorta, the renal veins return cleansed blood directly to the inferior vena cava. Blood from the peritubular capillaries or vasa recta will first be directed to the cortical radiate (interlobular) veins. From here, the blood will be sent to the arcuate veins, to the interlobar veins, and then to the renal vein, which leads to the vena cava.
Histology of the Kidney
The renal structures that conduct the essential work of the kidney cannot be seen by the naked eye. Only a light or electron microscope can reveal these structures. Even then, serial sections and computer reconstruction are necessary to give us a comprehensive view of the functional anatomy of the nephron and its associated blood vessels.
Nephrons are the “functional units” of the kidney and located in the renal cortex (Figure 25.5).
Nephrons cleanse the blood and balance the constituents of circulation. These structures take a simple filtrate of the blood and modify it into urine. The system’s ability to filter the blood resides in about 2 to 3 million glomeruli, which are distributed more or less equally between the two kidneys. Because glomeruli filter the blood based mostly on particle size, large elements like blood cells, platelets, antibodies, and albumen are excluded. All other solutes, such as ions, amino acids, vitamins, and wastes, are filtered to create a filtrate composition that is very similar to blood plasma. Overall, the principle task of the nephron population is to balance the plasma to homeostatic set points and excrete potential toxins in the urine. They do this by accomplishing three principle functions— filtration, reabsorption, and secretion. The functional regions that make up a single nephron include the renal corpuscle, proximal convoluted tubule, nephron loop, and distal convoluted tubule. While the renal corpuscle, proximal convoluted tubule and distal convoluted tubule are located in the cortex, the nephron loop is located in the medulla region of the kidney (Figure 25.6).
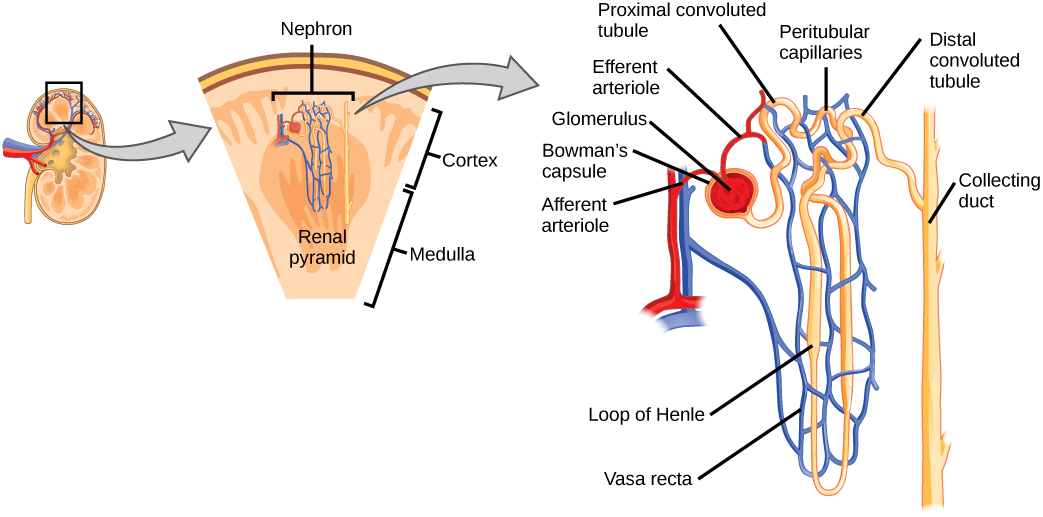
As the afferent arterioles enter into the nephron, they will form a tuft of high-pressure capillaries known as the glomerulus. Surrounding the glomerulus is a thin, double-walled capsule, known as the glomerular capsule (Bowman’s capsule) and the space between each is known as the capsular space. Together, the glomerulus and capsule are known as the renal corpuscle, making up the proximal end of each nephron (Figure 25.6). This region is where filtration takes place. Through this process, water and some solutes in the blood plasma will pass from the capillaries of the glomerulus and into the capsular space of the nephron to begin filtrate production.
The remaining portion of the nephron consists of a continuous and sophisticated tubule system (Figures 25.7 and 25.8). As blood passes through the glomerulus, 10 to 20 percent of the plasma filters through small spaces between the cells of the glomerulus. This filtered fluid is then captured by the Bowman’s capsule and funneled to the proximal convoluted tubule (PCT). Simple cuboidal cells form this tubule with prominent microvilli on the luminal surface, forming a brush border. These microvilli create a large surface area to maximize the reabsorption of some solutes (Na+, Cl–, glucose, etc.) from the blood and secretion of these back into the tubule for disposal. This is one of the most essential functions of this region of the nephron. Once filtrate leaves the PCT, it is directed into the nephron loop (Loop of Henle), which consists of two portions. The descending and ascending portions of the loop are simply continuations of the same tubule. They run adjacent and parallel to each other after having made a hairpin turn at the deepest point of their descent. The descending loop of Henle consists of an initial short, thick portion and long, thin portion, whereas the ascending loop consists of an initial short, thin portion followed by a long, thick portion. Fluid will then be directed to the last portion of the nephron, known as the distal convoluted tubule (DCT). These cells are not as active as those in the PCT; thus, there are fewer microvilli on their apical surface.
As fluid flows through this tubule system, water, glucose, and many electrolytes are returned to the blood. Any urea or other wastes that are collected are concentrated as they pass through the nephron and into the collecting duct, a tube that receives fluid from the nephrons. The collecting ducts are continuous with each nephron, but not technically part of it. In fact, each duct collects filtrate from several nephrons for final modification. Collecting ducts merge as they descend deeper in the medulla to form about 30 terminal ducts, which empty at a papilla.
The Ureter
As urine is formed, it drains into the calyces of the kidney, which merge to form the funnel shaped renal pelvis within each hilum. As the renal pelvis extends out of the hilum, it narrows to become the ureter of each kidney. The ureters go downwards, turn medially and pierce the bladder wall obliquely. This is important because it creates a one-way valve (a physiological sphincter rather than an anatomical sphincter) that allows urine into the bladder, but prevents the reflux of urine from the bladder back into the ureter.
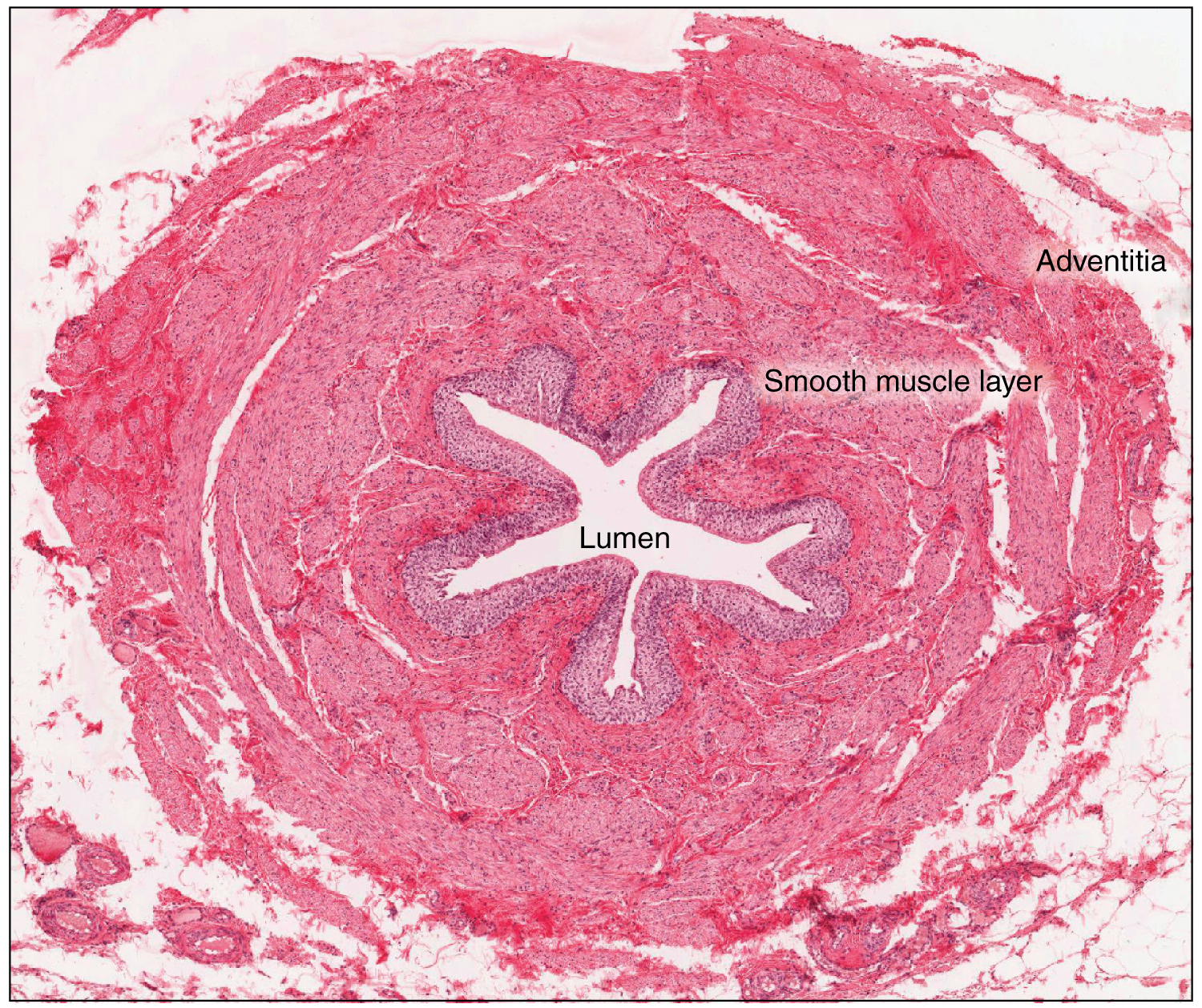
The ureters are approximately 30 cm long and consist of three tissue layers (Figure 25.9). The inner mucosa is lined with transitional epithelium and scattered goblet cells that secrete protective mucus. The thick muscular layer of the ureter consists of both longitudinal and circular smooth muscles that create the peristaltic contractions to move the urine into the bladder without the aid of gravity. Finally, a loose, outer adventitial layer composed of collagen and fat anchors the ureters between the parietal peritoneum and the posterior abdominal wall.
The Urinary Bladder
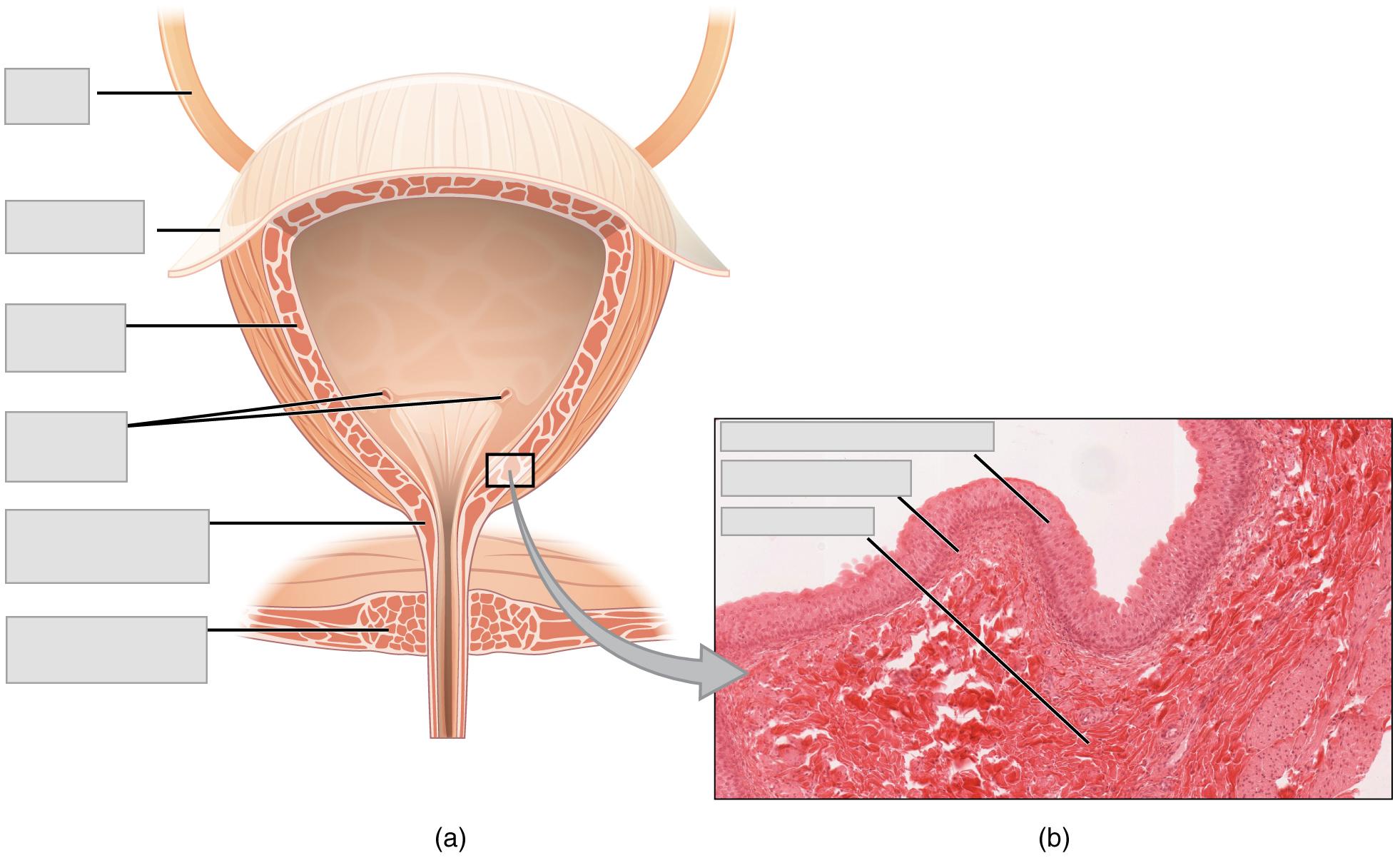
The urinary bladder is the primary organ that collects urine from both ureters (Figure 25.10). In females, the bladder lies anterior to the uterus, posterior to the pubic bone and anterior to the rectum. During late pregnancy, its capacity is reduced due to compression by the enlarging uterus, resulting in increased frequency of urination. In males, the anatomy is similar, minus the uterus, and with the addition of the prostate inferior to the bladder. The bladder is partially retroperitoneal (outside the peritoneal cavity) with its peritoneal-covered “dome” projecting into the abdomen when the bladder is distended with urine.
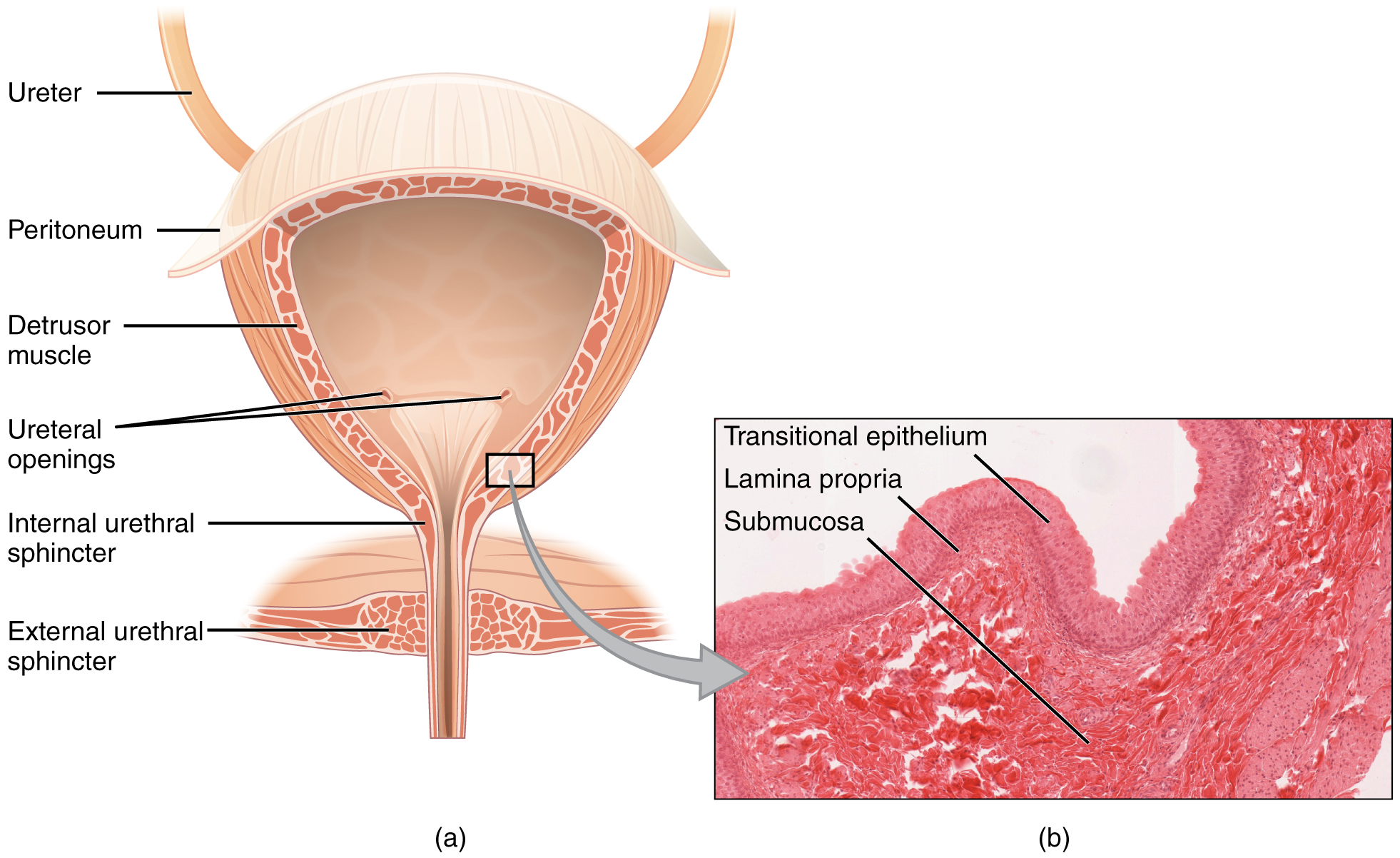
The bladder is unique in the fact that it is a highly distensible organ composed of irregular crisscrossing bands of smooth muscle, collectively called the detrusor muscle. The interior surface is made of transitional epithelium that is structurally suited for the large volume fluctuations of the bladder. When empty, its cells resemble columnar epithelia, but when stretched, it “transitions” (hence the name) to a squamous appearance. The volume of urine that the adult bladder can collect and hold can range from nearly zero to 600 mL, so the makeup of this tissue must allow it to be adaptable.
In addition to its elasticity, the detrusor muscle can contract with significant force in the young. Though the bladder’s strength can significantly diminish with age, voluntary contractions of abdominal skeletal muscles can increase intra-abdominal pressure to promote more forceful bladder emptying.
The Urethra
The terminal organ of the urinary system is the urethra, which transports urine from the bladder to the outside of the body for disposal. The urethra is the only urologic organ that shows any significant anatomic difference between males and females; all other urine transport structures are identical.
The urethra in both males and females begins inferior and central to the two ureteric openings in the bladder. Together, these structures form the three points of a triangular-shaped area at the base of the bladder, known as the trigone. In both males and females, the proximal urethra is lined by transitional epithelium, whereas the terminal portion is a nonkeratinized, stratified squamous epithelium. In the male, pseudostratified columnar epithelium lines the urethra between these two cell types. Voiding is regulated by an involuntary autonomic nervous system-controlled internal urinary sphincter, which consists of smooth muscle, and a second voluntary external urinary sphincter that is made of skeletal muscle.
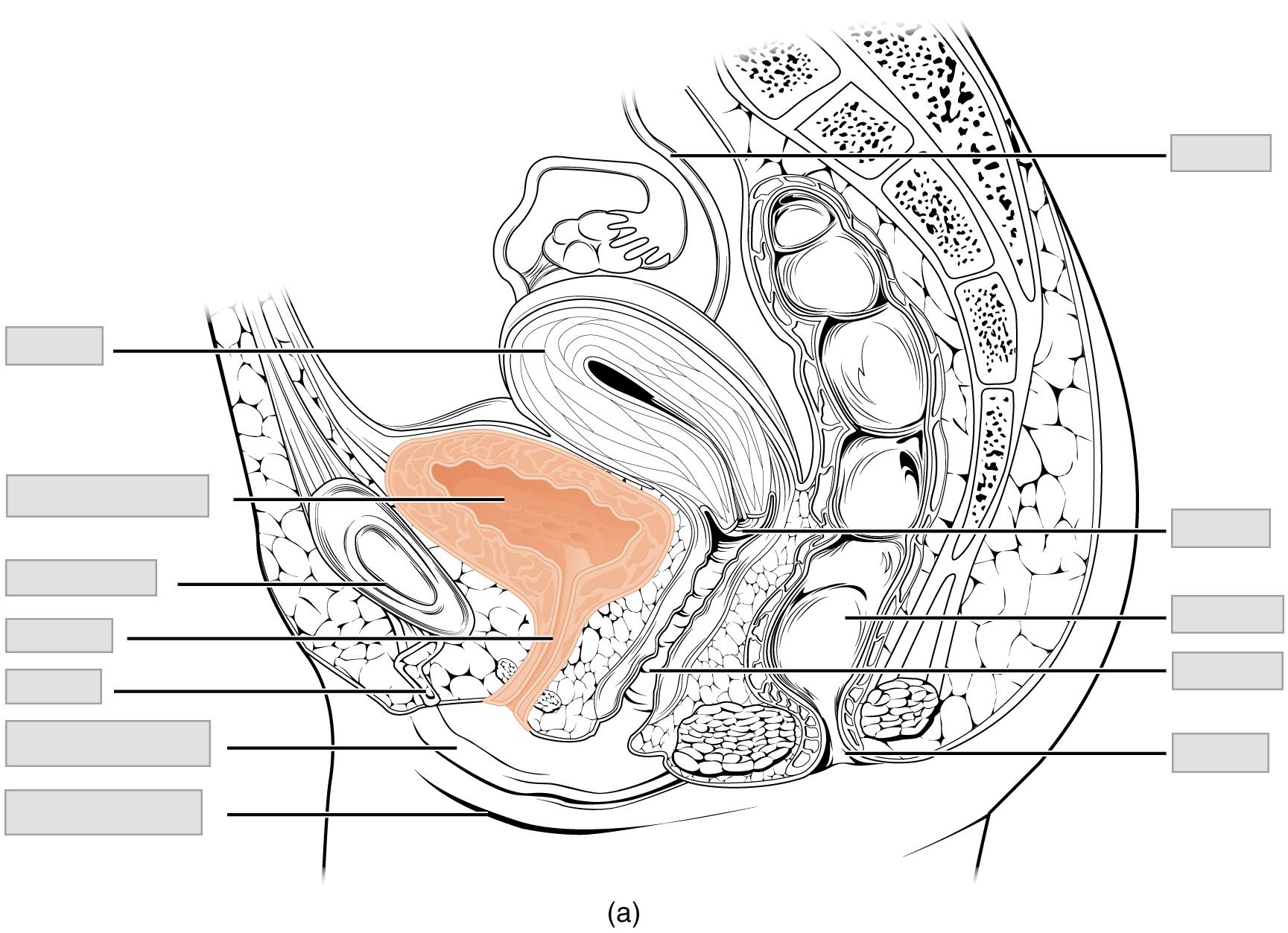
Female Urethra
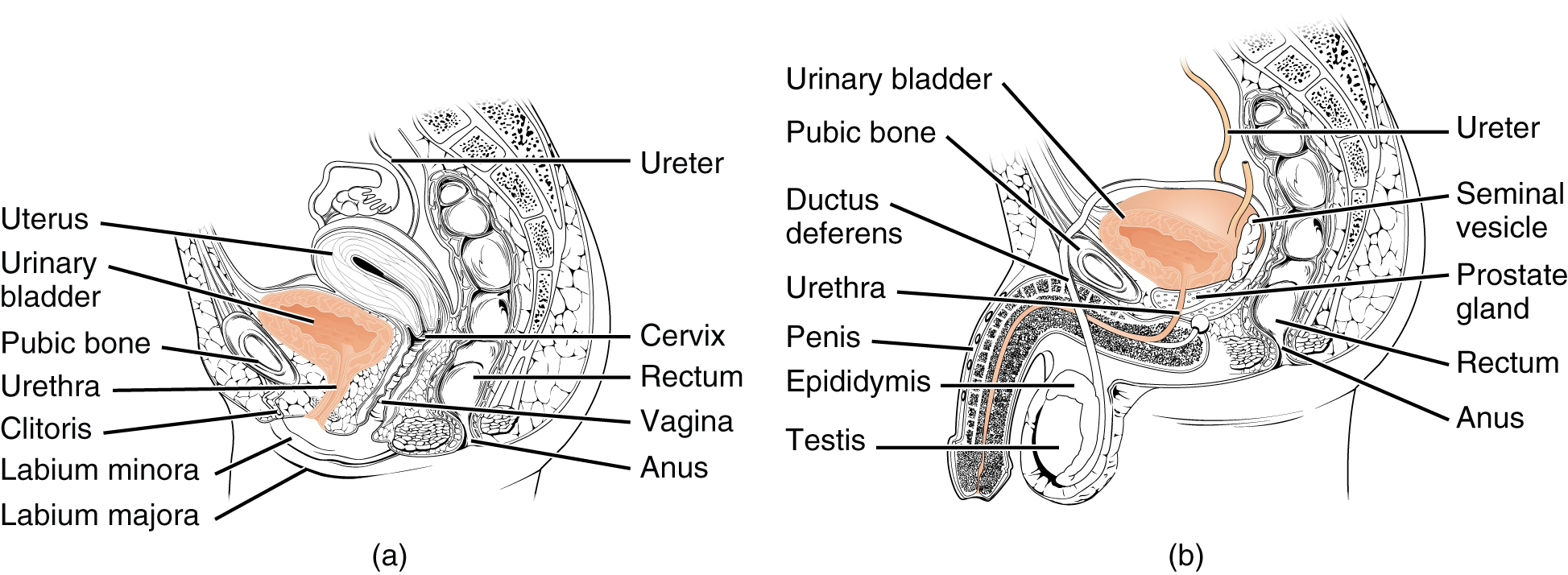
The female urethra (Figure 25.11a) is approximately 3 to 4 cm long and it passes from the urinary bladder to the external urethral orifice. The external urethral orifice is embedded in the anterior vaginal wall, inferior to the clitoris, superior to the vaginal opening, and medial to the labia minora. Its short length is less of a barrier to fecal bacteria than the longer male urethra and is the best explanation for the greater incidence of urinary tract infections (UTIs) in women. Voluntary control of the external urethral sphincter is a function of the pudendal nerve. It arises in the sacral region of the spinal cord, traveling via the S2–S4 nerves of the sacral plexus.
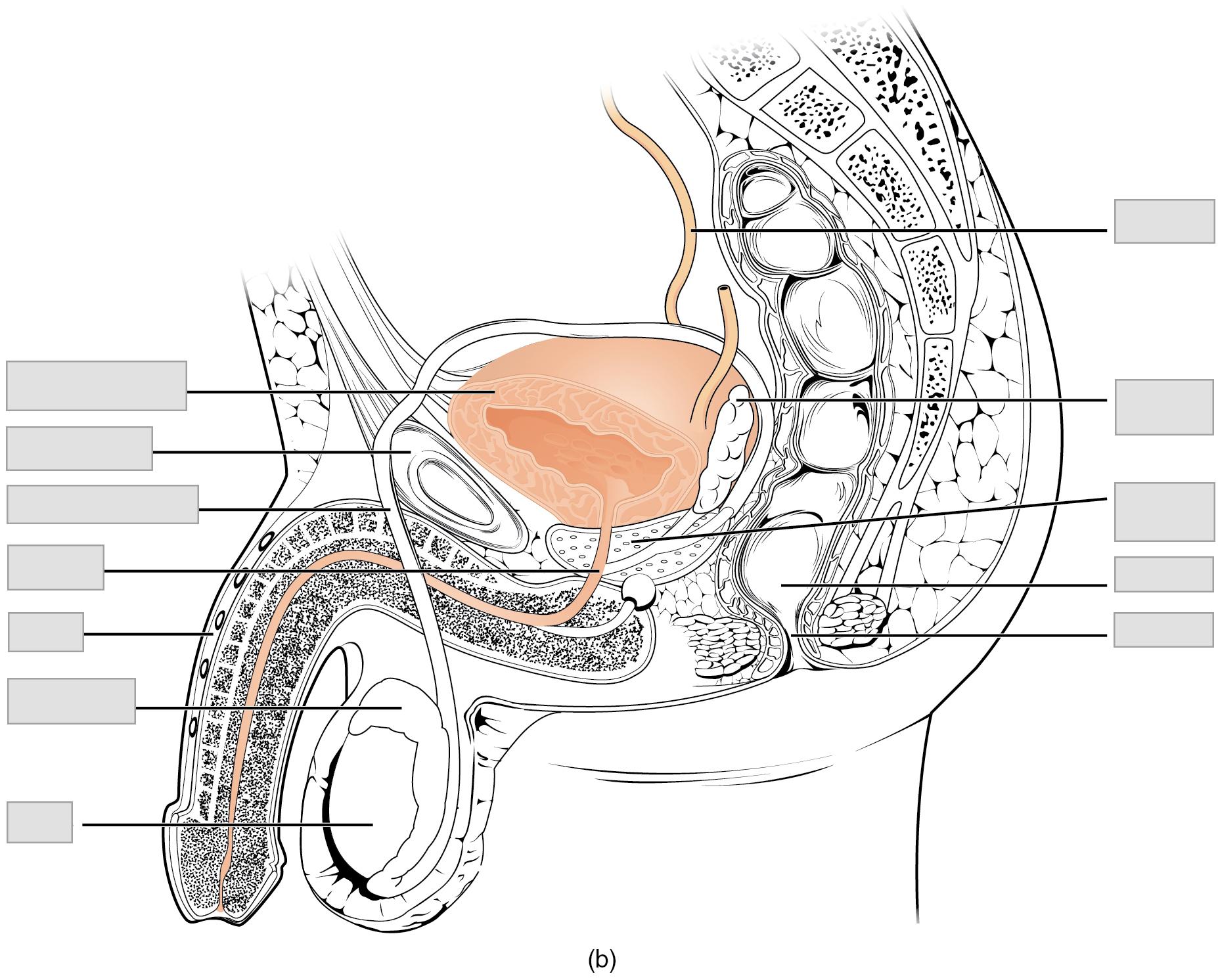
Male Urethra
The male urethra (Figure 25.11b) is much longer than the female urethra, averaging 20 cm in length. After leaving the urinary bladder, the urethra passes through the prostate gland, which is positioned inferior to the bladder, before passing below the pubic symphysis. It is divided into three regions: the prostatic urethra, the membranous urethra, and the spongy (penile) urethra. The first region of the urethra is the prostatic urethra and it passes through the prostate gland. During sexual intercourse, it receives sperm via the ejaculatory ducts and secretions from the seminal vesicles. Paired bulbourethral glands produce and secrete mucus into the urethra to buffer urethral pH during sexual stimulation. The mucus neutralizes the usually acidic environment and lubricates the urethra, decreasing the resistance to ejaculation. The prostatic urethra continues as the membranous urethra, which passes through the deep muscles of the perineum, where it is invested by the overlying urethral sphincters. Finally, the spongy urethra exits at the tip (external urethral orifice) of the penis, after passing through the erectile tissue (corpus spongiosum) of the penis. Mucous glands are found along much of the length of the urethra, ultimately helping to protect the urethra from the extreme pH of urine. Innervation is the same in both males and females.
PHYSIOLOGY
Introduction
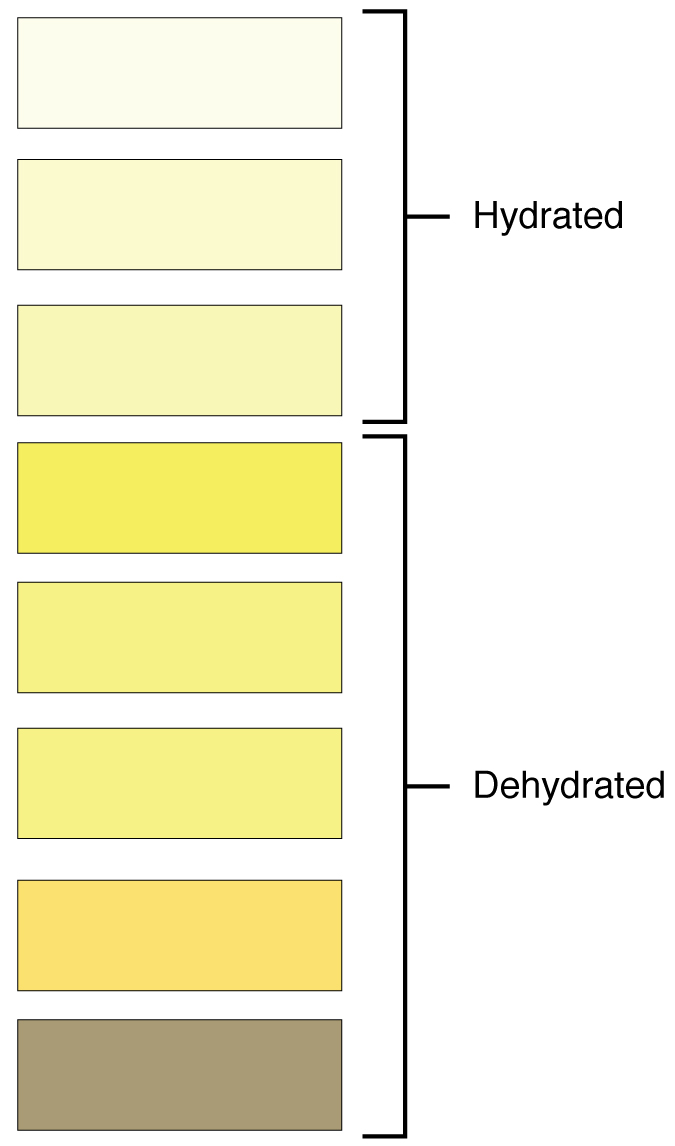
Urine is formed through the purification of plasma by glomerular filtration, tubular absorption, and secretion. The characteristics of the urine change, depending on influences such as water intake, exercise, environmental temperature, nutrient intake, and other factors. Some of the characteristics such as color and odor are rough descriptors of your state of hydration. For example, if you exercise or work outside, and sweat a great deal, your urine will turn darker and produce a slight odor, even if you drink plenty of water (Figure 25.12). Athletes are often advised to consume water until their urine is clear. This is good advice; however, it takes time for the kidneys to process body fluids and store it in the bladder. Another way of looking at this is that the quality of the urine produced is an average over the time it takes to make that urine. Producing clear urine may take only a few minutes if you are drinking a lot of water or several hours if you are working outside and not drinking much. In a normal, healthy individual, about 0.6 – 2.5 L of urine may be produced daily.
The color, clarity, and components of urine provide clues to the health and function of the kidneys and the body in general. The color of urine is determined mostly by the breakdown products of red blood cell destruction. The “heme” of hemoglobin is converted by the liver into water-soluble forms that can be excreted into the bile and indirectly into the urine. This yellow pigment is urochrome. Some foods (ex. beets, berries, or rhubarb), as well as some vitamins and drug therapies may alter the color of one’s urine. Dehydration may produce darker, more concentrated urine that may also possess the slight odor of ammonia. Most of the ammonia produced from protein breakdown is converted into urea by the liver, so ammonia is rarely detected in fresh urine. The strong ammonia odor you may detect in bathrooms or alleys is due to the breakdown of urea into ammonia by bacteria in the environment. About one in five people detect a distinctive odor in their urine after consuming asparagus; other foods such as onions, garlic, and fish can impart their own aromas! These food-caused odors are harmless though. While freshly voided urine is usually clear, it will become cloudy upon standing due to bacterial growth. Persistently cloudy (turbid) urine may indicate an infection. The waste products of metabolism (CO2, urea, uric acid, creatinine, NaCl, ammonia) are all normal constituents of urine. However, the presence of substances like albumin, glucose, or ketones, or changes in pH or urine output are key factors in identifying renal diseases or other metabolic disorders.
Various tests (both physical and chemical) have been developed for routine urinalysis. Some of these tests and their procedures are described below (tests for pH, specific gravity, glucose, protein, and ketones). Recently, the dipstick method has been developed to replace many of these individual tests, and is commonly used in most doctors’ offices. These test strips can not only detect many substances (ex. blood, bilirubin, protein, ketones, pH, glucose, and nitrites), but also their relative amounts.
pH
Freshly voided urine usually has a pH around 6.0, but the pH of normal urine samples can range from 4.7 – 7.5. Urine pH is highly influenced by a person’s diet. A high-protein diet often results in acidic urine, while a vegetable-rich diet results in more alkaline urine. The pH is also subject to diurnal fluctuations. Urine samples that are 24 hours old or older gradually become more alkaline due to the bacterial breakdown of urea. Urine that is consistently acidic is indicative of metabolic or respiratory acidosis, methanol poisoning, or metabolic disorders such as phenylketonuria. At the other end of the spectrum, production of consistently alkaline urine is a sign of metabolic or respiratory alkalosis or a urinary tract infection. It can also result from urine retention in the bladder, anemia, alkaline therapy, or obstructing gastric ulcers.
Ketones
Ketones are intermediary products of fat metabolism and are not usually present in urine in any detectable amount. Finding ketones in the urine suggests that the body is using fat as an energy source in preference to glucose. Conditions leading to insufficient carbohydrate reserves will cause elevated levels of acetoacetic acid, acetone, and beta hydroxybutyric acid in the blood and urine, also known as ketonuria. Ketonuria can be brought on by hypothermia, dietary imbalances (starvation or inadequate carbohydrate intake), diabetes mellitus, or genetically or chemically-induced metabolic disorders. Diabetes mellitus is the most common disorder associated with urine ketones. Progressive ketosis, a state of raised ketone levels, can lead to coma and death.
Proteins
Due to their large size, protein molecules are usually restricted to the glomerular capillaries during the filtration process in the nephron. This means that only trace amounts of protein should be found in a normal urine, approximately 10 mg / 100 mL (dL) in a random sample. However, under certain physiological and pathological conditions, increased levels of proteins can be detected in the urine. Pathologic albuminuria is found in cases of glomerular damage, febrile diseases, anemia, hypertension, and toxemia of pregnancy. Excessive protein ingestion, excessive muscular exertion, prolonged exposure to cold and acute abdominal diseases may lead to a condition known as physiologic albuminuria.
Glucose
Under normal conditions, urine will also contain only trace amounts of glucose (≤ 30 mg per 100 mL of urine). When glucose levels exceed this, the condition is known as glucosuria. This is found in cases of diabetes mellitus, pregnancy, excess stress, renal tubule damage, or brain damage. The renal threshold for glucose is about 160 mg/100 mL. In cases of glucosuria, blood glucose levels will exceed this amount and as a result, the excess glucose cannot be absorbed by the kidneys and it will “spill” into the urine. Incidentally, excess Vitamin C (ascorbic acid) contamination of the urine (> 400 mg/L) can give a false positive result for this test.
Specific Gravity
Specific gravity is a measure of the quantity of solutes per unit volume of a solution and is traditionally easier to measure than osmolarity. Urine will always have a specific gravity greater than pure water (water = 1.00) due to the presence of solutes. Distilled water is generally used as a reference for calibrating a urine hydrometer and determining the specific gravity of urine samples. Normally, the specific gravity of a urine sample is between 1.015 and 1.025, however, normal samples can vary anywhere from 1.002 – 1.030. As the amount of dissolved solid in a urine solution increases, so does the specific gravity. The production of consistently dilute urine (specific gravity < 1.015) results in a condition called hyposthenuria. This state is usually indicative of conditions such as chronic nephritis, diabetes insipidus, or cardiovascular problems. Urine which is consistently concentrated (specific gravity > 1.030) results in hypersthenuria. This condition is indicative of such disorders as acute nephritis and diabetes mellitus.
Pre-Laboratory Questions
- Where are the kidneys located within the body?
a. abdomen
b. anterior abdominal wall
c. anterior to parietal peritoneum
d. posterior to parietal peritoneum
- Urine comes out of the body through this
a. ureter
b. urethra
- Where does filtration take place within the nephron?
a. renal corpuscle
b. proximal convoluted tubule
c. distal convoluted tubule
d. collecting duct
- Trace the pathway that urine would take once it is produced in the renal tubules to when it is released through the process of urination (micturition).
a. papillary duct → minor calyx → major calyx → renal pelvis →
ureter → urinary bladder → urethra
b. papillary duct → major calyx → minor calyx → renal pelvis →
ureter → urinary bladder → urethra
c. papillary duct → renal pelvis → minor calyx → major calyx →
ureter → urinary bladder → urethra
d. papillary duct → ureter → minor calyx → major calyx → renal pelvis → urinary bladder → urethra
- What is the correct composition of the urine?
a. 90% water/10% solutes
b. 95% water/5% solutes
c. 80% water/20% solutes
d. 85% water/15% solutes
Exercises
- Exercise 1 The kidney (optional)
- Exercise 2 Blood supply to the kidney (optional)
- Exercise 3 Pig or sheep kidney dissection
- Exercise 4 Histology of the kidney
- Exercise 5 The ureter
- Exercise 6 The urinary bladder (optional)
- Exercise 7 The urethra (optional)
- Exercise 8 Urinalysis
Exercise 1 The Kidney (optional)
Required Materials
- The Urinary Tract poster
- Kidney, Nephron, Glomerulus model
- Torso model
Procedure
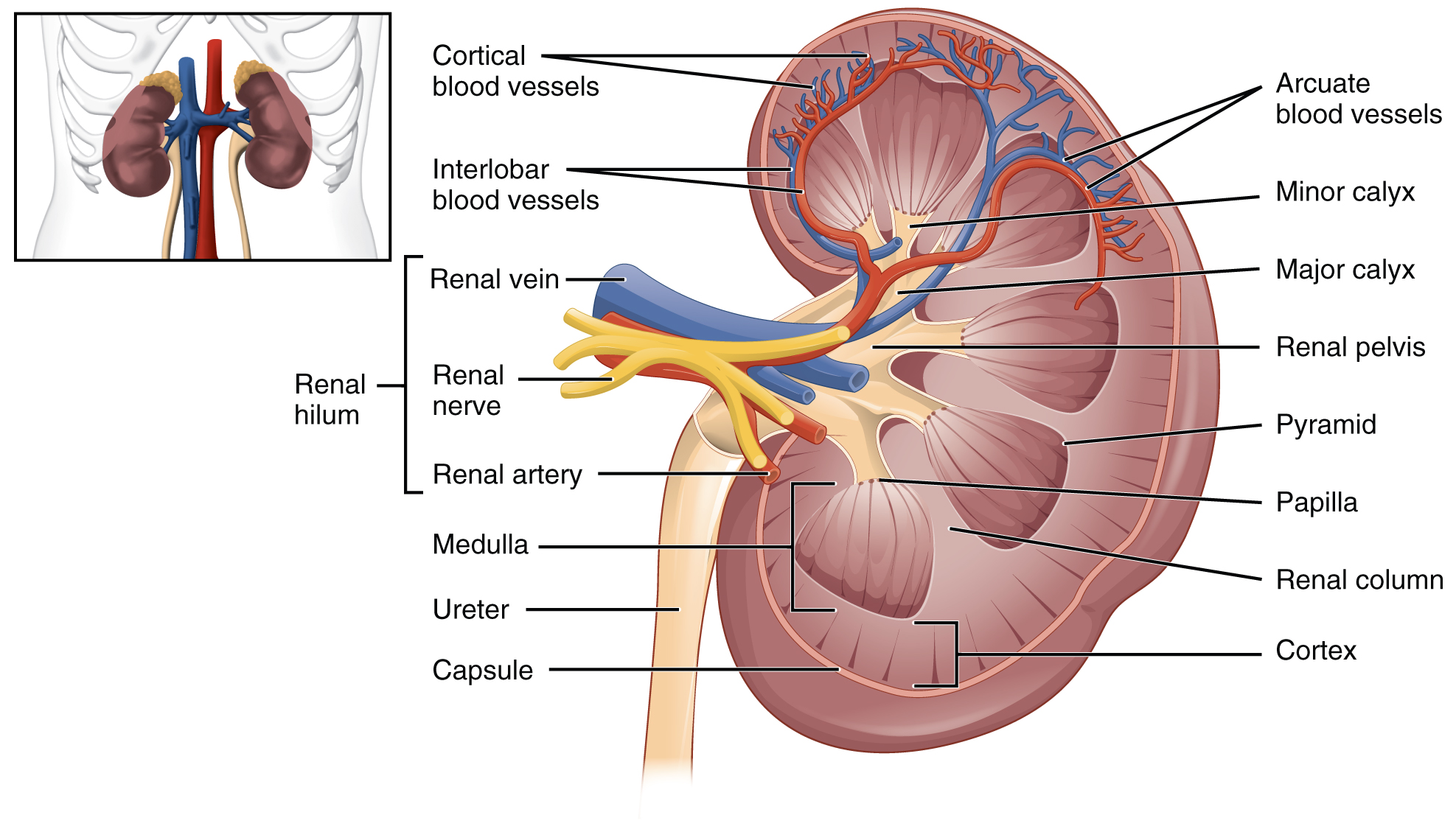
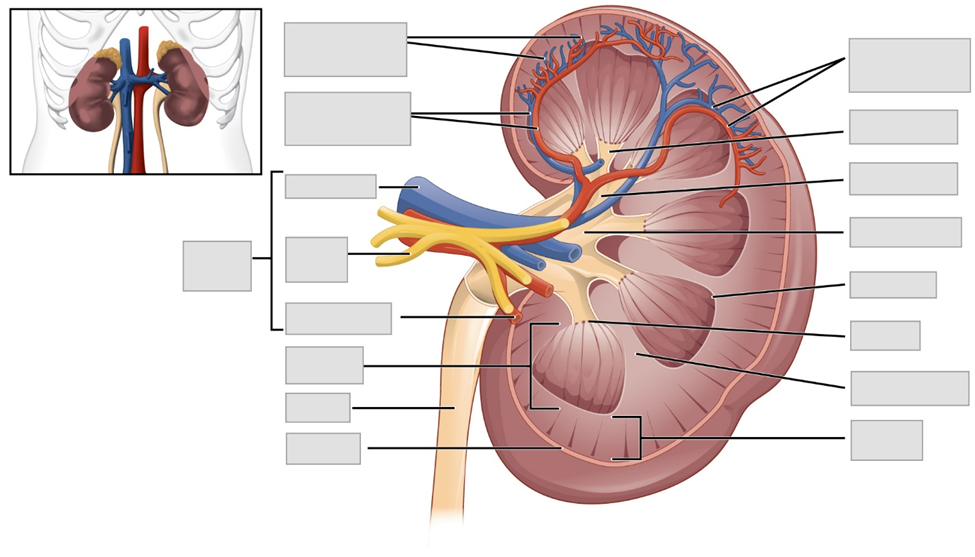
- Use the models and posters to observe the following features of the kidney and urinary system. Label these features on the image given below.
| Arcuate Blood Vessels | Pyramid |
| Capsule | Renal Artery |
| Cortex | Renal column |
| Cortical Blood Vessels | Renal Hilum |
| Interlobar Blood Vessels | Renal Nerve |
| Major calyx | Renal pelvis |
| Medulla | Renal Vein |
| Minor calyx | Ureter |
| Papilla |
Exercise 2 Blood supply to the kidney (optional)
Required Materials
- The Urinary Tract poster
- Kidney, Nephron, Glomerulus model
- Torso model
Procedure
- Use the models and posters to observe the following features of the blood vessels of the kidney and urinary system. Label these features on the image given below.
| Afferent Arteriole | Interlobular Artery |
| Arcuate Artery | Interlobular Vein |
| Arcuate Vein | Peritubular Capillaries |
| Efferent Arterioles | Renal Artery |
| Glomerulus | Renal Vein |
| Interlobar Artery | Segmental Artery |
| Interlobar Vein |
Exercise 3 Pig or sheep kidney dissection
Required Materials
- Preserved pig or sheep kidney dissection specimen
- Dissection tray
- Dissection instruments
- Gloves
- T-pins for labeling
- Labeling tape
- Marker pens
Procedure
1.Obtain one dissection specimen per group. Place in tray.
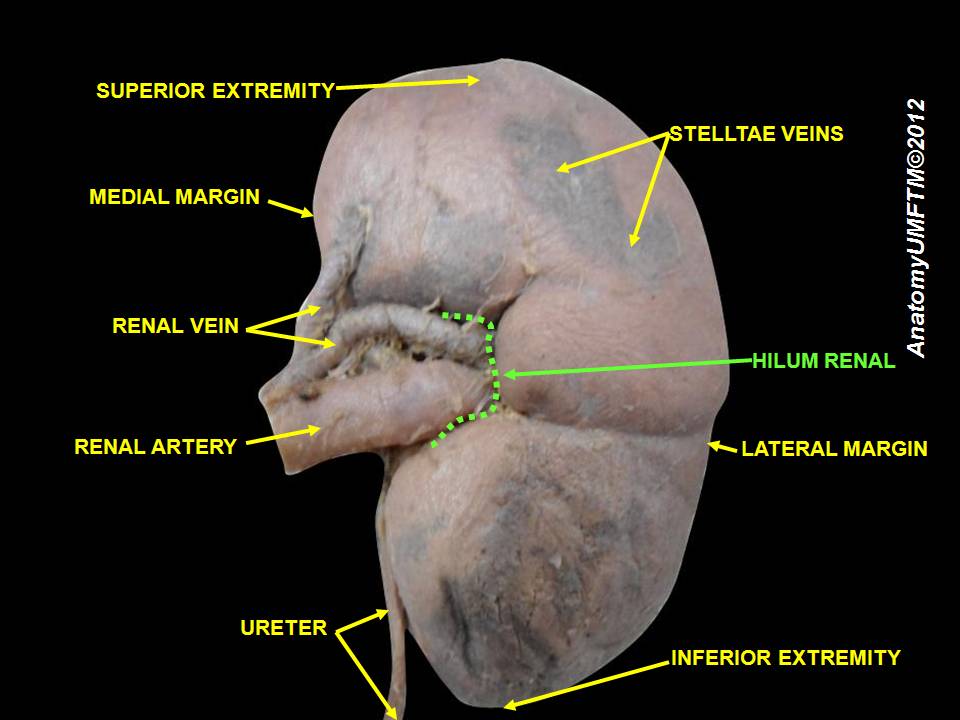
2. Observe and label the superficial structures indicated below. To label, use the T-pins and place tape on them you can write on. Label as many of the features shown in the figure below on your specimen. Take a picture of the labeled specimen and paste it below.
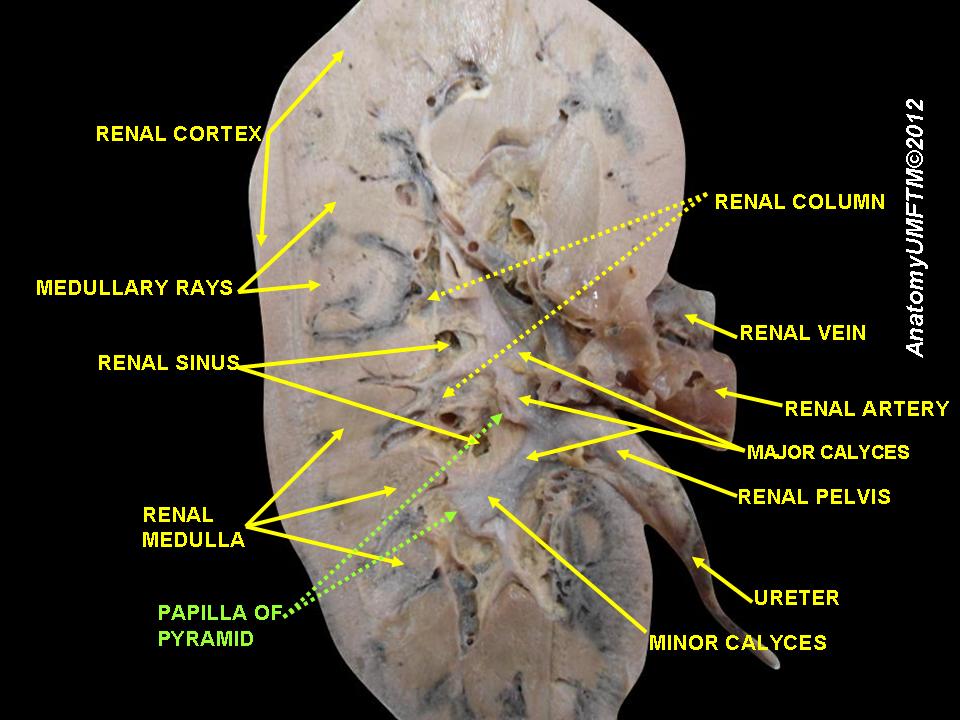
3. Using the image below as a guide and a sharp instrument (scalpel, knife) dissect the pig or sheep kidney. Observe and label the internal structures indicated on the dissected section below. To label, use the T-pins and place tape on them you can write on. Label as many of the features shown in the figure below on your specimen. Take a picture of the labeled specimen and paste it below.
Exercise 4 Histology of the kidney
Required Materials
- Compound microscope
- Microscope lens paper
- Microscope lens cleaning solution
- Microscope immersion oil
- Slide of Mammal Kidney Median
Procedure
- Obtain a slide of the kidney and place it on the microscope stage
- Bring the structures into focus at low power and scan the regions for the cortex and medulla.
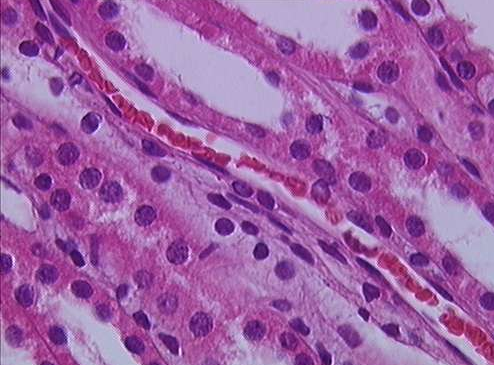
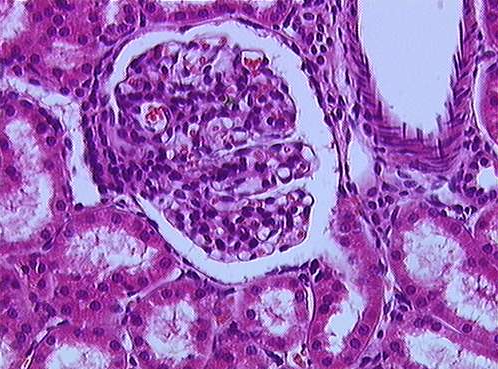
- Next, change to high power and examine the glomerulus and other structures.
- Identify
-
- Basement membrane
- Brush border
- Distal convoluted tubule
- Glomerulus
- Macula densa
- Proximal convoluted tubule
- Collecting duct
- Nephron loop
- Sketch the histological structures as seen through the microscope in the space provided below and label the parts shown above. Provide one low magnification and one high magnification sketch in the space below.
Exercise 5 The ureter
Required Materials
- Compound microscope
- Microscope lens paper
- Microscope lens cleaning solution
- Microscope immersion oil
- Slide of Human Ureter
Procedure
- Obtain a slide of the ureter and place it on the microscope stage
- Bring the structures into focus at low power and scan the regions for the various parts of the ureter. Next, change to high power and examine the structures
- Identify
-
- Adventitia
- Lumen
- Smooth muscle layer
- Sketch the histological structures of the ureter as seen through the microscope in the space provided below and label the parts shown above. Provide a low magnification and a high magnification sketch.
Exercise 6 The urinary bladder (optional)
Required Materials
- The Urinary Tract poster
- Kidney, Nephron, Glomerulus model
- Torso model
Procedure
- Use the models, posters and Figure 25.10 in Background to observe the following features of the urinary bladder. Label these features on the image given below.
| Detrusor muscle | Submucosa |
| External urethral sphincter | Transitional epithelium |
| Internal urethral sphincter | Ureteral openings |
| Lamina propria | Ureter |
| Peritoneum |
Exercise 7 The urethra (optional)
Required Materials
- The Urinary Tract poster
- Kidney, Nephron, Glomerulus model
- Male Pelvis Model
- Female Pelvis Model
- Torso model
Procedure
- Use the models, posters and Figure 25.11 in Background to observe the following features of the female and male pelvis. Label these features on the images given below.
| Anus | Pubic bone |
| Cervix | Rectum |
| Clitoris | Seminal vesicle |
| Ductus deferens | Testis |
| Epididymis | Ureter |
| Labium majora | Urethra |
| Labium minora | Urinary bladder |
| Penis | Uterus |
| Prostate gland | Vagina |
Exercise 8 Urinalysis
Required Materials
- Sterile urine collection containers
- Marker or wax pencil
- 4-factor urinary test strips (glucose, ketone, protein, pH)
- Four disposable pipets
- Test tube rack
- Artificial urine samples from each of four “patients” and one normal
- Beakers
- Graduated cylinder
- Gloves
Procedure
- You should work in groups of 2-4 to complete this activity. Make sure that you thoroughly clean your workspace before and after the activity to ensure that you do not contaminate your samples or leave a mess behind.
- In this exercise, you will use artificial urine samples to analyze the dissolved and suspended components. You also have the option of using your own urine, collected with the sterile cups with lid and handled carefully.
- Obtain five clean cups. Using the marker or wax pencil, label each tube with the name or number of each artificial urine sample. If you are using your own urine, you can leave it in the sterile cup with lid until use.
- Measure 10 mL of each “simulated” or fake urine sample.
- Record your observations of the physical characteristics of each sample (color, clarity and smell) in Table 1, below.
- For color: urine is normally a pale yellow. This is due to a pigment called urochrome, which is a metabolic product of hemoglobin breakdown. High levels of vitamin B may cause urine to artificially be bright yellow, while low fluid intake may cause urine to be a deep yellow color.
- For clarity: fresh urine is typically clear or slightly cloudy. Urine turbidity (clarity) is often affected when red blood cells, white blood cells, epithelial cells, bacteria, mucus, lipids, or crystals. Crystals generally make urine cloudy or opaque.
- For smell: urine should have a faint, but characteristic odor. Consumption of certain food, such as asparagus, may produce compounds, leading to stronger odors.
- Once all of your observations are recorded, keep your samples and continue below.
- To determine the chemical composition of the urine samples (fake or real) dip an unused 4-factor urinary test strip into each urine sample. Use a new strip for each sample.
- Using the comparison chart provided on the bottle of strips, identify and record the pH, ketones, protein, and glucose amount in Table 2 below.
Analysis
Table 1. Physical Characteristics of Urine
| Sample | Color | Clarity | Smell |
| Sample #1 | |||
| Sample #2 | |||
| Sample #3 | |||
| Sample #4 | |||
| Sample #5 | |||
| Your sample |
Table 2. Chemical Composition of Urine
| Sample | pH | Glucose | Protein | Ketones |
| Sample #1 | ||||
| Sample #2 | ||||
| Sample #3 | ||||
| Sample #4 | ||||
| Sample #5 | ||||
| Your sample |
Analysis Questions
- Based on your observations, which of the 5 samples is normal?
- What are some abnormalities you observed in each of the other 4 “patient” samples?
Post-laboratory Questions
Post-laboratory questions
- The smallest functional unit of the kidney is known as what?
a. glomerular capsule
b. nephron
c. Bowman’s capsule
d. renal calyx
- The renal corpuscle is comprised of what two components?
a. glomerulus
b. nephron
c. Bowman’s capsule
d. renal calyx
- Name the four regions of the renal tubule:
a. proximal convoluted tubule
b. loop of Henle
c. distal convoluted tubule
d. collecting duct
e. glomerular capsule
- What are the components of the juxtaglomerular apparatus?
a. juxtaglomerular cells
b. nephron
c. Bowman’s capsule
d. macula densa
- Body’s “water-treatment plant” is composed of the following
a. kidneys
b. ureter
c. urinary bladder
d. urethra
e. adrenal glands
- Urine leaves the body through the _________ (urethra/ureter)
- The _______ (right/left) kidney is positioned at a slightly higher level than the other
- The following enzyme is released by the kidney
a. angiotensin
b. angiotensinogen
c. renin
d. erythropoietin
- The thick structure that covers the kidney
a. connective tissue
b. capsule
c. Bowman’s capsule
d. renal corpuscle
- The following hormone is released by the kidney
a. angiotensin
b. angiotensinogen
c. renin
d. erythropoietin
- __________ gland is located on the superior aspect of the kidney
a. pineal
b. thymus
c. adrenal
d. thyroid
- The _________ (renal column/renal papilla) is the extension of the renal cortex projecting into the renal medulla
- The correct number of major renal calyx is
a. 10-20
b. 1
c. 100
d. 2-3
- The minor calyx extends into the
a. renal pyramid
b. renal cortex
c. renal column
d. renal pelvis
- The ureter extends into the kidney as
a. renal pelvis
b. major calyx
c. minor calyx
d. renal pyramid
e. renal capsule
- The components of nephron is
a. afferent arteriole
b. renal corpuscle
c. efferent arteriole
d. renal tubule
- The urinary bladder is located in the __________ (abdominal/pelvic) cavity
- Trigone is a part of
a. nephron
b. urinary bladder
c. ureter
d. urethra
- Components of male urethra include
a. prostatic urethra
b. membranous urethra
c. trigone
d. spongy urethra
- Components of net glomerular filtration pressure are
a. blood pressure
b. glomerular hydrostatic pressure
c. plasma colloid osmotic pressure
d. capsular hydrostatic pressure
- Filtrate from the glomerulus goes into the
a. ureter
b. renal pelvis
c. renal tubule
d. juxtaglomerular apparatus
- Each kidney receives about __________ % of the cardiac output
a. 12.5
b. 1.5
c. 5
d. 25
- The liquid that comes out of renal corpuscle is the __________ (filtrate/urine)
- __________% of the filtrate from the glomerulus will be reabsorbed in the renal tubules
a. 25
b. 55
c. 99
d. 72
- Trace the correct order of urinary tubule from the renal corpuscle to the renal papilla.
a. proximal convoluted tubule → distal convoluted tubule → nephron loop → collecting
duct → renal papilla
b. proximal convoluted tubule → collecting duct → nephron loop → distal convoluted
tubule → renal papilla
c. proximal convoluted tubule → renal papilla → distal convoluted tubule → collecting
duct → nephron loop
d. proximal convoluted tubule → nephron loop → distal convoluted tubule → collecting
duct → renal papilla
