
Reactive Oxygen Species Produced by 5-Aminolevulinic Acid Photodynamic Therapy in the Treatment of Cancer
 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
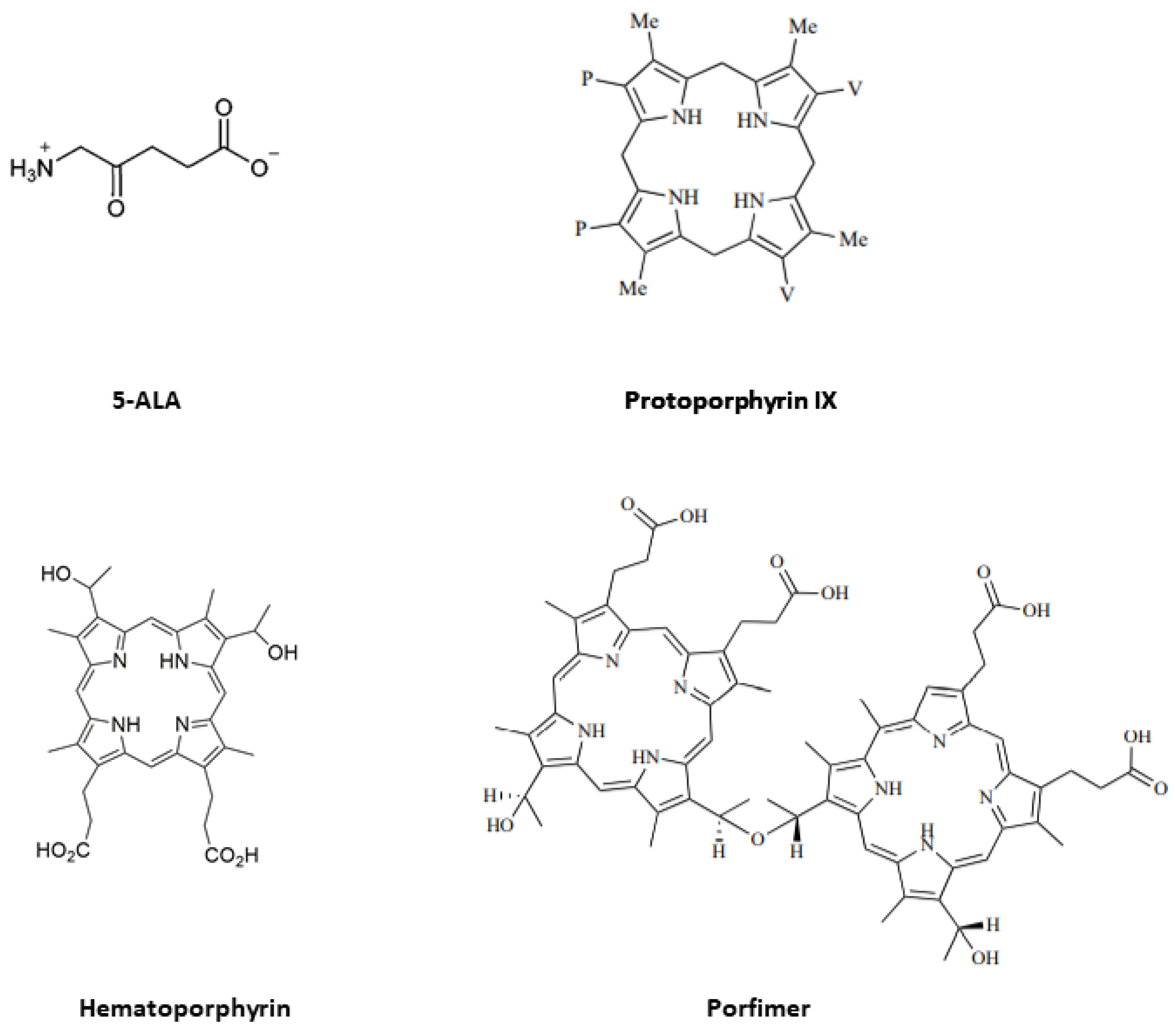
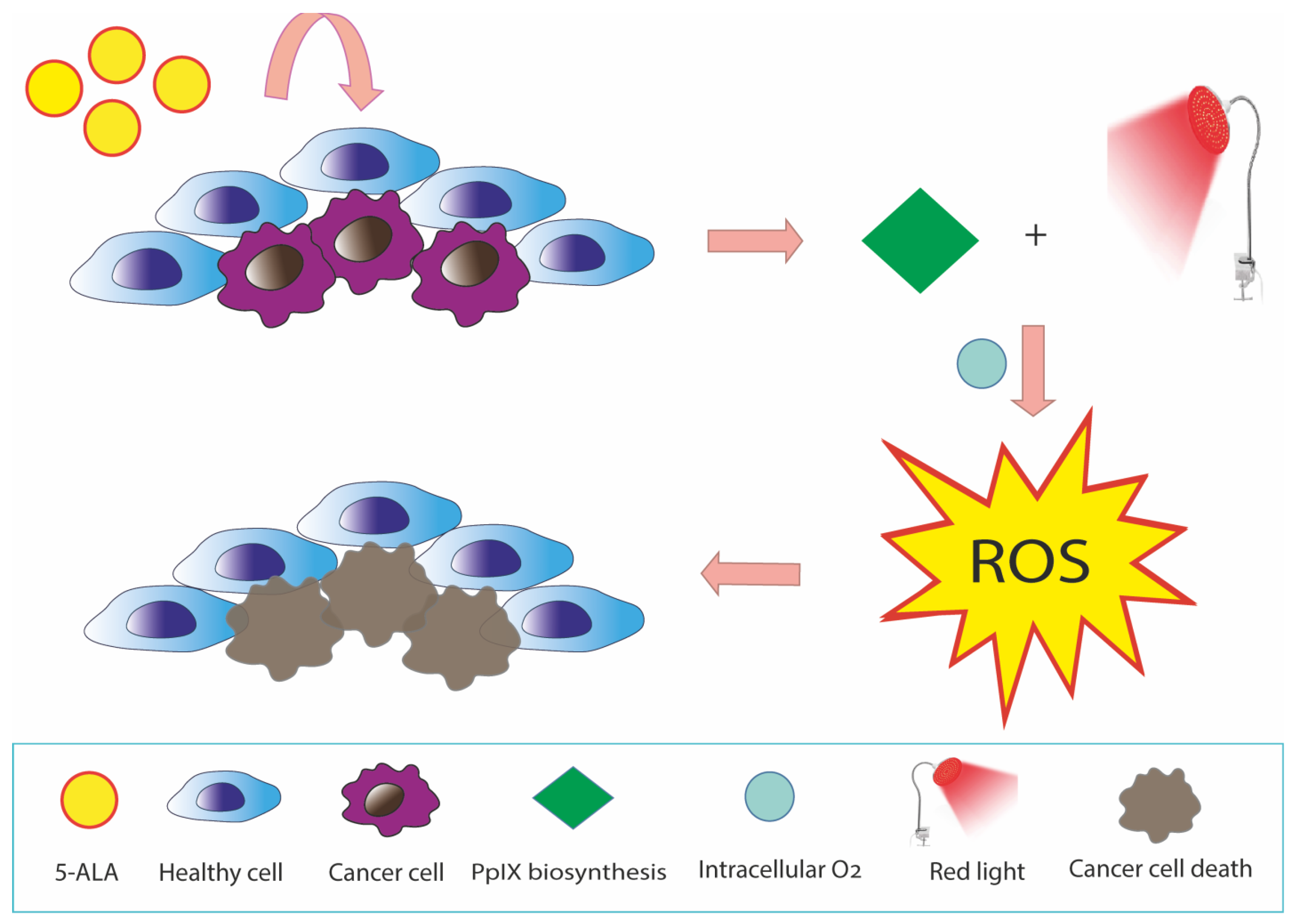
:1. Introduction: 5-Aminolevulinic Acid Photodynamic Therapy
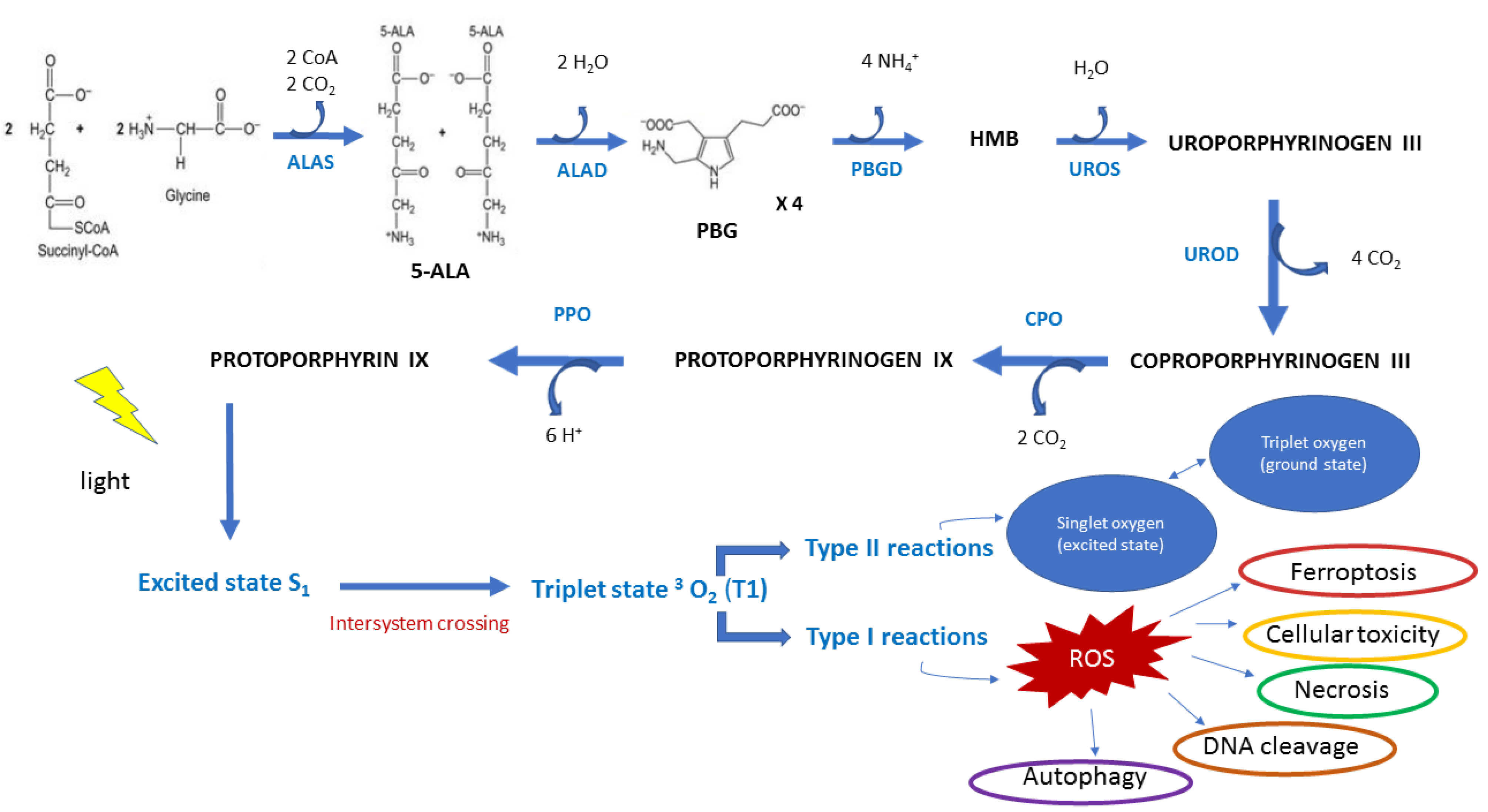
2. Inorganic Nutrients in the Biosynthesis of Heme
3. ROS Production by 5-ALA-PDT
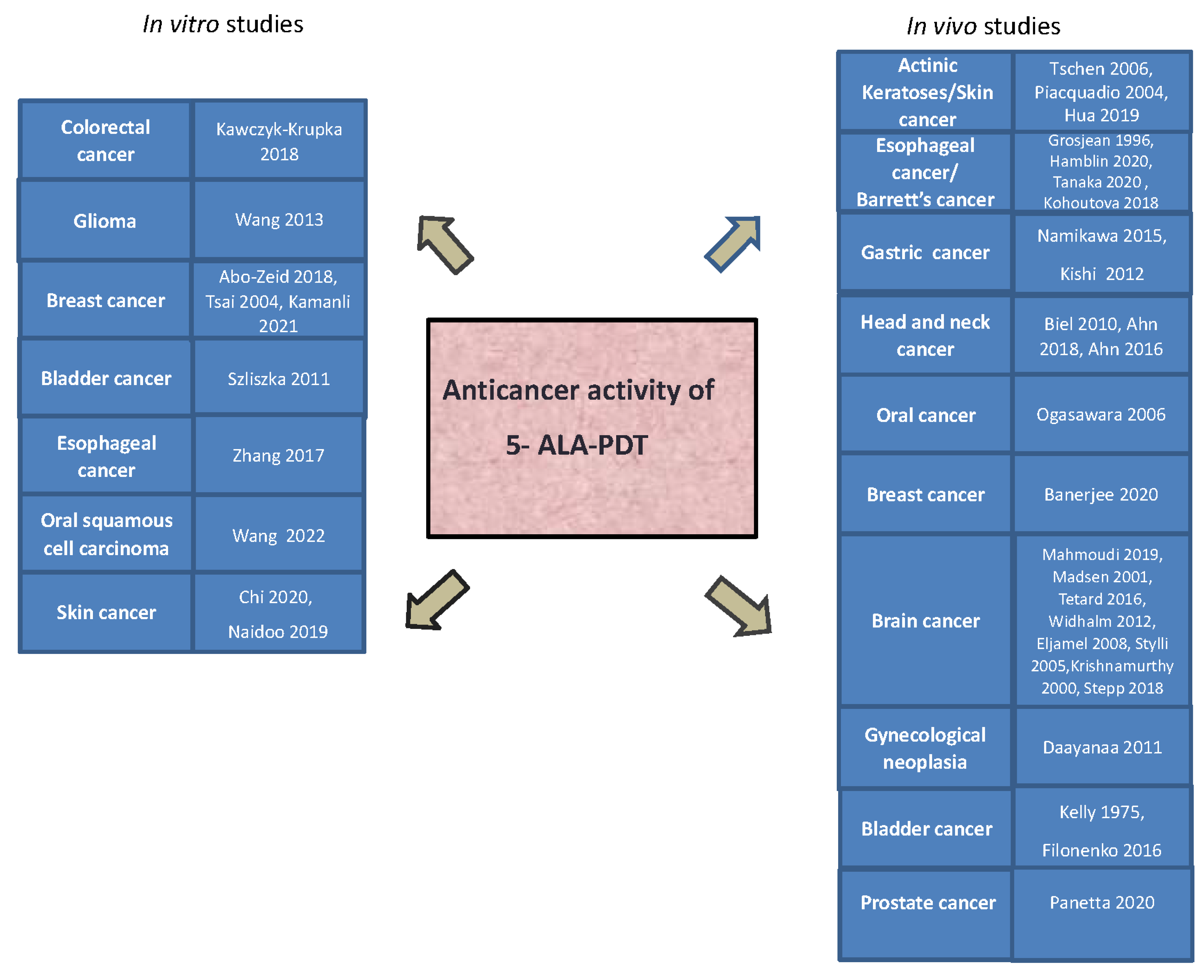
4. 5-ALA-PDT Treatment in Different Type of Cancers
4.1. In Vitro Studies
4.1.1. Colorectal Cancer
4.1.2. Glioma
4.1.3. Breast Cancer
4.1.4. Bladder Cancer
4.1.5. Esophageal Cancer
4.1.6. Oral Potentially Malignant Disorders and Oral Squamous Cell Carcinoma
4.1.7. Skin Cancer
4.2. Clinical Applications of 5-ALA-PDT-In Vivo Studies
4.2.1. Esophageal Cancer and Barrett’s Esophagus
4.2.2. Gastric Cancer
4.2.3. Head and Neck Cancer
4.2.4. Oral Cancer
4.2.5. Breast Cancer
4.2.6. Brain Cancer
4.2.7. Gynecological Neoplasia
4.2.8. Bladder Cancer
4.2.9. Prostate Cancer
4.2.10. Actinic Keratoses/Skin Cancer
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Anwar, S.; Almatroudi, A.; Alsahli, M.A.; Khan, M.A.; Khan, A.A.; Rahmani, A.H. Natural products: Implication in cancer prevention and treatment through modulating various biological activities. Anti-Cancer Agents Med. Chem. (Former. Curr. Med. Chem.-Anti-Cancer Agents) 2020, 20, 2025–2040. [Google Scholar] [CrossRef] [PubMed]
- Bentzen, S.M.; Heeren, G.; Cottier, B.; Slotman, B.; Glimelius, B.; Lievens, Y.; Van den Bogaert, W. Towards evidence-based guidelines for radiotherapy infrastructure and staffing needs in Europe: The ESTRO QUARTS project. Radiother. Oncol. 2005, 75, 355–365. [Google Scholar] [CrossRef] [PubMed]
- Dörr, W.; Hendry, J.H. Consequential late effects in normal tissues. Radiother. Oncol. 2001, 61, 223–231. [Google Scholar] [CrossRef]
- Nurgali, K.; Jagoe, R.T.; Abalo, R. Adverse effects of cancer chemotherapy: Anything new to improve tolerance and reduce sequelae? Front. Media SA 2018, 9, 245. [Google Scholar]
- Lobo, V.; Patil, A.; Phatak, A.; Chandra, N. Free radicals, antioxidants and functional foods: Impact on human health. Pharmacogn. Rev. 2010, 4, 118. [Google Scholar] [CrossRef]
- dos Santos, A.L.F.; De Almeida, D.R.Q.; Terra, L.F.; Baptista, M.C.S.; Labriola, L. Photodynamic therapy in cancer treatment—An update review. J. Cancer Metastasis Treat. 2019, 5, 25. [Google Scholar] [CrossRef]
- Myrzakhmetov, B.; Arnoux, P.; Mordon, S.; Acherar, S.; Tsoy, I.; Frochot, C. Photophysical properties of protoporphyrin IX, pyropheophorbide-a, and Photofrin® in different conditions. Pharmaceuticals 2021, 14, 138. [Google Scholar] [CrossRef]
- Allison, R.R.; Bagnato, V.S.; Sibata, C.H. Future of oncologic photodynamic therapy. Future Oncol. 2010, 6, 929–940. [Google Scholar] [CrossRef]
- Razum, N.; Balchum, O.J.; Profio, A.E.; Carstens, F. Skin photosensitivity: Duration and intensity following intravenous hematoporphyrin derivates, HpD and DHE. Photochem. Photobiol. 1987, 46, 925–928. [Google Scholar] [CrossRef]
- Sternberg, E.D.; Dolphin, D. Second generation photodynamic agents: A review. J. Clin. Laser Med. Surg. 1993, 11, 233–241. [Google Scholar] [CrossRef]
- Casas, A.; Batlle, A. Aminolevulinic acid derivatives and liposome delivery as strategies for improving 5-aminolevulinic acid-mediated photodynamic therapy. Curr. Med. Chem. 2006, 13, 1157–1168. [Google Scholar] [CrossRef]
- Khaing Oo, M.K.; Yang, X.; Du, H.; Wang, H. 5-aminolevulinic acid-conjugated gold nanoparticles for photodynamic therapy of cancer. Future Sci. 2008, 3, 777–786. [Google Scholar] [CrossRef]
- Oenbrink, G.; Jurgenlimke, P.; Gabel, D. Accumulation of porphyrins in cells: Influence of hydrophobicity aggregation and protein binding. Photochem. Photobiol. 1988, 48, 451–456. [Google Scholar] [CrossRef]
- Lopez, R.F.V.; Lange, N.; Guy, R.; Bentley, M.V.L.B. Photodynamic therapy of skin cancer: Controlled drug delivery of 5-ALA and its esters. Adv. Drug Deliv. Rev. 2004, 56, 77–94. [Google Scholar] [CrossRef]
- Musiol, R.; Serda, M.; Polanski, J. Prodrugs in photodynamic anticancer therapy. Curr. Pharm. Des. 2011, 17, 3548–3559. [Google Scholar] [CrossRef]
- Wachowska, M.; Muchowicz, A.; Firczuk, M.; Gabrysiak, M.; Winiarska, M.; Wańczyk, M.; Bojarczuk, K.; Golab, J. Aminolevulinic acid (ALA) as a prodrug in photodynamic therapy of cancer. Molecules 2011, 16, 4140–4164. [Google Scholar] [CrossRef]
- Hino, H.; Murayama, Y.; Nakanishi, M.; Inoue, K.; Nakajima, M.; Otsuji, E. 5-Aminolevulinic acid-mediated photodynamic therapy using light-emitting diodes of different wavelengths in a mouse model of peritoneally disseminated gastric cancer. J. Surg. Res. 2013, 185, 119–126. [Google Scholar] [CrossRef]
- Pascale, R.M.; Calvisi, D.F.; Simile, M.M.; Feo, C.F.; Feo, F. The Warburg effect 97 years after its discovery. Cancers 2020, 12, 2819. [Google Scholar] [CrossRef]
- Icard, P.; Shulman, S.; Farhat, D.; Steyaert, J.-M.; Alifano, M.; Lincet, H. How the Warburg effect supports aggressiveness and drug resistance of cancer cells? Drug Resist. Updates 2018, 38, 1–11. [Google Scholar] [CrossRef]
- Shinoda, Y.; Kato, D.; Ando, R.; Endo, H.; Takahashi, T.; Tsuneoka, Y.; Fujiwara, Y. Systematic review and meta-analysis of in vitro anti-human cancer experiments investigating the use of 5-aminolevulinic acid (5-ALA) for photodynamic therapy. Pharmaceuticals 2021, 14, 229. [Google Scholar] [CrossRef] [PubMed]
- Helander, L.; Krokan, H.E.; Johnsson, A.; Gederaas, O.A.; Plaetzer, K. Red versus blue light illumination in hexyl 5-aminolevulinate photodynamic therapy: The influence of light color and irradiance on the treatment outcome in vitro. J. Biomed. Opt. 2014, 19, 088002. [Google Scholar] [CrossRef] [PubMed]
- Hartl, B.A.; Hirschberg, H.; Marcu, L.; Cherry, S.R. Characterizing low fluence thresholds for in vitro photodynamic therapy. Biomed. Opt. Express 2015, 6, 770–779. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Farrell, T.J.; Patterson, M.S. Comparison of photodynamic therapy with different excitation wavelengths using a dynamic model of aminolevulinic acid-photodynamic therapy of human skin. J. Biomed. Opt. 2012, 17, 088001. [Google Scholar] [CrossRef] [PubMed]
- Hartmans, E.; Linssen, M.D.; Sikkens, C.; Levens, A.; Witjes, M.J.; van Dam, G.M.; Nagengast, W.B. Tyrosine kinase inhibitor induced growth factor receptor upregulation enhances the efficacy of near-infrared targeted photodynamic therapy in esophageal adenocarcinoma cell lines. Oncotarget 2017, 8, 29846. [Google Scholar] [CrossRef]
- Algorri, J.F.; Ochoa, M.; Roldán-Varona, P.; Rodríguez-Cobo, L.; López-Higuera, J.M. Photodynamic therapy: A compendium of latest reviews. Cancers 2021, 13, 4447. [Google Scholar] [CrossRef]
- Waarts, M.R.; Stonestrom, A.J.; Park, Y.C.; Levine, R.L. Targeting mutations in cancer. J. Clin. Investig. 2022, 132, e154943. [Google Scholar] [CrossRef]
- Bhagavan, N.; Ha, C.-E. Essentials of Medical Biochemistry with Clinical Cases, 2nd ed.; Academic press: Cambridge, MA, USA, 2015; Chapter 27; pp. 511–529. [Google Scholar]
- Kumari, A. Remembering Structures, Cycles, and Pathways by Mnemonics; Academic Press: London, UK, 2018. [Google Scholar]
- Zorov, D.B.; Juhaszova, M.; Sollott, S.J. Mitochondrial reactive oxygen species (ROS) and ROS-induced ROS release. Physiol. Rev. 2014, 94, 909–950. [Google Scholar] [CrossRef]
- Dickinson, B.C.; Chang, C.J. Chemistry and biology of reactive oxygen species in signaling or stress responses. Nat. Chem. Biol. 2011, 7, 504–511. [Google Scholar] [CrossRef]
- Carmody, R.J.; Cotter, T.G. Signalling apoptosis: A radical approach. Redox Rep. 2001, 6, 77–90. [Google Scholar] [CrossRef]
- Pelicano, H.; Carney, D.; Huang, P. ROS stress in cancer cells and therapeutic implications. Drug Resist. Updates 2004, 7, 97–110. [Google Scholar] [CrossRef]
- Morselli, E.; Galluzzi, L.; Kepp, O.; Vicencio, J.-M.; Criollo, A.; Maiuri, M.C.; Kroemer, G. Anti-and pro-tumor functions of autophagy. Biochim. Biophys. Acta (BBA)-Mol. Cell Res. 2009, 1793, 1524–1532. [Google Scholar] [CrossRef]
- Murphy, M.P. How mitochondria produce reactive oxygen species. Biochem. J. 2009, 417, 1–13. [Google Scholar] [CrossRef]
- Han, D.; Williams, E.; Cadenas, E. Mitochondrial respiratory chain-dependent generation of superoxide anion and its release into the intermembrane space. Biochem. J. 2001, 353, 411–416. [Google Scholar] [CrossRef]
- Fukai, T.; Ushio-Fukai, M. Superoxide dismutases: Role in redox signaling, vascular function, and diseases. Antioxid. Redox Signal. 2011, 15, 1583–1606. [Google Scholar] [CrossRef]
- Bienert, G.P.; Chaumont, F. Aquaporin-facilitated transmembrane diffusion of hydrogen peroxide. Biochim. Et Biophys. Acta (BBA)-Gen. Subj. 2014, 1840, 1596–1604. [Google Scholar] [CrossRef]
- Reczek, C.R.; Chandel, N.S. ROS-dependent signal transduction. Curr. Opin. Cell Biol. 2015, 33, 8–13. [Google Scholar] [CrossRef]
- Bedard, K.; Krause, K.-H. The NOX family of ROS-generating NADPH oxidases: Physiology and pathophysiology. Physiol. Rev. 2007, 87, 245–313. [Google Scholar] [CrossRef]
- Toledano, M.B.; Planson, A.-G.; Delaunay-Moisan, A. Reining in H2O2 for safe signaling. Cell 2010, 140, 454–456. [Google Scholar] [CrossRef]
- Block, K.; Gorin, Y. Aiding and abetting roles of NOX oxidases in cellular transformation. Nat. Rev. Cancer 2012, 12, 627–637. [Google Scholar] [CrossRef]
- Moloney, J.N.; Cotter, T.G. ROS Signalling in the Biology of Cancer. In Seminars in Cell & Developmental Biology; Elsevier: Amsterdam, The Netherlands, 2018; Volume 80, pp. 50–64. [Google Scholar]
- Zou, Z.; Chang, H.; Li, H.; Wang, S. Induction of reactive oxygen species: An emerging approach for cancer therapy. Apoptosis 2017, 22, 1321–1335. [Google Scholar] [CrossRef] [PubMed]
- Lai, H.W.; Sasaki, R.; Usuki, S.; Nakajima, M.; Tanaka, T.; Ogura, S.-I. Novel strategy to increase specificity of ALA-Induced PpIX accumulation through inhibition of transporters involved in ALA uptake. Photodiagnosis Photodyn. Ther. 2019, 27, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.; Thompson, C. The role of the Bcl-2 family in the regulation of outer mitochondrial membrane permeability. Cell Death Differ. 2000, 7, 1182–1191. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, Y.; Hagiya, Y.; Nakajima, M.; Ishizuka, M.; Tanaka, T.; Ogura, S.-I. The heme precursor 5-aminolevulinic acid disrupts the Warburg effect in tumor cells and induces caspase-dependent apoptosis. Oncol. Rep. 2014, 31, 1282–1286. [Google Scholar] [CrossRef] [PubMed]
- Ito, H.; Nishio, Y.; Hara, T.; Sugihara, H.; Tanaka, T.; Li, X.-K. Oral administration of 5-aminolevulinic acid induces heme oxygenase-1 expression in peripheral blood mononuclear cells of healthy human subjects in combination with ferrous iron. Eur. J. Pharmacol. 2018, 833, 25–33. [Google Scholar] [CrossRef]
- Jin, J.-Q.; Wang, Q.; Zhang, Y.-X.; Wang, X.; Lu, Z.-y.; Li, B.-W. Effect of ALA-PDT on inhibition of oral precancerous cell growth and its related mechanisms. Lasers Med. Sci. 2022, 37, 3461–3472. [Google Scholar] [CrossRef]
- Coupienne, I.; Fettweis, G.; Rubio, N.; Agostinis, P.; Piette, J. 5-ALA-PDT induces RIP3-dependent necrosis in glioblastoma. Photochem. Photobiol. Sci. 2011, 10, 1868–1878. [Google Scholar] [CrossRef]
- Ishizuka, M.; Abe, F.; Sano, Y.; Takahashi, K.; Inoue, K.; Nakajima, M.; Kohda, T.; Komatsu, N.; Ogura, S.-I.; Tanaka, T. Novel development of 5-aminolevurinic acid (ALA) in cancer diagnoses and therapy. Int. Immunopharmacol. 2011, 11, 358–365. [Google Scholar] [CrossRef]
- Kitagawa, T.; Yamamoto, J.; Tanaka, T.; Nakano, Y.; Akiba, D.; Ueta, K.; Nishizawa, S. 5-Aminolevulinic acid strongly enhances delayed intracellular production of reactive oxygen species (ROS) generated by ionizing irradiation: Quantitative analyses and visualization of intracellular ROS production in glioma cells in vitro. Oncol. Rep. 2015, 33, 583–590. [Google Scholar] [CrossRef]
- Owari, T.; Tanaka, N.; Nakai, Y.; Miyake, M.; Anai, S.; Kishi, S.; Mori, S.; Fujiwara-Tani, R.; Hojo, Y.; Mori, T. 5-Aminolevulinic acid overcomes hypoxia-induced radiation resistance by enhancing mitochondrial reactive oxygen species production in prostate cancer cells. Br. J. Cancer 2022, 127, 350–363. [Google Scholar] [CrossRef]
- Shishido, Y.; Amisaki, M.; Matsumi, Y.; Yakura, H.; Nakayama, Y.; Miyauchi, W.; Miyatani, K.; Matsunaga, T.; Hanaki, T.; Kihara, K. Antitumor effect of 5-aminolevulinic acid through ferroptosis in esophageal squamous cell carcinoma. Ann. Surg. Oncol. 2021, 28, 3996–4006. [Google Scholar] [CrossRef]
- Kim, C.H.; Chung, C.-W.; Choi, K.H.; Yoo, J.-J.; Kim, D.H.; Jeong, Y.-I.; Kang, D.H. Effect of 5-aminolevulinic acid-based photodynamic therapy via reactive oxygen species in human cholangiocarcinoma cells. Int. J. Nanomed. 2011, 6, 1357–1363. [Google Scholar]
- Suprihadi, A.; Pustimbara, A.; Ogura, S.-I. 5-aminolevulinic acid and sodium ferrous citrate decreased cell viability of gastric cancer cells by enhanced ROS generation through improving COX activity. Photodiagnosis Photodyn. Ther. 2022, 40, 103055. [Google Scholar] [CrossRef]
- Kawczyk-Krupka, A.; Latos, W.; Oleś, P.; Czuba, Z.P.; Latos, M.; Krupka, M.; Pengyun, H.; Xu, C.; Cieślar, G.; Sieroń, A. The influence of 5-aminolevulinic photodynamic therapy on colon cancer cell interleukin secretion in hypoxia-like condition in vitro. Photodiagnosis Photodyn. Ther. 2018, 23, 240–243. [Google Scholar] [CrossRef]
- Wang, C.; Chen, X.; Wu, J.; Liu, H.; Ji, Z.; Shi, H.; Gao, C.; Han, D.; Wang, L.; Liu, Y. Low-dose arsenic trioxide enhances 5-aminolevulinic acid-induced PpIX accumulation and efficacy of photodynamic therapy in human glioma. J. Photochem. Photobiol. B Biol. 2013, 127, 61–67. [Google Scholar] [CrossRef]
- Abo-Zeid, M.A.; Abo-Elfadl, M.T.; Mostafa, S.M. Photodynamic therapy using 5-aminolevulinic acid triggered DNA damage of adenocarcinoma breast cancer and hepatocellular carcinoma cell lines. Photodiagnosis Photodyn. Ther. 2018, 21, 351–356. [Google Scholar] [CrossRef]
- Tsai, T.; Hong, R.L.; Tsai, J.C.; Lou, P.J.; Ling, I.F.; Chen, C.T. Effect of 5-aminolevulinic acid-mediated photodynamic therapy on MCF-7 and MCF-7/ADR cells. Lasers Surg. Med. Off. J. Am. Soc. Laser Med. Surg. 2004, 34, 62–72. [Google Scholar] [CrossRef]
- Kamanlı, A.F.; Yıldız, M.Z.; Özyol, E.; Deveci Ozkan, A.; Sozen Kucukkara, E.; Guney Eskiler, G. Investigation of LED-based photodynamic therapy efficiency on breast cancer cells. Lasers Med. Sci. 2021, 36, 563–569. [Google Scholar] [CrossRef]
- Szliszka, E.; Kawczyk-Krupka, A.; Czuba, Z.P.; Sieron, A.; Krol, W. Effect of ALA–mediated photodynamic therapy in combination with tumor necrosis factor–related apoptosis–inducing ligand (TRAIL) on bladder cancer cells. Cent. Eur. J. Urol. 2011, 64, 175. [Google Scholar] [CrossRef]
- Zhang, X.; Cai, L.; He, J.; Li, X.; Li, L.; Chen, X.; Lan, P. Influence and mechanism of 5-aminolevulinic acid-photodynamic therapy on the metastasis of esophageal carcinoma. Photodiagnosis Photodyn. Ther. 2017, 20, 78–85. [Google Scholar] [CrossRef]
- Wang, X.; Yuan, Z.; Tao, A.; Wang, P.; Xie, W.; Yang, S.; Huang, J.; Wen, N. Hydrogel-based patient-friendly photodynamic therapy of oral potentially malignant disorders. Biomaterials 2022, 281, 121377. [Google Scholar] [CrossRef] [PubMed]
- Chi, Y.-F.; Qin, J.-J.; Li, Z.; Ge, Q.; Zeng, W.-H. Enhanced anti-tumor efficacy of 5-aminolevulinic acid-gold nanoparticles-mediated photodynamic therapy in cutaneous squamous cell carcinoma cells. Braz. J. Med. Biol. Res. 2020, 53, e8457. [Google Scholar] [CrossRef] [PubMed]
- Naidoo, C.; Kruger, C.A.; Abrahamse, H. Targeted photodynamic therapy treatment of in vitro A375 metastatic melanoma cells. Oncotarget 2019, 10, 6079. [Google Scholar] [CrossRef] [PubMed]
- Grosjean, P.; Savary, J.-F.; Mizeret, J.; Wagnieres, G.; Woodtli, A.; Theumann, J.-F.; Fontolliet, C.; Van den Bergh, H.; Monnier, P. Photodynamic therapy for cancer of the upper aerodigestive tract using tetra (m-hydroxyphenyl) chlorin. J. Clin. Laser Med. Surg. 1996, 14, 281–287. [Google Scholar] [CrossRef]
- Hamblin, M.R. Photodynamic therapy for cancer: What’s past is prologue. Photochem. Photobiol. 2020, 96, 506–516. [Google Scholar] [CrossRef]
- Tanaka, Y.; Murayama, Y.; Matsumoto, T.; Kubo, H.; Harada, K.; Matsuo, H.; Kubota, T.; Okamoto, K.; Otsuji, E. Efficacy of 5-aminolevulinic acid-mediated photodynamic therapy in a mouse model of esophageal cancer. Oncol. Lett. 2020, 20, 82. [Google Scholar] [CrossRef]
- Kohoutova, D.; Haidry, R.; Banks, M.; Butt, M.A.; Dunn, J.; Thorpe, S.; Lovat, L. Long-term outcomes of the randomized controlled trial comparing 5-aminolaevulinic acid and Photofrin photodynamic therapy for Barrett’s oesophagus related neoplasia. Scand. J. Gastroenterol. 2018, 53, 527–532. [Google Scholar] [CrossRef]
- Namikawa, T.; Yatabe, T.; Inoue, K.; Shuin, T.; Hanazaki, K. Clinical applications of 5-aminolevulinic acid-mediated fluorescence for gastric cancer. World J. Gastroenterol. WJG 2015, 21, 8769. [Google Scholar] [CrossRef]
- Kishi, K.; Fujiwara, Y.; Yano, M.; Inoue, M.; Miyashiro, I.; Motoori, M.; Shingai, T.; Gotoh, K.; Takahashi, H.; Noura, S. Staging laparoscopy using ALA-mediated photodynamic diagnosis improves the detection of peritoneal metastases in advanced gastric cancer. J. Surg. Oncol. 2012, 106, 294–298. [Google Scholar] [CrossRef]
- Biel, M.A. Photodynamic therapy of head and neck cancers. Photodyn. Ther. Methods Protoc. 2010, 635, 281–293. [Google Scholar]
- Ahn, P.H.; Finlay, J.C.; Gallagher-Colombo, S.M.; Quon, H.; O’Malley, B.W., Jr.; Weinstein, G.S.; Chalian, A.; Malloy, K.; Sollecito, T.; Greenberg, M. Lesion oxygenation associates with clinical outcomes in premalignant and early stage head and neck tumors treated on a phase 1 trial of photodynamic therapy. Photodiagnosis Photodyn. Ther. 2018, 21, 28–35. [Google Scholar] [CrossRef]
- Ahn, P.H.; Quon, H.; O’Malley, B.W.; Weinstein, G.; Chalian, A.; Malloy, K.; Atkins, J.H.; Sollecito, T.; Greenberg, M.; McNulty, S. Toxicities and early outcomes in a phase 1 trial of photodynamic therapy for premalignant and early stage head and neck tumors. Oral Oncol. 2016, 55, 37–42. [Google Scholar] [CrossRef]
- Ogasawara, T.; Miyoshi, N.; Sano, K.; Kitagawa, Y.; Yamada, T.; Ogawa, T.; Miyauchi, K.; Kinoshita, H. Influence of administration methods on the accumulation of ALA-induced Pp-IX in mouse tongue tumors. Oral Dis. 2006, 12, 415–419. [Google Scholar] [CrossRef]
- Banerjee, S.M.; El-Sheikh, S.; Malhotra, A.; Mosse, C.A.; Parker, S.; Williams, N.R.; MacRobert, A.J.; Hamoudi, R.; Bown, S.G.; Keshtgar, M.R.S. Photodynamic Therapy in Primary Breast Cancer. J. Clin. Med. 2020, 9, 483. [Google Scholar] [CrossRef]
- Mahmoudi, K.; Garvey, K.; Bouras, A.; Cramer, G.; Stepp, H.; Jesu Raj, J.; Bozec, D.; Busch, T.; Hadjipanayis, C. 5-aminolevulinic acid photodynamic therapy for the treatment of high-grade gliomas. J. Neuro-Oncol. 2019, 141, 595–607. [Google Scholar] [CrossRef]
- Madsen, S.J.; Sun, C.H.; Tromberg, B.J.; Hirschberg, H. Development of a novel indwelling balloon applicator for optimizing light delivery in photodynamic therapy. Lasers Surg. Med. Off. J. Am. Soc. Laser Med. Surg. 2001, 29, 406–412. [Google Scholar] [CrossRef]
- Tetard, M.-C.; Vermandel, M.; Leroy, H.-A.; Leroux, B.; Maurage, C.-A.; Lejeune, J.-P.; Mordon, S.; Reyns, N. Interstitial 5-ALA photodynamic therapy and glioblastoma: Preclinical model development and preliminary results. Photodiagnosis Photodyn. Ther. 2016, 13, 218–224. [Google Scholar] [CrossRef]
- Widhalm, G.; Minchev, G.; Woehrer, A.; Preusser, M.; Kiesel, B.; Furtner, J.; Mert, A.; Di Ieva, A.; Tomanek, B.; Prayer, D. Strong 5-aminolevulinic acid-induced fluorescence is a novel intraoperative marker for representative tissue samples in stereotactic brain tumor biopsies. Neurosurg. Rev. 2012, 35, 381–391. [Google Scholar] [CrossRef]
- Eljamel, M.S.; Goodman, C.; Moseley, H. ALA and Photofrin® Fluorescence-guided resection and repetitive PDT in glioblastoma multiforme: A single centre Phase III randomised controlled trial. Lasers Med. Sci. 2008, 23, 361–367. [Google Scholar] [CrossRef]
- Stylli, S.S.; Kaye, A.H.; MacGregor, L.; Howes, M.; Rajendra, P. Photodynamic therapy of high grade glioma–long term survival. J. Clin. Neurosci. 2005, 12, 389–398. [Google Scholar] [CrossRef]
- Krishnamurthy, S.; Powers, S.K.; Witmer, P.; Brown, T. Optimal light dose for interstitial photodynamic therapy in treatment for malignant brain tumors. Lasers Surg. Med. Off. J. Am. Soc. Laser Med. Surg. 2000, 27, 224–234. [Google Scholar] [CrossRef]
- Stepp, H.; Stummer, W. 5-ALA in the management of malignant glioma. Lasers Surg. Med. 2018, 50, 399–419. [Google Scholar] [CrossRef] [PubMed]
- Daayana, S.; Winters, U.; Stern, P.L.; Kitchener, H.C. Clinical and immunological response to photodynamic therapy in the treatment of vulval intraepithelial neoplasia. Photochem. Photobiol. Sci. 2011, 10, 802–809. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.; Snell, M.; Berenbaum, M. Photodynamic destruction of human bladder carcinoma. Br. J. Cancer 1975, 31, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Filonenko, E.; Kaprin, A.; Alekseev, B.; Apolikhin, O.; Slovokhodov, E.; Ivanova-Radkevich, V.; Urlova, A. 5-Aminolevulinic acid in intraoperative photodynamic therapy of bladder cancer (results of multicenter trial). Photodiagnosis Photodyn. Ther. 2016, 16, 106–109. [Google Scholar] [CrossRef]
- Panetta, J.V.; Cvetkovic, D.; Chen, X.; Chen, L.; Ma, C.C. Radiodynamic therapy using 15-MV radiation combined with 5-aminolevulinic acid and carbamide peroxide for prostate cancer in vivo. Phys. Med. Biol. 2020, 65, 165008. [Google Scholar] [CrossRef]
- Tschen, E.; Wong, D.; Pariser, D.; Dunlap, F.; Houlihan, A.; Ferdon, M.; Phase IV ALA-PDT Actinic Keratosis Study Group. Photodynamic therapy using aminolaevulinic acid for patients with nonhyperkeratotic actinic keratoses of the face and scalp: Phase IV multicentre clinical trial with 12-month follow up. Br. J. Dermatol. 2006, 155, 1262–1269. [Google Scholar] [CrossRef]
- Piacquadio, D.J.; Chen, D.M.; Farber, H.F.; Fowler, J.F., Jr.; Glazer, S.D.; Goodman, J.J.; Hruza, L.L.; Jeffes, E.W.; Ling, M.R.; Phillips, T.J. Photodynamic Therapy With Aminolevulinic Acid Topical Solution andVisible Blue Light in the Treatment of Multiple Actinic Keratoses of the Faceand Scalp: Investigator-Blinded, Phase 3, Multicenter Trials. Arch. Dermatol. 2004, 140, 41–46. [Google Scholar] [CrossRef]
- Hua, H.; Cheng, J.-W.; Bu, W.-B.; Liu, J.; Ma, W.-W.; Ni, N.; Shi, J.; Zhou, B.-R.; Luo, D. 5-aminolaevulinic acid-based photodynamic therapy inhibits ultraviolet B-induced skin photodamage. Int. J. Biol. Sci. 2019, 15, 2100. [Google Scholar] [CrossRef]
- Yang, X.; Palasuberniam, P.; Kraus, D.; Chen, B. Aminolevulinic acid-based tumor detection and therapy: Molecular mechanisms and strategies for enhancement. Int. J. Mol. Sci. 2015, 16, 25865–25880. [Google Scholar] [CrossRef]
- Kennedy, J.; Pottier, R.; Pross, D. Photodynamic therapy with endogenous protoporphyrin: IX: Basic principles and present clinical experience. J. Photochem. Photobiol. B Biol. 1990, 6, 143–148. [Google Scholar] [CrossRef]
- Peng, Q.; Warloe, T.; Berg, K.; Moan, J.; Kongshaug, M.; Giercksky, K.E.; Nesland, J.M. 5-Aminolevulinic acid-based photodynamic therapy: Clinical research and future challenges. Cancer 1997, 79, 2282–2308. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pignatelli, P.; Umme, S.; D’Antonio, D.L.; Piattelli, A.; Curia, M.C. Reactive Oxygen Species Produced by 5-Aminolevulinic Acid Photodynamic Therapy in the Treatment of Cancer. Int. J. Mol. Sci. 2023, 24, 8964. https://doi.org/10.3390/ijms24108964
Pignatelli P, Umme S, D’Antonio DL, Piattelli A, Curia MC. Reactive Oxygen Species Produced by 5-Aminolevulinic Acid Photodynamic Therapy in the Treatment of Cancer. International Journal of Molecular Sciences. 2023; 24(10):8964. https://doi.org/10.3390/ijms24108964
Chicago/Turabian StylePignatelli, Pamela, Samia Umme, Domenica Lucia D’Antonio, Adriano Piattelli, and Maria Cristina Curia. 2023. "Reactive Oxygen Species Produced by 5-Aminolevulinic Acid Photodynamic Therapy in the Treatment of Cancer" International Journal of Molecular Sciences 24, no. 10: 8964. https://doi.org/10.3390/ijms24108964