Pneumoconiosis is a set of pulmonary diseases associated with inhalation of an agent (e.g., dust, fumes, fibre), normally in an industrial setting where retention of a particular component is a key causative factor.1 There is no cure for pneumoconiosis, and it progressively affects patients by causing respiratory symptoms, physical impairment, and premature death.2 Due to poor control of occupational hazards, pneumoconiosis has become a serious occupational health concern across the world, especially in developing countries such as China, Brazil, and India.2,3 According to the Global Burden of Disease study,4,5 the incidence of pneumoconiosis increased from 36,186 cases in 1990 to 60,055 cases in 2017, and 125,000 deaths resulted from pneumoconiosis annually as of 2010.
In China,6 the incidence of pneumoconiosis kept increasing from 2000 to 2016, with more than 20,000 new cases per year after 2010. In 2019, the Chinese National Health Commission issued the “Pneumoconiosis Prevention and Control Action Plan”, aiming to enhance diagnosis, treatment, and pulmonary rehabilitation (PR) for pneumoconiosis patients from the grassroots level.7 Pneumoconiosis mainly occurs in rural migrant workers who are employed in unhealthy and unsafe working conditions,8 and it causes serious mental problems,9 economic hardship,10 and reduced quality of life (QoL)11 in patients. To support the vulnerable migrant workers with pneumoconiosis, a patient advocacy non-governmental organisation (NGO) named Love Save Pneumoconiosis (LSP)12 was established in 2011, and it has been promoting community-based pulmonary rehabilitation (CBPR) programs for migrant workers with pneumoconiosis since 2016.
PR is a comprehensive intervention based on a thorough patient assessment followed by patient-tailored therapies that include but are not limited to, exercise training, education, social support, and behavioural change,13 which is the most effective therapeutic strategy in managing chronic obstructive pulmonary disease.14 Recent quantitative studies have validated PR’s effect on pneumoconiosis patients’ lung function, physical performance, and health-status outcomes.15,16 However, qualitative evidence regarding PR’s impact on pneumoconiosis patients’ health and lives is lacking in the literature. Therefore, this study applied a qualitative approach to address this knowledge gap by exploring pneumoconiosis patients’ experience in a CBPR program.
METHODS
Study design
Rather than starting with a theory, this qualitative study adopted the phenomenological perspective to inductively develop patterns of meaning through participants’ views of their situations and experiences.17 Web-based semi-structured interviews using a self-made interview guide were conducted. The interview Guide was designed by reviewing relevant literature and referring to Chenail’s18 report on conducting qualitative research on patients’ experiences. Thematic analysis was applied to analyse participants’ narratives, for it allows researchers to discover common themes and thoughts from more than one participant and it is beneficial to allocate a narrative to the diverse data to gain a clear, logical understanding of the participant’s thoughts and to convey their experience.19
Study setting
The study was set in Sanchuan Pulmonary Rehabilitation Centre in Henan province. LSP established the PR centre in August 2018, and it had 215 registered pneumoconiosis patients by May 2021. The CBPR program included physical exercise (e.g., biking, dumbbell lifting, stretching exercise, breathing training), health education, leisure activities, home visits, as well as financial support and donation (e.g., financial support for medical expenses and children’s education, donation of essential medical equipment, medicine, food, and daily goods) from the NGO.
Participants and recruitment
The convenience sampling method was used to recruit participants. A PR instructor working in the PR centre assisted with the recruitment in May 2021. In this study, we only targeted male patients as pneumoconiosis is dominantly prevalent among men. The eligibility criteria for participation were: 1) man with a certified occupational pneumoconiosis diagnosis; 2) being over 18 years old; 3) PR participation was longer than one month; 4) being able to communicate in Chinese, and 5) absence of medical or cognitive conditions that would prohibit participation. Participants were acknowledged of the purpose and methods of this study by reading the recruitment post. A shopping card valuing 50 CNY (US$7.76) was rewarded to participants for their participation.
Data collection
Participants’ demographic and medical information was collected using a Patient Information form (Online Supplementary Document, Appendix A). The first author conducted the interview following the self-made Interview Guide (Online Supplementary Document, Appendix B) via Zoom videoconferencing platform.20 Before starting the interviews, the interviewer introduced herself and explained her background of growing up in a coal mine industrial area and her research interest in immigrant workers with pneumoconiosis. Participants attended the interviews during their exercise break or after the PR session in June 2021. All interviews took place in a private meeting room in the PR centre. All participants provided verbal and written consent to participate in this study and agreed to video record the interviews.
Data analysis
Data analysis was performed using the thematic analysis method. The interview data were transcribed and translated into English for analysis. Firstly, the authors thoroughly read the transcript and familiarised themselves with the data. Then a primary line-by-line coding using NVivo21 was carried out to identify the initial meaning codes. Based on the initial coding, a secondary paper-based coding was performed to confirm and finalise the meaning codes. After coding, codes that shared collective meaning were clustered into subcategories, and subcategories were furtherly abstracted into categories. Finally, categories were summarised into four themes based on their similarities and interrelationships. Although the development of the codes, subcategories, categories, and themes was described linearly, back-and-forth discussions and revisions were carried out to ensure an accurate and meaningful interpretation of participants’ responses.
Ethics considerations
This study was conducted according to the principles of the World Medical Association Declaration of Helsinki, and it was approved by the Research Ethics Committee at St. Luke’s International University in Japan (Approval Number: 20-A086) and Central South University in China (Approval Number: E202121). Written informed consent was obtained from all participants.
RESULTS
Characteristics of participants
Data saturation was reached after fifteen interviews, as all the topics from the Interview Guide (Online Supplementary Document, Appendix B) were fully covered after completing thirteen interviews, and no new themes were generated in the last two interviews. Interviews ranged from 31 to 72 minutes (median 42 minutes) in length. The fifteen participants aged from 49 to 71 (median 54). Their education level was primary school (8 participants) or middle school (7 participants). Most of them lived within 5km away from the PR centre. Their median registered PR attendance in the CBPR program was 170 (20-256) times. Participants’ sociodemographic and medical characteristics are shown in Table 1.
Experience of patients with pneumoconiosis in CBPR
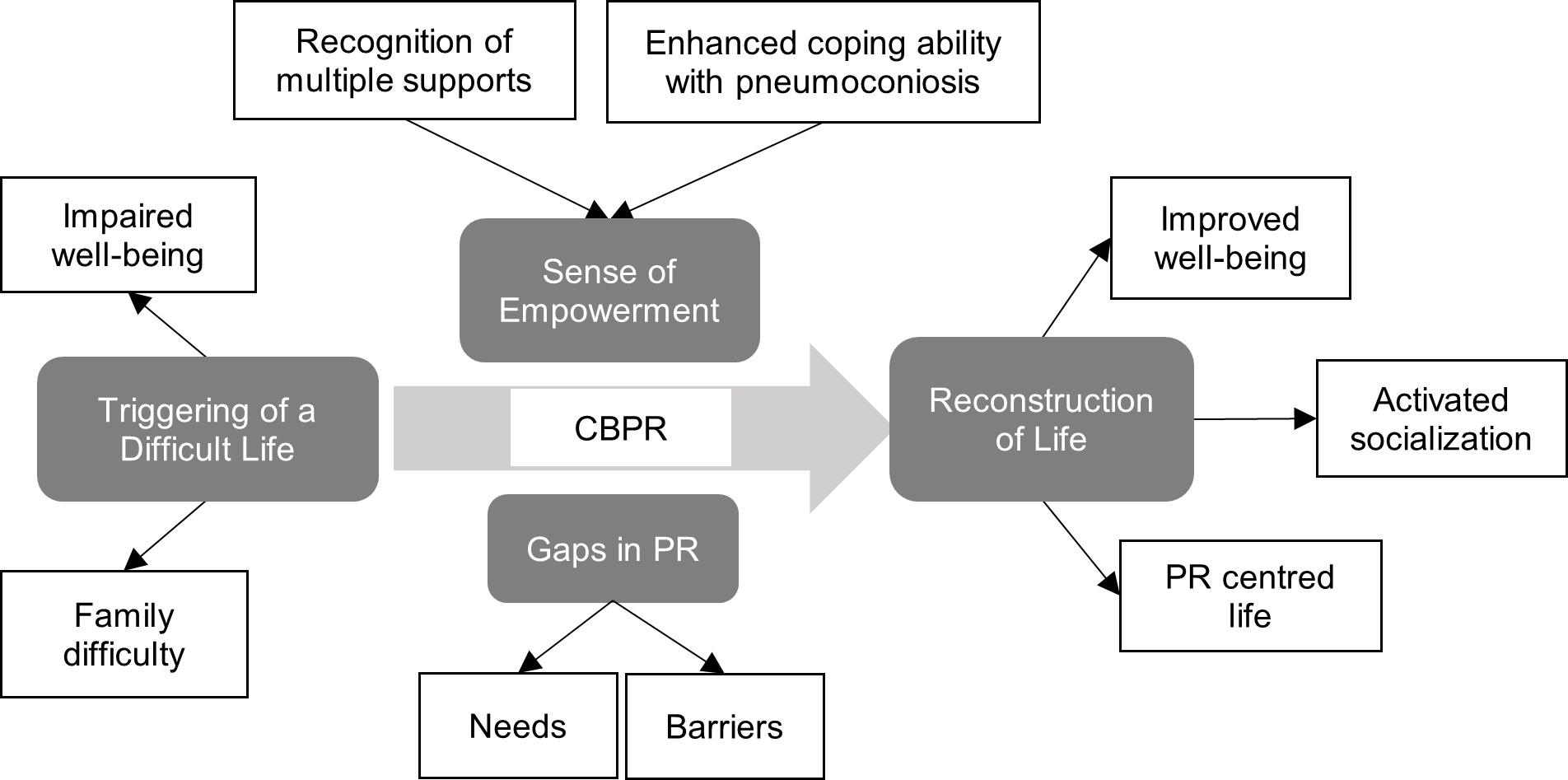
Interview data on pneumoconiosis patients’ experience in CBPR was concentrated into 26 sub-categories, nine categories, and four themes: triggering of a difficult life, reconstruction of life, sense of empowerment, and gaps in PR. Themes, categories, and subcategories are elaborated in Table 2. A schematic representation of the situation is shown in Figure 1.

Triggering of a Difficult Life
Living with pneumoconiosis, participants suffered respiratory symptoms (e.g., dyspnoea, cough, and wheezing) and had limited physical ability and mobility to perform daily activities. Their deteriorating physical health increased the risk of exacerbation, and some of them experienced frequent hospitalisation. In addition to the physical suffering, participants suffered severe mental problems from pneumoconiosis. Knowing the disease was incurable, they felt devastated and hopeless, and some of them even anticipated impending death. The poor physical and mental health disturbed their social confidence and put them at high risk of social isolation.
I will have to go to the hospital if I catch a cold. I have been hospitalised several times this year. Catching colds is very frightening to me. (02)
I thought my life could only last for a few months and I would die very soon when I was told I had pneumoconiosis. (06)
I used to be out of breath when I came to the 3rd floor. I was thinking like, I’m still young, but my health is no better than an older man’s, which frustrated me very much. (03)
Having pneumoconiosis, (In the past) I felt very stressed. It made me feel I was inferior to others. I didn’t want to talk to other people or even stay with them. (14)
Pneumoconiosis also triggered heavy financial strain and care burden in participants’ families. As the disease progressed, many participants lost their workability and became dependent, which made it impossible for them to support their families. The financial difficulty was a major cause of their mental stress and sometimes even restrained them from seeking timely and necessary treatment. Due to their inability to support the family, their wives had to shoulder the heavy family burden of being the only breadwinners, caregivers, and housekeepers in their families.
I need to feed my family…. I feel so stressed when thinking that my parents and children are relying on me. My parents have diseases and they can’t take care of themselves, and my child needs to go to school. (08)
I can’t work now. We have no income but some financial aid from the government. Generally, I don’t take medicine unless my condition is severe. Usually, I just put up with it…. (I couldn’t do anything but) wait and see. (06)
Knowing my health is not good, my wife tries to reduce my stress by sharing the family burden as much as possible. (14)
Reconstruction of Life
The CBPR program provided pneumoconiosis patients with an opportunity to reconstruct their lives. During their participation in PR, participants experienced restored physical and mental health and improved QoL. They reported improved physical capacity in performing PR exercises and daily activities. They also sensed alleviation in their symptoms (e.g., breathing difficulty) and a reduced risk of exacerbation. The only participant who didn’t see any noticeable physical improvement explained his health condition and stated that PR retarded his disease progression. Besides the physical benefits, participants also reported improved mental state, daily diet, and sleep quality.
Sometimes I go up the hill to pick up some herbal medicine and firewood. It used to be difficult, but now I can do it without too much effort. (12)
I still wheeze when I walk and don’t feel any noticeable improvement because the disease is getting worse and worse, and I know that…. It seems as if the effect is insignificant, but if I didn’t do exercise, my condition would have been worse. (02)
As I started to exercise, my mood improved, and I could sleep well. I’m not as scared as before. Now three years have passed, and my condition is still okay. (06)
Participants experienced activated socialisation and developed peer support and a sense of belonging in the CBPR program. Pneumoconiosis patients participating in the CBPR program shared similar backgrounds and occupational experiences, which enabled them to have mutual understanding and trusting. They were willing to actively engage in their peer conversations and show sympathy and encouragement to their peers. Participants also enjoyed group activities such as playing chess and singing karaoke in the PR centre. Many of them stated that the atmosphere in the PR centre was pleasant and relaxing that they would spend time in the PR centre rather than stay home.
There are many pneumoconiosis patients here. We do exercises together and talk with each other. We have chances to talk about our feelings and problems. (02)
We encourage each other to exercise by sharing our good experiences. If somebody has too much stress, we can talk to him, and it will help him reduce his stress. (13)
I feel very good the moment when I enter here. Even though you don’t exercise, it’s good to chat with people or play chess with each other. You can just have a good time here. (03)
It’s easy to feel stressed and unhappy when staying alone. Coming outside and meeting people here makes me feel relaxed and happy. (05)
As participants gained positive physical and psychosocial experiences in the CBPR program, they tended to lead a PR-centred life. Many participants formed a habit to do exercise. For some people, PR had become an essential daily routine that they would not skip; as one participant described, “skipping PR was like skipping meals for me”. Participants showed high intrinsic and extrinsic motivation to take PR. Those with young children were highly self-motivated to take PR to prolong their survival so that they could keep their families complete and watch their children grow up. Many participants expressed gratitude for the CBPR program and were motivated to take PR to show their appreciation.
I developed a habit of exercising after I came to the rehabilitation centre. I can always find time to exercise, whether rainy or sunny, no matter when and where. (06)
(My motivation for taking PR is) To save my life and keep my family complete. As long as I am here, my family is fine, and my children have a father, so I keep exercising and try to stay in a good mood. It’s good for both my family and me. (02)
I am grateful that this PR centre was built in Sanchuan. Personally speaking, it’s very beneficial for me. I’m quite satisfied that my body has recovered to this extent…. I formed a habit of exercising. When the time comes, I want to come here. If I don’t have anything to do at home, the best thing I can do is to come here and exercise. (03)
Sense of Empowerment
Through taking PR, participants were empowered with strengthened disease-adapting and coping abilities. Instead of being devastated and frustrated, they learned to accept and adapt to pneumoconiosis by adopting positive thinking. Participants regained hope and confidence to maximise their remaining health by adhering to PR and applying healthy behaviours. As they gained greater control over their health, they tried to positively influence their peer patients by sharing their good experiences.
Before, I always thought that pneumoconiosis was incurable, and I worried about the side effects of the medicine…. Now I know I don’t need to stress myself with negative thoughts. (14)
By doing exercise, you can stay healthy and live for a few more years. It’s for your own sake. Now the society and policy are getting better and better. To experience more of it, you need to have the courage to live. (09)
Some people think nothing can make a big difference because they believe the disease is incurable. However, I want to encourage them to put away the psychological burden and focus on exercise…. You will get experience if you continue, and you can share your experience to help others. (02)
Participants were empowered by the support from their families, PR staff, volunteers, and the NGO. Their families’ understanding, caring, and their supportive words and gestures positively influenced participants to take PR. The PR instructors were perceived as patient, responsible, and trustworthy by participants. They not only gave PR instructions but also conducted regular home visits to investigate patients’ family difficulties and link them to necessary support from the NGO. As a patient advocacy NGO, LSP kept offering donations and financial and social support to help migrant workers with pneumoconiosis and gained their heartful gratitude.
Sometimes my wife encourages me to go for a walk when I’m not feeling very well or don’t want to move. She would accompany me for a walk outside and then suggest coming to the PR centre…. Now I can always come without being reminded or pushed by her. (03)
The PR instructor always tells us that PR is good for pneumoconiosis and that the effect could be better than medicine…. She also tries to help us to have a good mindset and encourage us to continue to exercise. (04)
Volunteers come to give us donations, such as rice, wheat, oil, and quilts when winter comes. They support us as much as they can…. Knowing that many kind people care about us, we have no reason to give up on ourselves. (10)
Gaps in PR
Although participants were highly appreciative of and satisfied with the CBPR program and no perceived downsides of PR were reported, they still had unmet needs and barriers in the CBPR program. They needed additional equipment and services in the PR centre, including adequate exercise equipment such as bikes, oxygen machines for renting, leisure entertainment, countermeasures for emergencies, and health check-up services. They also expected supporting policies for pneumoconiosis families and financial support for their children’s education. Participants identified barriers to taking PR as lack of knowledge, exacerbations, conflicting priorities, and environmental obstacles (e.g., bad weather, inconvenient roads, and long-distance).
Well, there will be no income if I can’t work any longer… then my child’s education will be a problem. I have nothing to expect but support for my child to go to school. That will be enough. (07)
Love Save Pneumoconiosis and the volunteers have helped us a lot…. I hope the government takes more responsibility to help improve our lives. (06)
If my parents are ill or hospitalised, I will have to take care of them. If there is field labour to do, I will not be able to come. (08)
DISCUSSION
This study disclosed pneumoconiosis patients’ experience in PR and added to the understanding of the CBPR program’s impact on the health and lives of rural migrant workers with pneumoconiosis in China. Pneumoconiosis caused deteriorating physical health, severe mental stress, social isolation and financial hardship to patients. The CBPR program allowed them to restore their physical and psychosocial health, and they achieved reconstructing their lives by leading a PR-centred life. Participating in the CBPR program, pneumoconiosis patients recognised multiple supports and were empowered with enhanced disease-coping abilities and strengthened hope to survive. Overall, participants reflected on their positive experience in the CBPR program, despite their unmet needs and existing barriers in PR.
Pneumoconiosis patients’ disease-suffering experiences regarding respiratory symptoms, deteriorating physical condition, limited mobility, and social isolation are also reported among patients with other chronic respiratory diseases.22,23 This study highlighted pneumoconiosis patients’ serious mental suffering, which is in line with Huang and Hu’s9 report on the significant low self-esteem and high level of anxiety and depression among pneumoconiosis patients compared to the general population in China. As middle-aged men who are expected to take a pivotal family role in traditional Chinese families, their inability to support their family harms their self-esteem and confidence and burdens them with heavy mental stress. Meanwhile, their wives experience jeopardised physical, emotional, and social well-being from the demanding and overloaded care burden.10,24 These findings suggest that future research on the family-oriented management of pneumoconiosis is needed to improve the health and lives of both pneumoconiosis patients and their caregivers.
Pneumoconiosis patients’ healthy transition and life reconstruction experiences in the CBPR program are congruent with former PR-related studies revealing patients’ PR experience in terms of reduced symptoms, improved physical, mental, emotional, and social function, enhanced sense of control, and increased disease management ability.25–27 Pneumoconiosis patients reported improvements in their mental state, physical capacity, mobility, and daily activities, which corroborated the quantitative evidence regarding PR’s effectiveness in improving physical functional capacity,15,16 psychological symptoms,28 and QoL16 for patients with chronic respiratory diseases. In this study, pneumoconiosis patients also delightfully reported their active social life in the CBPR program. They shared commonalities and mutual understanding and had a sense of bonding and belonging in their groups. For pneumoconiosis patients who bear heavy mental stress and are socially isolated, peer support in the CBPR program may effectively reduce their mental problems, boost their social confidence, and increase their participation in PR.
A sense of empowerment was abstracted from pneumoconiosis patients’ narratives in this study. In China, migrant workers with pneumoconiosis are part of the lowest socio-economic populations who face social and spatial injustice and have limited access to social resources and health services.8 The NGO-supported CBPR program functioned as a patient advocating and supporting platform that links pneumoconiosis patients to necessary support and health resources. Participating in the CBPR program, participants recognised multiple supports from their families, peer patients, PR staff, volunteers, and the NGO. They not only developed enhanced disease-coping skills but also regained hope and confidence to maximise their health and lives. These findings suggest that promoting the CBPR program and providing multiple supports to patients and their families are critical strategies to empower the vulnerable migrant workers with pneumoconiosis in China.
In contrast to the low uptake and poor adherence in PR reported among COPD patients in former studies,29–31 this study encouragingly found that pneumoconiosis patients had relatively high uptake and good adherence in PR. Several reasons may contribute to this finding. First of all, participants showed strong motivation to take PR. They were highly self-motivated to stay health so that they could take care of their families, especially their young children. They were also motivated to take PR to show their appreciation for the support they received from the CBPR program. It was reported that patients living alone or lacking family support had low motivation to take PR.30 In this study, all participants lived with their families, and family support positively influenced them to take PR. Financial strain was reported as an important barrier for patients with low economic status to use PR services.32 This NGO-supported CBPR program for pneumoconiosis patients was free, and patients could receive donations and apply for financial support for their hospitalisation and their children’s education, which might be a critical incentive factor that facilitated their participation. Another contributing factor was their convenient access to the CBPR program for travelling distance and transportation were identified as significant barriers that hinder patients’ uptake and adherence to PR.30,33 Last but not least, comparing to patients with other chronic respiratory conditions, pneumoconiosis patients in this study were averagely younger and thus, they might have a higher physical potential to take physical exercise and experience positive outcomes, which might have enhanced their continence in PR.
To achieve successful participation in PR, a flexible and tailored approach is required to deliver PR according to patients’ needs and preferences, and PR programs should be fun and provide experience that patients don’t want to miss.34,35 Among all the unmet needs stated by participants in this study, one participant passionately suggested integrating leisure entertainment (e.g., karaoke) into the CBPR program, which implies that enjoyment is a critical element to keep patients in PR. Participants’ barriers to PR identified in this study regarding lack of knowledge, bad health conditions, conflicting priorities, and environmental obstacles correspond to previous PR studies.30,32,33 Lacking knowledge and perceived benefit of PR interfered with both uptake and completion.30 The initial and essential step to engage patients in PR is to provide education and counselling to increase their knowledge and enhance their motivation for behavioural change, and ongoing adherence could be enhanced by tangible results, improved health outcomes, increased self-confidence, and a supportive environment in the PR program.36
Although this study achieved data saturation and gained insight into the CBPR program’s impact on pneumoconiosis patients’ health and lives, several limitations should be considered when interpreting the results of this study. Firstly, in this study, participating patients were highly homogeneous regarding their demographic characteristics and socioeconomic status, which may limit the representativeness of patients with different sociodemographic characteristics (e.g., underdiagnosed patients, young patients, patients with better social economic status, and female patients). Secondly, participants might want to appear grateful for the CBPR program and thus might have emphasised their positive experiences and neglected the downsides. Thirdly, the interviews were conducted in Chinese, and the interview data were translated into English for analysis. There were minor translation adjustments during the translation process. However, the meaning of what the participants said wasn’t changed.
CONCLUSIONS
The CBPR program integrating multiple supports empowered the vulnerable migrant workers with pneumoconiosis and facilitated their health transition and life reconstruction experience. To optimise their PR experience and improve their QoL, health service addressing their unmet needs and barriers in PR is needed. PR for pneumoconiosis patients with different sociodemographic characteristics and family-oriented management of pneumoconiosis should be explored in future research.
Acknowledgements
We want to express our gratitude to Dr Erika Ota, Dr Edward Barroga, and Dr Maasa Kobayashi for their valuable insight, comments, and advice on this study. We thank Dr Sarah E Porter for her English editing support in this manuscript. We also appreciate Ms Qiuli Shi’s support in participant recruitment. Finally, we would like to thank the fifteen participants for their contribution to this study. This study was approved by the Research Ethics Committee at St. Luke’s International University in Japan (Approval Number: 20-A086) and Central South University in China (Approval Number: E202121).
Data availability
The data supporting this study’s findings are available on request from the corresponding author (PM).
Funding
No funds, grants, or other financial support were received for this study.
Authorship contributions
This work is based on the master’s thesis of the first author (PM). YN supervised this work. PM and YN together developed the study conception and study design. PM was trained to conduct interviews and use NVivo to perform qualitative data analysis. PM conducted the interviews and translated the transcript. PM and YN performed data analysis. PM drafted the manuscript, and YN provided critical instruction and revision.
Competing interest
The authors completed the Unified Competing Interest form at http://www.icmje.org/disclosure-of-interest/ (available upon request from the corresponding author), and declare no conflicts of interest.
Corresponding author:
Panpan Ma
Email: [email protected]
Address: Room 207, Livil Shangri-La, Murakami 2092-3, Yachiyo, Chiba, 276-0028, Japan