
Sleep-disordered breathing encompasses various respiratory disturbances that disrupt normal ventilation and oxygenation during sleep.
Two common forms – hypopnea and hypoventilation – share some characteristics but have important differences in their underlying mechanisms and impacts on health.
What is Hypopnea?
Hypopnea refers to an abnormal shallow breathing event lasting at least 10 seconds with a 30% or greater reduction in airflow, accompanied by an oxygen desaturation of 3-4% or an arousal from sleep.
Hypopneas occur due to partial collapse and obstruction of the upper airway during sleep, commonly associated with obstructive sleep apnea. The partial blockage results in reduced airflow and depth of breathing.
What is Hypoventilation?
Hypoventilation indicates an overall reduction in respiratory minute ventilation leading to inadequate oxygenation and/or carbon dioxide elimination.
It involves breathing at an abnormally slow rate and decreased depth resulting in low oxygen (hypoxemia) and increased carbon dioxide (hypercapnia) levels.
Hypoventilation occurs commonly with obesity, chronic pulmonary disorders like COPD, and neuromuscular diseases impacting respiratory muscles. It can happen while awake or during sleep.
Characteristics of Hypopneas vs. Hypoventilation
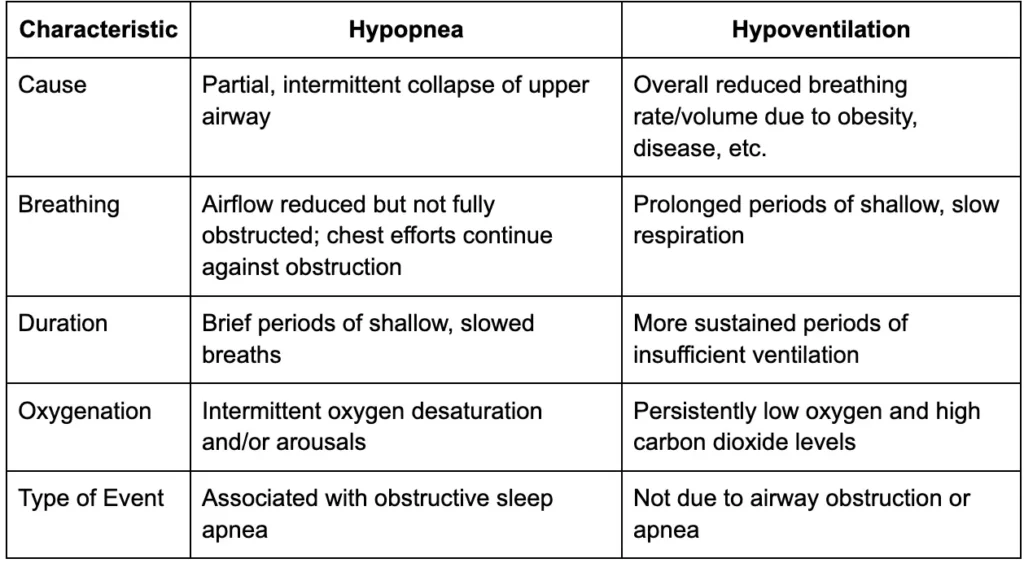
Causes and Risk Factors
Hypopnea Risk Factors
- Anatomical susceptibility: Having anatomical features like enlarged tonsils and adenoids, a small or receding jaw/chin, or a deviated septum/nasal obstruction make the airway more prone to collapse during sleep.
- Obesity: Excess weight deposits fat around the neck and throat, putting pressure on the airway and raising collapsibility during sleep respiration efforts. Even modest weight gain amplifies risk.
- Alcohol: Drinking especially before bed relaxes throat muscles and sedates the brain’s respiratory control center, diminishing the defenses against airway closure events.
- Sleeping pills: Sedatives like benzodiazepines and Z-drugs suppress the brain’s responsiveness, including its drive to keep the airway open during natural breathing pauses in sleep cycles.
Hypoventilation Risk Factors
- Lung disease: Conditions reducing lung capacity/compliance such as COPD or pulmonary fibrosis diminish the respiratory muscles’ ability to drawing adequate air into the lungs.
- Neuromuscular disorders: Diseases weakening muscles involved in breathing raise the work of ventilation and risk of inadequate gas exchange and carbon dioxide retention.
- Obesity: Excess abdominal weight compresses the diaphragm and chest cavity, requiring greater work to inflate the lungs which can lead to underventilation.
- Hypothyroidism: An underactive thyroid slows the body’s metabolic rate and respiratory drive, minimizing carbon dioxide clearance from tissues and blood.
- Respiratory center disorders: Rare conditions directly impacting the brain nerve centers responsible for automatic breathing patterns can disrupt ventilation.
Diagnosing Hypopnea and Hypoventilation
The gold standard for diagnosing both hypopnea and hypoventilation is an overnight polysomnography (PSG) test. During a PSG, several parameters are continuously monitored to detect respiratory events:
Airflow
Nasal/oral thermistors or pneumotachography measure airflow at the nose and mouth. Reductions in airflow (but not complete cessation) indicate hypopneas.
Respiratory Effort
Analysis of chest and abdominal movement using respiratory inductance plethysmography or measurements of tracheal sounds differentiate between obstructive and central events based on respiratory effort.
Oxygen Saturation
Pulse oximetry records oxygen saturation levels in the blood via a probe on the finger. It identifies desaturations (drops in oxygen) associated with respiratory events.
End-tidal Carbon Dioxide (etCO2)
A nasal cannula or face mask samples exhaled air to measure etCO2 levels. Elevated etCO2 indicates hypoventilation due to retention of carbon dioxide.
In addition to the polysomnography, doctors may consider:
Symptoms
Patients often report symptoms like excessive daytime sleepiness, fatigue, insomnia, and morning headaches. However, symptoms alone cannot confirm or rule out either condition.
Arterial Blood Gas Analysis
During wakefulness, blood samples are analyzed for oxygen and carbon dioxide levels. Low oxygen or high carbon dioxide would indicate hypoventilation.
Multiple Sleep Latency Test (MSLT)
Measures how quickly a person falls asleep during different daytime nap opportunities to objectively assess daytime sleepiness.
By comprehensively evaluating airflow, respiratory effort, oxygen levels, carbon dioxide levels, associated symptoms and objective tests, doctors can definitively diagnose hypopnea, hypoventilation or both conditions.
Symptoms of excessive sleepiness, morning headaches, and fatigue may prompt further respiratory testing. However, symptoms alone are not definitive.
Effects on Oxygenation and Ventilation
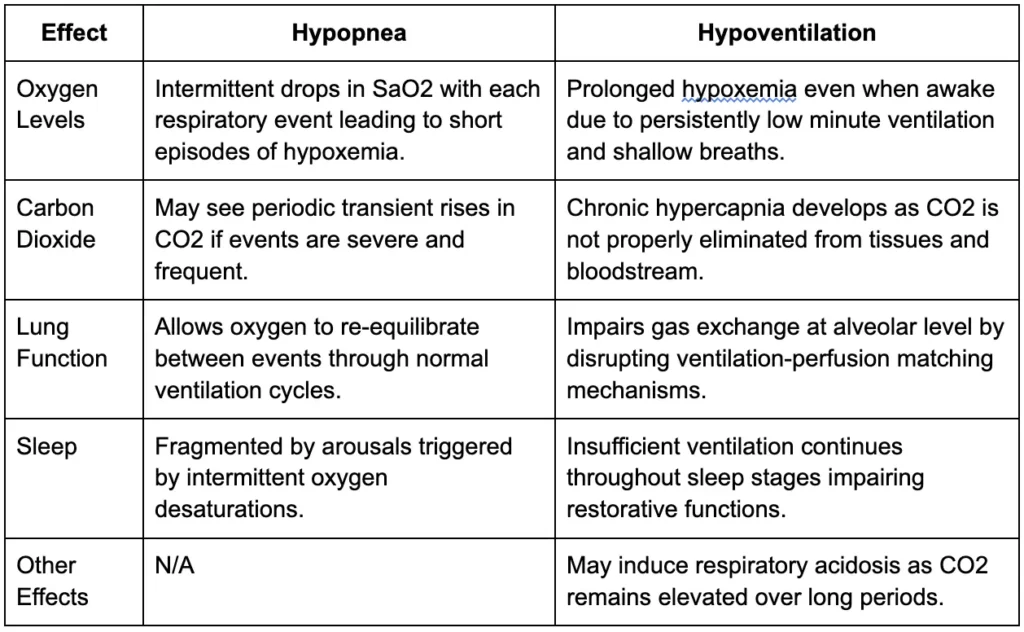
In summary, hypopneas trigger intermittent disruptions to oxygenation while hypoventilation induces prolonged hypoxemia and hypercapnia. The condition’s effects on lung gas exchange and sleep quality also differ based on event duration and respiratory patterns
Health Consequences
If untreated, both hypopnea and hypoventilation can result in:
- Hypertension and pulmonary hypertension
- Heart failure and arrhythmias
- Cognitive dysfunction and memory impairment
- Insulin resistance and glucose intolerance
- Fatigue, headaches and sleepiness
Hypoventilation may also progress to respiratory failure requiring intubation.
Treatment Considerations
NightLase®
An innovative new laser therapy called NightLase® offers a gentle, non-invasive treatment to improve sleep quality by reducing the effects of these common sleep disorders.
NightLase® utilizes a superficial Er:YAG laser to create a tightening effect in the soft tissues of the mouth and throat. The laser stimulates new collagen production, which firms up the soft palate and shrinks enlarged tonsils and tongue tissue. This tightening serves to open the airway, allowing for easier breathing during sleep. It also decreases vibration in the soft tissues, significantly reducing snoring sounds.
The NightLase® laser is extremely gentle and safe. No anesthesia is required, and patients report little to no pain during the procedure. The treatment sessions are performed in a dental or medical office and take less than an hour. A series of three to five treatments, spaced two weeks apart, is recommended to achieve the best results.
One of the key benefits of NightLase® is its lasting effects. Studies show improvements in sleep quality, snoring volume and apnea symptoms can persist for up to a year after treatment. And the non-invasive nature of the therapy means it can be repeated annually to maintain results.
For the many who struggle with poor sleep due to sleep apnea or bothersome snoring, NightLase® presents an excellent alternative to more invasive surgeries or devices. This innovative laser therapy is giving patients a pathway to better sleep and improved health.
Hypopnea
Positive Airway Pressure (PAP): CPAP/BiPAP acts as a pneumatic splint keeping the airway propped open, reducing respiratory effort requirements and events.
- Oral Appliances: Mandibular advancement devices reposition the lower jaw and tongue improving airway patency during sleep.
- Upper Airway Surgeries: For those with structural abnormalities, procedures like UPPP, tonsillectomy or tracheostomy can widen the airway.
- Weight Loss: Losing even a small amount of pounds through diet and exercise lessens neck fat depositions compressing the airway.
Hypoventilation
- Bronchodilators: Medications widen bronchioles easing airflow and reducing work of breathing, especially for those with lung disease.
- Lung Function Therapies: Chest physical therapy helps clear secretions and optimizes gas exchange through postural drainage and percussion.
- BiPAP: Delivered with an added backup rate feature to mechanically assist ventilation efforts by pushing more air into the lungs.
- Supplemental Oxygen: High-flow nasal cannula provides enriched oxygen improving saturation while still stimulating the respiratory center.
- Treating Causes: For those with disorders impacting muscles or respiratory control, addressing the underlying pathology optimizes ventilation.
For patients with both obstruction and hypoventilation, combination therapy is often required. The key is to accurately identify the condition through polysomnography.
Conclusion
Hypopnea represents intermittent reductions in airflow with sleep apnea, while hypoventilation indicates sustained global decreases in ventilation. Though they share effects on oxygenation, their distinct mechanisms have implications for diagnosis and tailored management. Treating the specific type of disordered breathing is crucial.