
More Information
Submitted: March 24, 2021 | Approved: April 06, 2021 | Published: April 07, 2021
How to cite this article: Brochier A, Cabo J, Guerrieri C, Belkhir L, Laterre PF, Deneys V. Autoimmune hemolytic anemia in COVID-19 patients, the « transmissible » direct Coombs test. J Hematol Clin Res. 2021; 5: 004-008.
DOI: 10.29328/journal.jhcr.1001016
Copyright License: © 2021 Brochier A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Direct antiglobulin test; Erythrocyte cryptic antigens; COVID-19
Abbreviations: AIHA: Autoimmune Hemolytic Anemia; ANK-1: Ankyrin 1; COVID-19: Coronavirus Disease 2019; DAT: Direct Antiglobulin Test; IAS: Irregular Antibody Screening; IAT: Indirect Antiglobulin Test; ICU: Intensive Care Unit; NT: Not Tested; RBCS: Red Blood Cells; SARS-Cov-2: Severe Acute Respiratory Syndrome Coronavirus 2

Autoimmune hemolytic anemia in COVID-19 patients, the « transmissible » direct Coombs test
Alice Brochier1*, Julien Cabo1, Claudine Guerrieri1, Leïla Belkhir2, Pierre-François Laterre3 and Véronique Deneys1*
1Hematology Department of Laboratory Medicine, Saint-Luc University Hospital, Brussels, Belgium
2Department of Internal Medicine and Infectious Diseases, Saint-Luc University Hospital, Brussels, Belgium
3Department of Intensive Care Medicine, Saint-Luc University Hospital, Brussels, Belgium
*Address for Correspondence: Alice Brochier, Hematology Department of Laboratory Medicine, Saint-Luc University Hospital, Avenue Hippocrate 10, 1200 Brussels, Belgium, Tel: +322764 6814; Email: alice.brochier@uclouvain.be
Véronique Deneys, Hematology Department of Laboratory Medicine, Saint-Luc University Hospital, Avenue Hippocrate 10, 1200 Brussels, Belgium, Email: veronique.deneys@uclouvain.be
Background: Like other viruses, the SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) appears to be responsible for several autoimmune complications. The occurrence of autoimmune hemolytic anemia has been described in several case reports. This AIHA was also noticeable by the important number of blood transfusions required for COVID-19 (coronavirus disease 2019) patients. By investigating RBC coating autoantibodies, this article attempts to clarify the autoimmune aspect of the anemia in the context of SARS-CoV-2 infection.
Results: A large population of COVID-19 patients selected at Saint-Luc University Hospital showed an average of 44% DAT positivity. In this population, the intensive care patients were more prone to DAT positivity than the general ward patients (statistically significant result). The positive DAT appeared « transmissible » to other RBCs via COVID-19 DAT-positive patient’s plasma.
Conclusion: The strongest hypothesis explaining this observation is the targeting of cryptic antigens by autoantibodies in COVID-19 patients.
The Direct Antiglobulin Test (DAT) or direct Coombs test is commonly used to detect the presence of antibodies or complement fractions on the red blood cells (RBCs) surface. It is performed to diagnose autoimmune hemolytic anemia (AIHA) [1,2].
The type of antiserum used allows to determine which antibody isotype coats the erythrocytes. The most commonly used antisera are directed against IgG antibodies or complement fragments (usually C3d). In a routine laboratory, 3 types of DAT results can be distinguished: IgG-specific DAT, associated with warm AIHA; C3d-specific DAT, associated with cold agglutinin syndrome/disease; and mixed DAT, mostly due to the fact that IgG1 and IgG3 also bind complement fragments. A mixed DAT can also be caused by a mixed autoimmune hemolytic anemia, with cold and warm autoantibodies [3,4].
A positive DAT reveals the presence of antibodies on the cell surface. The anti-RBC antibodies can be autoantibodies or can originate from drug intake, feto-maternal incompatibility, transfusion or transplantation [3,4]. These last causes need to be excluded in case of AIHA suspicion. AIHA can be of unknown etiology or secondary to infection (several bacteria and viruses, notably CMV or EBV), neoplasia or immune dysregulation, like autoimmune disorders or immune deficiencies [4,5].
A positive DAT, regardless of the presence of a clinical hemolysis, reduces the lifespan of circulating erythrocytes. Coated RBCs are captured and cleared from circulation by macrophages of the mononuclear phagocytic system [3].
The recent SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) pandemic has been the subject of numerous publications and case reports. A growing number of complications have been associated with the virus, notably the occurrence of AIHA, as well as other autoimmune disorders. A study has shown a correlation between the hemoglobin level at hospital admission and the severity of the coronavirus disease 2019 (COVID-19) [6]. This highlights the clinical importance of finding the cause and correctly treating the anemia occurring in these patients.
Our study aims to clarify the autoimmune aspect of the anemia observed and to suggest potential mechanisms underlying this autoimmune phenomenon.
Sample population
EDTA blood samples were collected from 225 patients hospitalized in the COVID-19 units at the Saint-Luc University Hospital (Brussels) on three distinct days.
Eight samples were selected from COVID-19 positive patients showing a DAT with ≥ 2+ agglutination intensity with an IgG component. The patients showed no positive reaction for an irregular antibody screening (IAS) at the time. Five samples were obtained from ICU (intensive care unit) patients and three from the general ward.
Three RBC types were used for elution testing: RBCs from a commercial panel, and DAT-negative RBCs from patients that either tested positive or negative for SARS-CoV-2 by PCR.
Alloadsorptions were performed using six RBC types: cord blood, RBCs from pooled blood units and RBCs from patients that tested either positive or negative for SARS-CoV-2 by PCR. These last RBCs were kept either overnight (= fresh RBCs) or for seven days (= older RBCs) at 4 °C. All these erythrocytes were DAT negative.
The design of the study is illustrated in figure 1.
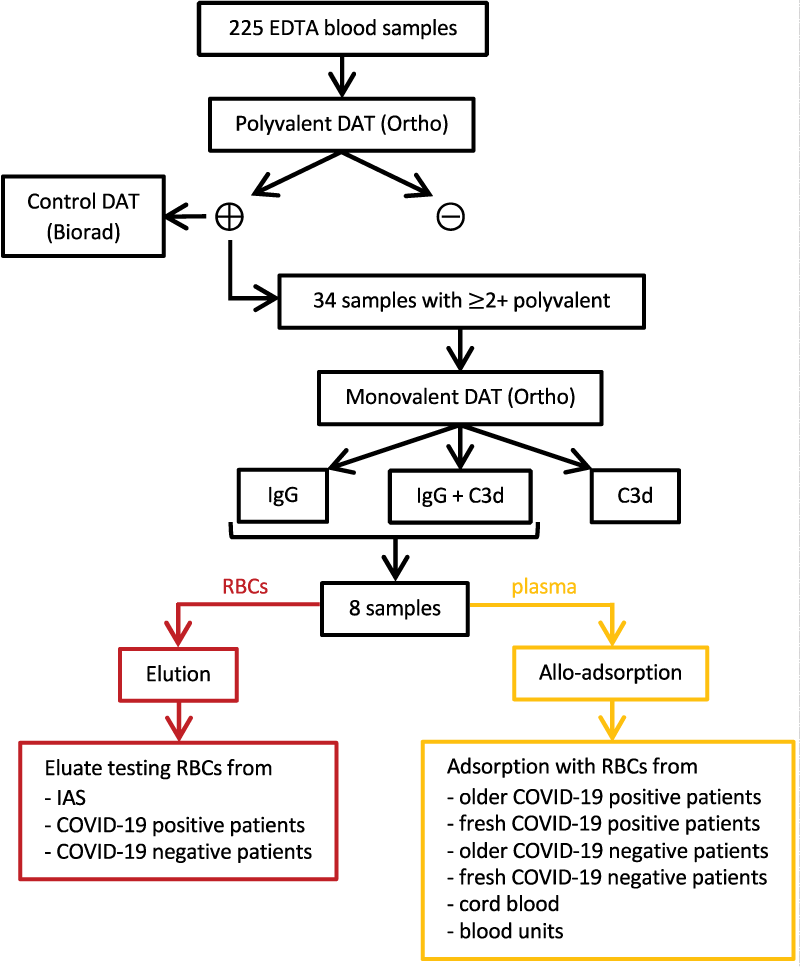
Figure 1: Design of the study.
Direct antiglobulin test
Each centrifuged EDTA sample was first tested using Ortho’s anti-IgG, -C3d; polyspecific gels on an OrthoVision automate (Ortho Clinical Diagnostics, Raritan, USA). The results obtained were visually confirmed. The agglutination force was semi-quantified from 0+ (no agglutination) to 4+ (complete agglutination). The positive samples were manually checked using LISS/Coombs ID-cards (Biorad, Hercules, USA). The results were visually assessed.
Samples showing at least a 2+ agglutination were tested for DAT-specificity using Ortho’s anti-IgG/anti-C3b, -C3d/control gels, allowing the determination of IgG-, C3- or a mixed specificity.
Elution
Elutions were performed with an acid-elution process (DiaCidel kit, Biorad). Each sample was centrifuged, and the plasma separated from the erythrocyte pellet. The erythrocytes were then washed once with saline and four times with the DiaCidel washing solution. The tubes were centrifuged at 2576 g for 6 minutes and the supernatant was removed. The last washing supernatant was considered as control of the efficiency of the washing procedure and tested for IAS (Ortho’s 0.8% Surgiscreen cells). Then, an elution solution containing an acidic glycin buffer was added to the RBCs in a 1:1 ratio. Every sample was homogenized and quickly centrifuged for 1 minute at 1449 g. The eluate was collected and neutralized by a buffer solution (pH of 6.5-7). The tube was centrifuged again for 1 minute at 1449 g to precipitate residual RBCs. The eluate was then used for indirect antiglobulin tests using the previously mentioned erythrocytes.
Alloadsorption
The RBCs used for alloadsorptions were washed five times with saline before use. They were then incubated in a 1:1 ratio with the plasmas collected from the eight COVID-19 patients or with control plasmas. These control plasmas were obtained from DAT-negative patients tested negative for SARS-CoV-2. Each plasma used had been tested negative for IAS and was ABO-compatible with the RBCs used. After at least two hours of incubation at 37°C, the samples were centrifuged at 2576 g for 6 minutes. The RBCs collected were tested for a DAT (Ortho’s anti-IgG, -C3d; polyspecific gels). The results were visually assessed.
Statistics
Figures were generated using GraphPad Prism 5.0 and Microsoft Excel 16.45. Statistics were calculated by Pearson’s χ2 test for DAT frequency comparison and by a one-way ANOVA with a Bonferroni test for mean comparison.
Direct antiglobulin test
Among the 225 samples, 99 were DAT-positive (44 from general ward patients and 55 from ICU patients) with an average positivity rate of 44%. DAT positivity ranged from 35% in the general ward to 56% in intensive care units. This was statistically significant (Pearson’s χ2 test, p < 0.01) (Figure 2A). Among all the DAT-positive samples obtained with Ortho, 67% also tested positive with the other method (Biorad).
The isotype was determined for samples showing a strong DAT positivity (≥ 2+). The majority (91.2%) showed an IgG-specificity alone (n = 20; 58.8%) or mixed (n = 11; 32.4%). The remaining RBC samples (n = 3; 8.8%) only showed C3d-specificity (Figure 2B).
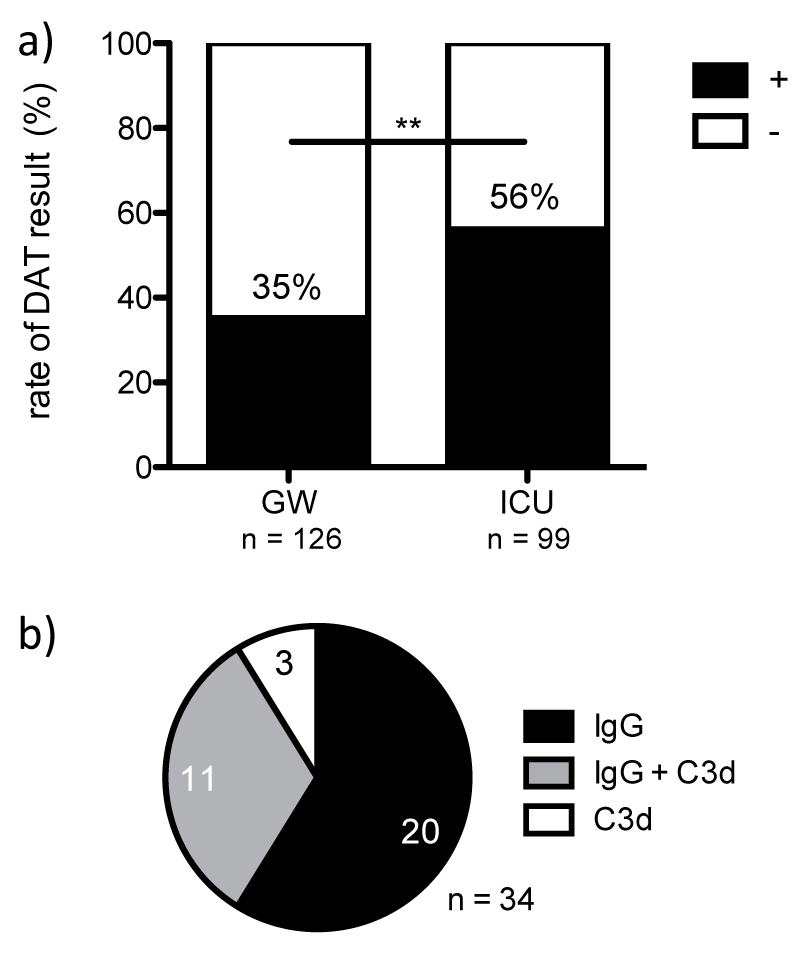
Figure 2: The amount of positive IgG-type DAT results in COVID-19 patients is high, particularly in the ICU. a) rate of DAT positivity according to type of hospitalization unit; b) rate of DAT positivity according to DAT specificity GW: General Ward; ICU: Intensive Care Unit; **p < 0.01.
Elution
The elution experiment generated negative results with all the RBC types used and when tested against an RBC commercial panel.
Alloadsorption
When incubated with COVID-19 positive patients’ plasma, all RBCs tested showed a positive DAT. The RBCs from sick patients showed a stronger agglutination than the RBCs from healthy people (Figure 3). This difference was statistically significant between the older COVID-19 positive RBCs and the RBCs from healthy people (cord blood, blood units). When incubated with the COVID-19 negative patients’ plasmas (control plasmas), only the sick patients’ RBCs showed agglutination. RBCs kept overnight reacted identically with the different plasmas regardless of the COVID-19 state of the patient. The difference became statistically significant with the older COVID-19 positive or negative patients’ RBCs. The older COVID-19 patients’ RBCs also reacted more strongly than the fresh ones.
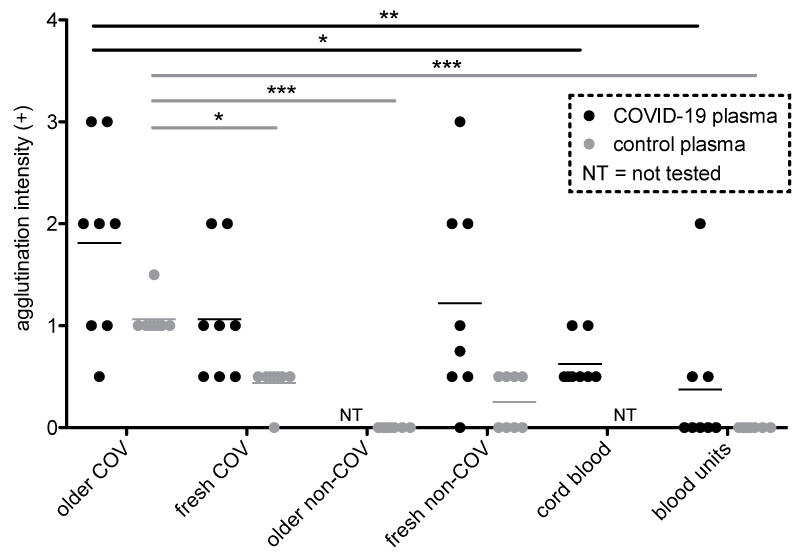
Figure 3: A positive direct Coombs test could be induced on six types of RBCs by incubation with COVID-19 patients’ plasmas. In black, the direct Coombs test on RBCs after incubation with the COVID-19 patients’ plasmas; in grey, the direct Coombs test on RBCs after incubation with the control plasmas. The relevant statistically significant differences are shown. NT: Not Tested; *p < 0.05; **p < 0.01; ***p < 0.001.
The direct antiglobulin test is frequently performed in a hospital blood transfusion service in order to diagnose immune-mediated hemolysis. The positivity rate of such tests is usually low, estimated to 0,008 up to 0,1% in a healthy blood donor population [7] and to 1-15% in patients suffering from acute illness [8-10]. Several case reports describe the onset of AIHA in patients suffering from COVID-19, associated with a positive DAT [11-15]. Moreover, other types of autoimmune complications are reported in SARS-CoV-2 infected patients, such as immune thrombocytopenic purpura [14,16], or Evans syndrome [17]. Bastard, et al. also report the presence of anti-interferon antibodies in some severe COVID-19 cases [18]. Consequently, the rate of DAT positivity has been investigated in the Saint-Luc University Hospital. 225 blood samples have been collected from patients hospitalized in COVID-19 units. The results obtained were striking, with a 44% positivity rate obtained by the Ortho gel method. 67% was confirmed positive by the more specific Biorad gel method. In fact, the Ortho method is well-known to be very sensitive [19].
The samples collected in the ICU showed a significantly higher positivity rate than those of the general ward. Accordingly, patients developing a positive DAT might be more at risk for admission in the ICU. This finding can be linked to the study showing that a lower hemoglobin level at admission is associated with a more severe disease evolution [6].
The majority of the DAT-positive samples tested showed an IgG-specificity, which was surprising, as viruses are usually known to stimulate a temporary cold agglutinin response, leading to a complement-specific DAT [20].
The positive direct Coombs test couldn’t be linked with a high degree of certainty to the SARS-CoV-2 infection in our patients. However, the clearly superior rate of positivity in this population (44%) compared to the one found in a non-COVID hospitalized population (up to 15%) [8,9] and the timeframe of the DAT becoming positive were highly suggestive.
A similar DAT rate was published by Berzuini, et al., who described 46% positivity. The RBC elutions performed by their team induced agglutination with RBCs from COVID-19 patients [21]. These results couldn’t be reproduced in our experiences. The discrepancy might be explained by the acid elution method, since a different elution kit was used.
To evaluate the target of the antibodies causing the DAT positivity, alloadsorptions were performed. Surprisingly, the antibodies in COVID-19 patient’s plasmas coated all the RBC types tested. Moreover, they affected RBCs from sick patients more than those from healthy people.
The strongest hypothesis for this phenomenon relies on the inflammatory context caused by sickness. A cytokine-rich inflammatory environment alters the antigen presentation process by the antigen presenting cells. This results in a modified antigen repertoire presented to T lymphocytes, of which cryptic antigens may be a part. These antigens don’t elicit T lymphocytes negative selection in the thymus. If they are more presented on the cell surface, they are more likely to elicit an immune response when encountering an autoreactive T lymphocyte. The stimulated T lymphocytes activate in turn autoreactive B lymphocytes to produce antibodies against the cryptic antigens [22-25]. This hypothesis is supported by the fact that RBCs from COVID-19 patients react with the control plasmas. We indeed all have immune reactivity against cryptic antigens. Repetitive exposure is a key factor for the occurrence of autoimmunity [22,25]. Viral infection has already been correlated with the exposure of cryptic antigens [24] and with hemolytic anemia [25-27]. Moreover, some viruses are known to act as B lymphocytes stimulators, and can therefore activate anergized autoreactive B cells [25]. This hypothesis doesn’t exclude the possibility that the antigen targeted might not be fully expressed on neonate RBCs. The anticoagulant might be another confounding factor, since blood units contain citrate instead of EDTA.
A second hypothesis is based on the existence of a shared epitope sequence between the SARS-CoV-2 spike protein and the ankyrin 1 (ANK-1) protein present on the RBC membrane [28]. Molecular mimicry is a well-known initiating event of autoimmune diseases [22,25]. Even if this similarity likely plays a role in the autoimmune phenomenon, it is probably not sufficient as isolated hypothesis. The cord blood RBCs express ANK-1 [29]. However, when added to COVID-19 patients’ plasmas, they react less intensively than the sick patients’ RBCs. This difference isn’t explained by the molecular mimicry hypothesis.
RBC transfusion is a known cause of alloantibody trigger. This can be observed by a positive DAT at first. The patients’ transfusion history hasn’t been reviewed for this article. However, the samples coming from the selected eight COVID-19 patients have been analyzed further. Their positive direct Coombs test observed couldn’t have been caused by an alloantibody. Both their plasma and eluate were tested negative by IAS. Had there been an alloantibody, the alloadsorption results would probably have shown greater variation depending on the presence of the targeted antigen.
A positive DAT with a negative elution can also be caused by drug-induced antibodies. Since the patients’ medication history has not been reviewed for the article, this hypothesis can’t be excluded.
Hospitalized COVID-19 patients show a direct Coombs test rate of 44%. The ICU patients were more prone to DAT positivity than general ward patients. The DAT can be “transmitted” to allogenous RBCs that have been in contact with the plasma of DAT-positive COVID-19 patients. A potential hypothesis would be that the antibodies coating the RBCs, causing the DAT, target cryptic antigens. Evidence supporting this hypothesis are the important inflammatory state caused by the COVID-19, the polyclonal stimulation of B lymphocytes by viral vector and the epitope shared between SARS-CoV-2 Spike protein and ANK-1 on the RBCs.
The authors would like to thank the Saint-Luc Hospital blood transfusion service staff for their experience and support.
Authorship contribution
A.B., C.G. and V.D. designed the research, A.B. and C.G. performed laboratory experiments, A.B., C.G. and V.D. analyzed the data, A.B. and J.C. made the figures, all authors contributed to writing the paper.
- Coombs RR, Mourant AE, Race RR. A new test for the detection of weak and incomplete Rh agglutinins. Br J Exp Pathol. 1945; 26: 255-266. PubMed: https://pubmed.ncbi.nlm.nih.gov/21006651/
- Zantek ND, Koepsell SA, Tharp DR, Jr., Cohn CS. The direct antiglobulin test: a critical step in the evaluation of hemolysis. Am J Hematol. 2012; 87: 707-709. PubMed: https://pubmed.ncbi.nlm.nih.gov/22566278/
- Jäger U, Barcellini W, Broome CM, Gertz MA, Hill A, et al. Diagnosis and treatment of autoimmune hemolytic anemia in adults: Recommendations from the First International Consensus Meeting. Blood Rev. 2020; 41: 100648. PubMed: https://pubmed.ncbi.nlm.nih.gov/31839434/
- Hill QA, Stamps R, Massey E, Grainger JD, Provan D, et al. The diagnosis and management of primary autoimmune haemolytic anaemia. Br J Haematol. 2017; 176: 395-411. PubMed: https://pubmed.ncbi.nlm.nih.gov/28005293/
- Michalak SS, Olewicz-Gawlik A, Rupa-Matysek J, Wolny-Rokicka E, Nowakowska E, et al. Autoimmune hemolytic anemia: current knowledge and perspectives. Immun Ageing. 2020; 17: 38. PubMed: https://pubmed.ncbi.nlm.nih.gov/33292368/
- Algassim AA, Elghazaly AA, Alnahdi AS, Mohammed-Rahim OM, Alanazi AG, et al. Prognostic significance of hemoglobin level and autoimmune hemolytic anemia in SARS-CoV-2 infection. Ann Hematol. 2021; 100: 37-43. PubMed: https://pubmed.ncbi.nlm.nih.gov/32918594/
- Hannon JL. Management of blood donors and blood donations from individuals found to have a positive direct antiglobulin test. Transfus Med Rev. 2012; 26: 142-152. PubMed: https://pubmed.ncbi.nlm.nih.gov/22000666/
- Parker V, Tormey CA. The Direct Antiglobulin Test: Indications, Interpretation, and Pitfalls. Arch Pathol Lab Med. 2017; 141: 305-310. PubMed: https://pubmed.ncbi.nlm.nih.gov/28134589/
- Freedman J. False-positive antiglobulin tests in healthy subjects and in hospital patients. J Clin Pathol. 1979; 32: 1014-1018. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1145883/
- Gehrs BC, Friedberg RC. Autoimmune hemolytic anemia. Am J Hematol. 2002; 69: 258-271. PubMed: https://pubmed.ncbi.nlm.nih.gov/11921020/
- Capes A, Bailly S, Hantson P, Gerard L, Laterre PF. COVID-19 infection associated with autoimmune hemolytic anemia. Ann Hematol. 2020; 99: 1679-1680. PubMed: https://pubmed.ncbi.nlm.nih.gov/32542444/
- Lazarian G, Quinquenel A, Bellal M, Siavellis J, Jacquy C, et al. Autoimmune haemolytic anaemia associated with COVID-19 infection. Br J Haematol. 2020; 190: 29-31. PubMed: https://pubmed.ncbi.nlm.nih.gov/32374906/
- Lopez C, Kim J, Pandey A, Huang T, DeLoughery TG. Simultaneous onset of COVID-19 and autoimmune haemolytic anaemia. Br J Haematol. 2020;190: 31-32. PubMed: https://pubmed.ncbi.nlm.nih.gov/32369626/
- Rosenzweig JD, McThenia SS, Kaicker S. SARS-CoV-2 infection in two pediatric patients with immune cytopenias: A single institution experience during the pandemic. Pediatr Blood Cancer. 2020; 67: e28503. PubMed: https://pubmed.ncbi.nlm.nih.gov/32564495/
- Zagorski E, Pawar T, Rahimian S, Forman D. Cold agglutinin autoimmune haemolytic anaemia associated with novel coronavirus (COVID-19). Br J Haematol. 2020; 190: e183-e184. PubMed: https://pubmed.ncbi.nlm.nih.gov/32460350/
- Zulfiqar AA, Lorenzo-Villalba N, Hassler P, Andrès E. Immune Thrombocytopenic Purpura in a Patient with Covid-19. N Engl J Med. 2020; 382: e43. PubMed: https://pubmed.ncbi.nlm.nih.gov/32294340/
- Li M, Nguyen CB, Yeung Z, Sanchez K, Rosen D, Bushan S. Evans syndrome in a patient with COVID-19. Br J Haematol. 2020; 190: e59-e61. PubMed: https://pubmed.ncbi.nlm.nih.gov/32420629/
- Bastard P, Rosen LB, Zhang Q, Michailidis E, Hoffmann HH, et al. Autoantibodies against type I IFNs in patients with life-threatening COVID-19. Science. 2020; 370: 4585. PubMed: https://pubmed.ncbi.nlm.nih.gov/32972996/
- Cid J, Nogués N, Montero R, Hurtado M, Briega A, et al. Comparison of three microtube column agglutination systems for antibody screening: DG Gel, DiaMed-ID and Ortho BioVue. Transfus Med. 2006; 16: 131-136. PubMed: https://pubmed.ncbi.nlm.nih.gov/16623919/
- Sokol RJ, Hewitt S, Stamps BK. Autoimmune haemolysis: an 18-year study of 865 cases referred to a regional transfusion centre. Br Med J (Clin Res Ed). 1981; 282: 2023-2027. PubMed: https://pubmed.ncbi.nlm.nih.gov/6788179/
- Berzuini A, Bianco C, Paccapelo C, Bertolini F, Gregato G, Cattaneo A, et al. Red cell-bound antibodies and transfusion requirements in hospitalized patients with COVID-19. Blood. 2020; 136: 766-768. PubMed: https://pubmed.ncbi.nlm.nih.gov/32559762/
- Lanzavecchia A. How can cryptic epitopes trigger autoimmunity? J Exp Med. 1995; 181: 1945-1948. PubMed: https://pubmed.ncbi.nlm.nih.gov/7539032/
- Lehmann PV, Forsthuber T, Miller A, Sercarz EE. Spreading of T-cell autoimmunity to cryptic determinants of an autoantigen. Nature. 1992; 358: 155-157. PubMed: https://pubmed.ncbi.nlm.nih.gov/1377368/
- Prasad S, Starck SR, Shastri N. Presentation of Cryptic Peptides by MHC Class I Is Enhanced by Inflammatory Stimuli. J Immunol. 2016; 197: 2981-2991. PubMed: https://pubmed.ncbi.nlm.nih.gov/27647836/
- Fagiolo E, Toriani-Terenzi C. Mechanisms of immunological tolerance loss versus erythrocyte self-antigens and autoimmune hemolytic anemia. Autoimmunity. 2003; 36: 199-204. PubMed: https://pubmed.ncbi.nlm.nih.gov/14563012/
- Seitz RC, Poschmann A, Hellwege HH. Monoclonal antibodies for the detection of desialylation of erythrocyte membranes during haemolytic disease and haemolytic uraemic syndrome caused by the in vivo action of microbial neuraminidase. Glycoconj J. 1997; 14: 699-706. PubMed: https://pubmed.ncbi.nlm.nih.gov/9337082/
- Taglietti F, Drapeau CM, Grilli E, Capone A, Noto P, et al. Hemolytic anemia due to acute cytomegalovirus infection in an immunocompetent adult: a case report and review of the literature. J Med Case Rep. 2010; 4: 334. PubMed: https://pubmed.ncbi.nlm.nih.gov/20964811/
- Angileri F, Légaré S, Marino Gammazza A, Conway de Macario E, Macario AJL, Cappello F. Is molecular mimicry the culprit in the autoimmune haemolytic anaemia affecting patients with COVID-19? Br J Haematol. 2020; 190: e92-e93. PubMed: https://pubmed.ncbi.nlm.nih.gov/32453861/
- Rank G, Sutton R, Marshall V, Lundie RJ, Caddy J, et al. Novel roles for erythroid Ankyrin-1 revealed through an ENU-induced null mouse mutant. Blood. 2009; 113: 3352-3362. PubMed: https://pubmed.ncbi.nlm.nih.gov/19179303/