
 Share on Facebook
Share on Facebook
 Share on LinkedIn
Share on LinkedIn
 Share by Email
Share by Email
 Print
Print
Slideshow
-

Slide
A 60-year-old man presents with rapidly growing lesions on his face, trunk, axillae, flexural areas, and groin. The lesions appeared 3 months earlier in his perianal area and extended rapidly to other areas. Previously, he was treated with topical agents for atopic dermatitis and seborrheic dermatitis without improvement. Examination reveals disseminated violaceous papules and plaques on the face, trunk, axillae, and perianal area; some lesions were confluent and ulcerated. Yellowish-red to skin-colored papules are present on the scalp. He has no palpable lymphadenopathy or organomegaly.
Langerhans cell histiocytosis (LCH) is a rare inflammatory neoplasia characterized by the accumulation of clonal CD207-positive myeloid dendritic cells.1,2 It presents most commonly in infants and young children, with an estimated incidence of two to nine cases per million per...
Submit your diagnosis to see full explanation.
Langerhans cell histiocytosis (LCH) is a rare inflammatory neoplasia characterized by the accumulation of clonal CD207-positive myeloid dendritic cells.1,2 It presents most commonly in infants and young children, with an estimated incidence of two to nine cases per million per year, compared with the incidence rate in adults, which is one to two cases per million per year.1,2 In addition, LCH has a slight predominance in boys and men.1,2
LCH is differentiated into two major categories based on the extent of disease, according to the Reclassification Working Group of the Histiocyte Society: single system (SS-LCH), in which a single organ system is involved, and multisystem (MS-LCH), in which two or more organ systems are involved.2 The skin is the second most commonly involved organ in SS-LCH disease after bone.3 Although the pathogenesis is unclear, two main hypotheses exist.2 The first hypothesis is that LCH is an inflammatory reaction elicited by antigenic stimulation that causes a cytokine storm, and the second is that LCH is a neoplastic condition resulting from BRAF-V600E pathway overactivation.2
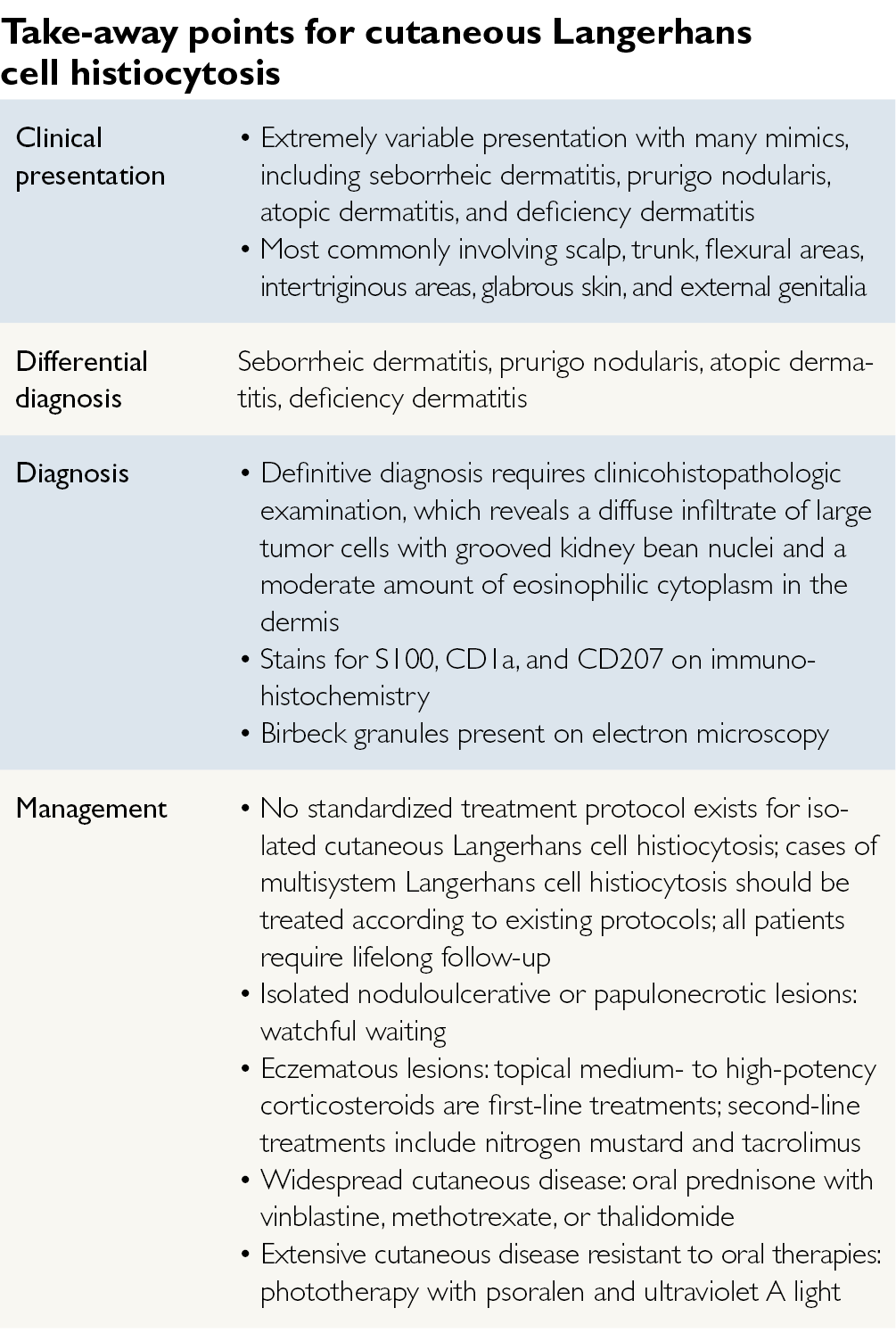
Skin lesions are a classic feature of LCH; however, cutaneous LCH lesions have a highly variable clinical appearance.1,2 Cutaneous LCH can present with yellowish-red to skin-colored papules or a seborrheic dermatitis-like eruption, commonly affecting the scalp, trunk, flexural, intertriginous areas, glabrous skin, and external genitalia.4-6 It can also present with erosive intertriginous eruptions, mimicking deficiency dermatitis and xanthomatous eruptions.3 Cutaneous LCH can also present with pruritic papules and nodules, mimicking prurigo nodularis.6 It can also present with petechiae, pustules, and vesicles, although this is less common.4 The presence of petechiae in the setting of seborrheic dermatitis should raise suspicion for LCH.4 In addition, the extent of cutaneous involvement may predict response to treatment.4 For example, patients younger than 3 months who have few and isolated lesions and patients with necrotic lesions and hypopigmented macules are more likely to have self-limited disease.4 However, patients with more extensive involvement, especially involving intertriginous and perineal areas, are less likely to have disease resolution without chemotherapy.4
Cutaneous LCH is diagnosed through a combination of clinicohistopathologic features and immunohistochemical stains for the S100 and CD1a proteins.4 Histopathologic findings of the lesions should show diffuse infiltration of large tumor cells with grooved kidney bean nuclei and a moderate amount of eosinophilic cytoplasm in the dermis.6 Equivocal cases can be diagnosed via electron microscopy demonstrating Birbeck granules or through immunohistochemical stains for Langerin (CD207), a monoclonal antibody that is associated with Birbeck granules.4 The differential includes seborrheic dermatitis, prurigo nodularis, eczema, and nutritional deficiency dermatitis, which may be distinguished from cutaneous LCH via histology and immunohistochemistry.
No standardized treatment protocols exist for isolated cutaneous LCH.7 In cases of MS-LCH, providers should follow LCH treatment protocols.2 In patients with isolated noduloulcerative or papulonecrotic cutaneous LCH lesions, providers should pursue watchful waiting because spontaneous healing may occur.2,7 For eczematous lesions, topical medium- to high-potency corticosteroids are the first-line treatment.2,7 Unfortunately, recurrence is common following treatment discontinuation.7 Other topical agents include nitrogen mustard and tacrolimus.2,7 In widespread cutaneous disease, systemic agents such as oral prednisone combined with vinblastine, methotrexate, and thalidomide are recommended.2,7 In extensive cutaneous disease resistant to oral therapies, phototherapy with psoralen and ultraviolet A light may be effective.2,7 All patients with cutaneous LCH require life-long follow-up because they may develop systemic involvement years after resolution of their skin lesions.4
In our case, because the patient was diagnosed with widespread cutaneous LCH, he was treated with a course of oral prednisone along with methotrexate. After this single course of therapy, the patient achieved nonactive disease, which continued through his 3-year follow-up visit.
Melinda Liu, BA, is a medical student and Maura Holcomb, MD, is a dermatology resident at Baylor College of Medicine in Houston.
References
- Simko SJ, Garmezy B, Abhyankar H, et al. Differentiating skin-limited and multisystem Langerhans cell histiocytosis. J Pediatr. 2014;165(5):990-996.
- Morren MA, Vanden Broecke K, Vangeebergen L, et al. Diverse cutaneous presentations of Langerhans cell histiocytosis in children: a retrospective cohort study. Pediatr Blood Cancer. 2016;63(3):486-492.
- Subramaniyan R, Ramachandran R, Rajangam G, Donaparthi N. Purely cutaneous Langerhans cell histiocytosis presenting as an ulcer on the chin in an elderly man successfully treated with thalidomide. Indian Dermatol Online J. 2015;6(6):407-409.
- Ng SS, Koh MJ, Tay YK. Cutaneous Langerhans cell histiocytosis: study of Asian children shows good overall prognosis. Acta Paediatr. 2013;102(11):e514-e518.
- Langerhans Cell Histiocytosis Treatment (PDQ®)-Patient Version. National Cancer Institute website. https://www.cancer.gov/types/langerhans/patient/langerhans-treatment-pdq Updated October 3, 2016. Accessed November 3, 2016.
- Sun WG, Zhong LS, Chen H. A case of adult generalized cutaneous Langerhans cell histiocytosis. Ann Dermatol. 2016;28(2):262-264.
- Dodd E, Hook K. Topical imiquimod for the treatment of childhood cutaneous Langerhans cell histiocytosis. Pediatr Dermatol. 2016;33(3):e184-e185.
- Park L, Schiltz C, Korman N. Langerhans cell histiocytosis. J Cutan Med Surg. 2012;16(1):45-49.
QUESTION

