CT Evaluation of Suspected Small Bowel Obstruction and Its EtiologyCT Evaluation of Suspected Small Bowel Obstruction and Its Etiology The Role of CT/CTA with Multiplanar and 3D Imaging in Diagnosis, Determining Cause, Identifying Complications and Guiding Patient Management: An Interactive Quiz |
Case 1: History of cirrhosis with palpable abdominal mass Patient with history of cirrhosis with longstanding abdominal mass, thought to be an umbilical hernia, who presents with acute abdominal pain, nausea, and vomiting 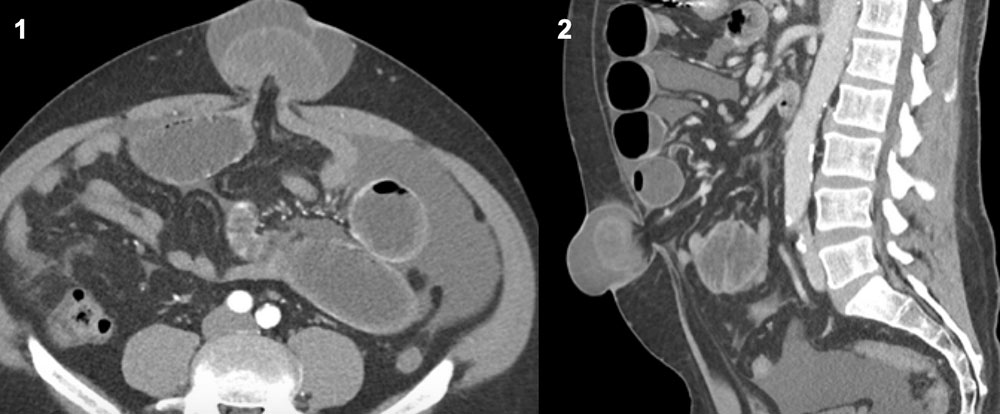 |
Case 1: Strangulated umbilical hernia Axial CECT in the arterial phase demonstrates a narrow neck umbilical hernia with incarcerated small bowel (red circle) with multiple loops of dilated small bowel proximal to the hernia (A). Sagittal reconstruction demonstrates the marked protrusion of the hernia (red circle) out of the anterior abdominal wall (B). 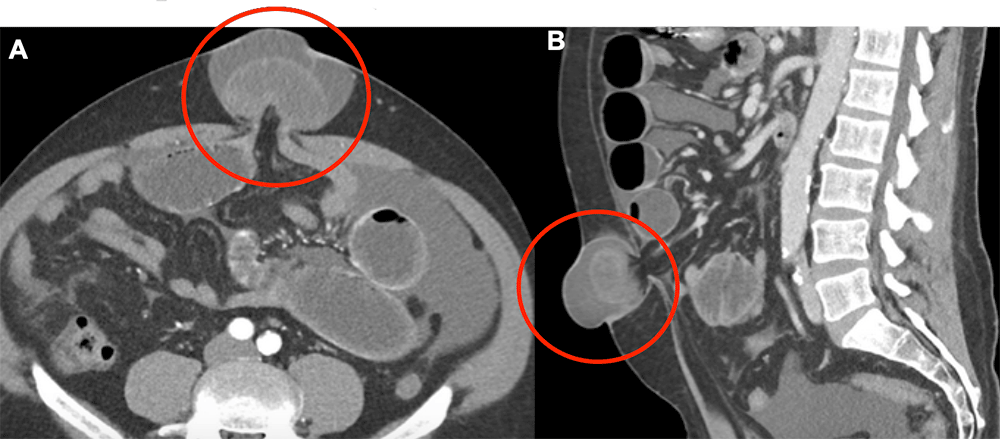 |
Case 2: Recent GYN laparoscopic surgery Patient status post laparoscopic bilateral salpingo-oophorectomy who presented with acute abdominal pain, distention, and vomiting on post-operative day 6.  |
Case 2: Incarcerated laparoscopic port site hernia Axial CECT in the arterial phase demonstrates a loop of bowel within the right lower quadrant soft tissue, at a trochar insertion site (red circle) with surrounding fat stranding (A, B). The stomach and small bowel are dilated proximal to the port site hernia (C). Pathology revealed necrotic ileum within the trochar hernia. 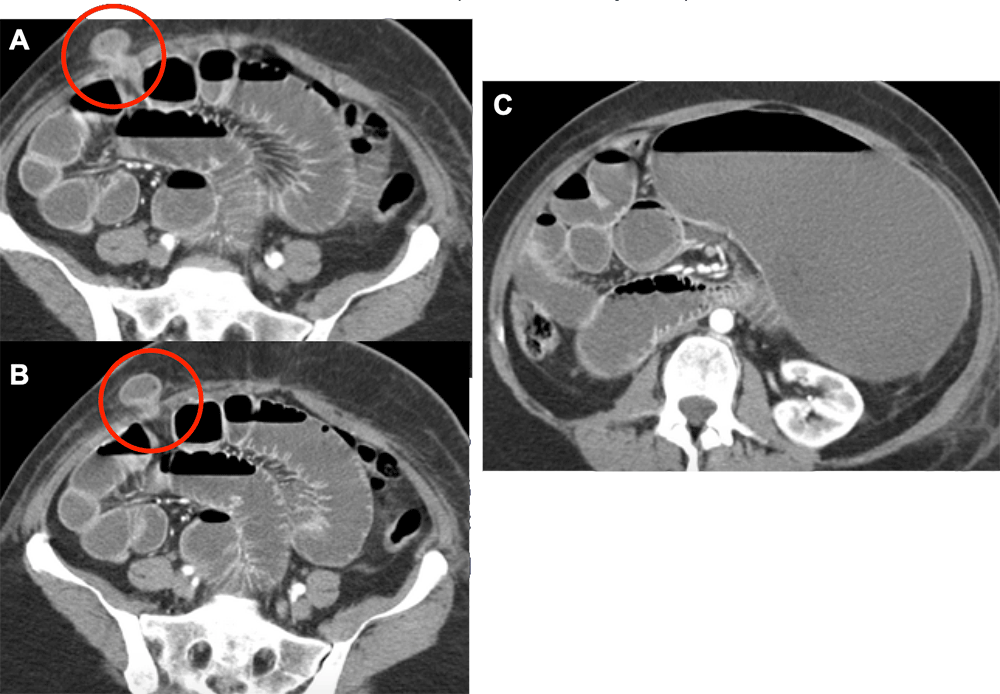 |
Case 3: Recent robotic prostatectomy Patient status post robotic prostatectomy who presents with acute onset abdominal pain and drainage from supraumbilical wound.  |
Case 3: Spigelian hernia Axial and coronal CECT in the arterial phase demonstrates small bowel herniating through a slit like defect in the right anterior abdominal wall (red arrow), consistent with a Spigelian hernia (A-C). Fluid filled, distended small bowel loops are proximal to the Spigelian hernia (B). Incidentally noted is a large amount of subcutaneous emphysema in the anterior abdominal wall (yellow arrows) related to the recent prostatectomy (A-C). Spigelian hernias are very rare comprising only 0.12% of all abdominal wall hernias. 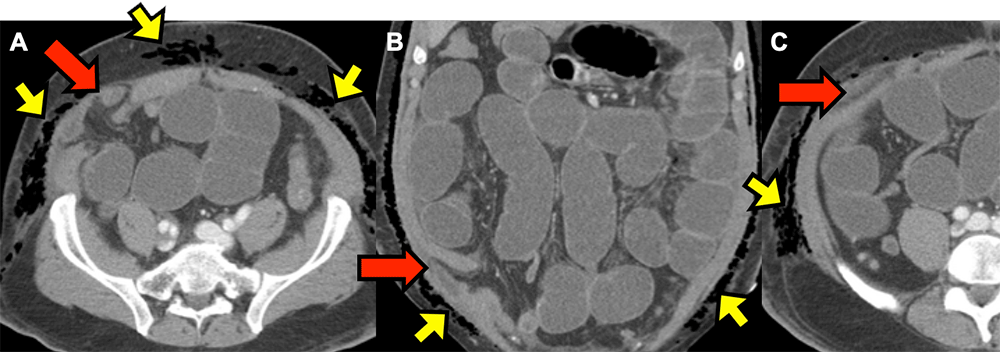 |
Case 4: History of primary biliary cirrhosis Patient with primary biliary cirrhosis who presents with progressive abdominal pain over 10 months with acute nausea and vomiting the week prior to admission. 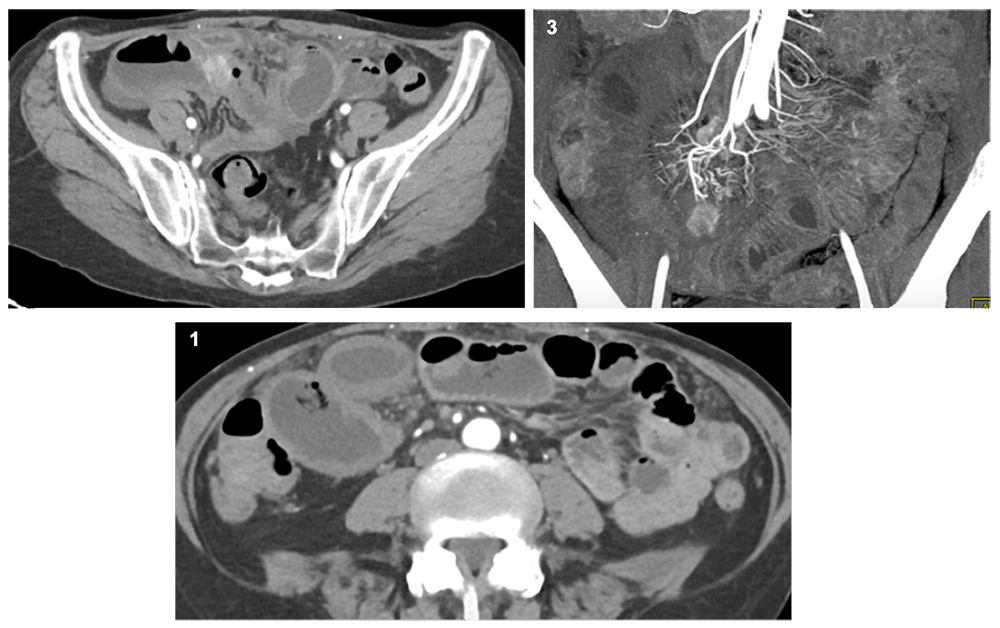 |
Case 4: Obstructing carcinoid tumor Axial CECT in the arterial phase demonstrates a 2cm x 2cm hypervascular mass (red arrow) associated with the ileum in the right lower quadrant with proximal small bowel dilation (A,B). 3D coronal reconstruction reveals a second hypervascular mass in the root of the mesentery measuring up to 2 cm encasing branches of the SMA (yellow arrow) (C). This constellation of findings was consistent with ileal carcinoid tumor, confirmed pathologically. Though no clear association has been shown between primary biliary cirrhosis (PBC) and ileal carcinoid, a few cases in the literature report patients with PBC and gastric carcinoid tumors. 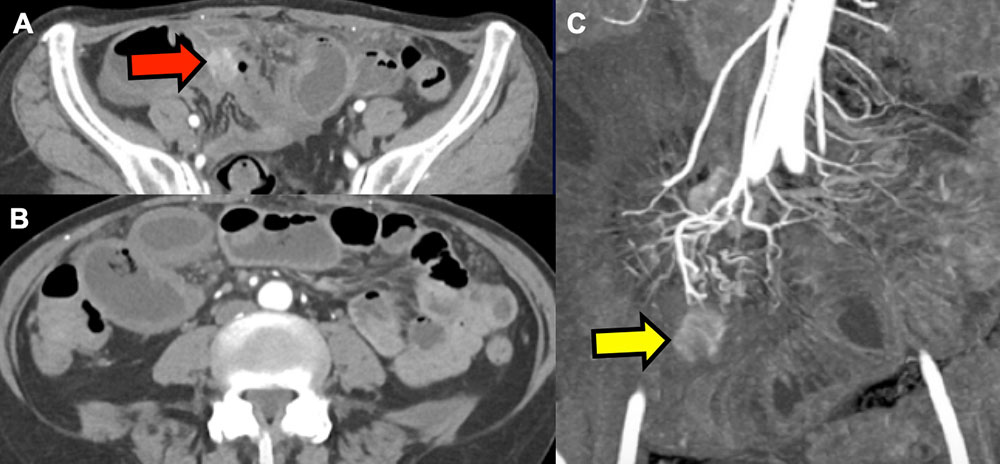 |
Case 5: Scrotal pain Patient with longstanding right inguinal mass presents with acute pain scrotal pain, nausea, and vomiting 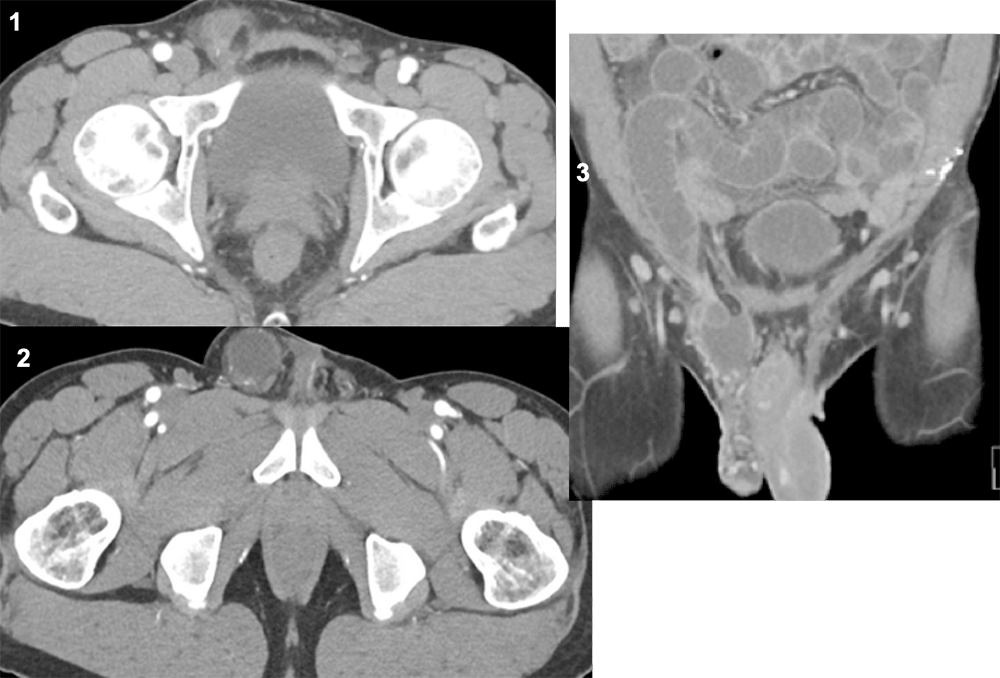 |
Case 5: Right inguinal hernia Axial CECT in the arterial phase demonstrates a narrow neck right inguinal hernia (red circle) with proximal small bowel dilation (A,B). Coronal reconstructions better delineate the extent of small bowel within the right inguinal hernia (yellow arrow) (C). The patient underwent emergent surgical reduction without requiring bowel resection. 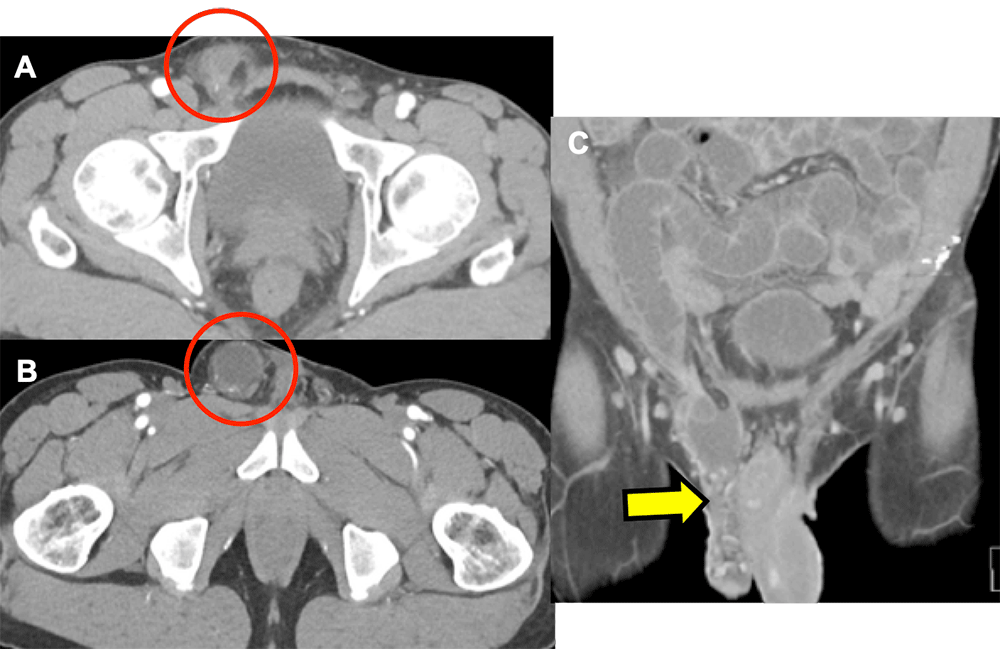 |
Case 6: History of heart transplant Patient with history of heart transplant presents with acute onset upper quadrant pain, nausea, and shortness of breath 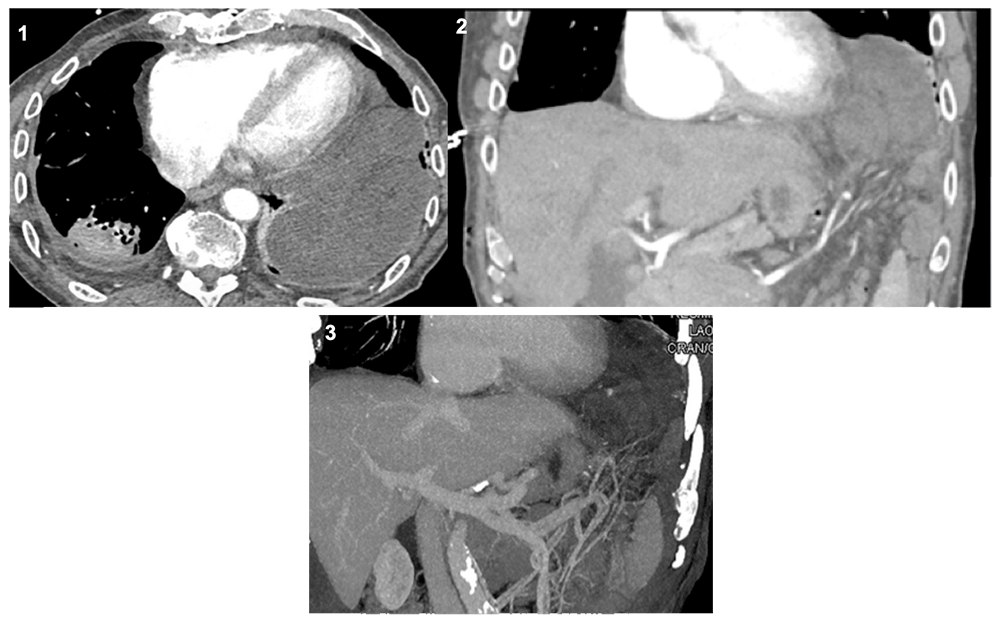 |
Case 6: Incarcerated diaphragmatic hernia Axial CECT in the arterial phase demonstrates multiple small bowel loops within the left thorax (red circle) (A,B). 3D coronal reconstructions in the arterial phase reveal an abrupt cutoff of vascular flow to the small bowel within the thorax (yellow arrows). 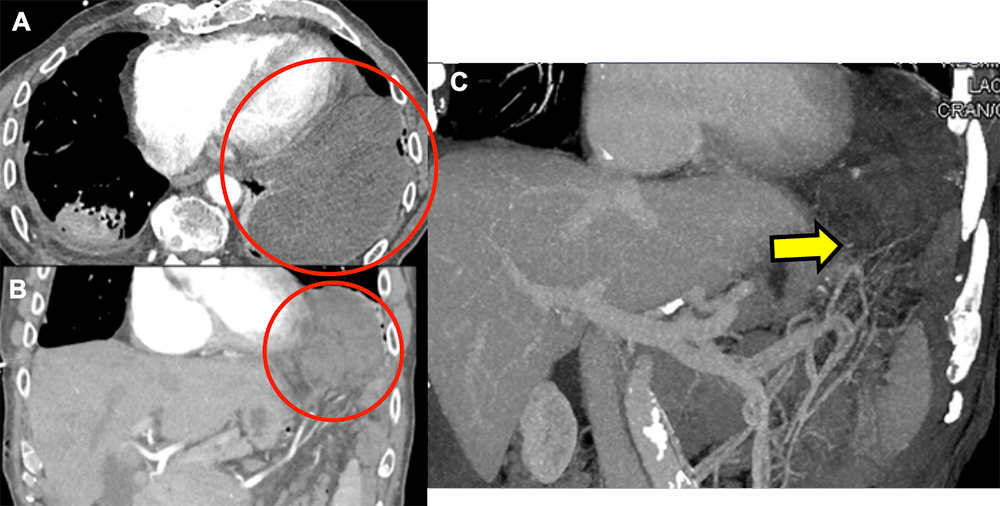 |
Case 7: History of Endometriosis Patient with history of endometriosis who presents with acute onset abdominal pain, nausea, and vomiting 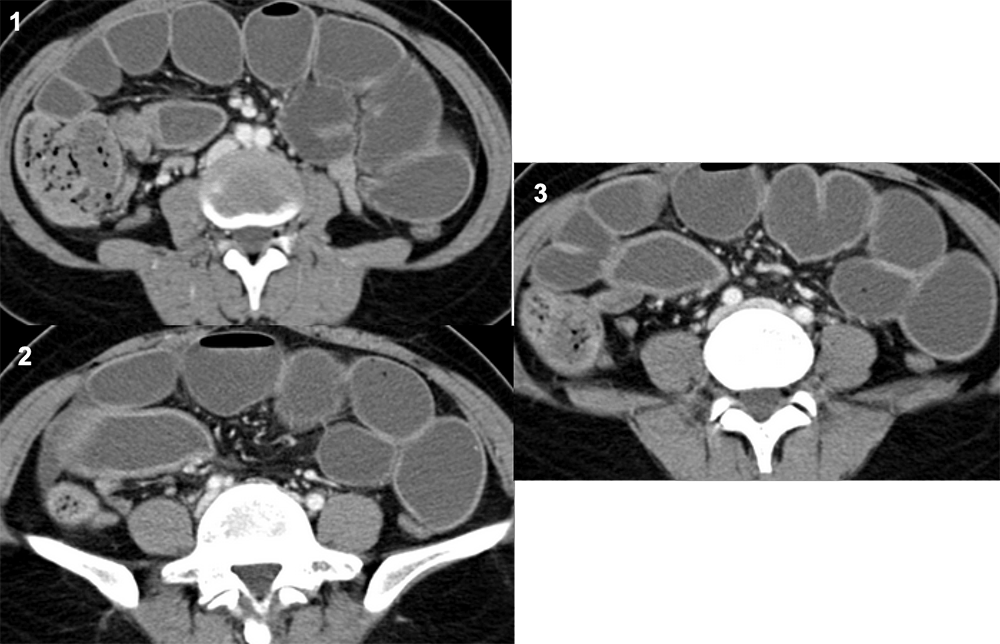 |
Case 7: Intestinal endometriosis Axial CECT in the arterial phase an area of focal soft tissue thickening in the right lower quadrant (red arrow) (A) with diffuse small bowel dilation (A,B). The area of thickening continues distally leading to a small bowel stricture (yellow arrow) (C) The patient was taken to the OR for resection. Pathology revealed extensive serosal endometriosis of the terminal ileum. 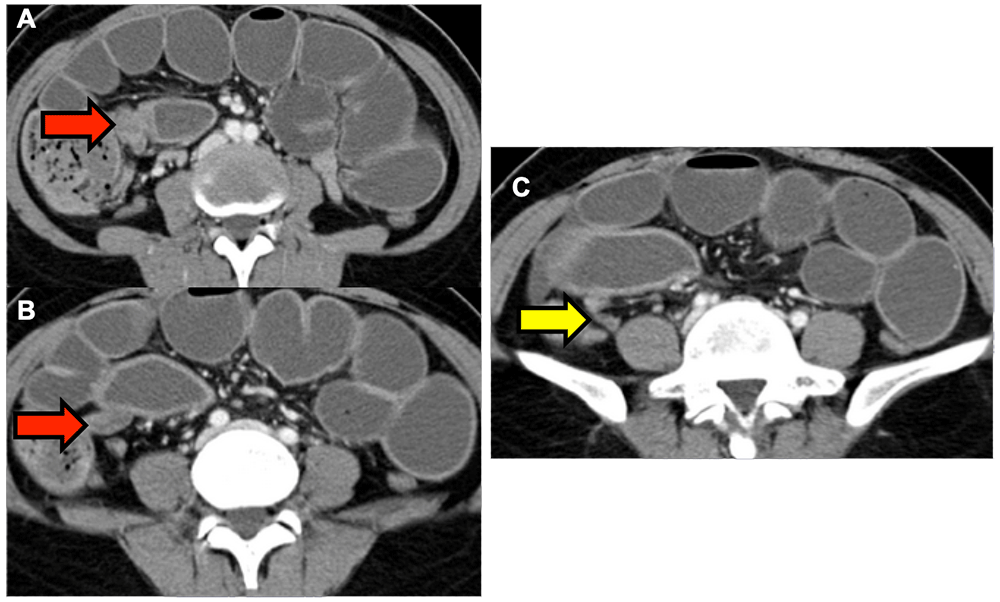 |
Case 8: History of Crohn’s Disease Patient with Crohn’s Disease presents with acute worsening of their chronic abdominal pain with nausea and vomiting. 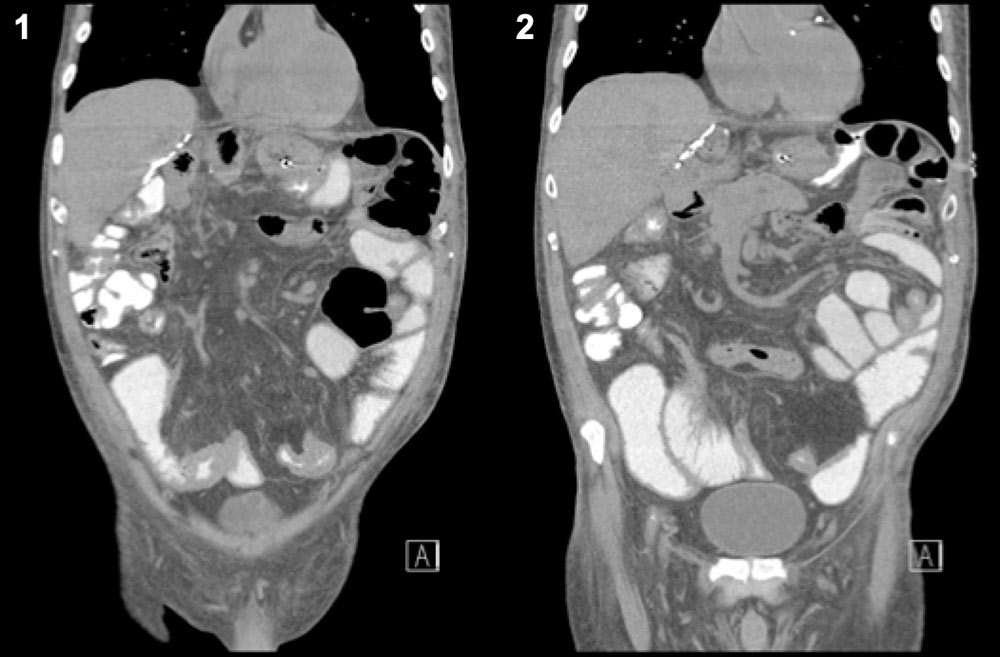 |
Case 8: Crohn’s Stricture Coronal CT with oral contrast only demonstrates an area of focal thickening of the distal ileum with narrowing of the bowel wall lumen in the lower abdomen (red arrows) and dilated proximal bowel (red box) (A, B). This constellation of findings is compatible with a classic inflammatory stricture seen in Crohn’s Disease. Sensitivity and specificity of MDCT in the diagnosis of inflammatory stricture in Crohn’s is approximately 85-93% and 100%, respectively. 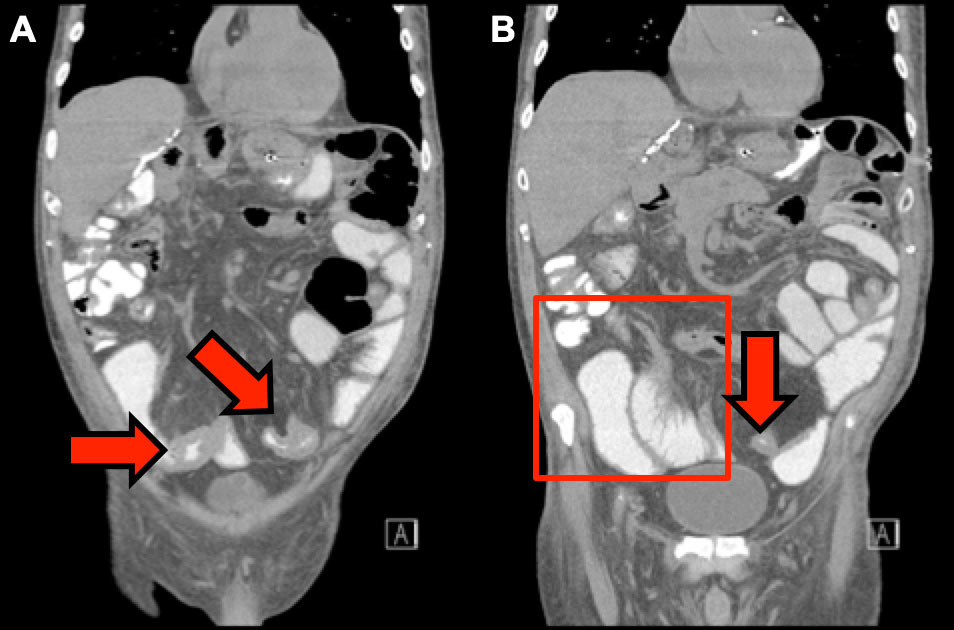 |
Case 9: History of serous adenocarcinoma Patient with history of ovarian serous adenocarcinoma status post surgical resection who presents with acute nausea, vomiting, and abdominal distention 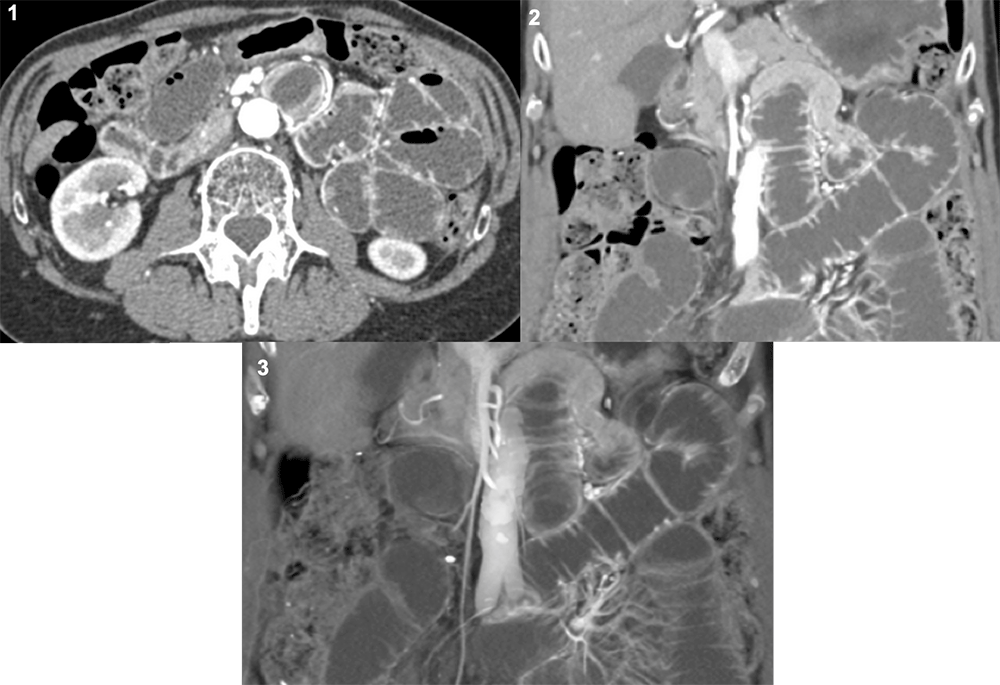 |
Case 9: Abdominal adhesions Axial and coronal CECT in the arterial phase demonstrates small bowel dilation with transition point in the right mid-abdomen (red arrow) and hyperenhancement of several small bowel loops (yellow arrow) (A, B). 3D coronal reconstruction redemonstrates transition point within the mid-abdomen. Adhesions most likely developed secondary to previous oncologic resection. 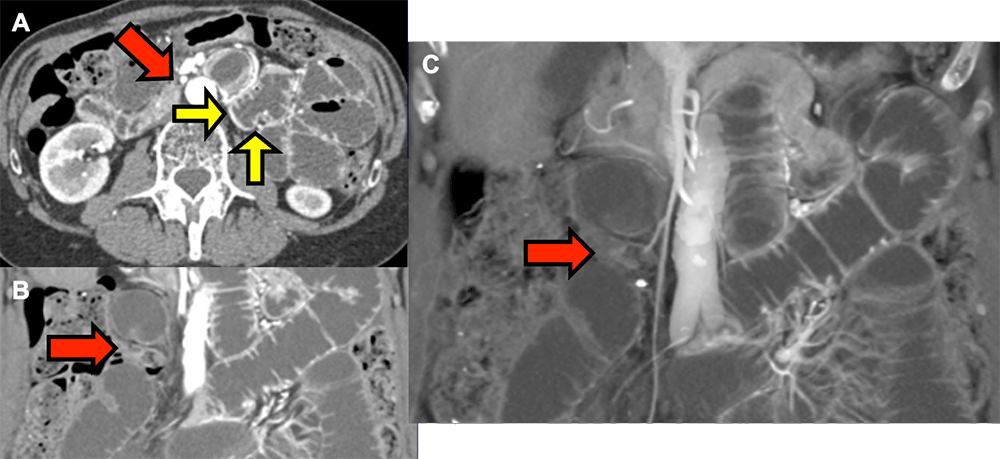 |
Case 10: History of cholelithiasis Patient with a history of cholelithiasis and multiple past episodes of right upper quadrant pain who presents with acute abdominal distention and diffuse colicky abdominal pain. 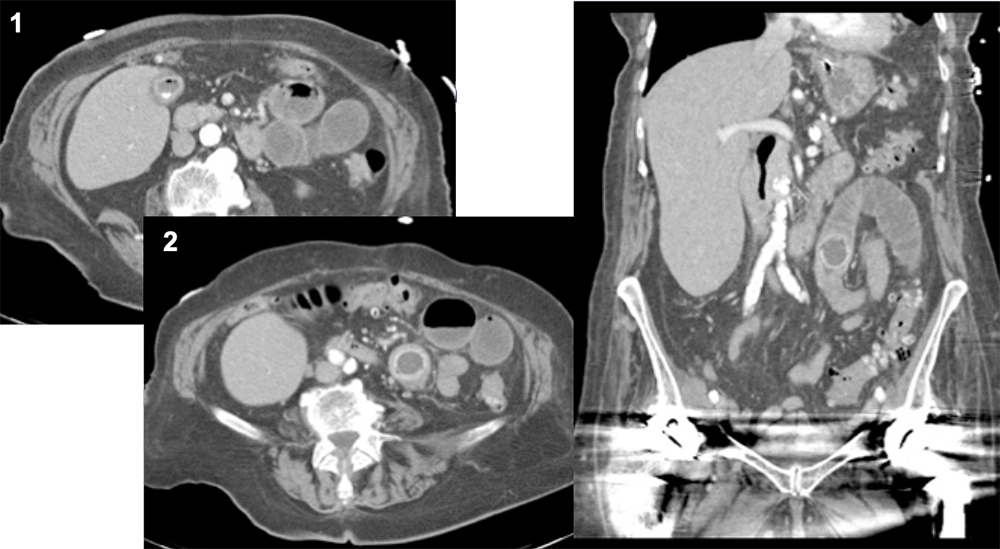 |
Case 10: History of cholelithiasis Axial and coronal CECT demonstrates cholelithiasis (red arrow) with a calcified gallstone within the small bowel lumen (yellow arrow) and minimal small bowel dilation proximal to the obstructing stone (red box). Additionally, there is air within the gallbladder lumen, like from a fistulous connection between the gallbladder and duodenum. Sensitivity and specificity of MDCT in the diagnosis of gallstone ileus is approximately 93% and 100%, respectively. 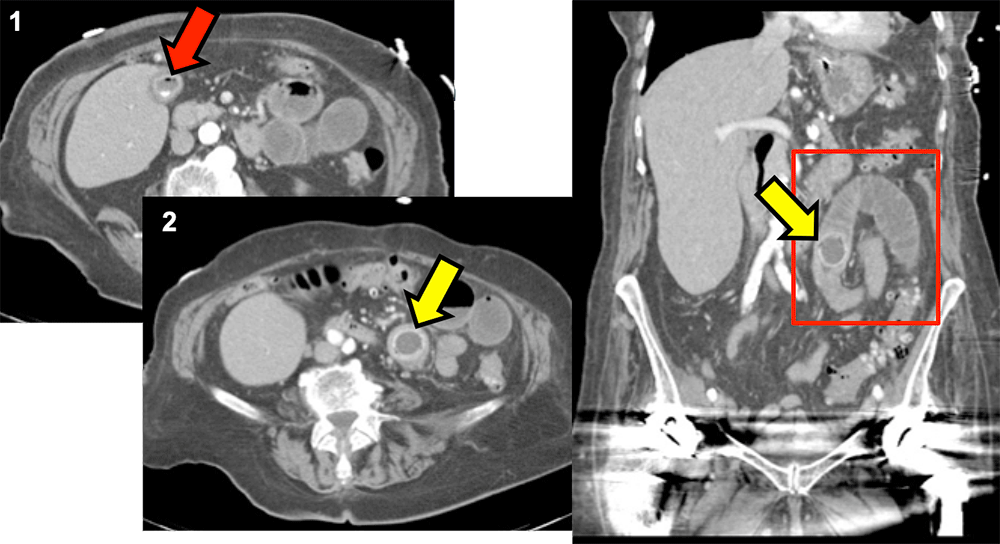 |
Case 11 19 year old woman status post pancreaticoduodenectomy for neuroendocrine tumor who presented with acute, severe abdominal pain. Coronal and sagittal MPRs 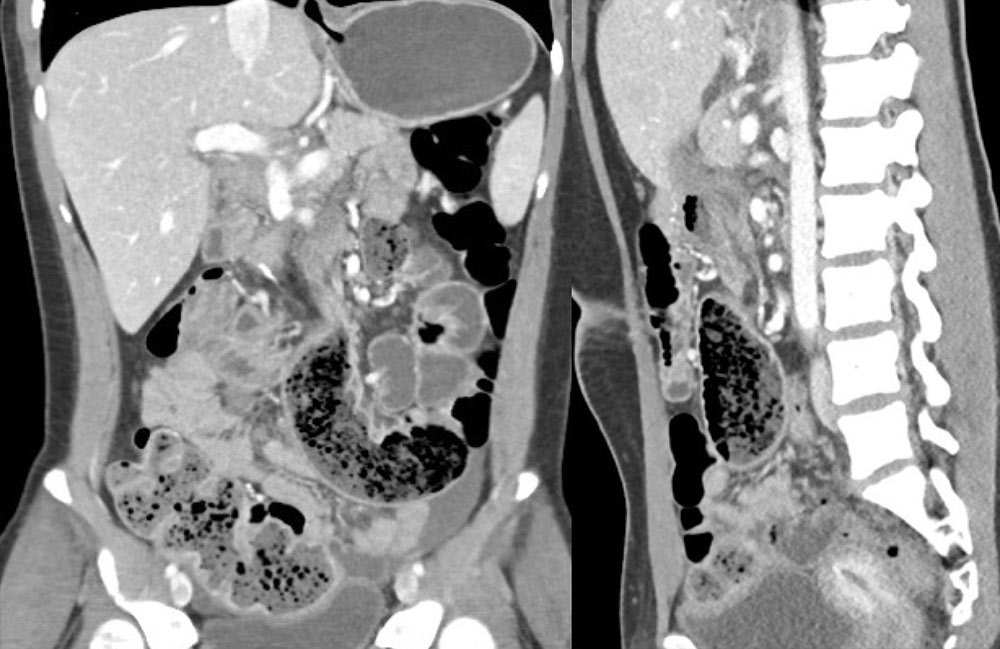 |
Case 11 Coronal and sagittal MPRs show a dilated loop of proximal small bowel with fecalized contents (red arrow) and collapsed segment folded on itself (yellow arrow) just distal to the point of obstruction (blue arrow). Concern for internal hernia confirmed at surgery. Hernia reduced and mesenteric defect repaired. Internal hernias present with acute severe pain, and imaging may be performed before the bowel dilates diffusely. 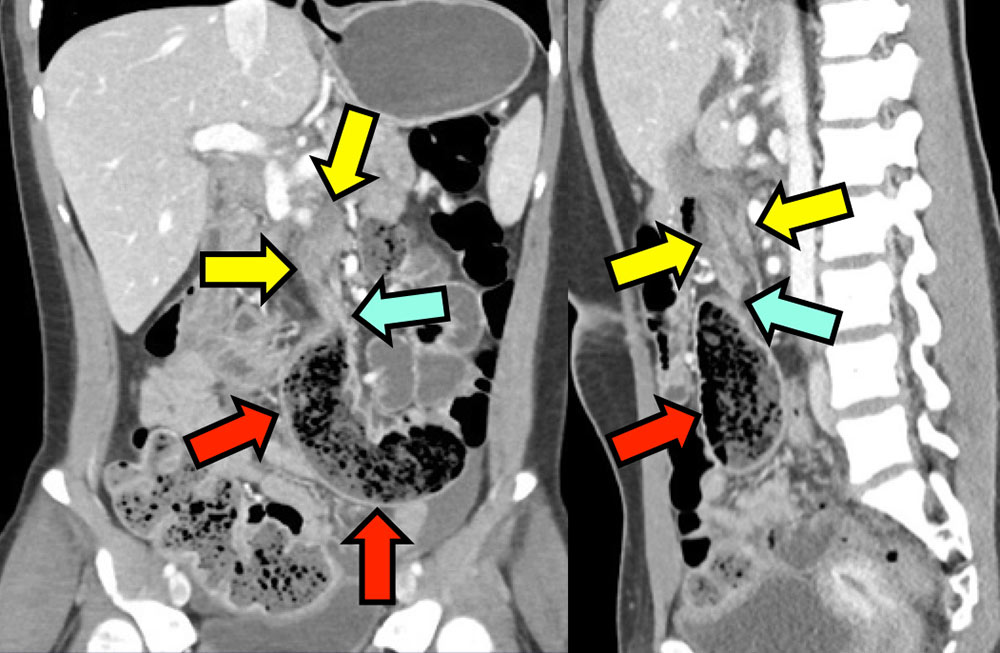 |
Case 12 55 year old man with abdominal pain and elevated lactate. 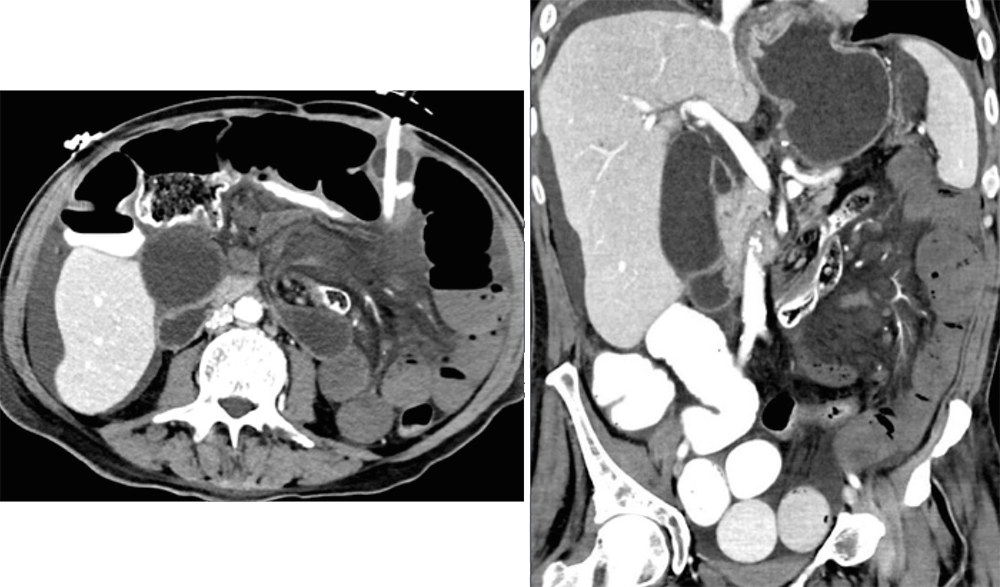 |
Case 12: Volvulus 55 year old man with abdominal pain and elevated lactate. Dilated small bowel in conjunction with whirled mesentery (yellow arrow) resulting in complete occlusion of the SMA (red arrow) and SMV (blue arrow). Note nonenhancing bowel loops with in left abdomen with mesenteric edema. Extensive infarcted bowel confirmed at surgery. 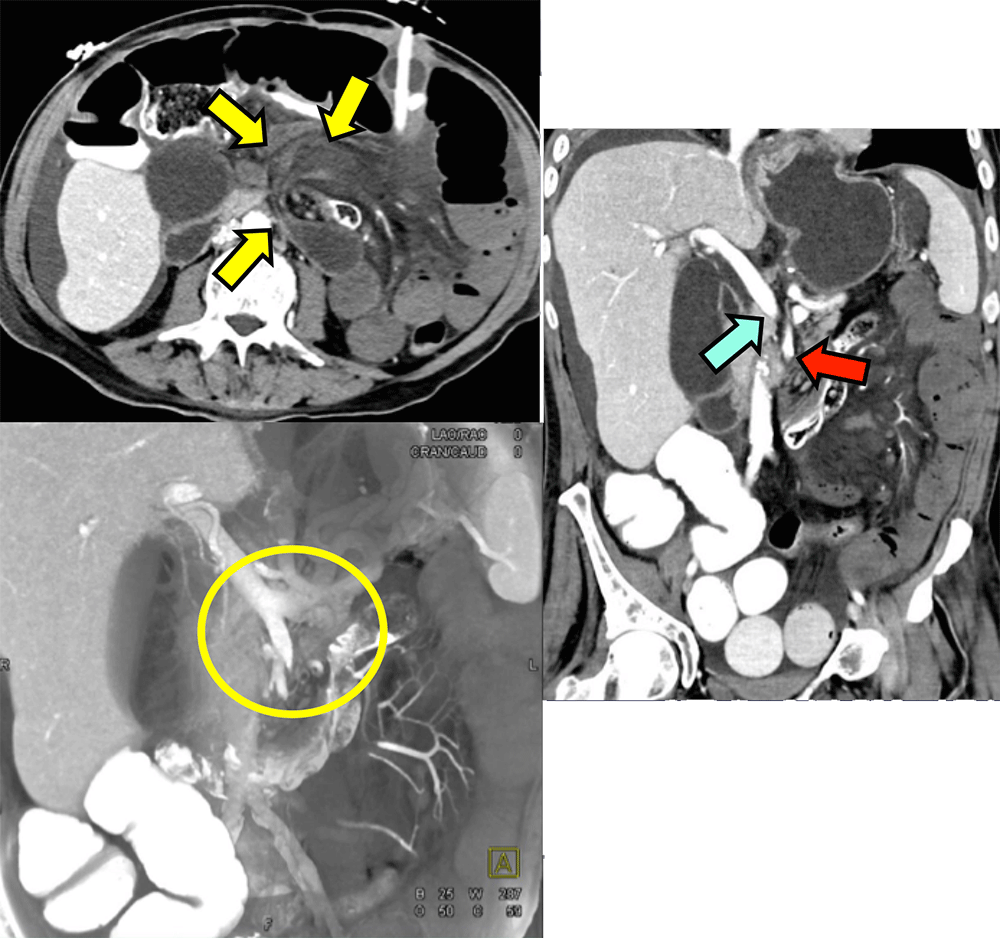 |
References
|
References
|