


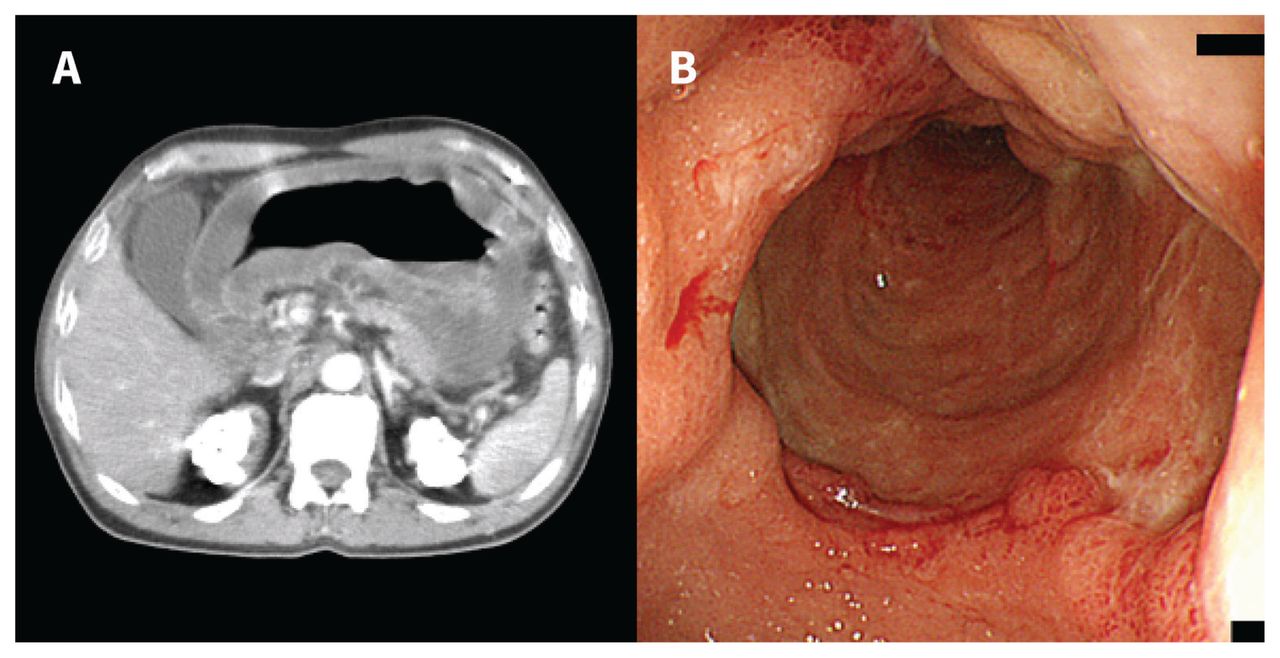
A 54-year-old man with type 2 diabetes presented to the emergency department via ambulance with a 3-day history of epigastric pain. He did not consume alcohol, had no previous abdominal complaints and was not on immunosuppressive medications. The patient had a fever and rebound tenderness in the periumbilical area. Blood tests showed an increased leukocyte count of 14.8 (normal 3.3–8.6) × 109/L and an elevated C-reactive protein level of 27.29 (normal < 0.14) mg/dL. Abdominal computed tomography (CT) showed diffuse circumferential thickening of the gastric wall (Figure 1A). We suspected phlegmonous gastritis and started the patient on meropenem and vancomycin. Upper gastrointestinal endoscopy showed diffuse erythema and edematous erosive changes in the gastric wall mucosa and purulent exudate (Figure 1B to 1D). Gastric aspirates and blood culture grew Streptococcus pyogenes. We diagnosed phlegmonous gastritis and transferred the patient to another hospital for a total gastrectomy. Gastric mucosa pathology showed extensive hemorrhagic necrosis in the lamina propria and severe edematous changes with neutrophil-dominant inflammatory cell infiltration in the submucosa. The patient was further treated with intravenous administration of ampicillin–sulbactam and was discharged home.
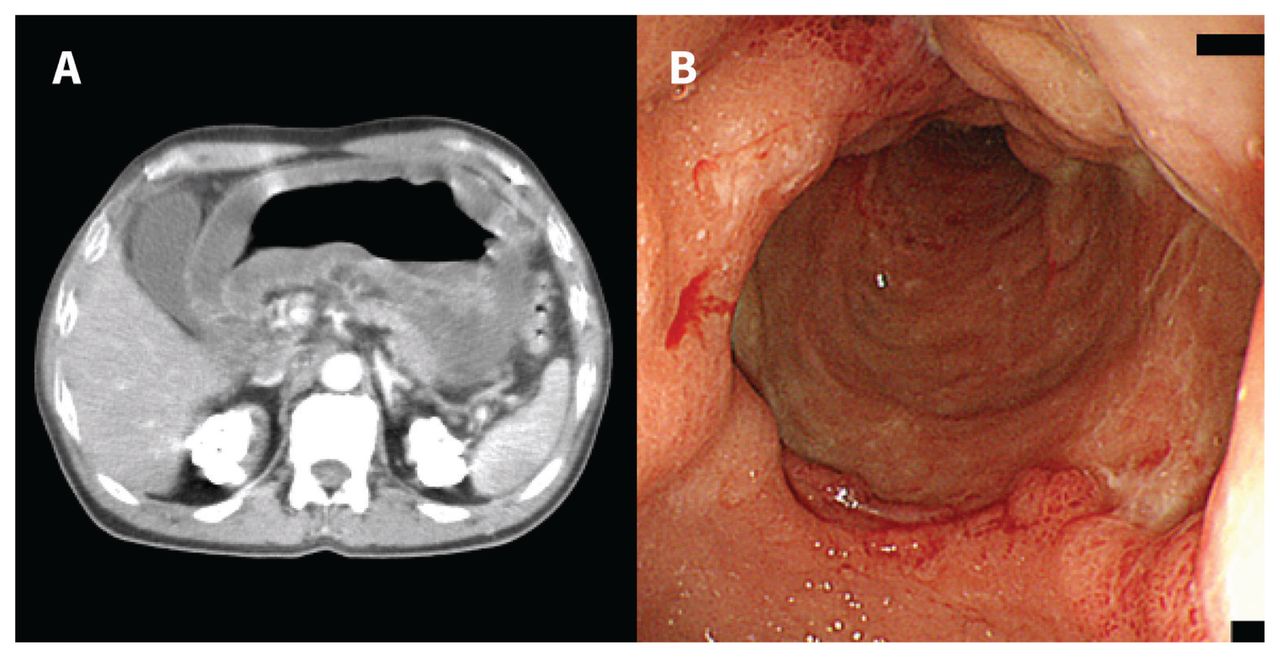
(A) Abdominal contrast-enhanced computed tomography scan of a 54-year-old man with phlegmonous gastritis showing diffuse circumferential thickening of the gastric wall. (B) Upper gastrointestinal endoscopy showed diffuse erythema and erosive edematous changes in the gastric wall mucosa and purulent exudate.
Phlegmonous gastritis is an acute pyogenic infection of the stomach. Underlying gastric diseases, chronic alcoholism and immunosuppression can be predisposing factors, but no underlying cause is identified in about 40% of patients.1 Streptococcus is the most common causative organism (about 70% of patients), whereas polymicrobial infection is implicated in nearly one-third of patients.1 The overall mortality is around 40%, which can be higher when diffuse stomach involvement is present.1 The symptoms of phlegmonous gastritis are nonspecific and include abdominal pain, nausea, vomiting and fever; thus, imaging plays a key role in diagnosis.1 A thickened gastric wall with or without an intramural low-density lesion on CT and fold thickening or extensive ulceration on endoscopy are typical findings.1,2 Peptic ulcer disease, gastric cancer and gastric lymphoma are the main differential diagnoses.1,2 For patients with diffuse disease, a combination of early gastrectomy with broad-spectrum antibiotics offers the best chance for survival.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
In this issue

{kind=link}
Article extras
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

