Glomerular Deposition of Nephritis-Associated Plasmin Receptor (NAPlr) and Related Plasmin Activity: Key Diagnostic Biomarkers of Bacterial Infection-related Glomerulonephritis

Abstract
:1. Introduction
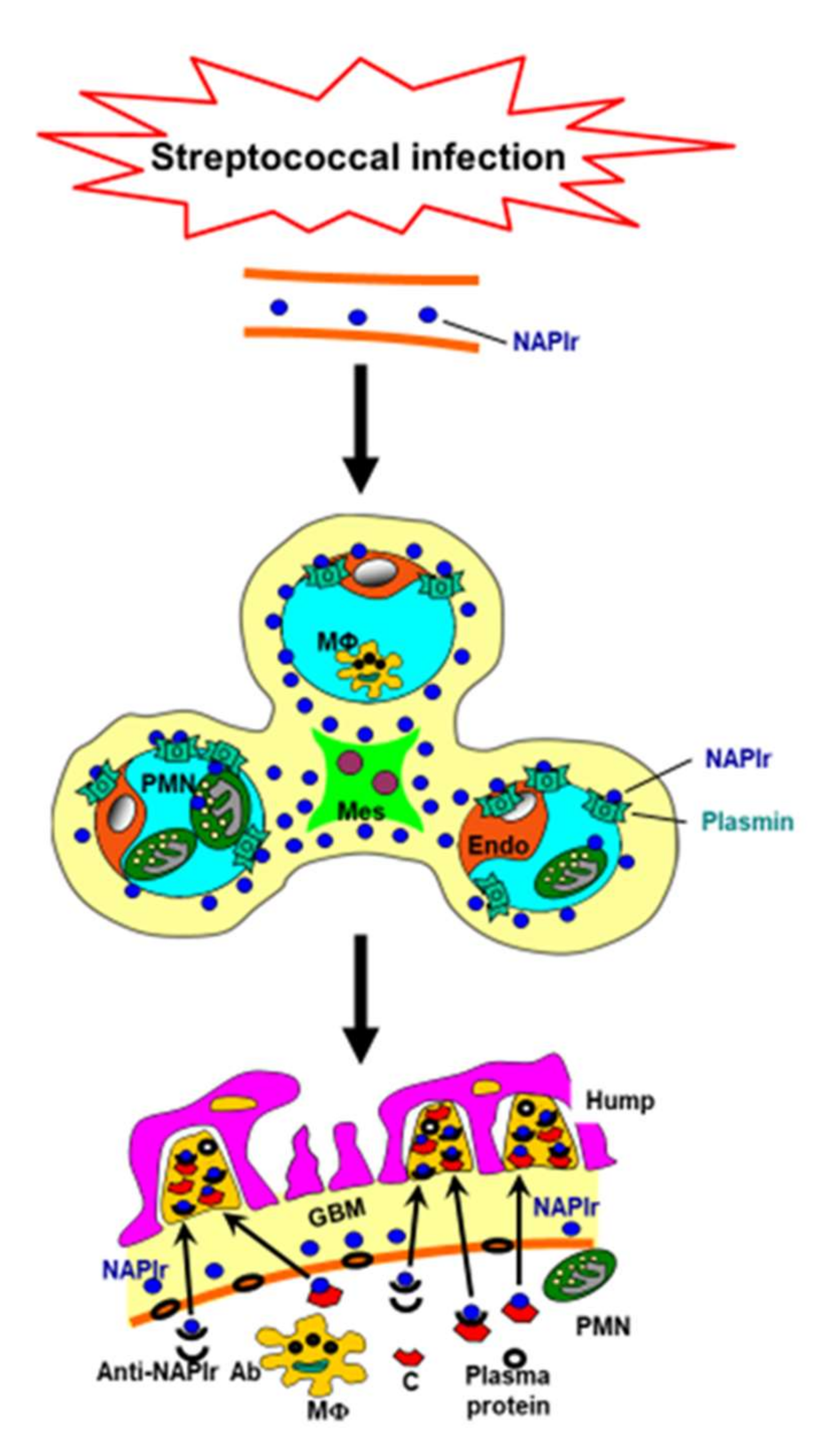
2. NAPlr and Plasmin Activity in Glomeruli as Biomarkers of PSAGN
3. Streptococcal Infection-related Nephritis (SIRN): Glomerular Diseases with NAPlr Deposition and Related Plasmin Activity Induced by Streptococcal Infection
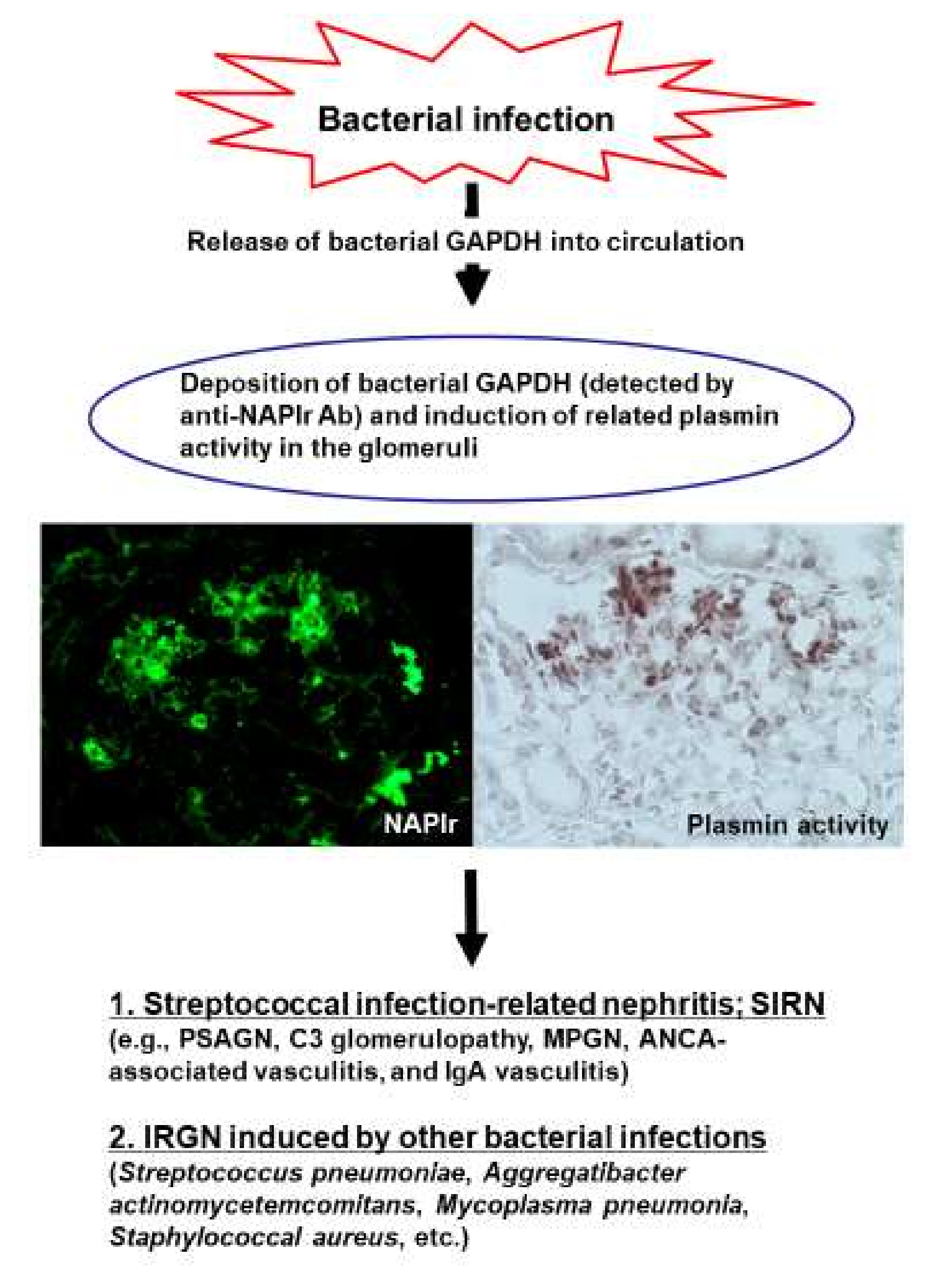
4. Glomerular NAPlr Deposition and Plasmin Activity as Candidates of General Biomarkers of Bacterial IRGN
5. NAPlr and Plasmin Activity in Extraglomerular Regions
6. Concluding Remarks
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Prasad, N.; Patel, M.R. Infection-Induced Kidney Diseases. Front. Med. 2018, 5, 327. [Google Scholar] [CrossRef] [PubMed]
- Oda, T.; Yoshizawa, N.; Yamakami, K.; Sakurai, Y.; Takechi, H.; Yamamoto, K.; Oshima, N.; Kumagai, H. The role of nephritis-associated plasmin receptor (NAPlr) in glomerulonephritis associated with streptococcal infection. J. Biomed. Biotechnol. 2012, 2012, 417675. [Google Scholar] [CrossRef] [PubMed]
- Soderholm, A.T.; Barnett, T.C.; Sweet, M.J.; Walker, M.J. Group A streptococcal pharyngitis: Immune responses involved in bacterial clearance and GAS-associated immunopathologies. J. Leukoc. Biol. 2018, 103, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Satoskar, A.A.; Parikh, S.V.; Nadasdy, T. Epidemiology, pathogenesis, treatment and outcomes of infection-associated glomerulonephritis. Nat. Rev. Nephrol. 2020, 16, 32–50. [Google Scholar] [CrossRef]
- Nasr, S.H.; Radhakrishnan, J.; D’Agati, V.D. Bacterial infection-related glomerulonephritis in adults. Kidney Int. 2013, 83, 792–803. [Google Scholar] [CrossRef] [Green Version]
- Usui, J.; Tawara-Iida, T.; Takada, K.; Ebihara, I.; Ueda, A.; Iwabuchi, S.; Ishizu, T.; Iitsuka, T.; Takemura, K.; Kawamura, T.; et al. Temporal Changes in Post-Infectious Glomerulonephritis in Japan (1976–2009). PLoS ONE 2016, 11, e0157356. [Google Scholar] [CrossRef] [Green Version]
- Nasr, S.H.; Fidler, M.E.; Valeri, A.M.; Cornell, L.D.; Sethi, S.; Zoller, A.; Stokes, M.B.; Markowitz, G.S.; D’Agati, V.D. Postinfectious glomerulonephritis in the elderly. J. Am. Soc. Nephrol. 2011, 22, 187–195. [Google Scholar] [CrossRef]
- Yoshizawa, N.; Yamakami, K.; Fujino, M.; Oda, T.; Tamura, K.; Matsumoto, K.; Sugisaki, T.; Boyle, M.D. Nephritis-associated plasmin receptor and acute poststreptococcal glomerulonephritis: Characterization of the antigen and associated immune response. J. Am. Soc. Nephrol. 2004, 15, 1785–1793. [Google Scholar] [CrossRef] [Green Version]
- Oda, T.; Yamakami, K.; Omasu, F.; Suzuki, S.; Miura, S.; Sugisaki, T.; Yoshizawa, N. Glomerular plasmin-like activity in relation to nephritis-associated plasmin receptor in acute poststreptococcal glomerulonephritis. J. Am. Soc. Nephrol. 2005, 16, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Butera, G.; Mullappilly, N.; Masetto, F.; Palmieri, M.; Scupoli, M.T.; Pacchiana, R.; Donadelli, M. Regulation of Autophagy by Nuclear GAPDH and Its Aggregates in Cancer and Neurodegenerative Disorders. Int. J. Mol. Sci. 2019, 20, 2062. [Google Scholar] [CrossRef] [Green Version]
- Terao, Y.; Yamaguchi, M.; Hamada, S.; Kawabata, S. Multifunctional glyceraldehyde-3-phosphate dehydrogenase of Streptococcus pyogenes is essential for evasion from neutrophils. J. Biol. Chem. 2006, 281, 14215–14223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergmann, S.; Rohde, M.; Hammerschmidt, S. Glyceraldehyde-3-phosphate dehydrogenase of Streptococcus pneumoniae is a surface-displayed plasminogen-binding protein. Infect. Immun. 2004, 72, 2416–2419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oda, T.; Yoshizawa, N.; Yamakami, K.; Tamura, K.; Kuroki, A.; Sugisaki, T.; Sawanobori, E.; Higashida, K.; Ohtomo, Y.; Hotta, O.; et al. Localization of nephritis-associated plasmin receptor in acute poststreptococcal glomerulonephritis. Hum. Pathol. 2010, 41, 1276–1285. [Google Scholar] [CrossRef]
- Rodriguez-Iturbe, B.; Batsford, S. Pathogenesis of poststreptococcal glomerulonephritis a century after Clemens von Pirquet. Kidney Int. 2007, 71, 1094–1104. [Google Scholar] [CrossRef] [Green Version]
- Fujino, M.; Yamakami, K.; Oda, T.; Omasu, F.; Murai, T.; Yoshizawa, N. Sequence and expression of NAPlr is conserved among group A streptococci isolated from patients with acute poststreptococcal glomerulonephritis (APSGN) and non-APSGN. J. Nephrol. 2007, 20, 364–369. [Google Scholar] [PubMed]
- Gopalakrishnan, N.; Jeyachandran, D.; Abeesh, P.; Dineshkumar, T.; Kurien, A.A.; Sakthirajan, R.; Balasubramaniyan, T. Infection-related glomerulonephritis in a renal allograft. Saudi J. Kidney Dis. Transplant. 2017, 28, 1421–1426. [Google Scholar]
- Bullen, A.; Shah, M.M. De Novo Postinfectious Glomerulonephritis Secondary to Nephritogenic Streptococci as the Cause of Transplant Acute Kidney Injury: A Case Report and Review of the Literature. Case Rep. Transplant. 2018, 2018, 2695178. [Google Scholar] [CrossRef]
- Sawanobori, E.; Umino, A.; Kanai, H.; Matsushita, K.; Iwasa, S.; Kitamura, H.; Oda, T.; Yoshizawa, N.; Sugita, K.; Higashida, K. A prolonged course of Group A streptococcus-associated nephritis: A mild case of dense deposit disease (DDD)? Clin. Nephrol. 2009, 71, 703–707. [Google Scholar] [CrossRef]
- Suga, K.; Kondo, S.; Matsuura, S.; Kinoshita, Y.; Kitano, E.; Hatanaka, M.; Kitamura, H.; Hidaka, Y.; Oda, T.; Kagami, S. A case of dense deposit disease associated with a group A streptococcal infection without the involvement of C3NeF or complement factor H deficiency. Pediatric Nephrol. 2010, 25, 1547–1550. [Google Scholar] [CrossRef]
- Yamakami, K.; Yoshizawa, N.; Wakabayashi, K.; Takeuchi, A.; Tadakuma, T.; Boyle, M.D. The potential role for nephritis-associated plasmin receptor in acute poststreptococcal glomerulonephritis. Methods 2000, 21, 185–197. [Google Scholar] [CrossRef]
- Okabe, M.; Tsuboi, N.; Yokoo, T.; Miyazaki, Y.; Utsunomiya, Y.; Hosoya, T. A case of idiopathic membranoproliferative glomerulonephritis with a transient glomerular deposition of nephritis-associated plasmin receptor antigen. Clin. Exp. Nephrol. 2012, 16, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Kohatsu, K.; Suzuki, T.; Yazawa, M.; Yahagi, K.; Ichikawa, D.; Koike, J.; Oda, T.; Shibagaki, Y. Granulomatosis With Polyangiitis Induced by Infection. Kidney Int. Rep. 2019, 4, 341–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yano, K.; Suzuki, H.; Oda, T.; Ueda, Y.; Tsukamoto, T.; Muso, E. Crescentic poststreptococcal acute glomerulonephritis accompanied by small vessel vasculitis: Case report of an elderly male. BMC Nephrol. 2019, 20, 471. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, Y.; Yoshizawa, N.; Oda, T.; Imakiire, T.; Suzuki, S.; Miura, S. Streptococcal origin of a case of Henoch-Schoenlein purpura nephritis. Clin. Nephrol. 2006, 65, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Iseri, K.; Iyoda, M.; Yamamoto, Y.; Kobayashi, N.; Oda, T.; Yamaguchi, Y.; Shibata, T. Streptococcal Infection-related Nephritis (SIRN) Manifesting Membranoproliferative Glomerulonephritis Type I. Intern. Med. 2016, 55, 647–650. [Google Scholar] [CrossRef] [Green Version]
- Prasto, J.; Kaplan, B.S.; Russo, P.; Chan, E.; Smith, R.J.; Meyers, K.E. Streptococcal infection as possible trigger for dense deposit disease (C3 glomerulopathy). Eur J. Pediatrics 2014, 173, 767–772. [Google Scholar] [CrossRef]
- Fremeaux-Bacchi, V.; Weiss, L.; Demouchy, C.; May, A.; Palomera, S.; Kazatchkine, M.D. Hypocomplementaemia of poststreptococcal acute glomerulonephritis is associated with C3 nephritic factor (C3NeF) IgG autoantibody activity. Nephrol. Dial. Transplant. 1994, 9, 1747–1750. [Google Scholar]
- Odaka, J.; Kanai, T.; Ito, T.; Saito, T.; Aoyagi, J.; Betsui, H.; Oda, T.; Ueda, Y.; Yamagata, T. A case of post-pneumococcal acute glomerulonephritis with glomerular depositions of nephritis-associated plasmin receptor. CEN Case Rep. 2015, 4, 112–116. [Google Scholar] [CrossRef] [Green Version]
- Komaru, Y.; Ishioka, K.; Oda, T.; Ohtake, T.; Kobayashi, S. Nephritis-associated plasmin receptor (NAPlr) positive glomerulonephritis caused by Aggregatibacter actinomycetemcomitans bacteremia: A case report. Clin. Nephrol. 2018, 90, 155–160. [Google Scholar] [CrossRef]
- Hirano, D.; Oda, T.; Ito, A.; Yamada, A.; Kakegawa, D.; Miwa, S.; Umeda, C.; Takemasa, Y.; Tokunaga, A.; Wajima, T.; et al. Glyceraldehyde-3-phosphate dehydrogenase of Mycoplasma pneumoniae induces infection-related glomerulonephritis. Clin. Nephrol. 2019, 92, 263–272. [Google Scholar] [CrossRef]
- Grundel, A.; Pfeiffer, M.; Jacobs, E.; Dumke, R. Network of Surface-Displayed Glycolytic Enzymes in Mycoplasma pneumoniae and Their Interactions with Human Plasminogen. Infect. Immun. 2015, 84, 666–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Modun, B.; Williams, P. The staphylococcal transferrin-binding protein is a cell wall glyceraldehyde-3-phosphate dehydrogenase. Infect. Immun. 1999, 67, 1086–1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takehara, E.; Mandai, S.; Shikuma, S.; Akita, W.; Chiga, M.; Mori, T.; Oda, T.; Kuwahara, M.; Uchida, S. Post-infectious Proliferative Glomerulonephritis with Monoclonal Immunoglobulin G Deposits Associated with Complement Factor H Mutation. Intern. Med. 2017, 56, 811–817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okabe, M.; Takamura, T.; Tajiri, A.; Tsuboi, N.; Ishikawa, M.; Ogura, M.; Ohashi, R.; Oda, T.; Yokoo, T. A case of infection-related glomerulonephritis with massive eosinophilic infiltration. Clin. Nephrol. 2018, 90, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Ando, F.; Sohara, E.; Ito, E.; Okado, T.; Rai, T.; Uchida, S.; Sasaki, S. Acute poststreptococcal glomerulonephritis with acute interstitial nephritis related to streptococcal pyrogenic exotoxin B. Clin. Kidney J. 2013, 6, 347–348. [Google Scholar] [CrossRef] [Green Version]
- Chang, J.F.; Peng, Y.S.; Tsai, C.C.; Hsu, M.S.; Lai, C.F. A possible rare cause of renal failure in streptococcal infection. Nephrol. Dial. Transplant. 2011, 26, 368–371. [Google Scholar] [CrossRef] [Green Version]
- Uchida, T.; Oda, T.; Takechi, H.; Matsubara, H.; Watanabe, A.; Yamamoto, K.; Oshima, N.; Sakurai, Y.; Kono, T.; Shimazaki, H.; et al. Role of tubulointerstitial plasmin in the progression of IgA nephropathy. J. Nephrol. 2016, 29, 53–62. [Google Scholar] [CrossRef]
- Yoshida, M.; Yamakawa, H.; Yabe, M.; Ishikawa, T.; Takagi, M.; Matsumoto, K.; Hamaguchi, A.; Ogura, M.; Kuwano, K. Diffuse alveolar hemorrhage in a patient with acute poststreptococcal glomerulonephritis caused by impetigo. Intern. Med. 2015, 54, 961–964. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Pathogen | Nucleotide | Amino acid | ||
|---|---|---|---|---|
| Identity | Similarity | Identity | Similarity | |
| Aggregatibacter actinomycetemcomitans | 59 | 59 | 50 | 85 |
| Mycoplasma pneumonia | 60 | 60 | 54 | 87 |
| Staphylococcal aureus | 54 | 54 | 67 | 92 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uchida, T.; Oda, T. Glomerular Deposition of Nephritis-Associated Plasmin Receptor (NAPlr) and Related Plasmin Activity: Key Diagnostic Biomarkers of Bacterial Infection-related Glomerulonephritis. Int. J. Mol. Sci. 2020, 21, 2595. https://doi.org/10.3390/ijms21072595
Uchida T, Oda T. Glomerular Deposition of Nephritis-Associated Plasmin Receptor (NAPlr) and Related Plasmin Activity: Key Diagnostic Biomarkers of Bacterial Infection-related Glomerulonephritis. International Journal of Molecular Sciences. 2020; 21(7):2595. https://doi.org/10.3390/ijms21072595
Chicago/Turabian StyleUchida, Takahiro, and Takashi Oda. 2020. "Glomerular Deposition of Nephritis-Associated Plasmin Receptor (NAPlr) and Related Plasmin Activity: Key Diagnostic Biomarkers of Bacterial Infection-related Glomerulonephritis" International Journal of Molecular Sciences 21, no. 7: 2595. https://doi.org/10.3390/ijms21072595