
 Share on Facebook
Share on Facebook
 Share on LinkedIn
Share on LinkedIn
 Share by Email
Share by Email
 Print
Print
Slideshow
-

Case #1
-

Case #2
Case #1
A 40-year-old Hispanic man presents with a bilateral rash on his arms that has been present for several weeks. The patient says the rash itches and appears to be getting worse. On examination, the patient has ill-defined erythematous patches and papules on his dorsal and ventral forearms, bilaterally. The patient has a past medical history of hypertension and diabetes. The patient works as a dishwasher in a restaurant and recently switched jobs approximately 2 months ago.
Case #2
A 35-year-old white man presents with a bilateral rash on his legs. The patient says the rash has been present for several months and itches intensely. The patient has been applying copious amounts of over-the-counter hydrocortisone. He says this helps a little but does not get rid of the rash. On examination, the patient has multiple circular, erythematous papular patches on his legs. The patient has no other relevant medical history.
Case #1: Contact dermatitisContact dermatitis is a localized inflammatory skin disease caused by the host's reaction to exogenous irritants or allergens.1 It is further divided into irritant contact dermatitis (ICD) and allergic contact dermatitis (ACD). ICD results from direct cytotoxic effect...
Submit your diagnosis to see full explanation.
Case #1: Contact dermatitis
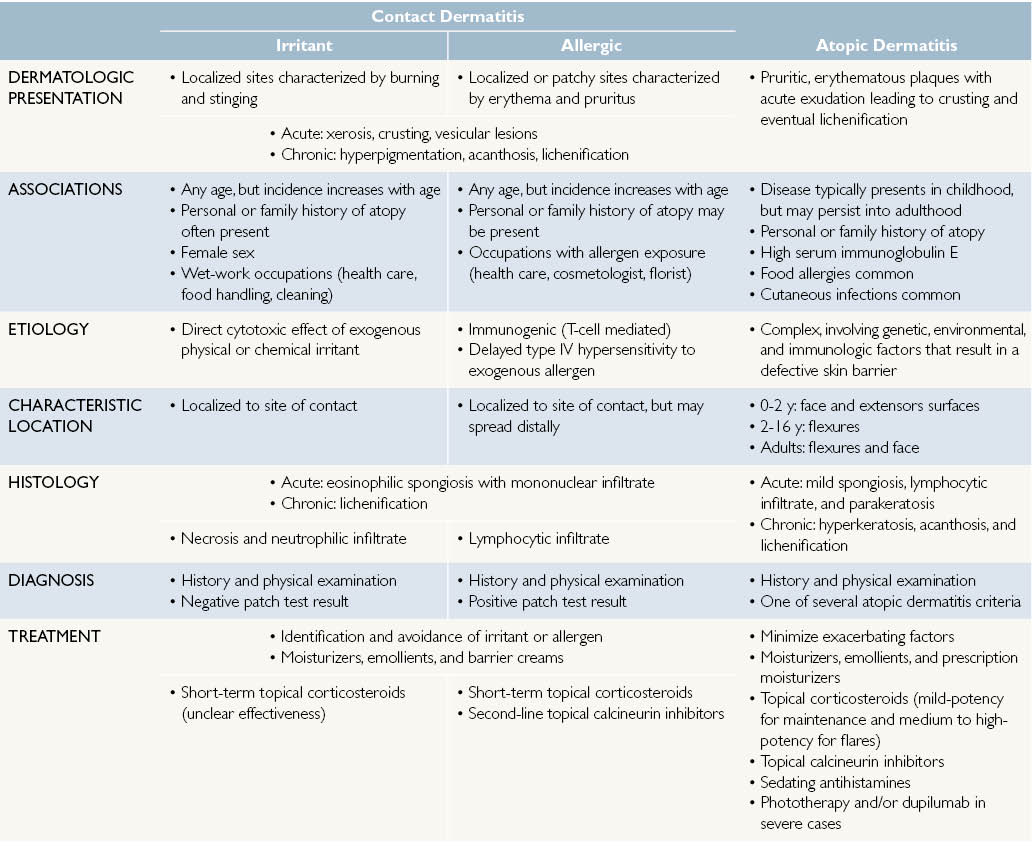
Contact dermatitis is a localized inflammatory skin disease caused by the host’s reaction to exogenous irritants or allergens.1 It is further divided into irritant contact dermatitis (ICD) and allergic contact dermatitis (ACD). ICD results from direct cytotoxic effect of a physical or chemical irritant upon initial or repeated contact. This reaction results in localized cytokine release,2 but does not induce an adaptive T-cell response. It typically presents with localized burning and stinging within 48 hours after exposure.3 In contrast, ACD is an allergic reaction in an individual previously sensitized to the allergen.1 Re-exposure to the allergen activates memory T cells to elicits a delayed (type IV) hypersensitivity reaction at the cutaneous site of contact.1,4 ACD typically presents with localized or patchy areas of erythema and pruritus.3
ICD is the most prevalent form of contact dermatitis and represents approximately 80% of occupational dermatitis.1 Individuals in professions necessitating prolonged exposure to wet conditions, such as food handling, healthcare professions, and cleaning, are particularly at risk for ICD.5 Mechanistically, prolonged exposure to water results in swelling of the stratum corneum, lipid disruption, and increased skin permeability.6 Other risk factors for ICD include female sex5 and history of atopic dermatitis.7 Common irritants include water, solvents, detergents, cleaning agents, and physical factors such as extreme temperature, humidity, or pressure.5
ACD has an estimated prevalence of 15% to 20%,8 and represents 20% of contact dermatitis cases.1 Risk factors for ACD include occupation, age,8 and (potentially) history of atopic dermatitis.9 Those in high-risk occupations include healthcare workers, florists, construction workers, and cosmetologists, due high exposure to allergic agents such as latex, resins, acrylics, and hair dyes.10 Although individuals of all ages are affected by ACD11, older adults show higher rates of ACD, likely due to increased exposure to potential allergens.12 Common allergens include poison ivy, metals, topical antibiotics, preservatives, paraphenylenediamine, hair care products, fragrances, and rubber.13,14
The pathogenesis of contact dermatitis begins with exposure to an exogenous substance. In ICD, this exposure results in epidermal barrier disruption that increases skin permeability and transepidermal water loss. In response to cellular damage, keratinocytes release cytokines that ultimately recruit mononuclear and polymorphonuclear cells.15 This process results in symptoms within a few hours of irritant exposure. In contrast, ACD results in the activation of antigen-specific helper T cells.16 During the sensitization phase of ACD, dendritic cells migrate from the skin to lymph nodes and present captured antigens to effector T cells. Once activated, T cells proliferate, migrate to cutaneous tissues, and are primed to stimulate antigen-specific inflammation. The initial sensitization process take a few weeks to develop, but results in rapid inflammation with 48 hours upon re-exposure to the allergen.
Clinically, patients with acute contact dermatitis present with localized erythema, dry skin, edema, oozing, crusting, and vesicular lesions.1 As the disease progresses, scales, hyperpigmentation, and acanthosis may appear.16Chronic cases often present with lichenification and fissuring.1
Histologic changes in acute contact dermatitis include eosinophilic spongiosis and mononuclear infiltration.14 ACD cases may also present with lymphocytic infiltrate. Necrosis, neutrophilic infiltrate, and acanthosis may also be seen in severe cases of acute ICD. Histology of chronic stages may show chronic spongiotic dermatitis and lichenification.
Diagnosis of contact dermatitis requires a detailed history of exposures, and occupational and recreational risk factors. Clinical features of ICD include (1) rapid postexposure onset of symptoms, (2) localized symptoms of pain, burning, and stinging, (3) erythematous, scalded epidermis or chronic features of hyperkeratosis, scaling, or lichenification, and (4) a negative patch test result.17 In contrast, ACD may present will a slower onset of symptoms dominated by pruritus and greater potential for diffuse or patchy distribution and/or spreading beyond the original contact site.1 In addition to a thorough history and physical examination, patch testing can be used to diagnose ACD.16 For this test, dilutions of chemicals are applied to the patient’s back and evaluated after 2 to 3 days. A positive test result is indicative of ACD; however, this diagnosis cannot be ruled out with a negative test result, because not all potential allergens are represented. For both ICD and ACD, skin biopsy is not a routine diagnostic technique. The differential for contact dermatitis includes other forms of dermatitis (such as atopic dermatitis), psoriasis, seborrheic dermatitis, and fungal infection.
Treatment of contact dermatitis begins with identification of the offending agent and subsequent avoidance of that irritant or allergen.1 If symptoms persist, treatment turns to limiting inflammation. First, barrier creams are used to limit irritant diffusion. Second, moisturizers or emollients limit water loss and restore epidermal barrier function. These should be applied several times a day and especially after bathing. Topical corticosteroids are an effective treatment for ACD in the short term, but should not be used extensively. Evidence is unclear if topical corticosteroids are effective for treatment of ICD. Topical calcineurin inhibitors, such as pimecrolimus cream or tacrolimus ointment, are second-line treatment options for ACD.
The patient in this vignette was diagnosed with ICD. The patient was advised to wear full-arm gloves while washing dishes and to avoid excessive contact with soaps and water. With the use of gloves, his rash resolved within 1 month.
Case #2: Atopic dermatitis (eczema)
Atopic dermatitis, commonly known as eczema, is a chronic pruritic inflammatory disease of endogenous origin.19 It typically manifests in children, but it may affect adults as well. Symptoms include pruritus, erythema, dry skin, exudate, crusting, and lichenification. Patients often present with a family history of atopy, the tendency to develop allergic diseases such as atopic dermatitis, asthma, and allergic rhinitis, and elevated serum immunoglobulin E (IgE) levels.19
Atopic dermatitis is more common in children than adults. Nearly 11% of American children are diagnosed with eczema.20 Most of these cases resolve; however, the disease may persist into adulthood.21 Persistence is associated with female sex, increased disease severity (higher levels of xerosis, pruritus, and impact on daily living), and age of onset between 6 and 11 years of age.22 During infancy, boys show a higher prevalence of atopic dermatitis; interestingly, however, this prevalence switches to girls after puberty.23 Prevalence is also higher in developed countries1 and in patients with a family history of atopy.23
The cause of atopic dermatitis is complex, involving a combination of genetic, environmental, and immunologic factors that result in a defective skin barrier. In healthy skin, the stratum corneum consists of layers of dead cells, corneocytes, within a matrix of ceramides, cholesterol, free fatty acids, and filaggrin breakdown products, namely natural moisturizer factor (NMF).24 Disruption of this protective barrier can lead to the excessive transepidermal water loss and increased susceptibility to microbial infection such as Staphylococcus aureus seen in atopic dermatitis.19,25 Loss-of-function mutations in the filaggrin gene result in defective barrier function and are associated with the development of atopic dermatitis.24 Reduced barrier function is also associated with unrestricted protease activity, abnormal tight junctions, microbes, and proinflammatory cytokines.25 Immune dysregulation has also been associated with atopic dermatitis. For example, the strong IgE response common to atopic dermatitis may be due to overexpression of type 2 helper T cells (Th2); however, the exact role of IgE is yet to be determined.26
Clinically, patients with acute atopic dermatitis present with erythematous, pruritic papules and serous exudate that crust with scratching.14,19 As the disease progresses, the skin becomes dry and scaly, and chronic stages are characterized by lichenification and hyperpigmentation.14 The typical presentation varies with age.19 Before 2 years of age, atopic dermatitis presents in acute stages on extensor surfaces, cheeks, and the scalp. In patients between 2 and 16 years, the disease typically presents in a flexural distribution, specifically the antecubital and popliteal fossae, neck creases, ankles, and wrists. During adulthood, atopic dermatitis becomes more localized, especially to flexures and often the face, and lichenification is common. Additional sites for adult eczema include the hand and eyelids. Histologically, acute atopic dermatitis presents with mild spongiosis, lymphocytic infiltrate, and parakeratosis.14 Later stages are characterized by hyperkeratosis, parakeratosis, and acanthosis. Serology typically shows elevated IgE levels and eosinophilia.
Diagnosis of atopic dermatitis relies upon patient history, clinical features, and morphology and distribution of skin lesions. Several diagnostic criteria have been created, namely the Hanifin and Raika criteria19 and the UK Working Party’s Diagnostic criteria for atopic dermatitis.27 The UK criteria defines atopic dermatitis as pruritic skin plus 3 of the following: (1) skin crease involvement, (2) history of asthma or hay fever, (3) dry skin within the past year, (4) symptoms before the age of 2 years, and (5) dermatitis of the flexural areas if >4 or dermatitis of the cheeks, forehead, or extensor surfaces if <4. Furthermore, several disease severity scales exist that assess factors such area of skin affected, amount of itching, impact on sleep, and impact on daily living.28 Skin biopsy is not a routine diagnostic measure.
The differential diagnosis for atopic dermatitis includes contact dermatitis, seborrheic dermatitis, and scabies.19 A patient with contact dermatitis presents with a history of irritant or allergen exposure and a localized inflammatory reaction. A patch test can be performed to determine a diagnosis of allergic contact dermatitis. Infants with seborrheic dermatitis present with greasy scales, salmon colored skin, and scalp involvement, and pruritus will not be a prominent symptom. Patients with scabies present with secondary eczematous changes in volar regions and skin folds. Detection of mites and eggs confirm a diagnosis of scabies.
No cure exists for atopic dermatitis; however, several treatment options exist for symptom management. All patients should minimize exacerbating factors such as overheating skin, prolonged bathing, low humidity environments, food allergens, emotional stress.25,29 It is also important to maintain skin hydration, particularly after bathing, through use of creams, ointments, and prescription moisturizers containing natural moisturizer factor and ceramide, natural components of the epidermal matrix.25,30 Topical anti-inflammatory agents are enlisted if symptoms persist.25 Acute flares are managed with medium- to high-potency corticosteroids, but for maintenance it is recommended to use low-potency corticosteroids, especially when treating children.25,31 In addition, topical calcineurin inhibitors, such as pimecrolimus cream or tacrolimus ointment, are nonsteroidal immunomodulators used to limit inflammation in patients older than 2 years.19,25 To promote sleep and control pruritic symptoms, antihistamines are used; however, efficacy is unclear.31 One study did show sedating antihistamines to be superior to nonsedating antihistamines at controlling pruritus.32 For severe cases of atopic dermatitis, the addition of phototherapy1 or dupilumab19,33 may be indicated. Dupilumab is a human monoclonal antibody targeting the interleukin 4 receptor-α. It was approved for use in March, 2017, for moderate to severe atopic dermatitis not sufficiently controlled with topical options, and has shown large improvements in controlling pruritic symptoms. Therapeutic trials assessing its safety and efficacy are ongoing in the pediatric population.34 In addition, anti-infective measures should be taken, as these patients have a higher risk of infection.25
The adult in this vignette was diagnosed with nummular eczema, a type of atopic dermatitis that commonly presents as circular eczematous patches in adults. The patient was prescribed triamcinolone, 0.1% ointment twice daily. The rash was completely clear at the patient’s 1-month follow-up.
McKenna Boyd, BA, is a medical student, Emma Weiss, BA, is a medical student, Christopher Rizk, MD, is a dermatology resident at the Baylor College of Medicine in Houston.
References
- Rashid RS, Shim TN. Contact dermatitis. BMJ. 2016;353:i3299.
- De Jongh CM, Verberk MM, Withagen CE, Jacobs JJ, Rustemeyer T, Kezic S. Stratum corneum cytokines and skin irritation response to sodium lauryl sulfate. Contact Dermatitis. 2006;54:325-333.
- Ahmed S. Contact dermatitis. InnovAiT. 2015;8:653-659.
- Saint-Mezard P, Berard F, Dubois B, Kaiserlian D, Nicolas JF. The role of CD4+ and CD8+ T cells in contact hypersensitivity and allergic contact dermatitis. Eur J Dermatol. 2004;14:131-138.
- Dickel H, Kuss O, Schmidt A, Kretz J, Diepgen TL. Importance of irritant contact dermatitis in occupational skin disease. Am J Clin Dermatol. 2002;3:283-289.
- Warner RR, Boissy YL, Lilly NA, et al. Water disrupts stratum corneum lipid lamellae: damage is similar to surfactants. J Invest Dermatol. 1999;113:960-966.
- Dickel H, Bruckner TM, Diepgen TL, Schmidt A. Impact of atopic skin diathesis on occupational skin disease incidence in a working population. J Invest Dermatol. 2003;121:37-40.
- Peiser M, Tralau T, Heidler J, et al. Allergic contact dermatitis: epidemiology, molecular mechanisms, in vitro methods and regulatory aspects. Current knowledge assembled at an international workshop at BfR, Germany. Cell Mol Life Sci. 2012;69:763-781.
- Thyssen JP, Linneberg A, Engkilde K, Menné T, Johansen JD. Contact sensitization to common haptens is associated with atopic dermatitis: new insight. Br J Dermatol. 2012;166:1255-1261.
- Mowad CM, Anderson B, Scheinman P, Pootongkam S, Nedorost S, Brod B. Allergic contact dermatitis. J Am Acad Dermatol. 2016;74:1029-1040.
- Simonsen AB, Deleuran M, Johansen JD, Sommerlund M. Contact allergy and allergic contact dermatitis in children – a review of current data. Contact Dermatitis. 2011;65:254-265.
- Prakash AV and Davis MD. Contact dermatitis in older adults: a review of the literature. Am J Clin Dermatol. 2010;11:373-381.
- Wentworth AB, Yiannias JA, Keeling JH, et al. Trends in patch-testing results and allergen changes in the standard series: a Mayo clinic 5-year retrospective review (January 1, 2006 to December 31, 2010). J Am Acad Dermatol. 2014;70:269-275.
- Wu H, Brandling-Bennett HA, Harrist TJ. Noninfectious vesiculobullous and vesiculopustular disease. In: Elder DE, ed. Lever’s Histopathology of the Skin. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins;2015:237-240.
- Spiekstra SW, Toebak MJ, Sampat-Sardjoepersad S, et al. Induction of cytokine (interleukin-1alpha and tumor necrosis factor-alpha) and chemokine (CCL20, CCL27, and CXCL8) alarm signals after allergen and irritant exposure. Exp Dermatol. 2005;14:109-116.
- Kostner L, Anzengruber F, Guillod C, Recher M, Schmid-Grendelmeier P, Navarini AA. Allergic contact dermatitis. Immunol Allergy Clin North Am. 2017;37:141-152.
- Rietschel RL. Clues to an accurate diagnosis of contact dermatitis. Dermatol Ther. 2004;17:224.
- Boehncke W-H, Schön MP. Psoriasis. Lancet. 2015;386:983-994.
- Weidinger S, Novak NN. Atopic dermatitis. Lancet. 2016;387:1109-1122.
- Shaw TE, Currie GP, Koudelka CW, Simpson EL. Eczema prevalence in the United States: data from the 2003 National Survey of Children’s Health. J Invest Dermatol. 2011:131:67-73.
- Vinding GR, Zarchi K, Ibler KS, Miller IM, Ellervik C, Jemec GB. Is adult atopic eczema more common than we think?—a population-based study in Danish adults. Acta Derm Venereol. 2014;94:480-482.
- Kim JP, Chao LX, Simpson EL, Silverberg JI. Persistence of atopic dermatitis (AD): a systematic review and meta-analysis. J Am Acad Dermatol. 2016;75:681-687.
- Pyun BY. Natural history and risk factors of atopic dermatitis. Allergy Asthma Immunol Res. 2015;7:101-105.
- Sandillands A, Sutherland C, Irvine AD, McLean WH. Filaggrin in the frontline: role in skin barrier function and disease. J Cell Sci. 2009;122:1285-1294.
- Leung DY. New insights into atopic dermatitis: role of skin barrier and immune dysregulation. Allergol Int. 2013;62:151-161.
- Fallon PG, Sasaki T, Sandilands A, et al. A homozygous frameshift mutation in the mouse Flg gene facilitates enhanced percutaneous allergen priming. Nat Genet. 2009;41:602-608.
- Williams HC, Burney PG, Hay RJ, et al. The U.K. Working Party’s Diagnostic Criteria for Atopic Dermatitis. I. Derivation of a minimum set of discriminators for atopic dermatitis. Br J Dermatol. 1994;131:383-396.
- Eichenfield LF, Tom WL, Chamlin SL, et al. Guidelines of care for the management of atopic dermatitis. J Am Acad Dermatol. 2013;70:338-351.
- Langan SM, Bourke JF, Silcocks P, Williams HC. An exploratory prospective observational study of environmental factors exacerbating atopic eczema in children. Br J Dermatol. 2006;154:979-980.
- Miller DW, Koch SB, Yentzer BA, et al. An over-the-counter moisturizer is as clinically effective as, and more cost-effective than, prescription barrier creams in the treatment of children with mild-to-moderate atopic dermatitis: a randomized, controlled trial. J Drugs Dermatol. 2011;10:531-537.
- Strathie Page S, Weston S, Loh R. Atopic dermatitis in children. Aust Fam Physician. 2016;45:293-296.
- Nuovo J, Ellsworth AJ, Larson EB. Treatment of atopic dermatitis with antihistamines: lessons from a single-patient, randomized clinical trial. J Am Board Fam Pract. 1992;5:137-142.
- Beck LA, Thaci D, Hamilton JD, et al. Dupilumab treatment in adults with moderate-to-severe atopic dermatitis. N Engl J Med. 2014;371:130-139.
- Hamilton JD, Ungar B, Guttman-Yassky E. Drug evaluation review: dupilumab in atopic dermatitis. Immunotherapy. 2015;7:1043-1058.
QUESTION

