
What diagnosis would you suspect on the basis of the radiographic findings?
How do you read these images?
A 5-month-old girl is brought for evaluation of a neck swelling that had appeared 2 days earlier and had pro- gressively enlarged. She has also had cough and subjective fever. She has had no difficulty in breathing. The mother reports that the infant has had decreased appetite and limited neck movement on the right side for the past few hours. The patient has been otherwise healthy. Immunizations are up-to-date.
The infant is irritable and appears ill; temperature is 39.4oC (102.8oF), heart rate is 152 beats per minute, and respiration rate is 34 breaths per minute. She has a swelling on the right side of the neck with mild erythema and bilateral cervical lymphadenopathy. Throat examination reveals minimal erythema. The infant has decreased range of motion of the neck to the right, without torticollis.
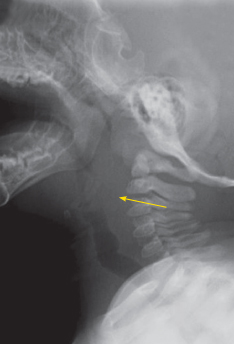
Anteroposterior and lateral views of the soft tissues of the neck are shown.
What diagnosis would you suspect on the basis of the radiographic findings?
A. Croup.
B. Epiglottitis.
C. Bacterial tracheitis.
D. Foreign body.
E. Retropharyngeal abscess.

The anteroposterior radiograph shows an asymmetric soft tissue swelling of the right lateral neck and mild tracheal buckling, which does not indicate mass effect. The lateral view shows widening of the retropharyngeal soft tissues; there is also prominence of the adenoids, with narrowing of the nasopharyngeal airway. Vertebral body alignment and epiglottis, aryepiglottic folds, and glottis appear normal. No foreign body is visible.
The retropharyngeal space extends from the base of the skull to the mediastinum. It is limited anteriorly by the posterior pharyngeal wall, laterally by the carotid sheath, and posteriorly by the prevertebral fascia. Infection of the retropharyngeal space most commonly occurs in children younger than 6 years as a complication of an upper respiratory tract illness. In older children, the infection usually results from penetrating pharyngeal trauma. Retropharyngeal cellulitis progresses to phlegmon to abscess and often represents a suppurative infection of the lymph nodes (the nodes of Rouvière) that occupy the space. These nodes atrophy before puberty and drain the nasopharynx, paranasal sinuses, and middle ear. Retropharyngeal abscess is predominantly caused by Streptococcus pyogenes, Staphylococcus aureus, and respiratory anaerobes.
Retropharyngeal abscesses in children can be life- threatening. The clinical presentation varies depending on the extent of disease. Cellulitis may present similarly to pharyngitis, whereas an abscess may present with signs of airway obstruction.
The initial step in the evaluation of an infant or child with a potential deep neck space infection is assessment of the airway for obstruction. When the diagnosis is unclear, plain radiographs may be necessary. In patients with a retropharyngeal abscess, the prevertebral space is wider than twice the anteroposterior measurement of the vertebral body: greater than 7 mm at C2 or greater than 14 mm at C6. The soft tissue inflammation (phlegmon or abscess) may also reverse the normal lordotic cervical spine curvature. When suspi- cion is high, a CT scan with intravenous contrast is the preferred study to assess abscess formation and extent of disease.1
Management includes empiric antibiotics with incision and drainage when the abscess causes imminent airway obstruction, is larger than 2 cm, or fails to resolve with antibiotic treatment alone. Exclusive antibiot- ic treatment is effective in only 25% of patients. Taking into consideration the growing prevalence of community-acquired methicillin-resistant S aureus, clindamycin is often the first-line agent of choice. Reported complications (aspiration pneumonia, carotid artery sheath or internal jugular vein infection, osteomyelitis, and necrotizing fasciitis) are rare with timely institution of therapy.
In this infant, an initial CT scan of the neck showed lymphadenopathy and phlegmon. A second CT scan, performed 3 days later because of persistent fever and neck swelling despite antibiotic treatment, showed ab- scesses in the retrophar yngeal and posterior cer vical spaces. Incision and drainage under anesthesia was performed with complete resolution.
1. Arora B, Mahajan P. Child with fever and neck pain. Consultant For Pediatricians. 2010;9:357-360.