 Gunhild Nynke Thomsen1†
Gunhild Nynke Thomsen1† Mette Niemann Christoffersen1†Hanne Merete Lindegaard2†Jesper Rømhild Davidsen3†Gitte Nyvang Hartmeyer4†
Mette Niemann Christoffersen1†Hanne Merete Lindegaard2†Jesper Rømhild Davidsen3†Gitte Nyvang Hartmeyer4† Kristian Assing5†Charlotte G. Mortz6†Raquel Martin-Iguacel7†
Kristian Assing5†Charlotte G. Mortz6†Raquel Martin-Iguacel7† Michael Boe Møller8†Anette Drøhse Kjeldsen9†Troels Havelund10†
Michael Boe Møller8†Anette Drøhse Kjeldsen9†Troels Havelund10† Daniel El Fassi11,12†Sigurd Broesby-Olsen6†Michael Maiborg13†Sofie Lock Johansson14†Christen Lykkegaard Andersen11,12,15†Hanne Vestergaard1†
Daniel El Fassi11,12†Sigurd Broesby-Olsen6†Michael Maiborg13†Sofie Lock Johansson14†Christen Lykkegaard Andersen11,12,15†Hanne Vestergaard1† Ole Weis Bjerrum1*
Ole Weis Bjerrum1*- 1Department of Hematology, Odense University Hospital, Odense, Denmark
- 2Department of Rheumatology, Odense University Hospital, Denmark; Research Unit for Rheumatology, Odense University Hospital, Odense, Denmark; University of Southern Denmark, Odense, Denmark
- 3Department of Respiratory Medicine, Odense University Hospital, Denmark; Odense Respiratory Research Unit (ODIN), Department of Clinical Research, University of Southern Denmark, Odense, Denmark
- 4Department of Clinical Microbiology, Odense University Hospital, Odense, Denmark
- 5Department of Clinical Immunology, Odense University Hospital, Odense, Denmark
- 6Department of Dermatology and Allergy Centre, Odense Research Centre for Anaphylaxis (ORCA), Odense University Hospital, Denmark; University of Southern Denmark, Odense, Denmark
- 7Department of Infectious Diseases , Odense University Hospital, Odense, Denmark
- 8Department of Pathology, Odense University Hospital, Odense, Denmark
- 9Department of ORL- Head and Neck Surgery and Audiology, Odense University Hospital, Odense, Denmark; University of Southern Denmark, Odense, Denmark
- 10Department of Gastroenterology and Hepatology, Odense University Hospital, Odense, Denmark
- 11Department of Hematology, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark
- 12Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark
- 13Department of Cardiology, Odense University Hospital, Odense, Denmark
- 14Department of Respiratory Medicine, Odense University Hospital, Odense, Denmark
- 15Centre for General Practice, Department of Public Health, University of Copenhagen, Copenhagen, Denmark
Eosinophilic granulocytes are normally present in low numbers in the bloodstream. Patients with an increased number of eosinophilic granulocytes in the differential count (eosinophilia) are common and can pose a clinical challenge because conditions with eosinophilia occur in all medical specialties. The diagnostic approach must be guided by a thorough medical history, supported by specific tests to guide individualized treatment. Neoplastic (primary) eosinophilia is identified by one of several unique acquired genetic causes. In contrast, reactive (secondary) eosinophilia is associated with a cytokine stimulus in a specific disease, while idiopathic eosinophilia is a diagnosis by exclusion. Rational treatment is disease-directed in secondary cases and has paved the way for targeted treatment against the driver in primary eosinophilia, whereas idiopathic cases are treated as needed by principles in eosinophilia originating from clonal drivers. The vast majority of patients are diagnosed with secondary eosinophilia and are managed by the relevant specialty—e.g., rheumatology, allergy, dermatology, gastroenterology, pulmonary medicine, hematology, or infectious disease. The overlap in symptoms and the risk of irreversible organ involvement in eosinophilia, irrespective of the cause, warrants that patients without a diagnostic clarification or who do not respond to adequate treatment should be referred to a multidisciplinary function anchored in a hematology department for evaluation. This review presents the pathophysiology, manifestations, differential diagnosis, diagnostic workup, and management of (adult) patients with eosinophilia. The purpose is to place eosinophilia in a clinical context, and therefore justify and inspire the establishment of a multidisciplinary team of experts from diagnostic and clinical specialties at the regional level to support the second opinion. The target patient population requires highly specialized laboratory analysis and therapy and occasionally has severe eosinophil-induced organ dysfunction. An added value of a centralized, clinical function is to serve as a platform for education and research to further improve the management of patients with eosinophilia. Primary and idiopathic eosinophilia are key topics in the review, which also address current research and discusses outstanding issues in the field.
1 Introduction
The differential count of white blood cells is a simple analysis to obtain diagnostic information, and deviations in the number of leukocytes reflect perturbed homeostasis. Leukocytosis and leukopenia, associated with neutrophilic granulocytes or lymphocytes, are important clues when evaluating a patient, indicating, for example, a feedback control request for immunocompetent cells to fight infections or a derailed leukopoiesis with or without maturation (1, 2). Eosinophilic granulocytes (eosinophils) are normally among the least abundant circulating white blood cells (<0.5 × 109/L). Unlike common leukocytes, a reduced number of eosinophils is not captured by the differential count and is normally not clinically paid attention to. In contrast to this, the observation of an increase in eosinophils in a differential count of blood or other samples can be a key piece of information that should be contextualized in advance in the individual (adult) patient. However, a structured approach is required to guide diagnostic and therapeutic decisions clinically, and the task is to isolate the impact of an increased eosinophil count (eosinophilia) from all other etiologic factors in the overall assessment (3–8).
Chronic myeloproliferative neoplasms (MPNs) include several distinct disorders, representing an autonomous turnover of one or more of the cells, circulating in the blood. MPNs include, according to the current WHO classification, breakpoint cluster region—Abelson1 (BCR-ABL1)-positive chronic myeloid leukemia (CML) and the BCR-ABL1-negative neoplasms, many of which are considered to be inflammatory conditions driving a clonal evolution in a biological continuum involving variable mutations and genetic structural aberrations (9–14). A separate category in the WHO classification is the myeloid/lymphoid neoplasms with eosinophilia and tyrosine kinase fusion genes (MLN-TK), which are usually prominent features at diagnosis (9).
Primary eosinophilia is rare and reflects clonal hematopoiesis in which the production of eosinophils is driven by a genetic or intrinsic cause. Causes of secondary eosinophilia are common and very different in nature and are characterized as being reactive to factors with an extrinsic impact on the eosinopoiesis. Secondary or reactive eosinophilia is driven, in particular, by the cytokine interleukin (IL)-5, produced by activated T lymphocytes (15, 16). This scenario of immunological crosstalk is associated with autoimmune, infectious, and inflammatory diseases; malignancy; and allergy, including iatrogenic, drug-induced adverse reactions (3–8). When no congenital, clonal, or reactive cause can be demonstrated, patients with persistent eosinophil counts of at least 1.5 × 109/L are categorized as idiopathic hypereosinophilic. This group can be subdivided into patients with no manifestations of eosinophilia [iHE, or hypereosinophilia of undetermined significance (iHEUS)] or idiopathic hypereosinophilic syndrome (iHES), when organ involvement due to eosinophils is present (3–8, 17–20). However, the overlap of symptoms, regardless of whether the cause of the disease is primary, secondary, or idiopathic eosinophilia—or a combination of them—is considerable, and characterizes the patient with an increased eosinophil count in blood as a clinical challenge.
Notwithstanding the cause, the presence of an increased number of circulating eosinophils in the blood may be associated with inappropriate organ involvement. In most cases, patients with secondary eosinophilia are treated successfully by the general practitioner (GP) or at departments specialized in the management of individual manifestations. However, it can be difficult to prove whether the patient has primary eosinophilia, secondary eosinophilia, or iHES—or whether the symptoms and cause of the eosinophilia can be attributed to an atypical presentation or represent more than one etiology. An insufficient response to symptoms, and unexplained persistent or recurrent eosinophilia despite adequate treatment may be a reason for a thorough reassessment. This review describes eosinophilia in a clinical context, particularly how a dedicated function with a multidisciplinary team is one way to provide a rational approach due to the complexity of demonstrating differential diagnosis and options for targeted treatment. Current unresolved issues in the management of eosinophilia are discussed.
2 Review of the eosinophil granulocyte in health and disease
2.1 The eosinophil granulocyte and pathophysiology
Eosinophils originate from a myeloid cluster of differentiation (CD) CD34+ precursors in the bone marrow and are part of the innate immune system (16, 21). Maturation takes a week on average and is influenced by a granulocyte-macrophage colony-stimulating factor (GM-CSF), IL3, and IL-5 and is driven by activation of transcription factor networks including PU.1, CCAAT/enhancer-binding protein (C/EBP), and GATA-binding protein 1 (GATA-1). All of the above are involved, but IL-5 and GATA-1 have key roles in eosinopoiesis and turnover; IL-5 is involved in egress from the bone marrow microenvironment into the bloodstream, promoting activation and survival and preventing apoptosis; and GATA-1 is a vital regulator of cell maturation (22–24).
The course of eosinophils subsequent to bone marrow release starts with circulation in the bloodstream for 8–18 h and terminates in peripheral organs for up to 12–14 days or longer (25, 26). At some point during circulation in the bloodstream, the eosinophil migrates through the lining of blood vessels and enters one of the numerous organs, possibly attracted by chemokines (27). Being mobile cells, they are distributed to the liver, lungs, skin, heart, reticuloendothelial system, glands, and digestive tract, but not to the esophagus, which is normally devoid of eosinophils. The cells remain in the organs as tissue-resident cells under homeostatic conditions. During this time, the cell may proliferate under inflammatory conditions and undergo terminal apoptosis (28, 29).
Eosinophils in the bloodstream or tissues are large, spherical cells, 12–17 μm in size with a bi-lobed nucleus, without a nucleolus, and exhibiting numerous coarse, rounded, and red-purple granules in the cytoplasm by routine staining (16, 24, 28). Figure 1 shows peripheral blood smears, illustrating mature eosinophil granulocytes from a patient with mild eosinophilia. Eosinophils can be compared morphologically to neutrophil granulocytes, lymphocytes, and platelets. Typically, less than one eosinophil granulocyte will be recognized in a field using light microscopy. Detection of more than one eosinophil in a 400× light microscopy field examination is an indication of eosinophilia, normally representing 1%–4% of all white blood cells (1, 2).
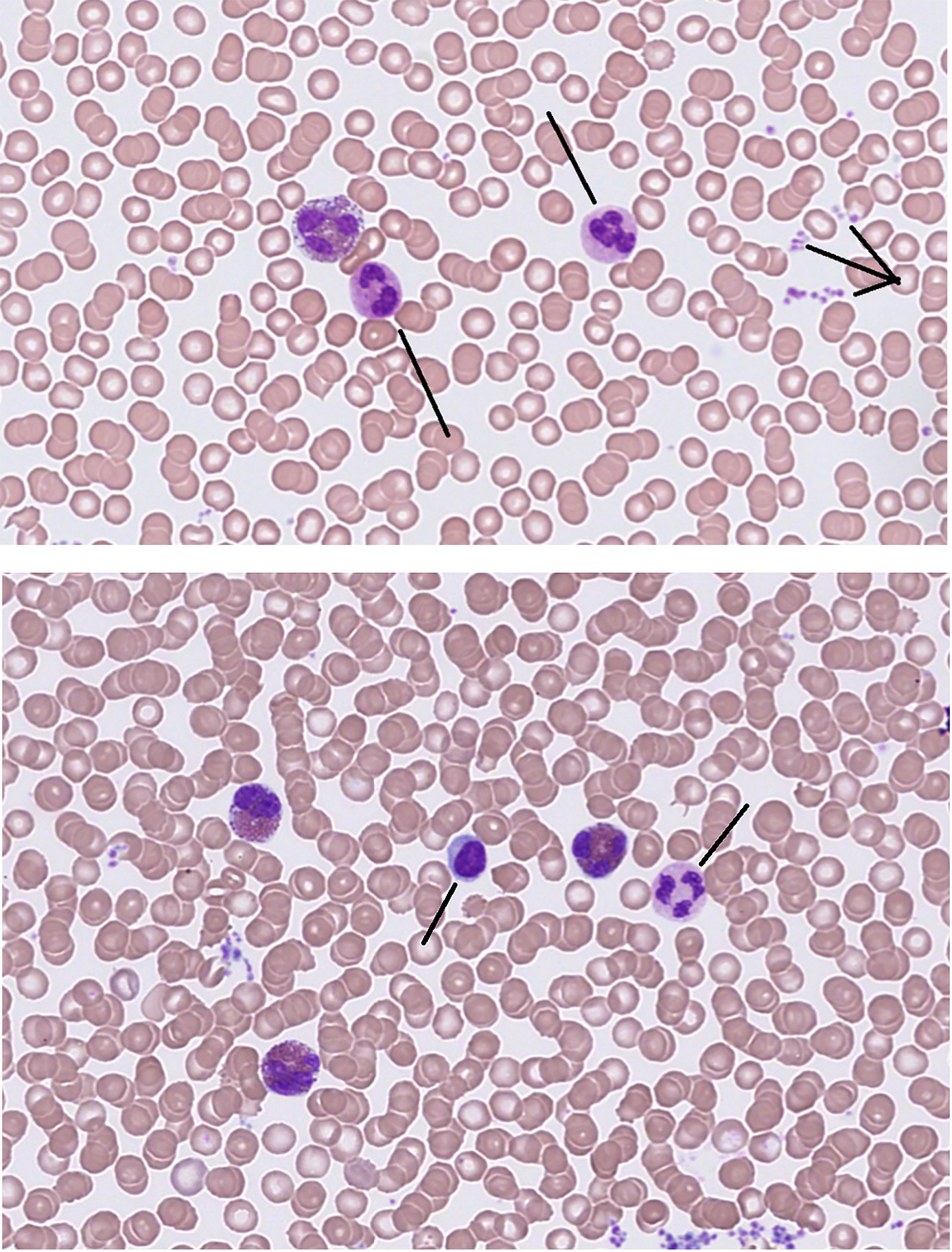
Figure 1 Eosinophil granulocytes in peripheral blood smear. Giemsa stain, 400×. Upper panel illustrates one eosinophil, neutrophil granulocytes (/), and aggregates of platelets (>). Lower panel shows eosinophil granulocytes, a mononuclear cell (/ lymphocyte), a polynuclear granulocyte (/ neutrophil), and thrombocytes (not marked).
The cell is easily identified by light microscopy in a blood smear by the appearance of the nucleus and coarse granules, which distinguish the appearance of eosinophils from other leukocytes (Figure 1). The cytoplasm contains not only the abundant and phenotypically characteristic-specific (also named secondary) granules, but also other organelles (not readily visible using light-microscopy) such as the smaller, azurophilic, and fewer primary granules. Both granules are lysosomes, storage sites for agents involved in tissue damage and inflammation. The secondary granules contain chemokines, growth factors, cytokines, and proteolytic enzymes such as the major basic protein, eosinophil peroxidase, eosinophil-derived neurotoxin, and eosinophil cationic protein (15, 23, 24, 26, 30). A predominant protein in eosinophils is galectin-10, which is now identified as a component of the peripheral cytoplasm. Upon secretion, it precipitates in tissues and body fluids as the Charcot–Leyden crystal protein, a lysophospholipase indicative of eosinophil granulocyte activity (31). The various proteases released from the specific granules contribute to the antimicrobial effect of the phagocytosing eosinophil granulocyte but may, at the same time, cause epithelial cell damage, and cytotoxicity, and contribute to fibrosis. The release of substances into tissues is damaging to microorganisms or bystander cells, causing organ damage. The concentration of proteases in body fluids may serve as a biomarker of inflammation involving eosinophils, reflecting a potential effect of circulating granule components (15, 28, 32).
Eosinophil granulocytes interact via their arsenal of surface-bound receptors (e.g., IgE, histamine, chemokine, cytokine, and adhesion) and the ability to secrete various proteins and other substances as mentioned above, that characterize both circulating and resident granulocytes (15, 23, 24, 33, 34). The dynamics are normally reflected in their ability to respond to infectious and inflammatory stimuli by increased numbers, eosinophilia in the blood and affected tissues, and activation. The release of preformed or stimulus-dependent chemokines, interleukins, leukotrienes, growth factors, and proteins behaves like a cascade, accompanied by a respiratory burst. The generation of reactive oxygen species upon assembly of the components of the enzyme nicotinamide adenine dinucleotide phosphate (NADPH) oxidase complex in the plasma membrane is higher per cell in eosinophils than in neutrophils (35, 36). Although the number of neutrophils is usually about 10 times higher, the increase in eosinophils in response to inflammatory or infectious stimuli contributes to the potential toxicity in the process, including harmful effects on bystander cells, through the release of granule content and reactive oxygen species. Like neutrophils, eosinophils are phagocytes that contribute to the direct control of helminth infections, and both granulocytes can form extracellular traps. This complex network of granule components and DNA is the ultimate contribution of the dying cell participating in parasitic infection and inflammation (15, 34, 37).
The phenotype of mature eosinophil granulocytes and precursor cells can be separated by the CD11b/CD62L expression, accompanied by upregulation and co-expression of various surface markers. These include C-C motif chemokine receptor 3 (CCR3, CD193), IL-5 receptor alpha (CD125), and sialic acid-binding Ig-like lectin 8 (siglec-8), a member of the CD33-related siglec subfamily, all of which are highly expressed on the surface of eosinophil granulocytes in blood and bone marrow (23, 28, 38, 39). Flow cytometry to identify eosinophils may be routinely performed, including a panel of monoclonal antibodies to detect myeloid proliferation according to Euroflow (40). However, flow cytometry may not be relevant if the eosinophil count is normal.
Being classified as an MPN, iHES carries the risk for vascular events both before and after diagnosis. The manifestations are almost always thrombotic, in both arterial and venous locations, and may be more frequently associated with clonal, primary eosinophilia. The thrombogenic potential of eosinophilia may be manifested in addition to other inherited or acquired risk factors for vascular events. The risk of bleeding may be minimal because severe thrombocytopenia or another-acquired hemorrhagic diathesis is very unusual in iHES. Retrospective analyses of HES cohorts report that 21%–24% of patients have experienced at least one event before diagnosis (41, 42). One study has linked increased expression of tissue factor (factor III or CD142), which is the initiator of thrombin generation, in eosinophil granulocytes examined in patients with iHES and secondary hypereosinophilia (43). In addition, eosinophils interact with platelets to promote atherosclerosis and thrombosis (44).
2.2 Epidemiology and definitions
An increase in the number of eosinophils is common and can be arbitrarily divided into three levels: mild (0.5–1.5 × 109/L), moderate (≥1.5 × 109/L), and severe (>5 × 109/L) eosinophilia. The term hypereosinophilia may be used to characterize all cases of moderate or severe eosinophilia (3–6).
The number of eosinophil granulocytes in the blood is routinely measured by automated machine analysis as part of the differential count. Minor variations in the normal threshold, defined as 0.4–0.5 × 109/L blood, may be observed between different machines and laboratories, but a manual count of (mature) eosinophils in the blood is rarely if ever, needed (45). An association within the normal range of blood eosinophil counts in adults has been reported to be correlated with several demographic factors including age, biological sex, race, BMI, and smoking status (46, 47). A diurnal variation in eosinophil count in healthy individuals has been reported to be higher at night and lower in the morning (48). Despite these variations in normal subjects, no specific recommendation has been made or deemed relevant for the interpretation of cell counts in patients with eosinophilia.
The incidence of eosinophilia varies worldwide. Although due to a plethora of reactive causes, it is more likely due to infection in tropical areas and inflammation in industrialized regions. A hospital incidence of over 10% has been reported in South Korea (49) and India (50). The incidence of eosinophilia in subjects having a blood sample taken over 10 years in the primary sector of a Western capital city was reported to be 4% in adults, reflecting that eosinophilia is a common problem to be contextualized clinically (51). In contrast, the incidence of eosinophilia in a large Canadian island district was 0.1% (52). The elevated cell count is transient in almost all patients with secondary eosinophilia, due to the impact of treatment or the self-limiting nature of the reaction, and the prevalence of eosinophilia remains low.
The definition of HES was introduced in 1968 and required that patients presented moderate or severe blood eosinophilia of unknown origin for more than 6 months, and for it to be responsible for organ damage (53, 54). The term in its original meaning is no longer applicable due to the options for treatment, the risk of irreversible symptoms, and the improvements in the diagnostic tools. Today, according to the agreed-upon definitions, HES reflects a heterogeneous group of disorders, presenting with persistent peripheral blood eosinophilia ≥1.5 × 109/L on two occasions, the absence of a secondary cause of eosinophilia, and evidence of eosinophil-associated end-organ damage, justified by excessive tissue eosinophilia (55, 56).
The incidence has been reported to be 0.036/100,000 for HES in the USA (57) and 0.018/100,000 specifically diagnosed with the most prevalent primary eosinophilia, a factor interacting with PAPOLA and CPSF1-platelet-derived growth factor receptor alpha (FIP1L1-PDGFRA)-positive neoplasms, in France (58). The reports underline the rarity of primary eosinophilia, and more precise estimates may be difficult to collect, although the WHO ICD system provides diagnostic registry codes for different subclasses of hypereosinophilia. The FIP1L1-PDGFRA primary myeloid neoplasm is more prevalent in male adults (58), but otherwise, iHES and clonal primary eosinophilia are overall not gender-specific and can be diagnosed at all ages. No valid data are available on the incidence in pediatric patients (59, 60).
Eosinophilia can be classified by diagnostic tests into congenital (familial) causes as primary (intrinsic, clonal) or secondary (extrinsic, reactive) (20, 55). The diagnosis by exclusion of iHES (with symptoms due to eosinophilia) may also be clinically sub-characterized as either a myeloid (mHES) or a lymphoid (lHES) phenotype (61, 62). The lymphoid HES subtype is driven by CD3−CD4+ IL-5, producing T cells and thus secondary, non-neoplastic eosinophilia that is glucocorticoid sensitive and often associated with, e.g., angioedema, skin lesions, pruritus, and fasciitis (63). Previously, concomitant manifestations such as cardiac involvement, hepatosplenomegaly, anemia, variable leuko- and thrombocyte counts, and steroid resistance were used to phenotypically characterize a myeloid HES (61, 62, 64), similar to other MPNs. Specific diagnostic tests are required to identify patients according to the updated criteria. The revisions of the WHO classifications of malignant eosinophilic disorders by molecular diagnostic markers since 2008 have established the cluster of MLN-TK identified by specific tyrosine kinase rearrangements (3–9).
2.3 Symptoms of eosinophilia
The presentation of patients with eosinophilia varies considerably, in terms of symptoms and severity. Over days to months, most patients may gradually experience a worsening of symptoms related to the cause of eosinophilia, whereas symptom flares are characteristic of iHES. The presence of an increased eosinophil count in the blood may have been indolent for years, or manifestations may be due to a recent onset involving one or more organs simultaneously. The clinical context at presentation in patients with an increased blood eosinophil count is not related to the classification of primary, secondary, or iHES, because the symptoms due to eosinophilia may mimic or be involved in the diseases listed in Supplementary Table 1 concerning organ manifestations (65–86) and Supplementary Table 2 concerning parasitic causes (87, 88). An exception is iHE/iHEUS, which by definition is asymptomatic eosinophilia (4–7, 20, 55).
The considerable overlap in patients presenting with eosinophilia as a clinical clue in differential diagnostics reflects how complex the correct diagnosis may be. Nevertheless, common pathologic conditions not associated with eosinophilia may manifest with similar symptoms. The recurrent question is to decide whether eosinophilia is an independent causative factor or whether the presence of eosinophilia is an additional causative factor to disorders that may have been present before the eosinophilia was noticed. Symptoms due to eosinophilia may thus be manifest in all organ systems in addition to pre-existing conditions, masked as a worsening (Supplementary Table 1).
B-symptoms, including weight loss, low-grade fever, and night sweats may occur in all patients with eosinophilia, whether primary, secondary, or iHES. In the individual patient, they may be attributed to cytokine signaling induced by eosinophils or other immunocompetent cells as part of a malignant, infectious, and inflammatory secondary cause (Supplementary Tables 1, 2).
Reports on cohorts with eosinophilia have been published describing manifestations in iHES (65) or cross-sectional symptom registries (66, 67). Studies from Western institutions cannot be compared due to methodological differences, but the institutional reports reflect the diversity of symptoms ascribed to primary or secondary eosinophilia (Supplementary Tables 1, 2). The most common organ involvement in patients with unexplained hypereosinophilia referred for examination involves dermatologic, respiratory, and gastrointestinal symptoms in approximately 45%, 35%, and 25%, respectively (65, 66). Registration of causes of unclassified eosinophilia identifies infection, allergy, and non-hematologic malignancy as common causes in different parts of the world (49, 50, 52, 61, 66, 67). These data support a multidisciplinary approach to patients who cannot be classified in a straightforward manner according to diagnostic guidelines or who do not respond adequately to proper treatment (Supplementary Tables 1, 2).
2.4 Diseases associated with eosinophilia
2.4.1 Diagnostic entities
Figure 2 depicts the clinical spectrum, contemplating diagnostic entities that approach a patient with eosinophilia in the causative context, including manifestations of organ involvement that may have overlapping presentations (Supplementary Tables 1, 2) (65–88). The threshold is chosen to align with the definition of iHE/iHEUS or iHES. Still, it applies to all cases with mild eosinophilia and patients without symptoms or with symptoms related to diagnoses other than eosinophilia. It may be important to examine in the same way patients with an increased or fluctuating eosinophil count observed over weeks to months or even years.

Figure 2 Pathophysiological algorithm and examples of diagnostic entities in patients with (moderate) eosinophilia. The diagram is not exhaustive. ABPA, allergic bronchopulmonary aspergillosis; BCR-ABL, breakpoint cluster region—abelson1; CBF, core binding factor; CML, chronic myeloid leukemia (t9;22) positive; DRESS, drug reaction eosinophilia systemic symptoms; EGPA, eosinophil granulomatous polyangiitis; ETV6, ETS variant transcription factor 6; FGFR1, fibroblast growth factor receptor 1; FLT3, Fms-related tyrosine kinase 3; HES, hypereosinophilic syndrome; ICI, immune checkpoint inhibitor; Ig, immunoglobulin; iHE, idiopathic hypereosinophilia; iHES, idiopathic hypereosinophilic syndrome; inv, inversion; JAK2, Janus kinase 2; MC, mixed cellularity; MDS, myelodysplastic neoplasm; MPN, myeloproliferative neoplasm; NS, nodular sclerosis; PDGFRA/B, platelet-derived growth factor A or B; t, translocation.
The descriptive manner in which eosinophilia is elucidated by pathophysiologic drivers can contribute to structuring the clinical approach and qualify diagnostic testing in a patient with newly diagnosed eosinophilia or for a second opinion at a later stage in a multidisciplinary forum. The information provided in Figure 2 is not exhaustive, as it is not possible to present a complete list. Figure 2 includes major groups of hematologic diagnoses as defined by the current WHO classification (9, 89). iHE and iHES are listed as clonal hematologic disorders, assuming that most cases, which at the moment are diagnosed by exclusion, may harbor a clonal driver in the eosinopoiesis (90). The algorithm indicates when eosinophils are part of the clonal disease, as described, for example, in some acute myeloid leukemias (AML) with recurrent genetic abnormalities, such as core-binding factor AML with t(8;21) or inv (16), including immature eosinophilia (91, 92). The differential diagnosis may include MLN-TK. Eosinophilia appears to be reactive and induced by cytokine signaling (IL-3) in B-acute lymphoblastic leukemia (B-ALL) with t(5;14) and with mature eosinophils circulating in the blood (93). Characterization of secondary eosinophilia can be hampered by difficulties in quantifying specific cytokine stimuli. These analyses are not done routinely at most institutions and therefore require scientific projects to accumulate data and describe the involvement of genetics as well as inflammation, e.g., in histiocytosis.
Eosinophilia is always present in iHE/iHEUS and iHES and is part of the diagnostic criterion. Eosinophilia is present in almost all cases of MLN-TK, caused by fusion genes involving a receptor [PDGFRA or B, fibroblast growth factor receptor (FGFR), fms like tyrosine kinase 3 (FLT3)], a transcription factor (ETV-6), or a non-receptor kinase (Janus kinase 2, JAK2). Eosinophilia is mandatory at diagnosis in chronic eosinophilic leukemia (CEL) (Figure 2) (6–9, 20, 58). Most patients with CML (in the chronic phase) present with mild or moderate absolute eosinophilia as part of the BCR-ABL1 oncogene-driven leukocytosis and may rarely present as eosinophilia (94). Eosinophilia is variable, and mild, if present, in Philadelphia-negative MPNs such as polycythemia vera (PV) or primary myelofibrosis (PMF), and essential thrombocytosis (ET) but is not part of the diagnostic criteria (9, 19, 95). Overlapping MPN/myelodysplastic neoplasms (MPN/MDS) and myeloid dysplastic neoplasms are rarely associated with eosinophilia, but eosinophilia may be observed as part of the perturbed hematopoiesis (9, 17, 95).
Figure 2 may serve as a catalog and inspiration for relevant diagnostic groups: autoimmune, infectious, clonal, etc., in the initial approach, emphasizing that the list is not exhaustive and that secondary, reactive causes are the most common (3–7, 20, 55, 64, 95) (Supplementary Tables 1, 2). The listed examples of benign disorders may (all) be associated with T-lymphocyte/cytokine-driven mature eosinophilia in the blood (or tissues, e.g., skin, lung, or gastrointestinal tract) and include common or very rare diagnoses such as asthma exacerbation (96), sarcoidosis (97), rheumatoid arthritis (98), and atopy (99) or IgG4-related diseases (IgG4-RD) (100). Eosinophilia may be part of the diagnostic criteria, e.g., a B-eosinophil count of at least 1 × 109/L (or evidence of extravascular eosinophilic predominant inflammation on biopsy) in eosinophilic granulomatosis with polyangiitis (EGPA, formerly Churg–Strauss syndrome) (75). Similarly, a significant number of eosinophils in the sputum, airway, or blood is required to diagnose eosinophilic asthma (73).
The eosinophil count is frequently increased in parasitic infections (Supplementary Table 2) (87, 88, 101), allergic bronchopulmonary aspergillosis (ABPA) (88, 102), or scabies (88, 103). Eosinophilia is a predominant clinical component in lHES, characterized by marked overproduction of eosinophil factor(s) by dysregulated CD3-CD4+ T cells, which are clonal in most cases (63), and in episodic angioedema with eosinophilia (Gleich syndrome), which is a multilineage cell cycle disorder (104). The entities Eosinophilic Pulmonary Disease (EPD) (71–73) and Eosinophilic Gastrointestinal Diseases (EGID) (78) can be considered working diagnoses, including chronic, immune-mediated disorders with a multifactorial etiology and characterized by an increase in eosinophil-predominant tissue inflammation on biopsy. Organ-specific entities include several specific diagnoses such as eosinophilic esophagitis and Loeffler's syndrome, which are often accompanied by blood eosinophilia. In Loeffler’s syndrome, the eosinophilia is transient, accompanied by fluctuating, mild to severe respiratory symptoms with fever, and interstitial, migratory pulmonary infiltrates. The shading represents an accumulation of eosinophils, most often in response to parasitic infection (69–73, 78, 105) (Supplementary Table 1). Finally, the information provided in Figure 2 may emphasize as clinically important that a patient may have eosinophilia for more than one reason, requiring separate treatments for proper care.
2.4.2 Eosinophilic granulomatosis with polyangiitis
Eosinophilic granulomatosis with polyangiitis (EPGA) (Churg–Strauss) is a rare and potentially life-threatening systemic vasculitis. For all practical purposes, EPGA always develops in patients with pre-existing asthma (74).
The disease is characterized by predominantly small-vessel vasculitis and extravascular necrotizing granulomas associated with eosinophilic inflammation. Most patients have moderate to high blood eosinophil counts. A blood eosinophil count ≥ 1 × 109/L and/or extravascular eosinophilic predominant inflammation on biopsy of affected tissue may support the current diagnostic criteria (75). It has been consistently found that 30%–40% of affected patients have antineutrophil cytoplasmic antibodies (ANCA), which can pose a diagnostic challenge in relation to the more common systemic vasculitis, although these are also rare in a tertiary rheumatology outpatient clinic (Supplementary Table 1 and Figure 2).
The involvement of the lungs is the most common organ affected together with maxillary sinusitis (allergic rhinitis and/or sinus polyposis). Other major manifestations in EGPA involve the skin, peripheral nerves and kidney, as palpable purpura, mononeuritis multiplex and glomerulonephritis, respectively. Less commonly, the heart is involved with congestive heart disease symptoms and subendocardial fibrosis, and the gastrointestinal tract and the eye are affected (74, 75). Therapy includes corticosteroids (CS) and immunosuppressive agents, which overlap with the treatment of iHES.
2.4.3 Histiocytosis and IgG4-related disease
Histiocytoses are very rare diseases. The prediagnostic phase is often long. It is uncommon for histiocytosis alone to present with peripheral eosinophilia, but it does occur, particularly when associated with another myeloid neoplasm. A retrospective study showed that 10% of adults with non-Langerhans cell histiocytosis have a concomitant MPN (106). Therefore, patients with histiocytosis discovered during the evaluation for eosinophilia should be offered bone marrow examination and testing for recurrently mutated myeloid genes. Hodgkinoid histiocytosis—a very rare entity—presents with eosinophilia and may mimic lymphoma (107).
In contrast to peripheral eosinophilia, tissue eosinophilia is common in histiocytosis, particularly Langerhans cell histiocytosis (formerly called eosinophilic granuloma), Erdheim–Chester disease, and ALK-positive histiocytosis (9, 95, 108–110).
In the setting of eosinophilia, the histiocytoses are most relevant as differential diagnoses to IgG4-RD, as the organ manifestations of Langerhans cell histiocytosis and Erdheim–Chester disease may resemble IgG4-RD (100, 108, 109). The distribution of lesions revealed by PET-CT scans may help to differentiate the diseases: bone involvement favors histiocytosis over IgG4-RD. Moreover, observation by imaging of perinephric changes is indicative, and demonstration of flasklike deformation in the distal femur due to meta-diaphyseal osteosclerosis, is pathognomonic for Erdheim-Chester disease. The finding of mutated v-Raf murine sarcoma viral oncogene homolog B (BRAF), rat sarcoma (RAS), or mitogen-activated protein kinase (MAPK) pathway genes supports a histiocytic diagnosis. Rosai–Dorfman disease is another histiocytosis that can be mistaken for IgG4-RD, as IgG4+ cells are often prominent in this condition (100).
It is currently unclear whether the eosinophilic infiltrate in histiocytic diseases is due to the disease itself or a phenomenon secondary to the inflammatory microenvironment.
IgG4-RD is an important differential diagnosis in hypereosinophilia (100). Of 100 patients with eosinophilia evaluated at a tertiary center, 9 had IgG4-RD (66). Presenting features of IgG4-RD are variable but include eosinophilia, allergy and nasal polyposis, salivary gland involvement, lymphadenopathy, sclerosing cholangitis, autoimmune pancreatitis, retroperitoneal fibrosis, and glomerulonephritis. Of note, only approximately 50% of Caucasians with IgG4-RD have elevated IgG4 levels in peripheral blood (100). Moreover, the organ manifestations of the other histiocytic diseases, Langerhans cell histiocytosis and particularly Erdheim–Chester disease may resemble IgG4-RD. PET-CT scans including the extremities to below the knee and evaluation for diabetes insipidus may help to discern between the disorders (108, 109). Kimura’s disease is a rare entity that primarily affects young to middle-aged Asians, typically causing cervical lymphadenopathy, peripheral eosinophilia, and increased IgE levels; it may resemble IgG4-RD and Rosai–Dorfman disease (111). Interestingly, Kimura’s disease has been reported to respond to an anti-Il5 monoclonal antibody (mepolizumab) (112).
2.4.4 Eosinophilia in malignancies
Blood eosinophilia and/or infiltration of eosinophils in the tumor tissue is encountered in patients diagnosed with common solid tumors, and the presence of eosinophilia in blood or infiltrating solid tumors is not consistent in any neoplasm (113). A potential beneficial role may be explained by the secretion of various enzymes and cytokines by eosinophils that influence tumor immunity and reduce tumor progression (114). Severe blood eosinophilia during symptom development may be a diagnostic clue for malignancy and therefore guide the diagnostic process (115, 116). Results indicate that blood eosinophilia may be a positive prognostic factor in some malignant solid tumors, when present (113, 117), whereas the presence of blood eosinophilia after surgical resection may indicate an unfavorable prognosis, relapse, or rapid disease progression (118). The inconsistent observation of blood or tissue eosinophilia in malignant tumor entities and the lack of robust, prospective data indicate that blood eosinophilia may be used cautiously as a simple biomarker in some oncologic patients, similar to a leukemoid reaction. Nonetheless, the numerous reports and studies of eosinophilia in solid tumors add to the possible functions of eosinophil granulocytes in this developing field related to the tumor microenvironment, which awaits further clarification (119, 120).
A unique feature has emerged with the introduction of immune checkpoint inhibitors (ICIs), approved for the treatment of several cancers. Mild to moderate, though rarely severe. blood eosinophilia may be observed in less than 5% of patients, a few weeks to many months after treatment initiation. Eosinophilia may be asymptomatic, and therapy with the ICI may proceed in a small proportion of patients (121, 122). Decisions on treatment strategy are based on the individual patient’s response to targeted treatment, the severity of organ damage, and measures to control the symptoms, including CS treatment. Close monitoring of eosinophil counts, manifestations due to eosinophil activity, and response to the ICI is appropriate. Co-administration of CS to lower the eosinophil count may be acceptable, while a differential diagnosis must be excluded (Figure 2). Blood eosinophilia may persist after discontinuation of ICI therapy, which poses additional concerns regarding monitoring and treatment strategies for eosinophilia and malignant diseases. ICI-induced eosinophilia may have a favorable prognostic impact (122, 123). In a significant percentage of patients with ICI-induced eosinophilia, treatment must be discontinued due to eosinophil-associated organ damage, such as heart, skin, and colon (124) (Supplementary Table 1).
3 Diagnostic workup in patients with eosinophilia
The clinical challenge of identifying a diagnosis in the individual patient with eosinophilia warrants a detailed medical history and examination, in addition to the results of routine blood tests. The circumstances mirror those of patients with MPN, when serial measurements of blood cell counts show increased numbers over time, and specific analyses are often needed for clarification.
Quantification of differential white blood cell counts may be more commonly performed in specialties that treat with immunosuppressants or chemotherapy, in the interest of neutrophil granulocytes and lymphocytes. These treatments may, however, reduce the absolute number of eosinophils or be associated with fluctuating numbers, perhaps masking a concurrent condition related to eosinophilia (Figure 2). Observation of eosinophils in such patients at the end of cycles or in treatment-free periods may be clinically informative, providing clues for extended follow-up, e.g., in a multidisciplinary approach.
Once the presence of a repeatedly elevated eosinophil count has been confirmed, the diagnostic workup can be viewed as a stepwise process as follows:
1. exclusion of secondary causes;
2. evaluation of primary causes; and
3. diagnosis by exclusion of idiopathic hypereosinophilia.
Secondary causes are overall much more common than primary eosinophilia or iHES. A wide variety of diseases may be associated with eosinophilia, and thus a thorough medical history and clinical examination are essential to identify the causes of (secondary) eosinophilia. Relevant information includes familial predisposition, concomitant disorders, previous malignancies, medications, travel, migration and exposures, medications, and the risk of drug reactions (Supplementary Tables 1, 2; Figure 2) (65–88, 101–103, 125, 126). Since all organs may be involved in patients with eosinophilia, it is essential to ask about symptoms and observe for findings, that may not be mentioned or readily identified but may be (highly) relevant in the clinical context.
If no obvious causes of secondary eosinophilia are found, the next step is to evaluate for primary causes. This evaluation includes the following:
a. complete blood cell count;
b. bone marrow biopsy, aspirate, and blood for morphologic studies; and
c. karyotype, molecular analysis, flow cytometry, or fluorescence in situ hybridization (FISH) to determine clonality.
Blood counts and morphology reveal the severity of eosinophilia and abnormalities in other blood cells that may point to an underlying hematologic disease/clonal eosinophilia. Abnormalities in the morphology of eosinophils have been described in HES and CEL, but they may also be seen in reactive conditions. Bone marrow biopsy including morphology, immunophenotyping, cytogenetics, and molecular analysis may reveal an underlying hematologic disease/clonal eosinophilia. In the case of eosinophilia, FISH/cytogenetics and molecular analysis (on bone marrow aspirate or peripheral blood cells) should specifically look for PDGFRA, PDGFRB, FGFR1, FLT3, ETV6, and JAK2 gene rearrangements (Figure 3).
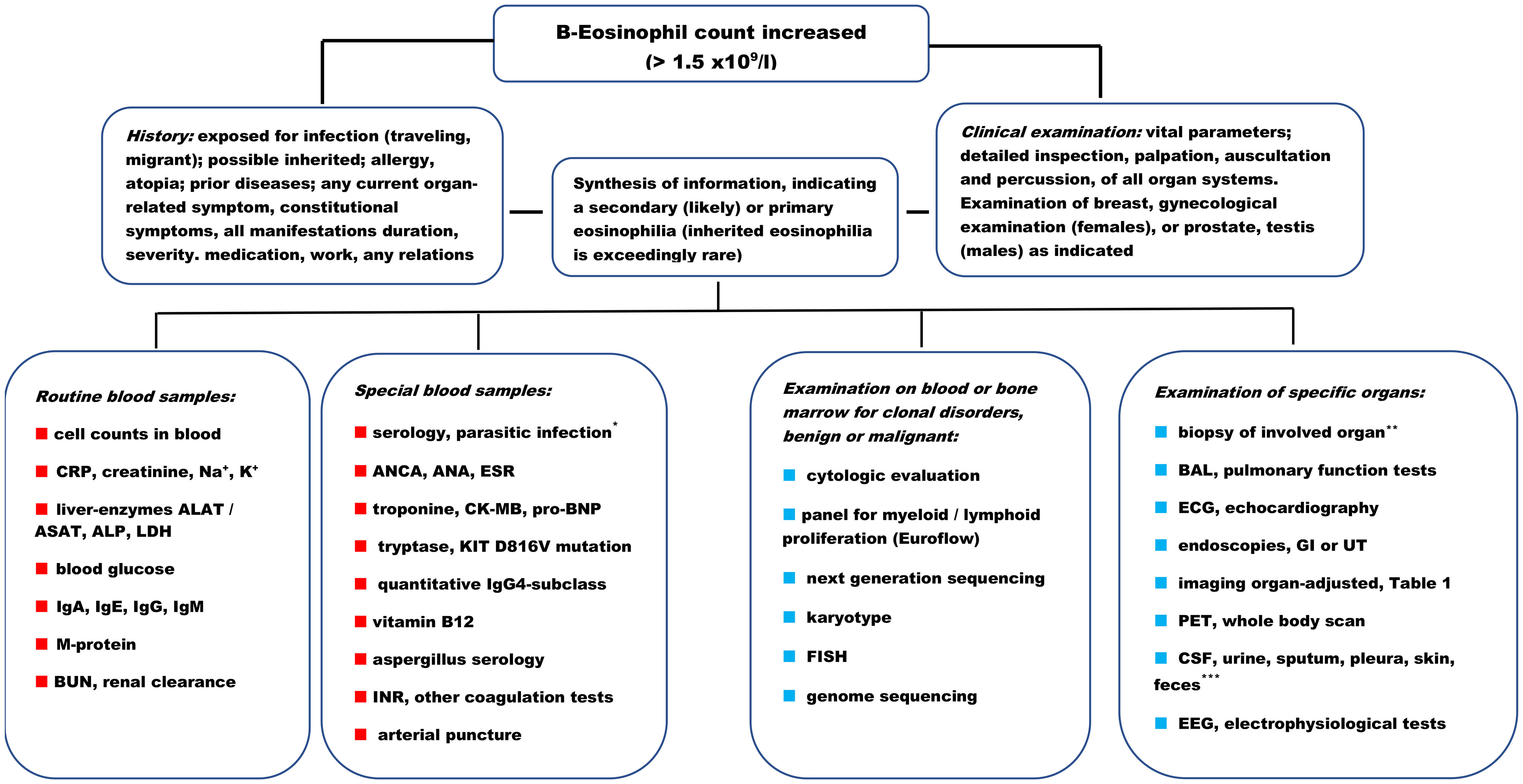
Figure 3 Diagnostic workup in patients with (moderate) eosinophilia. ALAT/ASAT, alanine aminotransferase/aspartate aminotransferase; ALP, alkaline phosphatase; ANA, antinuclear antibodies; ANCA, anti-neutrophil cytoplasmic antibodies; BAL, bronchoalveolar lavage; BUN, blood urea nitrogen; CK-MB, creatine kinase—myocardial band; CRP, C-reactive protein; CSF, cerebrospinal fluid; ECG, electrocardiogram; EEG, electroencephalogram; ESR, erythrocyte sedimentation rate; FISH, fluorescence in situ hybridization; GI, gastrointestinal tract; Ig, immunoglobulin; INR, international normalized ratio; K+, potassium; LDH, lactate dehydrogenase; M-protein, monoclonal protein; Na+, sodium; PET, positron emission tomography; pro-BNP, pro-b-type natriuretic peptide; UT, urinary tract. ⋆ See information provided in Supplementary Table 2. ⋆⋆ Skin, lung, lymph node, nasal polyp, liver, mucosa (GI, UT), muscle, myocardial, kidney, and brain. ⋆⋆⋆ For microscopy, culture, and other diagnostic tests (e.g., Mantoux in the skin). Proposals for blood samples and other tests to be adapted to pre-planned procedures at the department (e.g., routine laboratory packages). Proposals are not prioritized but must be selected and customized to the individual patient.
The diagnosis of iHE or iHES is established when the diagnostic workup for primary and secondary eosinophilia is inconclusive.
Figure 3 presents a flow diagram indicating primary, secondary, and idiopathic eosinophilia (3–7, 17–20, 61). The diagram is also applicable in patients with minimal eosinophilia but is aligned with iHES. The blood cell count may be repeated once or twice, if not retrospectively available over weeks and months, to ascertain a baseline value. The cell count may fluctuate and show a (significant) increase from day to day, which may be associated with worsening symptoms and the need for immediate treatment.
Examination of specific organs with biopsy or specialized analysis like magnetic resonance imaging (MRI), echocardiography, positron emission tomography (PET) scan, or organ function test (especially lung and heart) may be a part of the baseline workup for both secondary and primary causes, iHES, and iHE.
Routinely, patients with eosinophilia can be attended to in the outpatient clinic (67), but the urgency in symptom development, risk in procedures, and access to diagnostic procedures, or onset of treatment, e.g., with CS, may require hospitalization and parallel examination of primary and secondary causes. Access to specialized exams (MRI, PET echocardiography, organ function tests, etc.) may be limited to daytime or weekdays or may not be available at the current institution, which may lead to referral of patients with eosinophilia and acute manifestations to other institutions specialized in this condition.
Documentation of eosinophilic infiltration in tissues, such as skin, heart, kidney, lung, lymph nodes, and bone marrow, should be performed to demonstrate the association with iHES and primary eosinophilia or to help establish the diagnosis of a secondary course. However, an issue may be to commence cytoreductive treatment within hours of having established or recognized the potential association of eosinophilia and critical symptoms, to stabilize the patient and mitigate worsening. Response to treatment in an acute setting may be rapid—from hours to a few days. Therefore, it is valuable for the diagnostic workup if blood samples (and skin biopsy if relevant and bone marrow if possible) are obtained and kept for microscopy, flow cytometry, and clonal mutation analysis before treatment is initiated. If transfer to a tertiary center for eosinophilia is planned, a decision based on a conference with the center, or the regional hematology department is relevant to decide whether blood and bone marrow samples can be obtained for analysis before treatment starts. More invasive procedures or biopsies may be challenging to perform before initiation of treatment or transferal. Performing analysis in responding patients when the patient has a very low blood eosinophil count is unlikely to be similarly informative (Figure 3). The diagnostic process may be delayed, and the analysis may need to be repeated as the CS is tapered and the eosinophil count increases.
In conclusion, the diagnostic workup should be customized to the individual patient, based on organ manifestations (Supplementary Tables 1, 2) and interpretation of the pathophysiologic driver (Figure 2), and translated to conduct the relevant examinations (Figure 3).
In addition to the diagnostic workup, in cases of primary eosinophilia, iHE, and iHES, it may be recommended to register baseline cardiac and pulmonary function tests, notwithstanding any manifestations, but because vital organs are often involved in primary eosinophilia (3–7, 20, 41, 42, 53, 54, 58, 65–67).
4 Treatment of patients with eosinophilia
The first-line treatment in acute circumstances due to eosinophilia is CS, orally or intravenously at high doses (maximum 1 mg/kg prednisolone or equipotent Solu-Medrol), once a day. This is effective in approximately four out of five patients, with a gradual, often cytolytic reduction in the eosinophil count and typically an associated symptom relief. This improvement may be supported by other treatments, such as those for organ failure, infection, or a specific diagnosis, as indicated (Supplementary Tables 1, 2; Figure 2). The effect of CS on eosinophilia is rapid in CS-sensitive patients. CS can reduce the survival and function of eosinophils, block autocrine cytokine signaling, and impact the production of eosinopoietic factors derived from T lymphocytes or other immunoregulatory cells (127–130). It is not possible to predict whether a patient will respond to CS treatment (the first time CS is administered for eosinophilia) and benefit from the often-rapid effect. In patients who do not respond (sufficiently) to CS, this feature may support the interpretation of a myeloid, clonal genesis, driving the eosinophilia and overriding cytokine stimulation of eosinopoiesis, derived from T lymphocytes or macrophages. Patients with the FIP1L1-PDGFRA myeloid neoplasm with a tyrosine kinase fusion (Figure 2) are usually not sensitive to CS (58). The pattern of responsiveness to CS is often characteristic in the individual patient at the time of relapse of primary eosinophilia.
Upon diagnosis of secondary eosinophilia, treatment is initiated according to guidelines, perhaps supported by institutional recommendations, all aimed at reducing or eliminating symptoms and improving quality of life. Treatment may be directed at infectious diseases, inflammatory diseases, including autoimmune diseases, or malignancies accompanied by eosinophilia (Figure 2). Numerous medications are available for the management of this large patient population, which includes almost all patients with eosinophilia, and include antimicrobials, immune suppressants, anti-inflammatory drugs, or chemotherapy. Medical treatment is administered in different ways: orally, parenterally, applied on the skin, inhaled, or in other ways that target specific compartments (e.g., intrathecally), or may involve radiotherapy. CS is an example of an agent used systemically in EGPA, while it is routinely used by inhalation in asthma or ABPA. In addition, drugs supporting organ function may be needed, whether the cause is ascribed to eosinophilia or other factors. The list reflects the standard of care for all internal medicine diagnoses.
If the patient does not improve with treatment, or if (isolated) eosinophilia persists, then a follow-up assessment may be needed to exclude a concomitant disease, representing primary eosinophilia, (other) secondary eosinophilia, or very rare inborn errors of immunity or familial eosinophilia (Supplementary Tables 1, 2; Figure 2). Mild (perhaps moderate) eosinophilia may be acceptable, reflecting the number of eosinophils as a potential biomarker in patients with non-malignant disease who are otherwise, responding satisfactorily and are being monitored regularly according to standard of care (131, 132). However, an increased eosinophil count in patients with solid tumors (118) and Hodgkin’s lymphoma (133) should be followed, reflecting incomplete remission or relapse as secondary eosinophilia (Figure 2).
5 Primary and idiopathic eosinophilia
5.1 Specific diagnoses
The diagnostic entity “myeloid/lymphoid neoplasms with eosinophilia and tyrosine kinase gene fusions” (MLN-TK) was introduced in the 2008 WHO classification (134). The dissection of the genetic aberrations has contributed to identifying and including more patients in this clinically heterogeneous group and added information relevant to prognosis and treatment (9, 95). The neoplasms in this group are driven by constitutively active domains in tyrosine kinase fusion genes and may carry additional mutations in other genes that promote an increase in the number and survival of malignant cells (19, 135–137). Consequently, the pathophysiology of the disease and the clinical presentation of the patients with MLN-TK are very heterogeneous, emphasizing the importance of establishing a correct diagnosis. The application of cytogenetic and molecular analysis can be guided by the history (acute or chronic), examination findings (lymphadenopathy and splenomegaly), and laboratory tests (tryptase, blasts) (Figure 3) (138).
All the specific diagnoses included in the MLN-TK must be BCR-ABL1 negative and instead arise due to rearrangements and abnormal gene products in PDGFRA, PDGFRB, FGFR1, FLT3, ETV6, or JAK2 (9, 95, 135–137). The origin of fusion genes involves cryptic deletions or translocations of chromosomal regions during mitosis in hematopoietic stem cells, which result in dysregulated intracellular signaling and the development of distinct AML, MPN, MDS, overlapping forms, mixed phenotype acute leukemia, and T- or B-ALL or lymphoma.
Figure 4 provides examples of the clinical presentation and management of MLN-TK, representing the diversity of disease in primary, neoplastic (intrinsic) eosinophilia. The figure is not exhaustive, as the individual patient may present with variable symptoms from different organ systems (Supplementary Table 1). The partner combinations of the fusion genes in MLN-TK influence the clinical presentation, and a more—in this context—common partner and the associated phenotype is presented as an example in each of the six categories (Figure 4). Specific features that may be observed in blood samples, are indicated, but are not universally observed and may be influenced by variations in disease dynamics, patient comorbidity, and latency or initiation of treatment before referral for examination, e.g., anemia, thrombocytopenia, and related symptoms. In principle, all organs may be involved in MLN-TK (Supplementary Table 1), and the manifestations and clinical course from the presentation may be similar to those of acute or chronic leukemia (Figure 4).
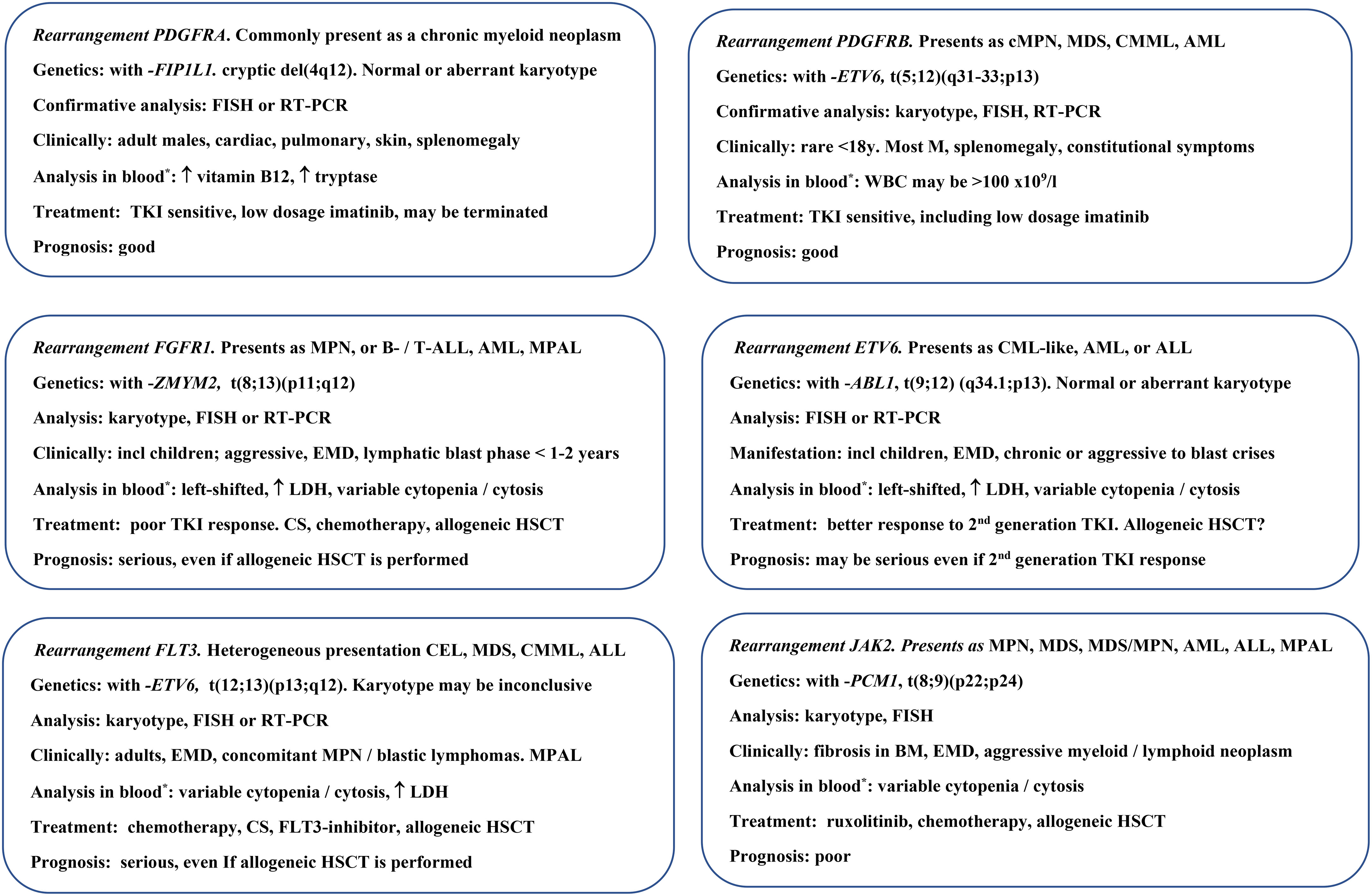
Figure 4 Myeloid/lymphoid neoplasms with eosinophilia and tyrosine kinase fusions (MLN-TK). One disease with a specific rearrangement occurring in the MLN-TK is described briefly. ABL1, abelson1; ALL, acute lymphocytic leukemia/lymphoblastic lymphoma; AML, acute myeloid leukemia; BM, bone marrow; CEL, chronic eosinophilic leukemia; CML, chronic myeloid leukemia; CMML, chronic myelomonocytic leukemia; MPN, myeloproliferative neoplasm; CS, corticosteroid; del, deletion; EMD, extramedullary disease; ETV6, ETS variant transcription factor 6; FGFR1, fibroblast growth factor receptor 1; FIP1L1, Factor interacting with PAPOLA and CPSF1; FISH, fluorescence in situ hybridization; FLT3, fms-related receptor tyrosine kinase 3; HSCT hematopoietic stem cell transplantation; incl, including; JAK2, Janus kinase 2; LDH, lactate dehydrogenase; M, male; MDS, myelodysplastic neoplasm; MPAL, mixed-phenotype acute leukemia; PCM1, Pericentriolar material 1; PDGFRA/B, platelet-derived growth factor A or B; RT-PCR, reverse transcription polymerase chain reaction; t, translocation; TKI, tyrosine kinase inhibitor, here: imatinib, dasatinib, and ponatinib; WBC, white blood cell count; ZMYM2, Zinc Finger MYM-Type Containing 2; *eosinophilia, mild–severe, almost always present.
Eosinophilia is a hallmark of patients with MLN-TK that develops de novo but may be absent in a minority of patients. The increase in blood eosinophils may be mild to severe, and variable within the same MLN-TK entity. This feature reflects the complexity of the perturbed cell biology and the importance of identifying the partner gene through different analyses for clonality to confirm the correct diagnosis and possibly initiate a targeted therapy (Figures 3, 4). The number of potential partners is different for each fusion gene, but one gene can be involved in different fusion gene relations, and the number of genes and related pathways involved is increasing, with at least 72 fusion gene combinations overall in MLN-TK (9, 19, 95, 135–138). A challenge in the diagnostic process is how to combine panels and methodologies with varying sensitivity and specificity in bone marrow samples (Figures 3, 4). The partner in a rearrangement may not always be identified at diagnosis. Tissue samples may also be taken from enlarged lymph nodes, skin, or organs, and samples may be stored in the freezer for additional analysis if needed later.
Eosinophilia is the dominant feature of blood cell analysis in CEL and the most frequent PDGFRA-associated MLN-TK (9, 58, 139). The entity CEL is characterized by persistent hypereosinophilia for at least 4 weeks, organ involvement due to eosinophilia, and evidence of both clonality and abnormal bone marrow morphology (e.g., erythroid or megakaryocytic dysplasia), but does not require increased blasts (≥2% in peripheral blood or 5%–19% in bone marrow). The former CEL “not otherwise specified (NOS),” has, by this revised description, been left out of the fifth WHO classification (9, 95, 134). The result of clonal analysis in patients with CEL must exclude the other MLN-TKs specifically as primary eosinophilia, and acute or chronic MPN in general, defined by cytogenetic or mutational criteria in the WHO classification (9, 95). The information provided by cytogenetic, mutational, and cytologic analysis justifies that CEL represents an independent MPN (Figures 2, 4), which often presents with organ involvement due to eosinophilia, and may share clinical features with PDGFRA-FIPL1 MLN-TK. CEL is different from iHE or iHES, both benign conditions, and is defined by persistent hypereosinophilia in the absence of a clonal or reactive cause, by clonality, and abnormal bone marrow morphology (140). Mutational analysis for a single or concurrent clonal driver in patients with CEL has been reported in a variety of genes involved in myeloproliferation, such as JAK2, additional sex combs like 1 (ASXL1), chaperonin containing TCP1 subunit 6B (CCT6B), tet methylcytosine dioxygenase 2 (TET2), enhancer of zeste homolog 2 (EZH2), Casitas B-lineage lymphoma (CBL), or signal transducer and activator of transcription (STAT). The clinical phenotype may therefore be differentially associated with different genotypes (141–144). Next-generation sequencing (NGS) or polymerase chain reaction (PCR) analysis can be performed in cases without clonality by other tests to examine the differential diagnosis of CEL and iHEUS or iHES, which may be therapeutically important, demonstrating a potential target (Figures 2–4).
Eosinophilia may be observed in a minority of patients with MPNs such asPV, PMF, or ET. However, it may be difficult to disentangle eosinophilia as part of the neoplastic process in these cases and, alternatively, it is appropriate to consider eosinophilia in these patients to be secondary, reactive to another condition. The diagnosis of an infectious or inflammatory condition in a patient with classic Philadelphia-negative MPN is imperative for optimal management (Supplementary Tables 1, 2; Figures 2, 3).
5.2 Treatment of primary and idiopathic eosinophilia
The approach may be wait-and-watch or may include any symptomatic treatment pending diagnostic clarification, such as antibiotics, xanthine oxidase inhibition, and fluid replacement, as indicated by the clinical circumstances since the dynamics and manifestations in the conditions are variable (Supplementary Table 1; Figures 2, 4). Unless diagnostic information is available at an early stage, e.g., by flow cytometry in AML, CS may be part of a first-line treatment to reduce symptoms and the blood eosinophil count. The final treatment strategy is decided by shared decision-making with the patient, based on full information and a complete diagnostic analysis (Figure 3). Participation in a clinical trial is recommended for all patients with primary eosinophilia and iHES, if possible. No treatment is indicated for eosinophilia in iHES.
Imatinib is authorized by the FDA and EMA for the treatment of advanced iHES and MLN-TK with FIP1L1-PDGFRA rearrangement, and mepolizumab is approved as an add-on treatment for adult patients with inadequately controlled iHES without an identifiable non-hematologic secondary cause. The administration of a tyrosine kinase inhibitor (TKI) or anti-IL5 monoclonal antibody (anti-IL5 mAB) is rational given the pathophysiology of iHES and MLN-TK with FIP1L1-PDGFRA, which involves the potential stimulation of eosinophils by IL-5 (23–27, 145, 146) and a highly sensitive constitutively active tyrosine kinase (58, 139, 147), respectively.
The treatment strategy in all patients other than MLN-TK with FIP1L1-PDGFRA in the first line is therefore based on established use and extrapolation, and a highly individual assessment. This includes information on the diagnosis of CEL, type of MNL-TK or iHES, symptoms, comorbidity, and patient preferences. Adverse events or a planned pregnancy may impact the decision during treatment (3–7, 20, 61, 62, 64, 65). Treatment of primary eosinophilia and iHES includes one or more drugs to reduce and preferably normalize the eosinophil count and any additional medications indicated to mitigate symptoms caused by eosinophilia and organ symptoms. Supportive treatment is highly individualized and may involve all internal medicine specialties (Supplementary Table 1).
Figure 4; Table 1 present the treatment options in MNL-TK, CEL, and iHES. Given the pathophysiologic mechanisms in MLN-TK, information on the clonal nature may indicate the use of TKI, chemotherapy, high-dose cytotoxic regimens, and stem cell support, including allogeneic hematopoietic stem cell transplantation (HSCT), with variable outcomes. Treatment of FIP1L1-PDGFRA MLN-TK shows a very high rate of durable complete remissions to low-dose imatinib, including undetectable residual disease by FISH or quantitative reverse transcriptase (RT) PCR. The potential cure of the patient is reflected by the discontinuation of imatinib in a small group of FIP1L1-PDGFRA MLN-TK patients (58). In contrast, the diversity of the diagnoses is reflected by indications for AML or ALL regimens in other patients of the same entity (Figure 4).
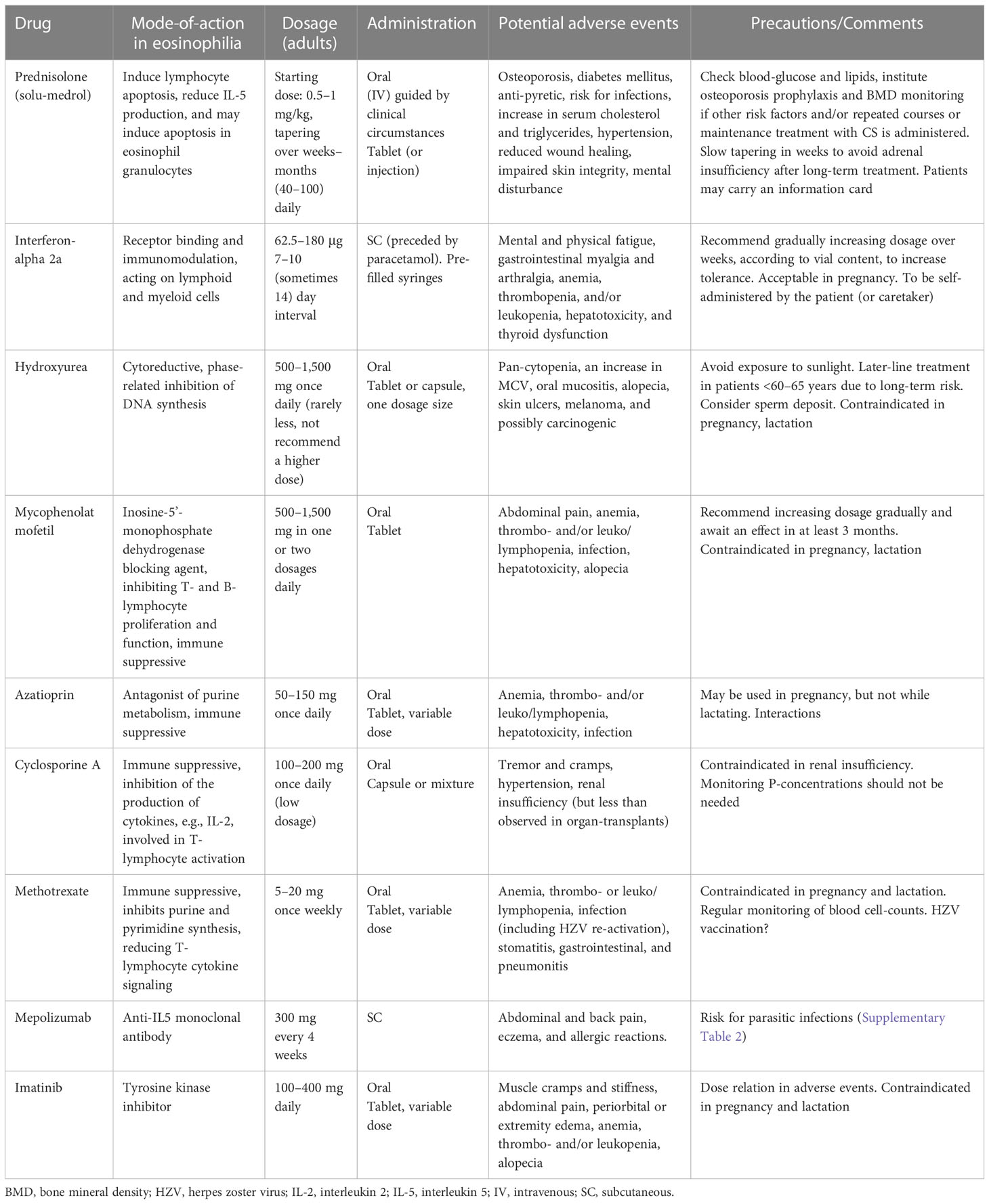
Table 1 Treatment options in chronic eosinophilic leukemia and idiopathic hypereosinophilic syndrome.
The treatment of CEL and iHES reflects the possible lymphoid or myeloid nature since the specific mechanism of the disease is not known in iHES and may not be translated from a clonal finding to a therapeutic agent in CEL (Table 2). There are no randomized clinical trials (RCTs) or robust data to support international agreement on the first or subsequent lines of treatment, after CS, and the decision will depend on the evaluation of the individual patient and treatment options.
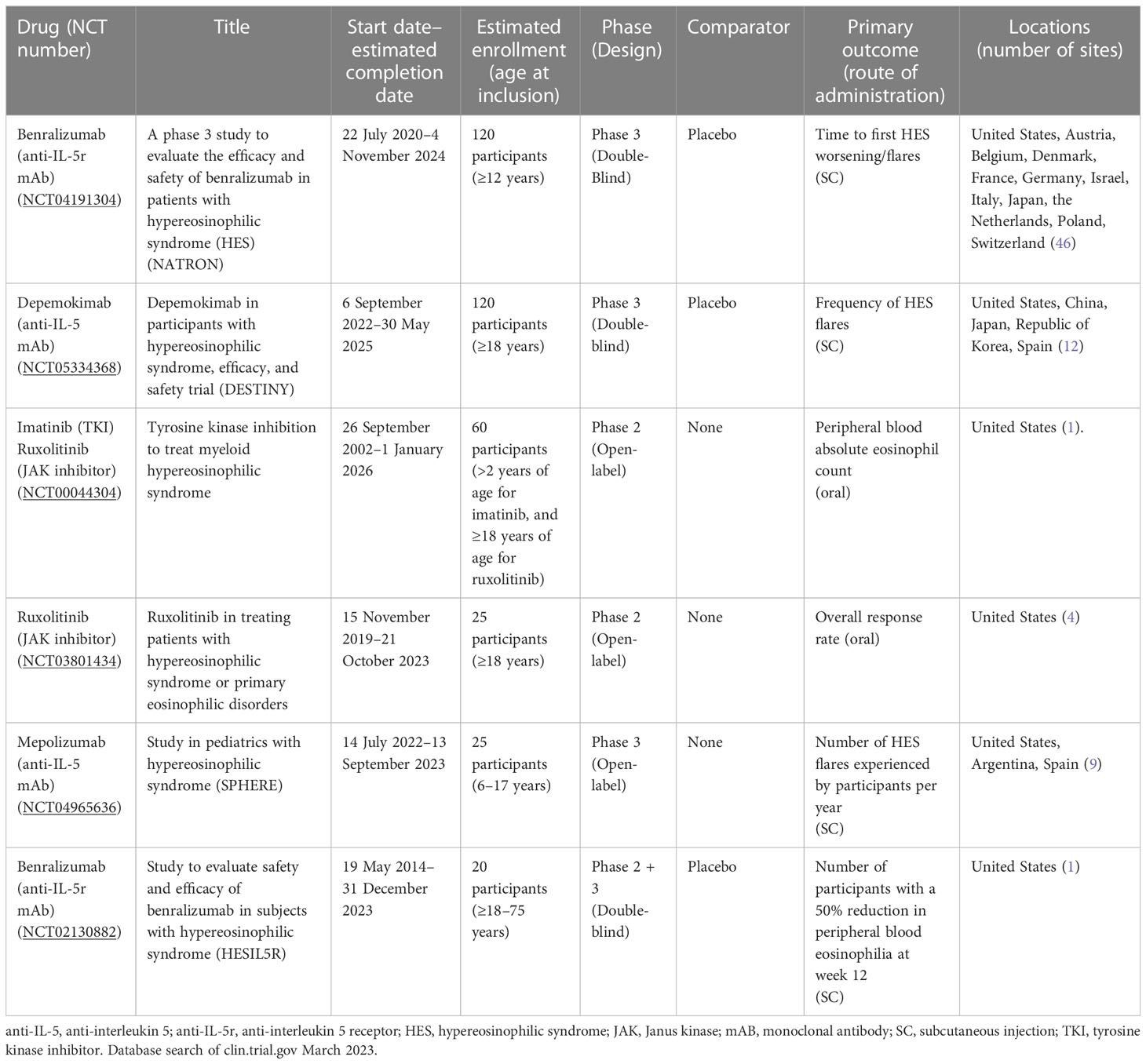
Table 2 Ongoing clinical trials in patients with primary eosinophilia.
CS is the drug of choice when immediate treatment is indicated in CEL and iHES, until clarification. Maintenance treatment, if CS is effective, should include steroid-sparing agents, due to the chronic nature or repeated need for CS, while tapering CS. Lack of CS sensitivity may indicate a “myeloid” phenotype, supporting, for example, interferon-alpha or hydroxyurea as a non-targeting treatment as the next line of treatment. Access to serum IL-5 or other cytokine levels may guide treatment with an immunosuppressive drug. However, validated and robust prospective results are not available, and pretreatment with CS may impact the analysis (145). The decision to introduce methotrexate, azathioprine, cyclosporine, or mycophenolate, instead of, for example, interferon-alpha or hydroxyurea, remains a clinical one (Table 1). The administration of these drugs is supported by case reports, small studies, retrospective analyses, and established use extrapolating from experience in lymphoproliferative and myeloproliferative diseases (63, 104, 148–151) (Table 2).
The lowest dose of CS or any agent should be used, and combination treatment may be administered, as in selected cases with PV or PMF, to reduce adverse events and maintain optimal efficacy. Efficacy may last from weeks to 2 - 3 months, preferably introducing only one drug at a time. Prophylaxis against osteoporosis should be initiated at an early stage in CS-sensitive patients with risk factors for bone density reduction, as CS may be used for months and repeatedly. Prophylactic antimicrobials for Pseudomonas infection may be contemplated in selected patients with chronic lung disease and long-term therapy with immunosuppressive agents (Table 1).
Imatinib is approved for advanced iHES, which is a heterogeneous group clinically identified with persistent symptoms due to eosinophilia, and unresponsive to administered lines of treatment. Imatinib may be effective in CEL or iHES because fusion genes, not detected by analysis, may be sensitive to TKI (152). A standard dose may be started and tapered if effective to the lowest effective dosage. Response to any treatment in CEL or iHES is variable (Table 1).
There are no internationally agreed-upon definitions of response to treatment in primary eosinophilia or iHES. Reduction in symptoms, flares, eosinophil count (complete response requires durable normalization), and any biomarker, particularly the clonal marker, may reflect a satisfactory effect.
Irrespective of the choice of treatment in CEL or iHES, drug discontinuation may be planned after months to years of treatment. It may be reasonable to taper the dosage, considering the drug and being aware that relapse of symptoms, typically manifested at the time of diagnosis is a risk. Patients with rare diagnoses such as primary eosinophilia or iHES should continue to be monitored and treated in specialized departments.
6 Ongoing research in primary eosinophilia
Several clinical trials have been completed or are ongoing with anti-IL5 biologicals in patients with secondary eosinophilia, such as eosinophilic asthma (153), eosinophilic esophagitis (154), and EGPA (155). The results of two RCTs have been published (145, 146) and several clinical studies are ongoing in targeted therapies regarding iHES and clonal eosinophilia. The rarity of these patients is a concern in the planning of clinical studies, and most centers may only be able to enroll one or two patients in a trial. This is a burden for the individual (hematology) department and may be a reason to decline participation. Referral to centers may be a way to mitigate this challenge, but the administrative work and bureaucracy are a challenge for the conduct of clinical studies, which may impact research activity in primary and idiopathic eosinophilia (156).
Table 2 provides information on six trials currently ongoing in Western countries, some of which are still recruiting. The table reflects the challenge due to the rarity of the diseases to conduct active comparator RCTs, instead of “physician’s choice,” which, in primary eosinophilia and iHES, may be very heterogeneous (Table 1 and Figure 4). This may impact the interpretation of the outcome and the option for blinding the study. Alternatively, blinding of the randomized trial is possible and valuable in placebo-controlled designs, which isolate the effect of the experimental treatment even as an add-on to a standard of care, e.g., CS and hydroxyurea. Inclusion criteria are defined across all ages, reflecting the age distribution of patients with this diagnostic entity. The trials in pediatric patients are of particular interest in order to mitigate any long-term effects of alternative immunosuppressive, immunomodulating, or cytoreductive treatments. It is also an added value for adult patients with iHES or primary eosinophilia to offer biological therapy to achieve disease control by targeted agents with acceptable safety profiles, possibly lifelong, as in all MPNs.
The primary outcomes of the trials are listed and reflect the interest in restricting eosinophilia (by blood cell count) or symptoms (by the rate of response or flares), which are rational and objective endpoints and relevant to patients to reflect a treatment benefit. In this context, the information presented in Table 2 shows that the administration of all agents in the current trials is either orally or subcutaneously, which is beneficial for chronic treatments and allows home administration. If possible, novel drugs in clinical trials for primary eosinophilia or iHES administered intravenously should be avoided in order to reduce patients’ time consumption/travel and stay at the hospital during treatment, and to reduce the use of resources at the department. This pattern, reflected in Table 2, is endorsed.
Dexpramipexole is an orally bioavailable synthetic aminobenzothiazole that has demonstrated encouraging results when treating HES with this potentially steroid-sparing agent (157, 158). One trial was started in 2014, but the status of the open-label, phase 2 study to evaluate the safety and efficacy of dexpramipexole (KNS-760704) in adults with iHES is unknown (NCT02101138).
Clinical studies of a second-generation TKI targeting BCR-ABL1, like dasatinib and nilotinib in the second line in patients with FIP1L1-PDGFRA MLN-TK, failing imatinib, or a JAK2-targeting TKI, like ruxolitinib, have possibly met the challenges of conducting clinical studies, even single-arm trials, in rare populations. One consequence may be the off-label use of these drugs, but it is pivotal to accumulate data on their efficacy and safety in patients with MLN-TK. This may be supported by centralized treatment of the patients or reporting to international registries.
7 Quality of life in primary and idiopathic eosinophilia
Patient-reported outcome (PRO) measures are today recognized as key endpoints in all clinical trials within hematological disorders (159). For BCR-ABL1-negative MPN, disease-specific tools for quality of life (QoL) assessment have been developed, e.g., the Myeloproliferative Neoplasm (MPN) Symptom Assessment Form Total Symptom Score (MPN-SAF-TSS) in ET, PV, and PMF (160), and in myelofibrosis specifically (161). The symptom burden among patients with MPN is highly correlated with QoL (162).
However, no specific tool to capture PRO in iHES, MLN-TK, or CEL has been developed and validated, and the MPN-SAF-TSS did not when established, include patients with these rarer acute and chronic myeloid conditions. Currently, general questionnaires like the European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30) (163, 164), the simpler EuroQol 5-dimensional questionnaire (EQ-5D-5L) (165), or the Patient Reported Outcome Measurement Information System (PROMIS) Short Form (SF) (166) are implemented and recommended in the monitoring of patients and clinical trials in oncology (166, 167). The EORTC-QLQ-C30 in particular has the advantage of being available in more than 100 languages and having electronic records, which may be useful in clinical trials. These tools may be feasible for capturing relevant subjective issues in patients with iHES or primary eosinophilia. The data on QoL are registered as secondary or exploratory endpoints and may therefore be of limited value in single-arm studies or otherwise unblinded trials due to the risk of bias. The multi-faceted manifestations of the target population (Supplementary Table 1) pose a challenge when trying to develop one homogeneous questionnaire in clinical trials of idiopathic and primary eosinophilia (Figures 2, 4). The placebo-controlled, blinded RCT of mepolizumab in iHES included QoL registered by SF12 (145). The survey demonstrated that baseline parameters were similar in the experimental and control groups and that QoL did not deteriorate during the study period. QoL measures are included in many ongoing trials (Table 2). Robust studies of QoL in primary eosinophilia, iHE, and iHES outside a clinical trial have not been done.
Tools like the Patient Global Impression of Change Item (PGIC) or the Patient Global Impression of Severity Item (PGIS) may be acceptable in clinical studies and for population studies due to the lack of more specific measures (168, 169). The Physician Global Assessment (PGA) has been used in several clinical settings as a disease activity instrument on a visual analog scale and was originally developed for systemic lupus erythematosus (170). However, PGA may not be adequate from an overall perspective in iHES or clonal eosinophilia because, although some symptoms may be objective, several are not (Supplementary Table 1), and the PGA may also be biased, influenced by the physician’s experience and circumstances of evaluation.
Thus, today, information regarding QoL in iHES and clonal eosinophilia outside clinical trials should be captured and monitored by detailed interviews with the individual patient due to the known plethora of symptoms in the population. This is a time-consuming challenge in the clinic, and electronic tools for comparing symptoms and variables, e.g., cell counts in blood, may be an important tool to improve the inclusion of this vital information when monitoring patients in the future (171).
8 Multidisciplinary team in eosinophilia
8.1 Description of the collaboration
A multidisciplinary team (MDT) in a hospital is a function specifically suited to cases with complex care needs due to the variable symptoms, diagnostic challenges, and individualized treatment. MDTs are appropriate for rare diseases because expertise is required to provide optimal care and coordinating work in professional MDTs also promotes improvement in patient management. This has been well described in the management of patients with benign or malignant surgical and medical disorders and in research (172–177). MDTs may also be called tertiary centers.
Establishing an MDT has to take into account the different facilities and disciplines at hand, and the effort necessary in an MDT requires a number of clinical and diagnostic facilities to join the collaboration. MDTs are most often organized in regional or university hospitals with centralized functions in several specialties, and thus with extensive and recurrent interaction with local/regional hospitals based on collaborating policies. This development is in line with the centralization of certain functions, to aim for and maintain the highest degree of competence. MDTs and centralized functions reflect the same interest but differ in—at least—the fact that centralized functions are often allocated to one department based on daily routines, whereas MDTs are only operational when several diagnostic and clinical departments have established and agreed to a manner in which to collaborate, as a local policy. The centralized function is expected to run 24/7, whereas MDTs typically have planned meetings at weekly intervals.
A tertiary center for eosinophilia is a specialized function serving a large population since the number of patients with a primary or idiopathic cause in need of specialized treatment at the department of hematology and the incidence of complex secondary cases is low. Inborn errors of immunity and familial cases are exceedingly rare (Figure 2). The population of Denmark is 5.85 million (in 2021), and two MDTs were allocated by government decision in 2017 at two university hospitals, each in a different part of the country. One is in the capital region (at Rigshospitalet, in Eastern Denmark) and the other is in the Southern Denmark region (at Odense University Hospital). Both MDTs are open to referrals from all five regions of the country, primarily for adult patients. Individual patients with eosinophilia can decide which MDT is more convenient for them to attend, but the contact with local/regional departments can be continuous due to the collaboration between departments at different institutions. Similarly, tertiary centers for other rare diagnoses have been established at Danish university hospitals. The Center for Eosinophilia is physically located in the Department of Hematology and collaborates with the six other hematology departments in Denmark, which are routinely involved in the management of patients following an initial referral at a regional level. The Department of Hematology may be appropriate to host the MDT due to the special differential diagnosis, including idiopathic and primary eosinophilia, and also including secondary cases of histiocytosis, malignant lymphoma, and leukemia, whereas the majority of secondary eosinophilia cases are optimally treated at other specialized departments (Supplementary Tables 1, 2; Figures 2–4).
8.2 Elements and benefits of an eosinophilia MDT
Figure 5 shows the principles of patient flow and functions in an eosinophilia MDT. It is important that GPs are also aware of the tertiary centers, e.g., through the dissemination of knowledge at regional meetings and in national medical journals (67, 178) (level 1) and that the specialized departments at the MDT hospital all serve as a filter for a second opinion in the MDT (level 2). Furthermore, GPs should be aware that there are no formal criteria for listing a case for an upcoming conference, which is planned regularly every 4–6 weeks. The MDT program can be planned 6 months in advance, each meeting lasting 60–75 min. The upcoming conference is announced via a mailing list to the colleagues in the MDT network and is sent out in advance with anonymized information on usually three to five patients. More detailed information can be retrieved in the secure areas of the hospital’s electronic filing system, which can be shared with all other hospitals in the region. The email information includes a video link for virtual participation in the MDT, which has been a positive outcome of the COVID pandemic (179). In this way, videoconferencing facilitates participation. The two centers for eosinophilia in Denmark organize conferences together four times a year to disseminate knowledge. This activity is made possible due to the use of virtual rooms. In principle, these conferences are open to all interested colleagues (nationwide) and participation is optional. The schedule for the MDT can include fixed days or be a rolling sequence to accommodate the numerous other activities on the ward, in the outpatient clinic, and at other conferences.
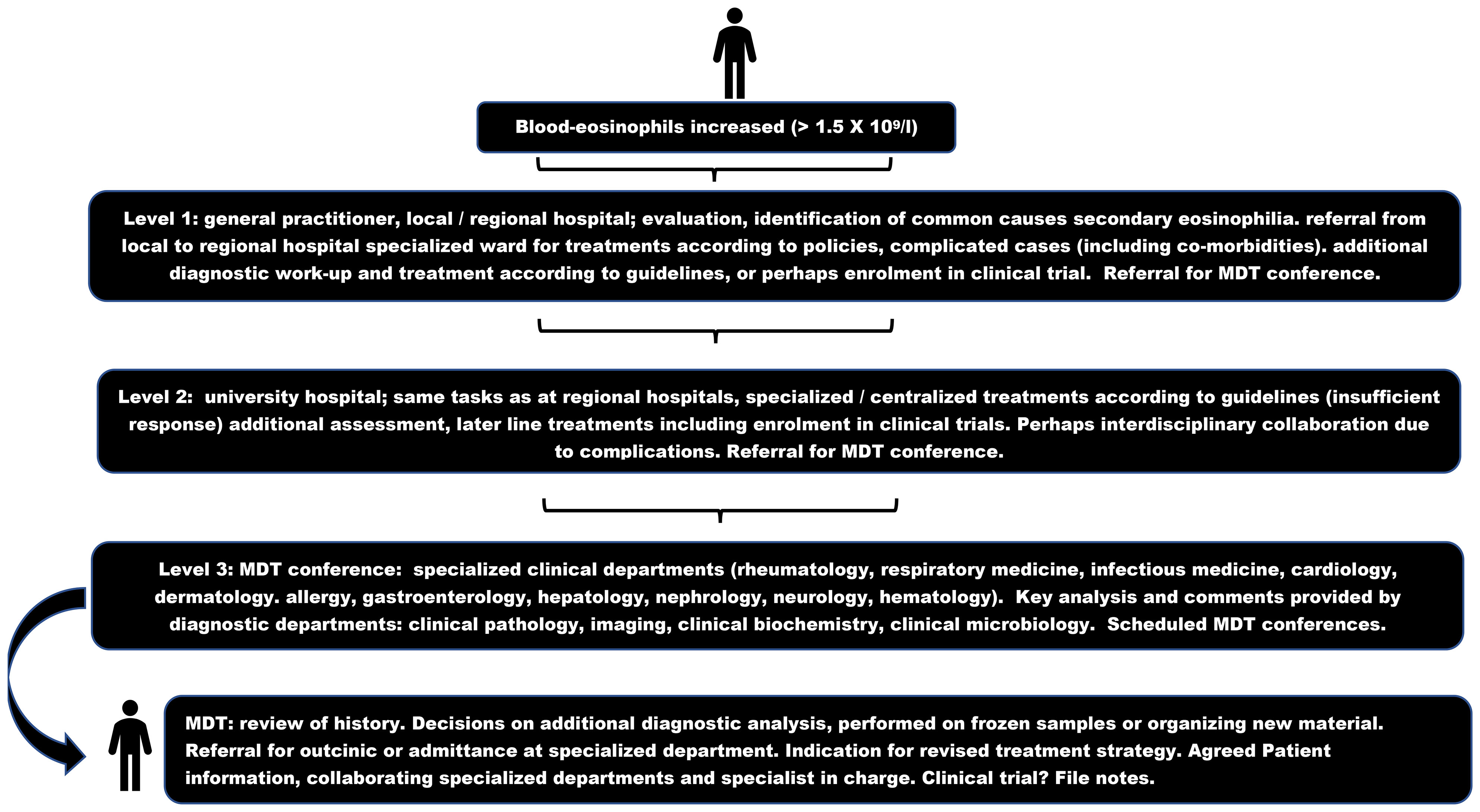
Figure 5 Multidisciplinary team flowchart in eosinophilia. MDT multidisciplinary team.
A major benefit of the organization of an MDT in eosinophilia is that it allows for direct contact with colleagues participating in the MDT during normal working hours. Colleagues can be contacted via an MDT telephone list and are more familiar with the task, and thus are more likely to be able to provide a qualified opinion directly than can be expected from both junior and senior doctors who are generally on-call. Naturally, cases can be discussed in a department within the MDT network, between on-call colleagues and colleagues participating in an MDT, if this is more feasible. It is our experience that an option for personal contact, through telephone lists for the MDT, is one of the aspects facilitating the process when, for various reasons (clinical circumstances, time, and presence) a discussion cannot await the next scheduled MDT to make decisions.
Figure 5 illustrates that most patients are referred from highly specialized departments at the MDT hospital or from collaborating hematology departments (67). The individual patient is presented by the physician most familiar with the case (most often the treating specialist). The case presentation may be in PowerPoint format, which can support the educational dimension of MDT conferences. Patients can be discussed in the MDT either during admission to the hospital or during follow-up in the outpatient clinic, reflecting the wide range of symptoms and severity in the target population (Supplementary Tables 1, 2; Figures 2–4). The purpose of discussing an eosinophilia case in the MDT is to agree on a second opinion, including the need for additional diagnostic tests, e.g., due to persistent eosinophilia and symptoms despite relevant treatment for secondary eosinophilia, and also to establish diagnoses of iHE and iHES per exclusionem. The next step is a treatment decision, according to the working diagnosis, to be implemented at the appropriate specialized department, either in the outpatient clinic or during admission to the ward. The scheduled conferences, both in the individual center and in the two national centers, must always include a plan for informing the patient (usually by phone) and any department or function involved (either by verbal information or by referral in writing). All decisions should be recorded as a conference note, and the next MDT will provide the opportunity for follow-up (Figure 5).
9 Discussion
A patient-centered function is fit for purpose due to the complex and challenging manifestations, diagnostics, and options for targeted or revised therapeutic strategy in a small proportion of adult patients with eosinophilia. This is the first presentation of the rationale for the MDT in eosinophilia (Supplementary Tables 1, 2; Table 1 and Figures 2–4). The MDT function is a well-established tool across medical disciplines (172–177), and MDTs have been implemented in departments treating eosinophilic esophagitis, possibly improving patient outcomes (180, 181), and have also been considered in Loeffler’s endocarditis (182). However, one difference between the MDT for patients with eosinophilia and other scheduled MDTs is that the MDT for eosinophilia typically starts by challenging and discussing the working diagnosis (Figure 5), whereas the diagnosis has been established unquestionably in (almost all referred patients) MDTs. The number of clinical and diagnostic departments in an eosinophilia MDT is high, requiring input from all medical specialties and diagnostic expertise (Figure 5). MDTs for established diagnoses in one specialty include additional expertise in specific fields, such as radiotherapists, physiotherapists, specially trained nurses, and nutritionists.
The MDT conferences in eosinophilia, if executed virtually, require an optimal technology for sound and image quality (179), and the sharing of specific parts of the patient’s files among the MDT participants. These may include data from blood samples, medical history and clinical findings, CT-PET-MRI scans and descriptions, and light microscopy images of tissue samples. It is very important to prioritize the patient information and decide on the physician in charge of the next steps, and the procedures. Activities must take precautions to avoid disclosure of personal data when disseminating information by mail or virtual systems.
The MDT forum can facilitate educational activities, sharing of experiences at all levels of medical training and specialization. Moreover, the collaboration between the two MDTs in Denmark supports the possibility of participating in international clinical trials, e.g., in iHES (Table 2), because the potential number of patients to be included is higher than in the individual centers. The accumulation and interest of patients with eosinophilia in MDTs facilitate research, e.g., cohort studies in chronic lymphocytic leukemia demonstrating the impact of eosinophilia at diagnosis (183) and a retrospective study advocating PCR analysis for T-cell receptor status in the diagnostic workup (Figures 2, 3), to be performed only if clonality has been demonstrated by flow analysis of lymphocyte subpopulations in blood or bone marrow samples (67).
The differential count in blood and readily identifiable eosinophil granulocytes in blood smear (Figure 1) are a simple source of information to guide toward the broad spectrum of conditions associated with eosinophilia, as opposed to conditions characterized by isolated neutrophilia, monocytosis, or lymphocytosis (1, 2). While isolated blood eosinophilia is characteristic of iHE, concomitant aberrations in other cell lines indicate other hematologic conditions, including iHES and MPNs, in addition to eosinophilia due to secondary causes (Figure 2). The biology of eosinophil granulocytes is well described (21–44), as is their role in various pathophysiologic states (Supplementary Tables 1, 2; Figure 2). The narration of eosinophil functions expanded from “a phagocyte” in innate immunity to a potential key player in the orchestration of homeostasis, normal development, and remodeling (15, 26, 28, 38). However, results from genetic knock-out models in animals, and more recently the possibility to observe any impact of treatments that deplete circulating eosinophils by IL-5 and IL-5 receptor-targeting treatments in functional knock-out humans, challenge the notion of the precise role of eosinophils in health (184–187). More robust results in patients treated with anti-IL5 biologicals or other targeted treatments, in primary or secondary eosinophilia, lowering the eosinophil count durably and maximally as well as research in this field is warranted.
Eosinophils are distributed after extravasation in numerous tissues, but it remains to be understood in more detail what triggers eosinophils to cause various end-organ manifestations in the individual patient (Supplementary Table 1). The distribution of eosinophils in human tissues is normally organ dependent and varies considerably. The distribution may be explained by tissue-specific chemokines or reflect the existence of eosinophil subpopulations in vivo (26, 29, 188, 189). The impact of cell subpopulations in primary or idiopathic eosinophilia has not been studied but may contribute to explaining the manifestations in different organs (65).
Current isotope scintigraphy is not readily applicable to eosinophils, in contrast to the information obtained from tracing neutrophils with a clinical benefit in diagnosis and treatment (190). An eosinophil-specific tracing technique could be a major step forward in the diagnosis and management of patients with eosinophilia, replacing or supporting invasive procedures. Perhaps monoclonal antibodies targeting epitopes, preferentially present on eosinophils, such as the IL5-receptor (Table 2) or siglec-8, could be labeled with an isotope serving as a tracer. However, cell death upon binding to the eosinophil plasma membrane would (most likely) be rapidly induced (191, 192). It may be considered whether antibody-functionalized magnetic particle imaging tracers could be a technique applicable to eosinophil granulocytes (193). Currently, imaging techniques indicating inflammation, like PET or gadolinium MRI and biopsies, remain part of the gold standard to demonstrate the involvement of eosinophils in damage.
The natural history of iHE and iHES, including triggering events for progression, is not well understood. Data on the population are available in retrospective, descriptive studies, which indicate the presence of severe anemia, hepatosplenomegaly, older age, and cardiac involvement in a scoring system to be prognostic. Patients with a low-risk score have a 5-year survival of over 95%, while a high-risk score indicates a 5-year survival of 62% (20, 194). Prospective MDT-orchestrated studies and multicenter studies can be a tool to accumulate data, as in the ongoing French COHESION study started in 2019 (NCT04018118). Similarly, the U.S. longitudinal study of familial hypereosinophilia started in 2005 (NCT00091871), may clarify details of the natural history of these rare disorders.
The number of eosinophils in the blood is not itself well-correlated with manifestations in patients with iHES (194, 195). Data have been presented that end-organ damage, to a variable extent in heart, lung, skin, and other tissues, may be explained by extravasation of eosinophils during the process, which affects the eosinophil count, and the risk of symptoms due to eosinophilia does not increase proportionately with counts higher than 1 × 109/L. The clinical implication is that a normal level or even a low number of eosinophilic granulocytes in circulation is not a safeguard for excluding the risk for eosinophilic involvement in symptomatic patients (196, 197). The clinical implication is that the number of eosinophils in the blood may not in itself be a risk factor in hypereosinophilia, and the clinical assessment and indication for treatment in asymptomatic patients require careful patient information to react to symptoms. The clinical explanation for a correlation between symptoms and eosinophil count, when treatment is started, may therefore reflect the effect of lowering an increased eosinophil count and the clearance of eosinophils in the affected tissues.
Finally, the prognostic information of the blood eosinophil count on admission to the emergency department has been studied in a large, unselected, adult population. Moderate or severe eosinophilia is a risk factor for a significantly increased 3-month mortality, in patients older than 70 years with hematologic disease and an elevated C-reactive protein (198). The results emphasize that awareness of the eosinophil count is a diagnostic clue in the management of hypereosinophilic patients to reduce diagnostic delay, especially of the underlying malignancy (8, 198) (Figure 2).
The iHEUS and iHES, respectively, may be examined in more detail at diagnosis to improve the classification. Whole exome sequencing and genome-wide methylation analysis identifying novel disease-associated mutations and methylation patterns, may be appropriate tools to convert the idiopathic status into identifiable mutation-driven entities (90, 141–144). A proportion of cases may thus be contextualized within the MLN-TK or CEL groups, and perhaps be of therapeutic relevance. Casuistic reports of MPN or MDS presenting as iHES, reflecting a diagnostic overlap may not represent a pathophysiologic continuum (199). Rather, the reports reflect the complexity of establishing a strict classification in the chronic myeloid neoplasms with eosinophilia.
The introduction of IL-5 targeting treatment in neoplastic or idiopathic hypereosinophilia mirrors the increasing interest in recent years in mABs targeting the IL-5 pathway for the treatment of hypereosinophilic conditions such as severe asthma and EGPA (33, 153, 200). Table 2 shows that trials are ongoing in two mABs against free IL-5 with mepolizumab or a long-acting formulation (depemokimab), both of which neutralize IL-5 and prevent receptor binding. One study involves an mAB targeting IL-5r (benralizumab). Preliminary, encouraging results from the trial (NCT02130882) on the efficacy and safety of the concept of receptor binding-induced antibody-dependent cellular cytotoxicity of eosinophils in iHES have been presented (201). Reslizumab, a different mAB against free IL-5, may be a candidate for the treatment of iHES (191). Therapeutic trials in the pipeline to support the ongoing studies in MLN-TK, CEL, and iHES (Table 2), may include TKIs targeting FRGFR, FLT3, or STAT pathways, anti-IgE mABs, perhaps anti-CD52 mABs, and biologicals interfering with IL signaling, all of which have been studied in other diseases (202, 203). All agents may be CS-sparing but are also associated with adverse events that must be included in the benefit–risk assessment to induce longer remissions and disease control in chronic conditions. siglec-8 may be a target for treating iHES and primary eosinophilic conditions in RCTs (92, 204, 205). Still, evidence-based treatment algorithms are missing on eosinophil-directed agents, as are additional guidelines for thrombotic prophylaxis in the target population. Current guidelines in eosinophilia are excellent, describing agents for individualized treatment while taking age, comorbidity, manifestations, and information on cytogenetic and mutational drivers into account (3–7, 17, 18, 20, 58, 61, 136, 137, 145–152) (Table 1; Figure 4).
QoL is reduced in symptomatic patients with neoplastic or idiopathic eosinophilia and may also be influenced by adverse events to CS or other treatments, which may not outweigh the benefit of symptom reduction (Table 1). The development of a disease-specific PRO is important to register and monitor the consequences of eosinophilia and therapeutic interventions. The first important steps have been taken to introduce and validate a questionnaire and to decide on endpoints to be implemented in clinical trials and care (206).
10 Conclusion
The observation of eosinophilia in the differential count or blood smear is common and should always merit a reflection as to why it is present. This may, in almost all cases, be readily explained by the diagnostic workup. However, the remaining cases with persistently increased counts and variable symptoms despite adequate interventions, or without a proper diagnosis, may be discussed in a patient-centered MDT. This activity is justified by the pathophysiologic basis and clinical manifestations involving medical and diagnostic specialties. It remains to be demonstrated that the activity in this forum translates to a clinical benefit in patient QoL, overall management, and prognosis. An MDT at a tertiary center can be instrumental to generate data, providing education, and contributing to research. The function supports not only the hematologic subpopulation of patients but also patients with eosinophilia in general.
Author contributions
GT, CA, HV, and OB designed the project and drafted a major part of the manuscript, Tables 1, 2; Figures 2–5. HL, JD, KA, CM, AK, TH, SB-O, MM, SJ, and OB created Supplementary Table 1. CH and RM-I created Supplementary Table 2. MBM created Figure 1, and MC created Table 2. DEF wrote the section on histiocytosis and IgG4-related disease. All authors contributed to the article and approved the submitted version.
Acknowledgments
The authors acknowledge the support from—and patient-centered discussions with—referring colleagues from both primary and secondary care.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1193730/full#supplementary-material
References
1. Tefferi A, Curtis AH, Inwards DJ. How to interpret and pursue an abnormal complete blood cell count in adults. Mayo Clin Proc (2005) 80(7):923–36. doi: 10.4065/80.7.923
2. Leach M. Interpretation of the full blood count in systemic disease – a guide for the physician. J R Coll Physicians Edinb (2014) 44(1):36–41. doi: 10.4997/JRCPE.2014.109
3. Tefferi A, Patnaik MM, Pardanani A. Eosinophilia: secondary, clonal and idiopathic. Br J Haematol (2006) 133(5):468–92. doi: 10.1111/j.1365-2141.2006.06038.x
4. Butt NM, Lambert J, Ali S, Beer PA, Cross NCP, Duncombe A, et al. Guideline for the investigation and management of eosinophilia. Br J Haematol (2017) 176(4):553–72. doi: 10.1111/bjh.14488
5. Nordic MPN Study Group. Care program for the diagnosis and treatment of eosinophilia 3rd version (2018). Available at: https://www.nmpn.org/index.php/guidelines (Accessed March 10, 2023).
6. Shomali W, Gotlib J. World health organization-defined eosinophilic disorders: 2022 update on diagnosis, risk stratification, and management. Am J Hematol (2022) 97(1):129–48. doi: 10.1002/ajh.26352
7. Klion AD. Approach to the patient with suspected hypereosinophilic syndrome. Hematol Am Soc Hematol Educ Program (2022) 2022(1):47–54. doi: 10.1182/hematology.2022000367
8. Chen B, Fu Y, Wang Z, Rong Q, Zhang Q, Xie J, et al. Eosinophilia attention, diagnosis, treatment, and awareness in physicians: a cross-sectional survey. Ther Adv Chronic Dis (2023) 14:20406223221146938. doi: 10.1177/20406223221146938
9. Khoury JD, Solary E, Abla O, Akkari Y, Alaggio R, Apperley JF, et al. The 5th edition of the world health organization classification of haematolymphoid tumours: myeloid and histiocytic/dendritic neoplasms. Leukemia (2022) 36(7):1703–19. doi: 10.1038/s41375-022-01613-1
10. Hasselbalch HC, Bjørn ME. MPNs as inflammatory diseases: the evidence, consequences, and perspectives. Mediators Inflammation (2015) 2015:102476. doi: 10.1155/2015/102476
11. Andersen M, Sajid Z, Pedersen RK, Gudmand-Hoeyer J, Ellervik C, Skov V, et al. Mathematical modelling as a proof of concept for MPNs as a human inflammation model for cancer development. PloS One (2017) 12(8):e0183620. doi: 10.1371/journal.pone.0183620
12. Masselli E, Pozzi G, Gobbi G, Merighi S, Gessi S, Vitale M, et al. Cytokine profiling in myeloproliferative neoplasms: overview on phenotype correlation, outcome prediction, and role of genetic variants. Cells (2020) 9(9):2136. doi: 10.3390/cells9092136
13. Fisher DAC, Fowles JS, Zhou A, Oh ST. Inflammatory pathophysiology as a contributor to myeloproliferative neoplasms. Front Immunol (2021) 12:683401. doi: 10.3389/fimmu.2021.683401
14. Nasillo V, Riva G, Paolini A, Forghieri F, Roncati L, Lusenti B, et al. Inflammatory microenvironment and specific T cells in myeloproliferative neoplasms: immunopathogenesis and novel immunotherapies. Int J Mol Sci (2021) 22(4):1906. doi: 10.3390/ijms22041906
15. Kouro T, Takatsu K. IL-5- and eosinophil-mediated inflammation: from discovery to therapy. Int Immunol (2009) 21(12):1303–09. doi: 10.1093/intimm/dxp102
16. Ramirez GA, Yacoub M-R, Ripa M, Mannina D, Cariddi A, Saporiti N, et al. Eosinophils from physiology to disease: a comprehensive review. BioMed Res Int (2018) 2018:9095275. doi: 10.1155/2018/9095275
17. Roufosse FE, Goldman M, Cogan E. Hypereosinophilic syndromes. Orphanet J Rare Dis (2007) 2:37. doi: 10.1186/1750-1172-2-37
18. Curtis C, Ogbogu P. Hypereosinophilic syndrome. Clin Rev Allergy Immunol (2016) 50(2):240–51. doi: 10.1007/s12016-015-8506-7
19. Reiter A, Gotlib J. Myeloid neoplasms with eosinophilia. Blood (2017) 129(6):704–14. doi: 10.1182/blood-2016-10-695973
20. Helbig G, Klion AD. Hypereosinophilic syndromes – an enigmatic group of disorders with an intriguing clinical spectrum and challenging treatment. Blood Rev (2021) 49:100809. doi: 10.1016/j.blre.2021.100809
21. Shamri R, Xenakis JJ, Spencer LA. Eosinophils in innate immunity: an evolving story. Cell Tissue Res (2011) 343(1):57–83. doi: 10.1007/s00441-010-1049-6
22. Yu C, Cantor AB, Yang H, Browne C, Wells RA, Fujiwara Y, et al. Targeted deletion of a high-affinity GATA-binding site in the GATA-1 promoter leads to selective loss of the eosinophil lineage in vivo. J Exp Med (2002) 195(11):1387–95. doi: 10.1084/jem.20020656
23. Rothenberg ME, Hogan SP. The eosinophil. Annu Rev Immunol (2006) 24:147–74. doi: 10.1146/annurev.immunol.24.021605.090720
24. Blanchard C, Rothenberg ME. Biology of the eosinophil. Adv Immunol (2009) 101:81–121. doi: 10.1016/S0065-2776(08)01003-1
25. Park YM, Bochner BS. Eosinophil survival and apoptosis in health and disease. Allergy Asthma Immunol Res (2010) 2(2):87–101. doi: 10.4168/aair.2010.2.2.87
26. Simon HU, Yousefia S, Germica N, Arnold IC, Haczkud A, Karaulov AV, et al. The cellular functions of eosinophils – collegium international allergologicum (CIA) update 2020. Int Arch Allergy Immunol (2020) 181(1):11–23. doi: 10.1159/000504847
27. Caral DC, Negrao-Correa D, Teixeira MM. Mechanisms underlying eosinophil trafficking and their relevance in vivo. Histol Histopathol (2000) 15:899–920. doi: 10.14670/HH-15.899
28. Wechsler ME, Munitz A, Ackerman SJ, Drake MG, Jackson DJ, Wardlaw AJ, et al. Eosinophils in health and disease: a state-of-the-art review. Mayo Clin Proc (2021) 96(10):2694–707. doi: 10.1016/j.mayocp.2021.04.025
29. Weller PF, Spencer LA. Functions of tissue-resident eosinophils. Nat Rev Immunol (2017) 17(12):746–60. doi: 10.1038/nri.2017.95
30. Acharya KR, Ackerman SJ. Eosinophil granule proteins: form and function. J Biol Chem (2014) 289(25):17406–15. doi: 10.1074/jbc.R113.546218
31. Melo RCN, Wang H, Silva TP, Imoto Y, Fujieda S, Fukuchi M, et al. Galectin-10, the protein that forms charcot-Leyden crystals, is not stored in granules but resides in the peripheral cytoplasm of human eosinophils. J Leukoc Biol (2020) 108(1):139–49. doi: 10.1002/JLB.3AB0220-311R
32. Rutten B, Young S, Rhedin M, Olsson M, Kurian N, Syed F, et al. Eosinophil-derived neurotoxin: a biologically and analytically attractive asthma biomarker. PloS One (2021) 16(2):e0246627. doi: 10.1371/journal.pone.0246627
33. McBrien CN, Menzies-Gow A. The biology of eosinophils and their role in asthma. Front Med (Lausanne) (2017) 4:93. doi: 10.3389/fmed.2017.00093
34. Renz H, Bachert C, Berek C, Hamelmann E, Levi-Schaffer F, Raap U, et al. Physiology and pathology of eosinophils: recent developments. summary of the focus workshop organized by DGAKI. Scand J Immunol (2021) 93(6):e13032. doi: 10.1111/sji.13032
35. Petreccia DC, Nauseef WM, Clark RA. Respiratory burst of normal human eosinophils. J Leuk Biol (1987) 41(4):283–8. doi: 10.1002/jlb.41.4.283
36. Sedgwick JB, Vrtis RF, Gourley MF, Busse WW. Stimulus-dependent differences in superoxide anion generation by normal human eosinophils and neutrophils. J Allergy Clin Immunol (1988) 81(5 Pt 1):876–83. doi: 10.1016/0091-6749(88)90945-1
37. Ueki S, Melo RC, Ghiran I, Spencer LA, Dvorak AM, Weller PF. Eosinophil extracellular DNA trap cell death mediates lytic release of free secretion competent eosinophil granules in humans. Blood (2013) 121(11):2074–83. doi: 10.1182/blood-2012-05-432088
38. Rosenberg HF, Dyer KD, Foster PS. Eosinophils: changing perspectives in health and disease. Nat Rev Immunol (2013) 13(1):9–22. doi: 10.1038/nri3341
39. Hassani M, van Staveren S, van Grinsven E, Bartels M, Tesselaar K, Leijte G, et al. Characterization of the phenotype of human eosinophils and their progenitors in the bone marrow of healthy individuals. Haematologica (2020) 105(2):e52–6. doi: 10.3324/haematol.2019.219048
40. van Dongen M, Lhermitte L, Böttcher S, Almeida J, van der Velden VHJ, Flores-Montero J, et al. EuroFlow antibody panels for standardized n-dimensional flow cytometric immunophenotyping of normal, reactive and malignant leukocytes. Leukemia (2012) 26(9):1908–75. doi: 10.1038/leu.2012.120
41. Wallace KL, Elias MK, Butterfield JH, Weiler CR. Hypereosinophilic syndrome and thrombosis: a retrospective review. J Allergy Clin Immunol (2013) 131(2):441. doi: 10.1016/j.jaci.2012.12.1105
42. Leiva O, Baker O, Jenkins A, Brunner AM, Al-Samkari H, Leaf RK, et al. Association of thrombosis with hypereosinophilic syndrome in patients with genetic alterations. JAMA Network Open (2021) 4(8):e2119812. doi: 10.1001/jamanetworkopen.2021.19812
43. Cugno M, Marzano AV, Lorini M, Carbonelli V, Tedeschi A. Enhanced tissue factor expression by blood eosinophils from patients with hypereosinophilia: a possible link with thrombosis. PloS One (2014) 9(11):e111862. doi: 10.1371/journal.pone.0111862
44. Marx C, Novotny J, Salbeck D, Zellner KR, Nicolai L, Pekayvaz K, et al. Eosinophil-platelet interactions promote atherosclerosis and stabilize thrombosis with eosinophil extracellular traps. Blood (2019) 134(21):1859–72. doi: 10.1182/blood.2019000518
45. Laufer P, Chryssanthopoulos C, Laufer R, Hause LL. The determination of the eosinophil count: comparison of two techniques. J Allergy Clin Immunol (1987) 79(3):438–41. doi: 10.1016/0091-6749(87)90360-5
46. Hartl S, Breyer M-K, Burghuber OC, Ofenheimer A, Schrott A, Urban MH, et al. Blood eosinophil count in the general population: typical values and potential confounders. Eur Respir J (2020) 55:1901874. doi: 10.1183/13993003.01874-2019
47. Pongdee T, Manemann SM, Decker PA, Larson NB, Moon S, Killian JM, et al. Rethinking blood eosinophil counts: epidemiology, associated chronic diseases, and increased risks of cardiovascular disease. J Allergy Clin Immunol Global (2022) 1:233–40. doi: 10.1016/j.jacig.2022.09.001
48. Winkel P, Statland BE, Saunders AM, Osborn H, Kupperman H. Within-day physiologic variation of leukocyte types in healthy subjects as assayed by two automated leukocyte differential analyzers. Am J Clin Pathol (1981) 75(5):693–700. doi: 10.1093/ajcp/75.5.693
49. Kim DW, Shin MG, Yun HK, Kim SH, Shin JH, Suh SP, et al. Incidence and causes of hypereosinophilia (corrected) in the patients of a university hospital. Korean J Lab Med (2009) 29(3):185–93. doi: 10.3343/kjlm.2009.29.3.185
50. Bansal R, Kaur A, Suri AK, Kaur P, Bansal M, Kaur R. Incidence of eosinophilia in rural population in north India: a study at tertiary care hospital. Ann Path Lab Med (2017) 4(1):A–43. doi: 10.21276/APALM.2017.1044
51. Andersen CL, Lindegaard H, Vestergaard H, Siersma VD, Hasselbalch HC, de Fine Olivarius N, et al. Risk of lymphoma and solid cancer among patients with rheumatoid arthritis in a primary care setting. PloS One (2014) 9(6):e99388. doi: 10.1371/journal.pone.0099388
52. Brigden M, Graydon C. Eosinophilia detected by automated blood cell counting in ambulatory north American outpatients. Arch Pathol Lab Med (1997) 121(9):963–7.
53. Hardy WR, Anderson RE. The hypereosinophilic syndromes. Ann Intern Med (1968) 68(6):1220–9. doi: 10.7326/0003-4819-68-6-1220
54. Chusid MJ, Dale DC, West BC, Wolff SM. The hypereosinophilic syndrome: analysis of fourteen cases with review of the literature. Med (Baltimore) (1975) 54(1):1–27. doi: 10.1097/00005792-197501000-00001
55. Valent P, Klion AD, Horny H-P, Roufosse F, Gotlib J, Weller PF, et al. Contemporary consensus proposal on criteria and classification of eosinophilic disorders and related syndromes. J Allergy Clin Immunol (2012) 130(3):607–12.e9. doi: 10.1016/j.jaci.2012.02.019
56. Mattis DM, Wang SA, Lu CM. Contemporary classification and diagnostic evaluation of hypereosinophilia. Am J Clin Pathol (2020) 154(3):305–18. doi: 10.1093/AJCP/AQAA056
57. Crane MM, Chang CM, Kobayashi MG, Weller PF. Incidence of myeloproliferative hypereosinophilic syndrome in the united states and an estimate of all hypereosinophilic syndrome incidence. J Allergy Clin Immunol (2010) 126(1):179–81. doi: 10.1016/j.jaci.2010.03.035
58. Rohmer J, Couteau-Chardon A, Trichereau J, Panel K, Gesquiere C, Abdelali RB, et al. Epidemiology, clinical picture and long-term outcomes of FIP1L1-PDGFRA-positive myeloid neoplasm with eosinophilia: data from 151 patients. Am J Hematol (2020) 95(11):1314–23. doi: 10.1002/ajh.25945
59. Burris D, Rosenberg CE, Schwartz JT, Zhang Y, Eby MD, Abonia JP, et al. Pediatric hypereosinophilia: characteristics, clinical manifestations, and diagnoses. J Allergy Clin Immunol Pract (2019) 7(8):2750–8.e2. doi: 10.1016/j.jaip.2019.05.011
60. Pallesen KAU, Herlin T, Holm M, Høst C, Christiansen M, Ramsing M, et al. Idiopathic hypereosinophilic syndrome: a rare diagnosis in children. Clin Case Rep (2020) 8(10):2013–6. doi: 10.1002/ccr3.3165
61. Klion AD. Eosinophilia: a pragmatic approach to diagnosis and treatment. Hematol Am Soc Hematol Educ Program (2015) 2015:92–7. doi: 10.1182/asheducation-2015.1.92
62. Roufosse F, Cogan E, Goldman M. Recent advances in pathogenesis and management of hypereosinophilic syndromes. Allergy (2004) 59(7):673–89. doi: 10.1111/j.1398-9995.2004.00465.x
63. Carpentier C, Verbanck S, Schandené L, Heimann P, Trépant A-L, Cogan E, et al. Eosinophilia associated with CD3–CD4+ T cells: characterization and outcome of a single-center cohort of 26 patients. Front Immunol (2020) 11:1765(11). doi: 10.3389/fimmu.2020.01765
64. Sheikha J, Weller PF. Advances in diagnosis and treatment of eosinophilia. Curr Opin Hematol (2009) 16(1):3–8. doi: 10.1097/MOH.0b013e32831c841f
65. Ogbogu PU, Bochner BS, Butterfield JH, Gleich GJ, Huss-Marp J, Kahn JP, et al. Hypereosinophilic syndrome: a multicenter, retrospective analysis of clinical characteristics and response to therapy. J Allergy Clin Immunol (2009) 124(6):1319–25.e3. doi: 10.1016/j.jaci.2009.09.022
66. Moller D, Tan J, Gauiran DTV, Medvedev N, Hudoba M, Carruthers MN, et al. Causes of hypereosinophilia in 100 consecutive patients. Eur J Haematol (2020) 105(3):292–301. doi: 10.1111/ejh.13437
67. Hougaard M, Thomsen GN, Kristensen TK, Lindegaard HM, Davidsen JR, Hartmeyer GN, et al. A retrospective cohort study of patients with eosinophilia referred to a tertiary centre. Dan Med J (2022) 69(4):A07210558.
68. Fourzali K, Yosipovitch G, Maderal A. An approach to hypereosinophilic syndrome presenting with cutaneous features. Dermatitis (2022) 33(6):387–95. doi: 10.1097/DER.0000000000000803
69. Ammirati E, Frigerio M, Adler ED, Basso C, Birnie DH, Brambatti M, et al. Management of acute myocarditis and chronic inflammatory cardiomyopathy: an expert consensus document. Circ Heart Fail (2020) 13(11):e007405. doi: 10.1161/circheartfailure.120.007405
70. Brambatti M, Matassini MV, Adler ED, Klingel K, Camici PG, Ammirati E. Eosinophilic myocarditis: characteristics, treatment, and outcomes. J Am Coll Cardiol (2017) 70(19):2363–75. doi: 10.1016/j.jacc.2017.09.023
71. Jeong YJ, Kim K-II, Seo IJ, Lee CH, Lee KN, Kim KN, et al. Eosinophilic lung diseases: a clinical, radiologic, and pathologic overview. Radiographics (2007) 27(3):617–37. doi: 10.1148/rg.273065051
72. Cottin V. Eosinophilic lung diseases. Clin Chest Med (2016) 37(3):535–56. doi: 10.1016/j.ccm.2016.04.015
73. Jackson DJ, Wechsler ME. Eosinophilic lung diseases (ERS monograph). Sheffield Eur Resp Soc (2022) 238 p. doi: 10.1183/2312508X.erm9522
74. Greco A, Rizzo MI, Virgilio AD, Gallo A, Fusconi M, Ruoppolo G, et al. Churg-Strauss syndrome. Autoimmun Rev (2015) 14(4):341–8. doi: 10.1016/j.autrev.2014.12.004
75. Grayson PC, Ponte C, Suppiah R, Robson JC, Craven A, Judge A, et al. 2022 American College of rheumatology/European alliance of associations for rheumatology classification criteria for eosinophilic granulomatosis with polyangiitis. Ann Rheum Dis (2022) 81(3):309–14. doi: 10.1136/annrheumdis-2021-221794
76. Fokkens WJ, Lund VJ, Hopkins C, Hellings PW, Kern R, Reitsma S, et al. European Position paper on rhinosinusitis and nasal polyps 2020. Rhinology (2020) 58(Suppl S29):1–464. doi: 10.4193/Rhin20.600
77. Lange B, Thilsing T, Al-kalemji A, Baelum J, Martinussen T, Kjeldsen A. The sino-nasal outcome test 22 validated for Danish patients. Dan Med Bull (2011) 58(2):A4235.
78. Walker MM, Potter M, Talley NJ. Eosinophilic gastroenteritis and other eosinophilic gut diseases distal to the oesophagus. Lancet Gastroenterol Hepatol (2018) 3(4):271–80. doi: 10.1016/S2468-1253(18)30005-0
79. Titlić M, Kodzoman K, Loncar D. Neurologic manifestations of hypereosinophilic syndrome–review of the literature. Acta Clin Croat (2012) 51(1):65–9.
80. Lee D, Ahn T-B. Central nervous system involvement of hypereosinophilic syndrome: a report of 10 cases and a literature review. J Neurol Sci (2014) 347(1-2):281–7. doi: 10.1016/j.jns.2014.10.023
81. Gauckler P, Shin JI, Mayer G, Kronbichler A. Eosinophilia and kidney disease: more than just an incidental finding? J Clin Med (2018) 7(12):529. doi: 10.3390/jcm7120529
82. Hasan A, Abdel-Al I, Nafie K, Rashad MF, Abozied H, Elhussiny MEA, et al. Clinicopathological characteristics and outcomes of eosinophilic cystitis: a retrospective study. Ann Med Surg (Lond) (2021) 68:102626. doi: 10.1016/j.amsu.2021.102626
83. Olbrich P, Aljaro PO, Freeman AF. Eosinophilia associated with immune deficiency. J Allergy Clin Immunol Pract (2022) 10(5):1140–53. doi: 10.1016/j.jaip.2022.02.016
84. Okamoto K, Morio T. Allergology international 2021. inborn errors of immunity with eosinophilia. Allergology Int (2021) 70(4):415–20. doi: 10.1016/j.alit.2021.08.008
85. Klion AD, Law MA, Riemenschneider W, McMaster ML, Brown MR, Horne M, et al. Familial eosinophilia: a benign disorder? Blood (2004) 103(11):4050–5. doi: 10.1182/blood-2003-11-3850
86. Babu SP, Chen Y-YK, Bonne-Annee S, Yang J, Maric I, Myers TG, et al. Dysregulation of interleukin 5 expression in familial eosinophilia. Allergy (2017) 72(9):1338–45. doi: 10.1111/all.13146
87. Ustianowski A, Zumla A. Eosinophilia in the returning traveler. Infect Dis Clin North Am (2012) 26(3):781–9. doi: 10.1016/j.idc.2012.05.004
88. O’Connell EM, Nutman TB. Eosinophilia in infectious diseases. Immunol Allergy Clin North Am (2015) 35(3):493–522. doi: 10.1016/j.iac.2015.05.003
89. Alaggio R, Amador C, Anagnostopoulos I, Attygalle AD, de Oliveira Araujo IB, Berti E, et al. The 5th edition of the world health organization classification of haematolymphoid tumours: lymphoid neoplasms. Leukemia (2022) 36(7):1720–48. doi: 10.1038/s41375-022-01620-2
90. Andersen CL, Nielsen HM, Kristensen LS, Søgaard A, Vikeså J, Jønson L, et al. Whole-exome sequencing and genome-wide methylation analyses identify novel disease associated mutations and methylation patterns in idiopathic hypereosinophilic syndrome. Oncotarget (2015) 6(38):40588–97. doi: 10.18632/oncotarget.5845
91. Haferlach T, Winkemann M, Löffler H, Schoch R, Gassmann W, Fonatsch C, et al. The abnormal eosinophils are part of the leukemic cell population in acute myelomonocytic leukemia with abnormal eosinophils (aml m4eo) and carry the pericentric inversion 16: a combination of may-Grünwald-Giemsa staining and fluorescence in situ hybridization. Blood (1996) 87(6):2459–63. doi: 10.1182/blood.V87.6.2459.bloodjournal8762459
92. Naymagon L, Marcellino B, Mascarenhas J. Eosinophilia in acute myeloid leukemia: overlooked and underexamined. Blood Rev (2019) 36:23–31. doi: 10.1016/j.blre.2019.03.007
93. Fournier B, Balducci E, Duployez N, Clappier E, Cuccuini W, Arfeuille C, et al. B-ALL with t(5;14)(q31;q32); IGH-IL3 rearrangement and eosinophilia: a comprehensive analysis of a peculiar IGH-rearranged b-ALL. Front Oncol (2019) 9:1374. doi: 10.3389/fonc.2019.01374
94. Langabeer SE. The eosinophilic variant of chronic myeloid leukemia. EXCLI J (2021) 20:1608–09. doi: 10.17179/excli2021-4462
95. Arber DA, Orazi A, Hasserjian RP, Borowitz MJ, Calvo KR, Kvasnicka H-M, et al. International consensus classification of myeloid neoplasms and acute leukemias: integrating morphologic, clinical, and genomic data. Blood (2022) 140(11):1200–28. doi: 10.1182/blood.2022015850
96. Nakagome K, Nagata M. Involvement and possible role of eosinophils in asthma exacerbation. Front Immunol (2018) 9:2220. doi: 10.3389/fimmu.2018.02220
97. Renston JP, Goldman ES, Hsu RM, Tomashefski JF Jr. Peripheral blood eosinophilia in association with sarcoidosis. Mayo Clin Proc (2000) 75(6):586–90. doi: 10.4065/75.6.586
98. Chen Z, Bozec A, Ramming A, Schett G. Anti-inflammatory and immune-regulatory cytokines in rheumatoid arthritis. Nat Rev Rheumatol (2019) 15(1):9–17. doi: 10.1038/s41584-018-0109-2
99. Liu F-T, Goodarzi H, Chen H-Y. IgE, mast cells, and eosinophils in atopic dermatitis. Clin Rev Allergy Immunol (2011) 41(3):298–310. doi: 10.1007/s12016-011-8252-4
100. Chen LYC, Mattman A, Seidman MA, Carruthers MN. IgG4-related disease: what a hematologist needs to know. Haematologica (2019) 104(3):444–55. doi: 10.3324/haematol.2018.205526
101. Ehrens A, Hoerauf A, Hübner MP. Eosinophils in filarial infections: inducers of protection or pathology? Front Immunol (2022) 13:983812. doi: 10.3389/fimmu.2022.983812
102. Barry J, Gadre A, Akuthota P. Hypersensitivity pneumonitis, allergic bronchopulmonary aspergillosis and other eosinophilic lung diseases. Curr Opin Immunol (2020) 66:129–35. doi: 10.1016/j.coi.2020.10.005
103. Roberts LJ, Huffam SE, Walton SF, Currie BJ. Crusted scabies: clinical and immunological findings in seventy-eight patients and a review of the literature. J Infect (2005) 50(5):375–81. doi: 10.1016/j.jinf.2004.08.033
104. Khoury P, Herold J, Alpaugh A, Dinerman E, Holland-Thomas N, Stoddard J, et al. Episodic angioedema with eosinophilia (Gleich syndrome) is a multilineage cell cycling disorder. Haematologica (2015) 100(3):300–7. doi: 10.3324/haematol.2013.091264
105. Botan A, Borges TKDS, Alves EAR, Couto SCP, Seidler HBK, Muniz-Junqueira MI. Enhanced activation of eosinophils in peripheral blood and implications for eosinophilic esophagitis diagnosis. J Gastroenterol Hepatol (2017) 32(7):1318–27. doi: 10.1111/jgh.13710
106. Papo M, Diamond EL, Cohen-Aubart F, Emile J-F, Roos-Weil D, Gupta N, et al. High prevalence of myeloid neoplasms in adults with non-langerhans cell histiocytosis. Blood (2017) 130(8):1007–13. doi: 10.1182/blood-2017-01-761718
107. Tsuyama N, Noguchi M, Asaka R, Sakata S, Baba S, Izumi H, et al. Hodgkinoid histiocytosis: an atypical nodal CD30 and S100-positive histiocytosis with eosinophilia. Histopathology (2022) 81(3):371–9. doi: 10.1111/his.14718
108. Goyal G, Heaney ML, Collin M, Cohen-Aubart F, Vaglio A, Durham BH, et al. Erdheim-Chester disease: consensus recommendations for evaluation, diagnosis, and treatment in the molecular era. Blood (2020) 135(22):1929–45. doi: 10.1182/blood.2019003507
109. Goyal G, Tazi A, Go RS, Rech KL, Picarsic JL, Vassallo R, et al. International expert consensus recommendations for the diagnosis and treatment of langerhans cell histiocytosis in adults. Blood (2022) 139(17):2601–21. doi: 10.1182/blood.2021014343
110. Kemps PG, Picarsic J, Durham BH, Hélias-Rodzewicz Z, Hiemcke-Jiwa L, van den Bos C, et al. ALK-positive histiocytosis: a new clinicopathologic spectrum highlighting neurologic involvement and responses to ALK inhibition. Blood (2022) 139(2):256–80. doi: 10.1182/blood.2021013338
111. Zhang X, Hyjek E, Vardiman J. A subset of rosai-dorfman disease exhibits features of IgG4-related disease. Am J Clin Pathol (2013) 139(5):622–32. doi: 10.1309/AJCPARC3YQ0KLIOA
112. Kinoshita M, Ogawa Y, Onaka M, Shimada S, Kawamura T. Mepolizumab-responsive kimura disease. J Allergy Clin Immunol Pract (2021) 9(7):2928–30. doi: 10.1016/j.jaip.2021.02.049
113. Hu G, Wang S, Zhong K, Xu F, Huang L, Chen W, et al. Tumor-associated tissue eosinophilia predicts favorable clinical outcome in solid tumors: a meta-analysis. BMC Cancer (2020) 20(1):454. doi: 10.1186/s12885-020-06966-3
114. Davis BP, Rothenberg ME. Eosinophils and cancer. Cancer Immunol Res (2014) 2(1):1–8. doi: 10.1158/2326-6066.CIR-13-0196
115. Lam BD, Hale AJ, Bullis SM, He YT, Khan S, Freed JA, et al. A retrospective review of 193 cases of severe eosinophilia in the northeast united states. Am J Med (2021) 134(6):e374–7. doi: 10.1016/j.amjmed.2020.11.022
116. Tal Y, Shamriz O, Hershko A. The etiology of severe eosinophilia in hospitalized patients. J Allergy Clin Immunol (2020) 145(2):AB66. doi: 10.1016/j.jaci.2019.12.731
117. Yang X, Wang L, Du H, Lin B, Yi J, Wen X, et al. Prognostic impact of eosinophils in peripheral blood and tumor site in patients with esophageal squamous cell carcinoma treated with concurrent chemoradiotherapy. Med (Baltimore) (2021) 100(3):e24328. doi: 10.1097/MD.0000000000024328
118. Zalewska E, Obołonczyk L, Sworczak K. Hypereosinophilia in solid tumors{{/amp]]mdash; case report and clinical review. Front Oncol (2021) 11:639395. doi: 10.3389/fonc.2021.639395
119. Grisaru-Tal S, Itan M, Klion AD, Munitz A. A new dawn for eosinophils in the tumour microenvironment. Nat Rev Cancer (2020) 20(10):594–607. doi: 10.1038/s41568-020-0283-9
120. Wendlinger S, Wohlfarth J, Kreft S, Siedel C, Kilian T, Dischinger U, et al. Blood eosinophils are associated with efficacy of targeted therapy in patients with advanced melanoma. Cancers (Basel) (2022) 14(9):2294. doi: 10.3390/cancers14092294
121. Bernard-Tessier A, Jeanville P, Champiat S, Lazarovici J, Voisin A-L, Mateus C, et al. Immune-related eosinophilia induced by anti-programmed death 1 or death-ligand 1 antibodies. Eur J Cancer (2017) 81:135–7. doi: 10.1016/j.ejca.2017.05.017
122. Simona SCS, Hua X, Pantenc J, Grees M, Renders S, Thomas D, et al. Eosinophil accumulation predicts response to melanoma treatment with immune checkpoint inhibitors. Oncoimmunology (2020) 9(1):1727116. doi: 10.1080/2162402X.2020.1727116
123. Baroz AR, Mambetsariev I, Fricke J, Pharaon R, Tan TT, Kidambi T, et al. Elevated eosinophil count following pembrolizumab treatment for non-small cell lung cancer. Cureus (2021) 13(7):e16266. doi: 10.7759/cureus.16266
124. Scanvion Q, Bénéb J, Gautierb S, Grandvuilleminc A, Le Beller C, Chenaf C, et al. Moderate-to-severe eosinophilia induced by treatment with immune checkpoint inhibitors: 37 cases from a national reference center for hypereosinophilic syndromes and the French pharmacovigilance database. Oncoimmunology (2020) 9(1):1722022. doi: 10.1080/2162402X.2020.1722022
125. Cho Y-T, Yang C-W, Chu C-Y. Drug reaction with eosinophilia and systemic symptoms (DRESS): an interplay among drugs, viruses, and immune system. Int J Mol Sci (2017) 18(6):1243. doi: 10.3390/ijms18061243
126. Schunkert EM, Divito SJ. Updates and insights in the diagnosis and management of DRESS syndrome. Curr Dermatol Rep (2021) 10(4):192–204. doi: 10.1007/s13671-021-00348-z
127. Altman LC, Hill JS, Hairfield WM, Mullarkey MF. Effects of corticosteroids on eosinophil chemotaxis and adherence. J Clin Invest (1981) 67(1):28–36. doi: 10.1172/JCI110024
128. Wallen N, Kita H, Weiler D, Gleich GJ. Glucocorticoids inhibit cytokine-mediated eosinophil survival. J Immunol (1991) 147(10):3490–5. doi: 10.4049/jimmunol.147.10.3490
129. Hallsworth MP, Litchfield TM, Lee TH. Glucocorticoids inhibit granulocyte-macrophage colony-stimulating factor-1 and interleukin-5 enhanced in vitro survival of human eosinophils. Immunology (1992) 75(2):382–5.
130. Schleimer RP, Bochner BS. The effects of glucocorticoids on human eosinophils. J Allergy Clin Immunol (1994) 94(6 Pt 2):1202–13. doi: 10.1016/0091-6749(94)90333-6
131. Grayson PC, Monach PA, Pagnoux C, Cuthbertson D, Carette S, Hoffman GS, et al. Value of commonly measured laboratory tests as biomarkers of disease activity and predictors of relapse in eosinophilic granulomatosis with polyangiitis. Rheumatol (Oxford) (2015) 54(8):1351–9. doi: 10.1093/rheumatology/keu427
132. Pavord ID, Agusti A. Blood eosinophil count: a biomarker of an important treatable trait in patients with airway disease. Eur Respir J (.2016) 47(5):1299–303. doi: 10.1183/13993003.00055-2016
133. Pinto A, Aldinucci D, Gloghini A, Zagonel V, Degan M, Perin V, et al. The role of eosinophils in the pathobiology of hodgkin's disease. Ann Oncol (1997) 8(Suppl 2):89–96. doi: 10.1093/annonc/8.suppl_2.S89
134. Vardiman JW, Thiele J, Arber DA, Brunning RD, Borowitz MJ, Porwit A, et al. The 2008 revision of the world health organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes. Blood (2009) 114(5):937–51. doi: 10.1182/blood-2009-03-209262
135. Baer C, Muehlbacher V, Kern W, Haferlach C, Haferlach T. Molecular genetic characterization of myeloid/lymphoid neoplasms associated with eosinophilia and rearrangement of PDGFRA, PDGFRB, FGFR1 or PCM1-JAK2. Haematologica (2018) 103(8):e348–50. doi: 10.3324/haematol.2017.187302
136. Pozdnyakova O, Orazi A, Kelemen K, King R, Reichard KK, Craig FE, et al. Myeloid/lymphoid neoplasms associated with eosinophilia and rearrangements of PDGFRA, PDGFRB, or FGFR1 or with PCM1-JAK2. Am J Clin Pathol (2021) 155(2):160–78. doi: 10.1093/ajcp/aqaa208
137. Zhang Y, Lu C, Wang E, Nguyen L, Lauw M, Ball S, et al. MPN-521 somatic mutational landscape and clinical response to upfront targeted tyrosine kinase inhibitors among patients with myeloid and lymphoid neoplasms with eosinophilia and rearrangements of PDGFRA, PDGFRB, FGFR1, JAK2, or FLT3. Clin Lymphoma Myeloma Leuk (2022) Suppl 2:S341. doi: 10.1016/S2152-2650(22)01466-5
138. Gerds AT, Gotlib J, Bose P, Deininger MW, Dunbar A, Elshoury A, et al. Myeloid/lymphoid neoplasms with eosinophilia and TK fusion genes, version 3.2021. J Natl Compr Canc Netw (2020) 18(9):1248–69. doi: 10.6004/jnccn.2020.0042
139. Gotlib J, Cools J. Five years since the discovery of FIP1L1–PDGFRA: what we have learned about the fusion and other molecularly defined eosinophilias. Leukemia (2008) 22(11):1999–2010. doi: 10.1038/leu.2008.287
140. Wang SA, Hasserjian RP, Tam W, Tsai AG, Geyer JT, George TI, et al. Bone marrow morphology is a strong discriminator between chronic eosinophilic leukemia, not otherwise specified and reactive idiopathic hypereosinophilic syndrome. Haematologica (2017) 102:1352–60. doi: 10.3324/haematol.2017.165340
141. Wang SA, Tam W, Tsai AG, Arber DA, Hasserjian RP, Geyer JT, et al. Targeted next-generation sequencing identifies a subset of idiopathic hypereosinophilic syndrome with features similar to chronic eosinophilic leukemia, not otherwise specified. Mod Pathol (2016) 29(8):854–64. doi: 10.1038/modpathol.2016.75
142. Cross NCP, Hoade Y, Tapper WJ, Carreno-Tarragona G, Fanelli T, Jawhar M, et al. Recurrent activating STAT5B N642H mutation in myeloid neoplasms with eosinophilia. Leukemia (2019) 33(2):415–25. doi: 10.1038/s41375-018-0342-3
143. Singh A, Baron J, Singh N, Peringeth G, Wang ES. Eosinophilia characterized by a rare CCT6B mutation and responsive to tyrosine kinase inhibition: case report and literature review. Leuk Res Rep (2021) 16:100279. doi: 10.1016/j.lrr.2021.100279
144. Kelemen K, Saft L, Craig FE, Orazi A, Nakashima M, Wertheim GB, et al. Eosinophilia/hypereosinophilia in the setting of reactive and idiopathic causes, well-defined myeloid or lymphoid leukemias, or germline disorders. Am J Clin Pathol (2021) 155(2):179–210. doi: 10.1093/ajcp/aqaa244
145. Rothenberg ME, Klion AD, Roufosse FE, Kahn JE, Weller PF, Simon H-U, et al. Treatment of patients with the hypereosinophilic syndrome with mepolizumab. N Engl J Med (2008) 358(12):1215–28. doi: 10.1056/NEJMoa070812
146. Roufosse F, Kahn J-E, Rothenberg ME, Wardlaw AJ, Klion AD, Kirby SY, et al. Efficacy and safety of mepolizumab in hypereosinophilic syndrome: a phase III, randomized, placebo-controlled trial. J Allergy Clin Immunol (2020) 146(6):1397–405. doi: 10.1016/j.jaci.2020.08.037
147. Intermesoli T, Delaini F, Acerboni S, Salmoiraghi S, Spinelli O, Guerini V, et al. A short low-dose imatinib trial allows rapid identification of responsive patients in hypereosinophilic syndromes. Br J Haematol (2009) 147(5):681–5. doi: 10.1111/j.1365-2141.2009.07893.x
148. Donald CE, Kahn MJ. Successful treatment of hypereosinophilic syndrome with cyclosporine. Am J Med Sci (2009) 337(1):65–6. doi: 10.1097/MAJ.0b013e318169569a
149. Bjerrum OW. Interferon treatment in patients with hypereosinophilia. Curr Drug Targets (2011) 12(3):429–32. doi: 10.2174/138945011794815211
150. Tabata R, Tabata C, Katashima Y, Yasumizu R. Effect of cyclosporine on lymphocytic variant hypereosinophilic syndrome. Int Immunopharmacol (2013) 16(4):488–91. doi: 10.1016/j.intimp.2013.04.033
151. Requena G, van den Bosch J, Akuthota P, Kovalszki A, Steinfeld J, Kwon N, et al. Clinical profile and treatment in hypereosinophilic syndrome variants: a pragmatic review. J Allergy Clin Immunol: In Pract (2022) 10(8):2125–34. doi: 10.1016/j.jaip.2022.03.034
152. Helbig G. Imatinib for the treatment of hypereosinophilic syndromes. Expert Rev Clin Immunol (2018) 14(2):163–70. doi: 10.1080/1744666X.2018.1425142
153. Doroudchi A, Pathria M, Modena BD. Asthma biologics: comparing trial designs, patient cohorts and study results. Ann Allergy Asthma Immunol (2020) 124(1):44–56. doi: 10.1016/j.anai.2019.10.016
154. Choudhury S, Baker S. Eosinophilic esophagitis: the potential role of biologics in its treatment. Clin Rev Allergy Immunol (2020) 59(2):150–9. doi: 10.1007/s12016-019-08749-6
155. Katsuno M. A review of anti-IL-5 therapies for eosinophilic granulomatosis with polyangiitis. Adv Ther (2023) 40(1):25–40. doi: 10.1007/s12325-022-02307-x
156. Gribben J, Macintyre E, Sonneveld P, Doorduijn J, Gisselbrecht C, Jäger U, et al. Reducing bureaucracy in clinical research: a call for action. Hemasphere (2020) 4(2):e352. doi: 10.1097/HS9.0000000000000352
157. Dworetzky SI, Hebrank GT, Archibald DG, Reynolds IJ, Farwell W, Bozik ME. The targeted eosinophil-lowering effects of dexpramipexole in clinical studies. Blood Cells Mol Dis (2017) 63:62–5. doi: 10.1016/j.bcmd.2017.01.008
158. Panch SR, Bozik ME, Brown T, Makiya M, Prussin C, Archibald DG, et al. Dexpramipexole as an oral steroid-sparing agent in hypereosinophilic syndromes. Blood (2018) 132(5):501–9. doi: 10.1182/blood-2018-02-835330
159. Goswami P, Oliva EN, Ionova T, Else R, Kell J, Fielding AK, et al. Hematological malignancy specific patient-reported outcome measure (HM-PRO): construct validity study. Front Pharmacol (2020) 11:1308. doi: 10.3389/fphar.2020.01308
160. Emanuel RM, Dueck AC, Geyer HL, Kiladjian J-J, Slot S, Zweegman S, et al. Myeloproliferative neoplasm (MPN) symptom assessment form total symptom score: prospective international assessment of an abbreviated symptom burden scoring system among patients with MPNs. J Clin Oncol (2012) 30(33):4098–103. doi: 10.1200/JCO.2012.42.3863
161. Gwaltney C, Paty J, Kwitkowski VE, Mesa RA, Dueck AC, Papadopoulos EI, et al. Development of a harmonized patient-reported outcome questionnaire to assess myelofibrosis symptoms in clinical trials. Leuk Res (2017) 59:26–31. doi: 10.1016/j.leukres.2017.05.012
162. Langlais BT, Geyer H, Scherber R, Mesa RA, Dueck AC. Quality of life and symptom burden among myeloproliferative neoplasm patients: do symptoms impact quality of life? Leuk Lymphoma (2019) 60(2):402–8. doi: 10.1080/10428194.2018.1480768
163. Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European organization for research and treatment of cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst (1993) 85(5):365–76. doi: 10.1093/jnci/85.5.365
164. Fayers P, Bottomley A, EORTC Quality of Life Group, Quality of Life Unit. Quality of life research within the EORTC-the EORTC QLQ-C30. European organisation for research and treatment of cancer. Eur J Cancer (2002) 38(Suppl 4):S125–33. doi: 10.1016/s0959-8049(01)00448-8
165. Feng Y-S, Kohlmann T, Janssen MF, Buchholz I. Psychometric properties of the EQ-5D-5L: a systematic review of the literature. Qual Life Res (2021) 30(3):647–73. doi: 10.1007/s11136-020-02688-y
166. Garcia SF, Cella D, Clauser SB, Flynn KE, Lad T, Lai J-S, et al. Standardizing patient-reported outcomes assessment in cancer clinical trials: a patient-reported outcomes measurement information system initiative. J Clin Oncol (2007) 25(32):5106–12. doi: 10.1200/JCO.2007.12.2341
167. Basch E, Abernethy AP, Mullins CD, Reeve BB, Smith ML, Coons SJ. Recommendations for incorporating patient-reported outcomes into clinical comparative effectiveness research in adult oncology. J Clin Oncol (2012) 30(34):4249–55. doi: 10.1200/JCO.2012.42.5967
168. Kamper SJ, Maher CG, Mackay G. Global rating of change scales: a review of strengths and weaknesses and considerations for design. J Man Manip Ther (2009) 17(3):163–70. doi: 10.1179/jmt.2009.17.3.163
169. Busner J, Targum SD. The clinical global impressions scale: applying a research tool in clinical practice. Psychiatry (Edgmont) (2007) 4(7):28–37.
170. Chessa E, Piga M, Floris A, Devilliers H, Cauli A, Arnaud L. Use of physician global assessment in systemic lupus erythematosus: a systematic review of its psychometric properties. Rheumatology (2020) 59(12):3622–32. doi: 10.1093/rheumatology/keaa383
171. Brochmann N, Zwisler A-D, Kjerholt M, Flachs EM, Hasselbalch HC, Andersen CL. A new internet-based tool for reporting and analysing patient-reported outcomes and the feasibility of repeated data collection from patients with myeloproliferative neoplasms. Qual Life Res (2016) 25(4):835–46. doi: 10.1007/s11136-015-1125-1
172. Epstein NE. Multidisciplinary in−hospital teams improve patient outcomes: a review. Surg Neurol Int (2014) 5(Suppl 7):S295–303. doi: 10.4103/2152-7806.139612
173. Tyler KH, Haverkos BM, Hastings J, Hu E, Philips R, Gru AA, et al. The role of an integrated multidisciplinary clinic in the management of patients with cutaneous lymphoma. Front Oncol (2015) 5:136. doi: 10.3389/fonc.2015.00136
174. Burke H, Davis J, Evans S, Flower L, Tan A, Kurukulaaratchy RJ. A multidisciplinary team case management approach reduces the burden of frequent asthma admissions. ERJ Open Res (2016) 2(3):00039–2016. doi: 10.1183/23120541.00039-2016
175. Taberna M, Moncayo FG, Jané-Salas E, Antonio M, Arribas L, Vilajosana E, et al. The multidisciplinary team (MDT) approach and quality of care. Front Oncol (2020) 10:85. doi: 10.3389/fonc.2020.00085
176. Fehervari M, Hamrang-Yousefi S, Fadel MG, Mills SC, Warren OJ, Tekkis PP. A systematic review of colorectal multidisciplinary team meetings: an international comparison. BJS Open (2021) 5(3):zrab044. doi: 10.1093/bjsopen/zrab044
177. Gonzales AA, Mastrolonardo A, Winget K, Ragulojan M, Fleming AJ, Singh SK. The role of a longitudinal, multidisciplinary clinic in building a unique research collaborative. Front Oncol (2022) 12:857699. doi: 10.3389/fonc.2022.857699
178. Bjerrum OW, El Fassi D, Madsen G, Stentoft J, Vestergaard H, Rønnov-Jessen D, et al. Eosinophilia. Ugeskr Laeger (2018) 180(37):V01180032.
179. Hurst W, Withington A, Kolivand H. Virtual conference design: features and obstacles. Multimed Tools Appl (2022) 81(12):16901–19. doi: 10.1007/s11042-022-12402-4
180. Hunter H, Pupinyte K, Wong T, Zeki S, Dunn JM, Toner E, et al. Multidisciplinary approach to the management of adult eosinophilic oesophagitis in the united kingdom. Clin Exp Allergy (2018) 48(12):1752–6. doi: 10.1111/cea.13279
181. McMurray JC, St Clair B, Spriet SW, Min SB, Brooks DI, Mikita CP. Outcomes of eosinophilic esophagitis in patients managed in a multidisciplinary clinic. Allergy Asthma Proc (2022) 43(1):78–84. doi: 10.2500/aap.2022.43.210102
182. Zhao Y, Jiang P, Chen X, Yao G. Case report: different clinical manifestations of the rare loeffler endocarditis. Front Cardiovasc Med (2022) 9:970446. doi: 10.3389/fcvm.2022.970446
183. Egholm GJ, Andersen MA, Andersen CL, Frederiksen H, Bjerrum OW, Niemann CU. Abnormal eosinophil count at CLL diagnosis correlates with shorter treatment free survival. Br J Haematol (2021) 192(3):e81–4. doi: 10.1111/bjh.17264
184. Jacobsen EA, Helmers RA, Lee JJ, Lee NA. The expanding role(s) of eosinophils in health and disease. Blood (2012) 120(19):3882–90. doi: 10.1182/blood-2012-06-330845
185. Gleich GJ, Klion AD, Lee JJ, Weller PF. The consequences of not having eosinophils. Allergy (2013) 68(7):829–35. doi: 10.1111/all.12169
186. Klion AD, Ackerman SJ, Bochner BS. Contributions of eosinophils to human health and disease. Annu Rev Pathol (2020) 15:179–209. doi: 10.1146/annurev-pathmechdis-012419-032756
187. Jacobsen EA, Jackson DJ, Heffler E, Mathur SK, Bredenoord AJ, Pavord ID, et al. Eosinophil knockout humans: uncovering the role of eosinophils through eosinophil-directed biological therapies. Annu Rev Immunol (2021) 39:719–57. doi: 10.1146/annurev-immunol-093019-125918
188. Sugiyama E, Takenaka T, Kato M, Minoshima A, Muto H, Fujita M, et al. Eosinophilic myocarditis without hypereosinophilia accompanied by giant cell infiltration. J Cardiol cases (2015) 12(5):169–71. doi: 10.1016/j.jccase.2015.07.004
189. Rodrigo-Muñoz JM, Gil-Martínez M, Sastre B, del Pozo V. Emerging evidence for pleiotropism of eosinophils. Int J Mol Sci (2021) 22(13):7075. doi: 10.3390/ijms22137075
190. Salmanoglu E, Kim S, Thakur ML. Currently available radiopharmaceuticals for imaging infection and the holy grail. Semin Nucl Med (2018) 48(2):86–99. doi: 10.1053/j.semnuclmed.2017.10.003
191. Roufosse F. Targeting the interleukin-5 pathway for treatment of eosinophilic conditions other than asthma. Front Med (Lausanne) (2018) 5:49. doi: 10.3389/fmed.2018.00049
192. Youngblood BA, Leung J, Falahati R, Williams J, Schanin J, Brock EC, et al. Discovery, function, and therapeutic targeting of siglec-8. Cells (2020) 10(1):19. doi: 10.3390/cells10010019
193. Chandrasekharan P, Barry Fung KL, Zhou XY, Cui W, Colson C, Mai D, et al. Non-radioactive and sensitive tracking of neutrophils towards inflammation using antibody functionalized magnetic particle imaging tracers. Nanotheranostics (2021) 5(2):240–55. doi: 10.7150/ntno.50721
194. Flaum MA, Schooley RT, Fauci AS, Gralnick HR. A clinicopathologic correlation of the idiopathic hypereosinophilic syndrome. i. hematologic manifestations. Blood (1981) 58(5):1012–20.
195. Schooley RT, Flaum MA, Gralnick HR, Fauci AS. A clinicopathologic correlation of the idiopathic hypereosinophilic syndrome. II. clinical manifestations. Blood (1981) 58(5):1021–6.
196. Rios-Navarro C, Gavara J, Vidal V, Bonanad C, Racugno P, Bayes-Genis A, et al. Characterization and implications of the dynamics of eosinophils in blood and in the infarcted myocardium after coronary reperfusion. PloS One (2018) 13(10):e0206344. doi: 10.1371/journal.pone.0206344
197. Bjerrum OW, Siersma V, Hasselbalch HC, Lind B, Andersen CL. Association of the blood eosinophil count with end-organ symptoms. Ann Med Surg (Lond) (2019) 45:11–8. doi: 10.1016/j.amsu.2019.06.015
198. Baisse A, Lafon T, Caumes S, Dumonteil S, Fauchais A-L, Parreau S. Acute hypereosinophilia in emergency department: variables associated with a 3−month mortality. Intern Emerg Med (2022) 17(1):279–83. doi: 10.1007/s11739-021-02808-7
199. Rai S, Espinoza JL, Morita Y, Tanaka H, Matsumura I. Severe eosinophilia in myelodysplastic syndrome with a defined and rare cytogenetic abnormality. Front Immunol (2018) 9:3031. doi: 10.3389/fimmu.2018.03031
200. Berti A, Atzeni F, Dagna L, Del Giacco S, Emmi G, Salvarani C, et al. Targeting the interleukin-5 pathway in EGPA: evidence, uncertainties and opportunities. Ann Rheum Dis (2023) 82(2):164–8. doi: 10.1136/ard-2022-223044
201. Kuang FL, Legrand F, Makiya M, Ware JA, Wetzler L, Magee T, et al. Benralizumab for PDGFRA-negative hypereosinophilic syndrome. N Engl J Med (2019) 380:1336–46. doi: 10.1056/NEJMoa1812185
202. Dispenza MC, Bochner BS. Diagnosis and novel approaches to the treatment of hypereosinophilic syndromes. Curr Hematol Malig Rep (2018) 13(3):191–201. doi: 10.1007/s11899-018-0448-8
203. Stella S, Massimino M, Manzella L, Pennisi MS, Tirrò E, Romano C, et al. Molecular pathogenesis and treatment perspectives for hypereosinophilia and hypereosinophilic syndromes. Int J Mol Sci (2021) 22(2):486. doi: 10.3390/ijms22020486
204. Kiwamotoa T, Kawasakib N, Paulson JC, Bochner BS. Siglec-8 as a drugable target to treat eosinophil and mast cell associated conditions. Pharmacol Ther (2012) 135(3):327–36. doi: 10.1016/j.pharmthera.2012.06.005
205. Legrand F, Cao Y, Wechsler J, Zhu X, Zimmermann N, Rampertaap S, et al. Siglec-8 in eosinophilic disorders: receptor expression and targeting using chimeric antibodies. J Allergy Clin Immunol (2019) 143(6):2227–37.e10. doi: 10.1016/j.jaci.2018.10.066
Keywords: clinical, diagnosis, eosinophilia, multidisciplinary, review, trial, treatment
Citation: Thomsen GN, Christoffersen MN, Lindegaard HM, Davidsen JR, Hartmeyer GN, Assing K, Mortz CG, Martin-Iguacel R, Møller MB, Kjeldsen AD, Havelund T, El Fassi D, Broesby-Olsen S, Maiborg M, Johansson SL, Andersen CL, Vestergaard H and Bjerrum OW (2023) The multidisciplinary approach to eosinophilia. Front. Oncol. 13:1193730. doi: 10.3389/fonc.2023.1193730
Received: 25 March 2023; Accepted: 25 April 2023;
Published: 18 May 2023.
Edited by:
Giuseppe Gaetano Loscocco, University of Florence, ItalyReviewed by:
Federica Bello, University of Florence, ItalyFrancesco Mannelli, Careggi University Hospital, Italy
Copyright © 2023 Thomsen, Christoffersen, Lindegaard, Davidsen, Hartmeyer, Assing, Mortz, Martin-Iguacel, Møller, Kjeldsen, Havelund, El Fassi, Broesby-Olsen, Maiborg, Johansson, Andersen, Vestergaard and Bjerrum. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ole Weis Bjerrum, ole.weis.bjerrum@rsyd.dk
†These authors have contributed equally to this work and share first authorship