
Advances in the Pathogenesis and Treatment of Resistant Hypertension
 , , , , ,
, , , , ,
Abstract
:1. Introduction
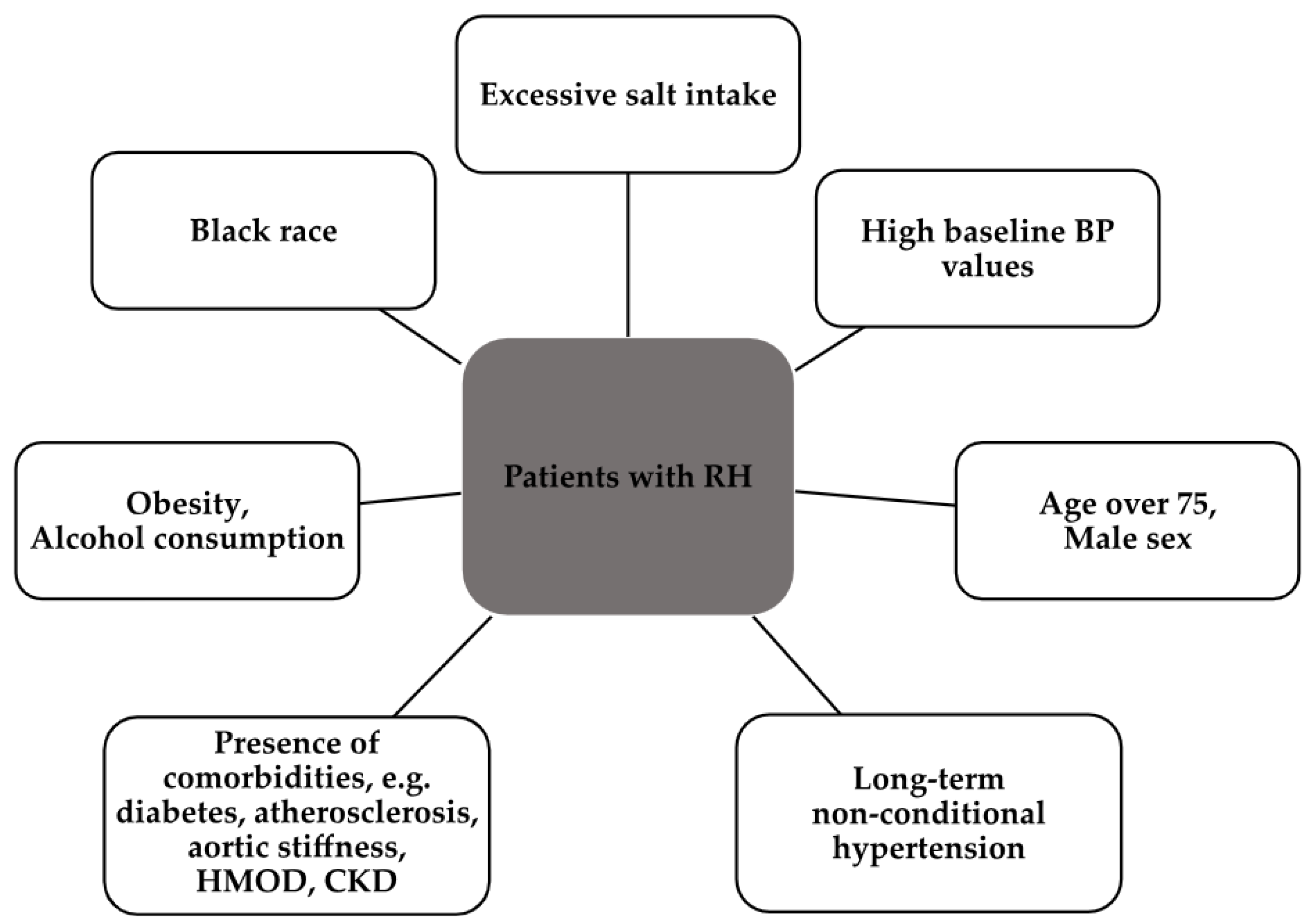
2. Epidemiology
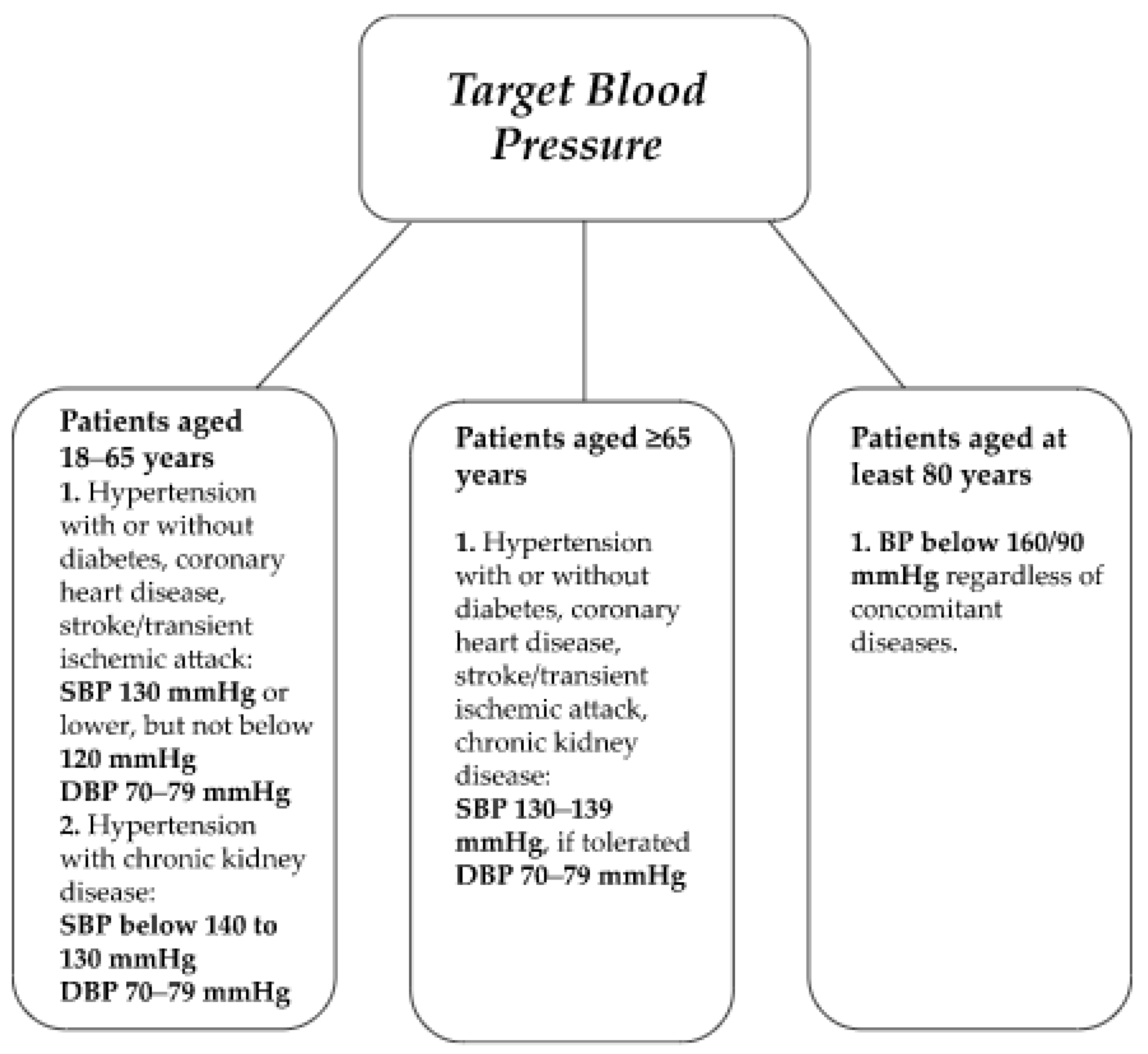
3. Target Blood Pressure Values
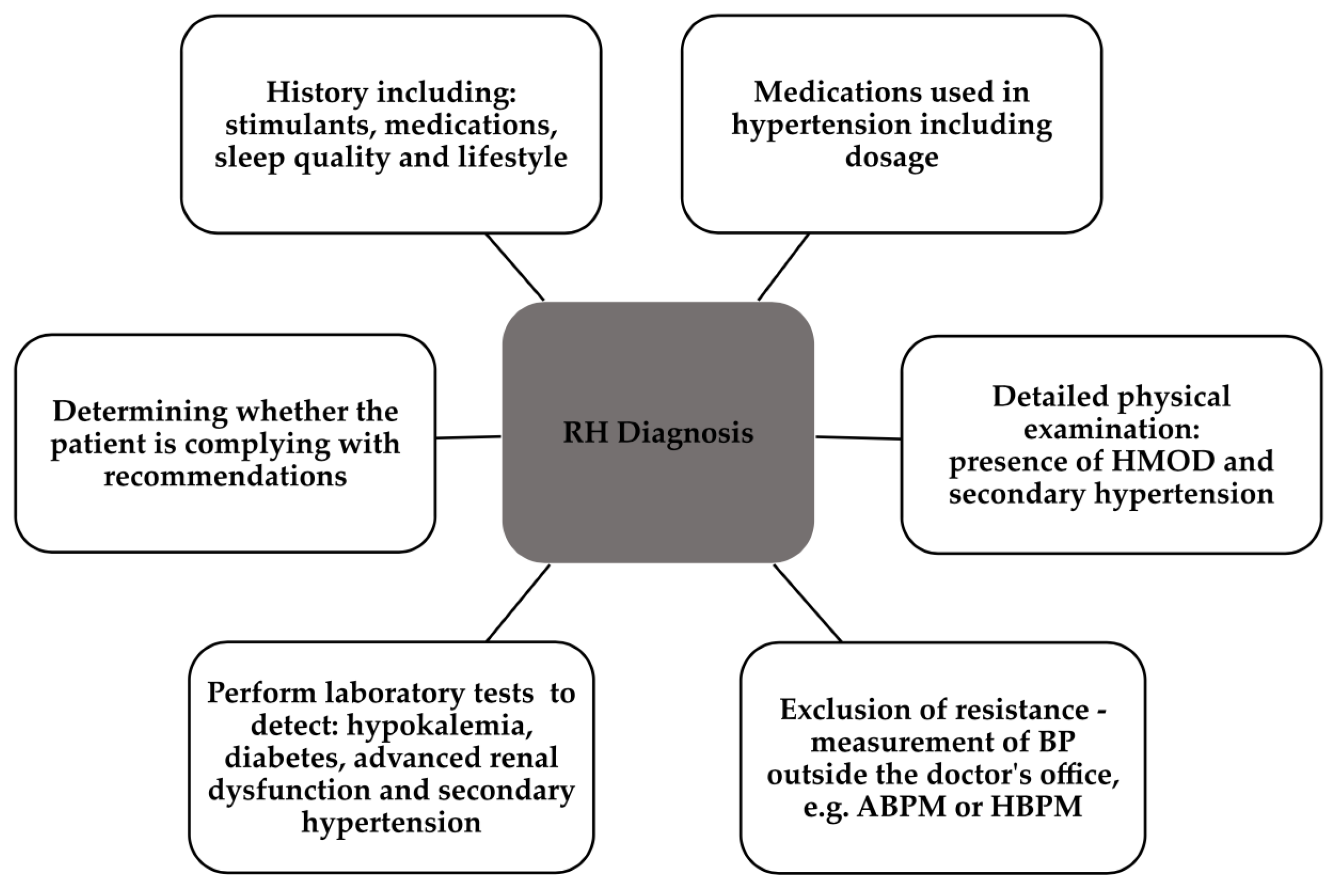
4. Diagnostics of RH
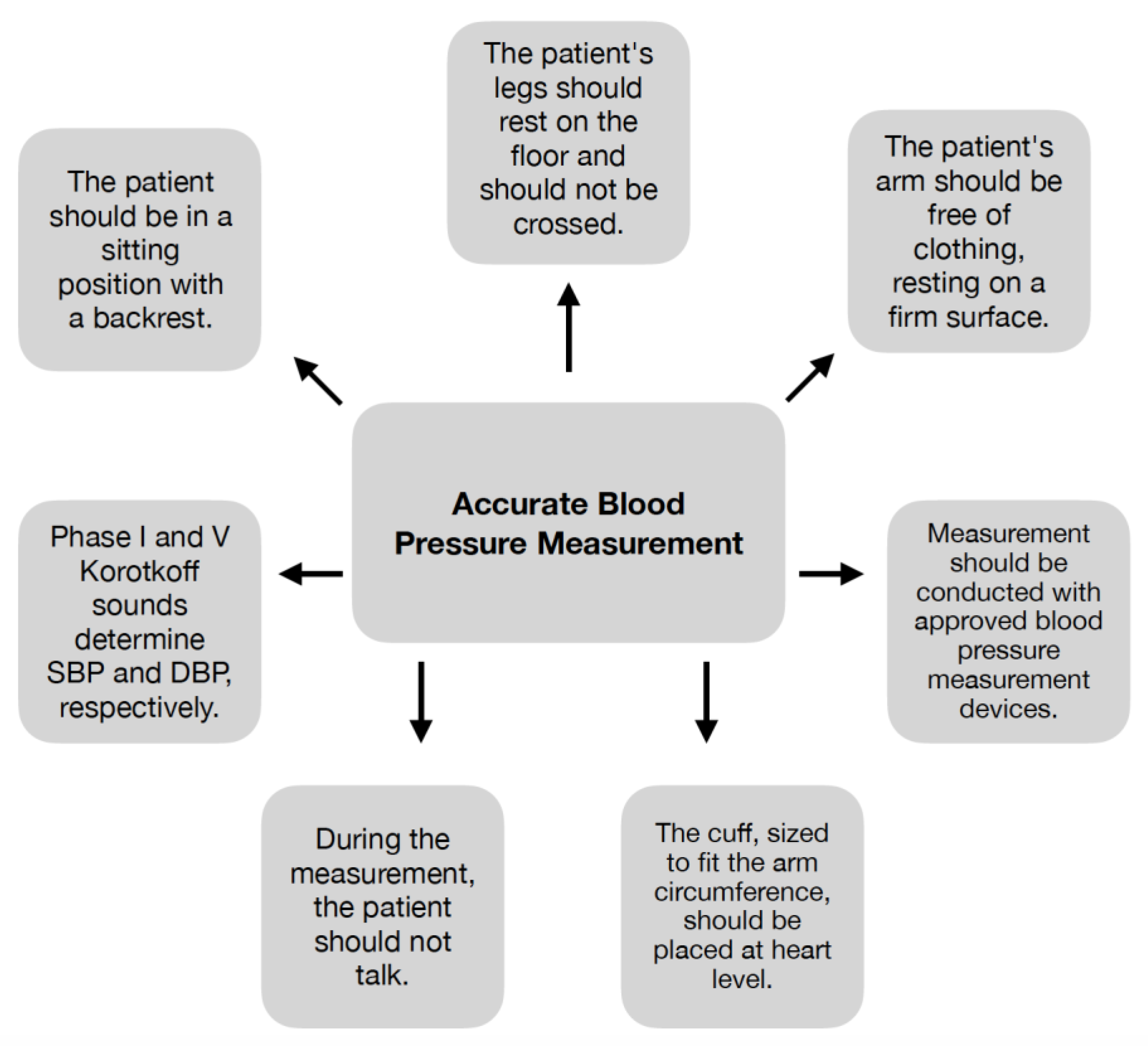
4.1. Accurate Blood Pressure Measurement
4.2. Secondary Hypertension Screening
4.3. Drug Adherence Estimation
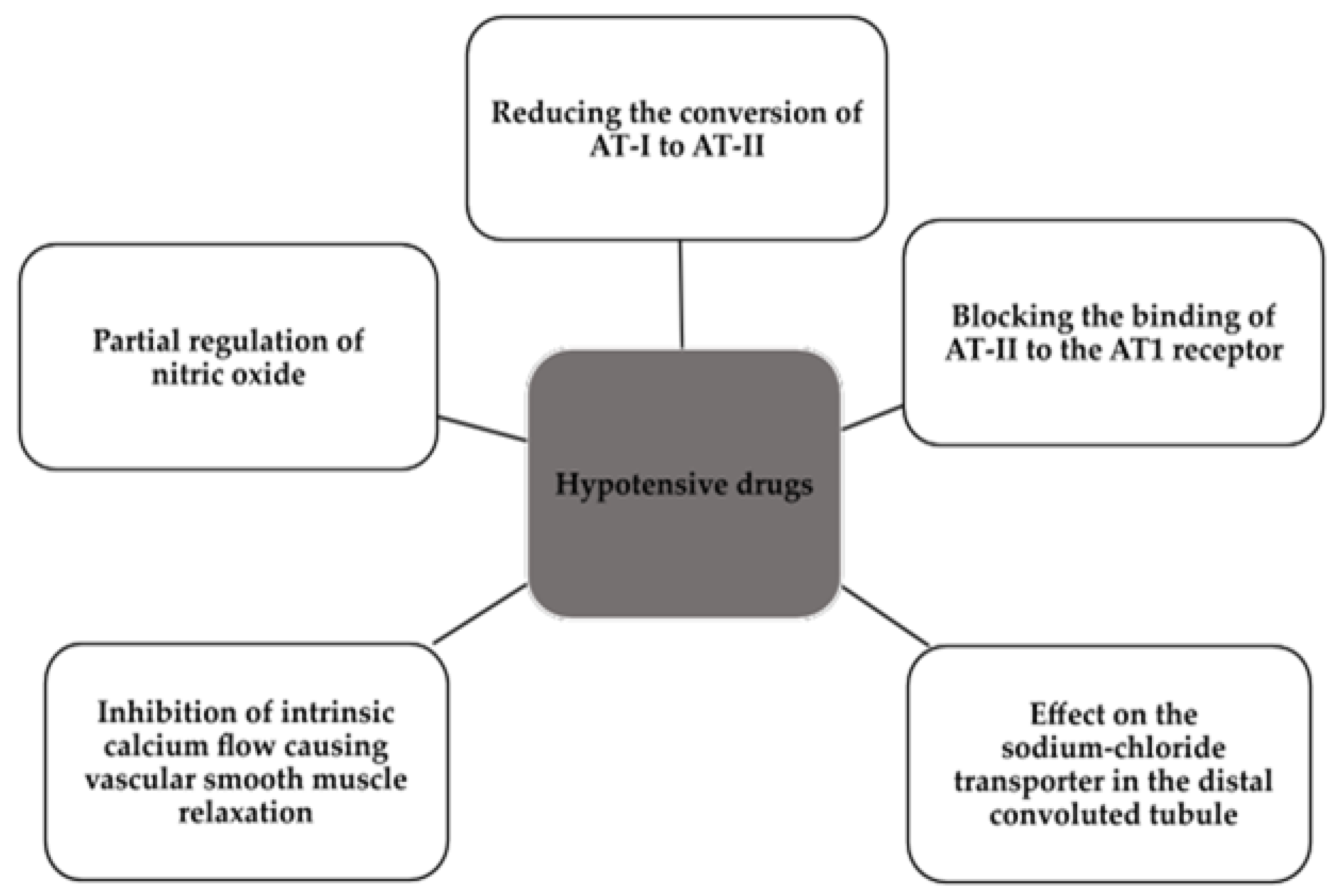
5. Pharmacological Treatment
- A blocker of the RAA system, with special emphasis on angiotensin-converting enzyme inhibitors (ACEis) and angiotensin receptor blockers (ARBs);
- A long-acting calcium channel blocker (CCB), most commonly amlodipine;
- A long-acting thiazide diuretic, i.e., indapamide or chlorthalidone.
6. Nonpharmacological Treatment
6.1. Renal Denervation
6.2. Carotid Baroreceptor Stimulation
6.3. Arteriovenous Fistula
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lamirault, G.; Artifoni, M.; Daniel, M.; Barber-Chamoux, N.; Nantes University Hospital Working Group On Hypertension. Resistant Hypertension: Novel Insights. Curr. Hypertens. Rev. 2020, 16, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Sarwar, M.S.; Islam, M.S.; Al Baker, S.M.; Hasnat, A. Resistant hypertension: Underlying causes and treatment. Drug Res. 2013, 63, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.M. Epidemiology, prognosis, and treatment of resistant hypertension. Pharmacotherapy 2013, 33, 1071–1086. [Google Scholar] [CrossRef] [PubMed]
- Acelajado, M.C.; Hughes, Z.H.; Oparil, S.; Calhoun, D.A. Treatment of Resistant and Refractory Hypertension. Circ. Res. 2019, 124, 1061–1070. [Google Scholar] [CrossRef] [PubMed]
- Judd, E.; Calhoun, D.A. Apparent and true resistant hypertension: Definition, prevalence and outcomes. J. Hum. Hypertens. 2014, 28, 463–468. [Google Scholar] [CrossRef]
- Ozemek, C.; Tiwari, S.; Sabbahi, A.; Carbone, S.; Lavie, C.J. Impact of therapeutic lifestyle changes in resistant hypertension. Prog. Cardiovasc. Dis. 2020, 63, 4–9. [Google Scholar] [CrossRef]
- Egan, B.M. Treatment Resistant Hypertension. Ethn. Dis. 2015, 25, 495–498. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104, Erratum in: Eur. Heart J. 2019, 40, 475. [Google Scholar] [CrossRef]
- Moreno, H. Pseudo and resistant hypertension: A chaotic perspective. J. Clin. Hypertens. 2022, 24, 698–703. [Google Scholar] [CrossRef]
- Doroszko, A.; Janus, A.; Szahidewicz-Krupska, E.; Mazur, G.; Derkacz, A. Resistant Hypertension. Adv. Clin. Exp. Med. 2016, 25, 173–183. [Google Scholar] [CrossRef]
- Nagarajan, N.; Jalal, D. Resistant Hypertension: Diagnosis and Management. Adv. Chronic. Kidney Dis. 2019, 26, 99–109. [Google Scholar] [CrossRef]
- Sarganas, G.; Neuhauser, H.K. Untreated, Uncontrolled, and Apparent Resistant Hypertension: Results of the German Health Examination Survey 2008–2011. J. Clin. Hypertens. 2016, 18, 1146–1154. [Google Scholar] [CrossRef] [PubMed]
- de la Sierra, A.; Segura, J.; Banegas, J.R.; Gorostidi, M.; de la Cruz, J.J.; Armario, P.; Oliveras, A.; Ruilope, L.M. Clinical features of 8295 patients with resistant hypertension classified on the basis of ambulatory blood pressure monitoring. Hypertension 2011, 57, 898–902. [Google Scholar] [CrossRef] [PubMed]
- Achelrod, D.; Wenzel, U.; Frey, S. Systematic review and meta-analysis of the prevalence of resistant hypertension in treated hypertensive populations. Am. J. Hypertens. 2015, 28, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Noubiap, J.J.; Nansseu, J.R.; Nyaga, U.F.; Sime, P.S.; Francis, I.; Bigna, J.J. Global prevalence of resistant hypertension: A meta-analysis of data from 3.2 million patients. Heart 2019, 105, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Tykarski, A.; Widecka, K.; Narkiewicz, K. Zasady postępowania w nadciśnieniu tętniczym—2019 rok Wytyczne Polskiego Towarzystwa Nadciśnienia Tętniczego. Próba komentarza na temat zmian i ich zasadności. Nadciśnienie Tętnicze w Praktyce 2019, 5, 99–152. [Google Scholar]
- Prejbisz, A.; Klocek, M.; Gąsowski, J.; Topór-Mądry, R.; Leśniak, W.; Kabat, M.; Czarnecka, D.; Kawecka-Jaszcz, K.; Narkiewicz, K.; Januszewicz, A. Factors associated with resistant hypertension in a large cohort of hypertensive patients: The Pol-Fokus study. Pol. Arch. Med. Wewn. 2015, 125, 249–259. [Google Scholar] [CrossRef]
- Gupta, A.K.; Nasothimiou, E.G.; Chang, C.L.; Sever, P.S.; Dahlöf, B.; Poulter, N.R.; ASCOT Investigators. Baseline predictors of resistant hypertension in the Anglo-Scandinavian Cardiac Outcome Trial (ASCOT): A risk score to identify those at high-risk. J. Hypertens. 2011, 29, 2004–2013. [Google Scholar] [CrossRef]
- Kim, H.M.; Shin, J. Role of home blood pressure monitoring in resistant hypertension. Clin. Hypertens. 2023, 29, 2. [Google Scholar] [CrossRef]
- Sudano, I.; Osto, E.; Ruschitzka, F. Blood Pressure-Lowering Therapy. In Prevention and Treatment of Atherosclerosis: Improving State-of-the-Art Management and Search for Novel Targets; von Eckardstein, A., Binder, C.J., Eds.; Springer: Cham, Switzerland, 2022. [Google Scholar]
- Singh, J.N.; Nguyen, T.; Kerndt, C.C.; Dhamoon, A.S. Physiology, Blood Pressure Age Related Changes. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- National Guideline Centre (UK). Evidence Review for Blood Pressure Targets: Hypertension in Adults (Update): Evidence Review J; National Institute for Health and Care Excellence (NICE): London, UK, 2022. [Google Scholar]
- Iqbal, A.M.; Jamal, S.F. Essential Hypertension. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Shalaeva, E.V.; Messerli, F.H. What is resistant arterial hypertension? Blood Press. 2023, 32, 2185457. [Google Scholar] [CrossRef]
- Beger, C.; Mayerböck, A.; Klein, K.; Karg, T.; Schmidt-Ott, K.M.; Randerath, O.; Limbourg, F.P. Current practice of blood pressure measurement in Germany: A nationwide questionnaire-based survey in medical practices. Blood Press. 2023, 32, 2165901. [Google Scholar] [CrossRef]
- Jordan, J.; Kurschat, C.; Reuter, H. Arterial Hypertension. Dtsch. Arztebl. Int. 2018, 115, 557–568. [Google Scholar] [CrossRef]
- Flack, J.M.; Adekola, B. Blood pressure and the new ACC/AHA hypertension guidelines. Trends Cardiovasc. Med. 2020, 30, 160–164. [Google Scholar] [CrossRef]
- Irving, G.; Holden, J.; Stevens, R.; McManus, R.J. Which cuff should I use? Indirect blood pressure measurement for the diagnosis of hypertension in patients with obesity: A diagnostic accuracy review. BMJ Open 2016, 6, e012429. [Google Scholar] [CrossRef]
- Mostafa, M.M.A.; Hasanin, A.M.; Alhamade, F.; Abdelhamid, B.; Safina, A.G.; Kasem, S.M.; Hosny, O.; Mahmoud, M.; Fouad, E.; Rady, A.; et al. Accuracy and trending of non-invasive oscillometric blood pressure monitoring at the wrist in obese patients. Anaesth. Crit. Care Pain. Med. 2020, 39, 221–227. [Google Scholar] [CrossRef]
- Zweiker, R.; Schumacher, M.; Fruhwald, F.M.; Watzinger, N.; Klein, W. Comparison of wrist blood pressure measurement with conventional sphygmomanometry at a cardiology outpatient clinic. J. Hypertens. 2000, 18, 1013–1018. [Google Scholar] [CrossRef]
- Pioli, M.R.; Ritter, A.M.; de Faria, A.P.; Modolo, R. White coat syndrome and its variations: Differences and clinical impact. Integr. Blood Press. Control. 2018, 11, 73–79. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, e13–e115, Erratum in: Hypertension 2018, 71, e140–e144. [Google Scholar]
- Muxfeldt, E.S.; Margallo, V.S.; Guimarães, G.M.; Salles, G.F. Prevalence and associated factors of obstructive sleep apnea in patients with resistant hypertension. Am. J. Hypertens. 2014, 27, 1069–1078. [Google Scholar] [CrossRef]
- Lloberes, P.; Lozano, L.; Sampol, G.; Romero, O.; Jurado, M.J.; Ríos, J.; Untoria, M.D.; Tovar, J.L. Obstructive sleep apnoea and 24-h blood pressure in patients with resistant hypertension. J. Sleep Res. 2010, 19, 597–602. [Google Scholar] [CrossRef]
- Sarathy, H.; Salman, L.A.; Lee, C.; Cohen, J.B. Evaluation and Management of Secondary Hypertension. Med. Clin. N. Am. 2022, 106, 269–283. [Google Scholar] [CrossRef]
- Bioletto, F.; Bollati, M.; Lopez, C.; Arata, S.; Procopio, M.; Ponzetto, F.; Ghigo, E.; Maccario, M.; Parasiliti-Caprino, M. Primary Aldosteronism and Resistant Hypertension: A Pathophysiological Insight. Int. J. Mol. Sci. 2022, 23, 4803. [Google Scholar] [CrossRef]
- Florczak, E.; Prejbisz, A.; Szwench-Pietrasz, E.; Sliwiński, P.; Bieleń, P.; Klisiewicz, A.; Michałowska, I.; Warchoł, E.; Januszewicz, M.; Kała, M.; et al. Clinical characteristics of patients with resistant hypertension: The RESIST-POL study. J. Hum. Hypertens. 2013, 27, 678–685. [Google Scholar] [CrossRef]
- Kario, K.; Kai, H.; Nanto, S.; Yokoi, H. Anti-hypertensive medication adherence in the REQUIRE trial: Post-hoc exploratory evaluation. Hypertens. Res. 2023, 46, 2044–2047. [Google Scholar] [CrossRef]
- Bourque, G.; Ilin, J.V.; Ruzicka, M.; Hundemer, G.L.; Shorr, R.; Hiremath, S. Non-Adherence is Common in Patients with Apparent Resistant Hypertension: A Systematic Review and Meta-Analysis. Am. J. Hypertens. 2023, 36, hpad013. [Google Scholar] [CrossRef]
- Lee, E.K.P.; Poon, P.; Yip, B.H.K.; Bo, Y.; Zhu, M.T.; Yu, C.P.; Ngai, A.C.H.; Wong, M.C.S.; Wong, S.Y.S. Global Burden, Regional Differences, Trends, and Health Consequences of Medication Nonadherence for Hypertension During 2010 to 2020: A Meta-Analysis Involving 27 Million Patients. J. Am. Heart Assoc. 2022, 11, e026582. [Google Scholar] [CrossRef]
- Feng, Y.; Zhao, Y.; Yang, X.; Li, Y.; Han, M.; Qie, R.; Huang, S.; Wu, X.; Zhang, Y.; Wu, Y.; et al. Adherence to antihypertensive medication and cardiovascular disease events in hypertensive patients: A dose-response meta-analysis of 2,769,700 participants in cohort study. QJM 2022, 115, 279–286. [Google Scholar] [CrossRef]
- Mai, A.; Voigt, K.; Schübel, J.; Gräßer, F. A drug recommender system for the treatment of hypertension. BMC Med. Inform. Decis Mak. 2023, 23, 89. [Google Scholar] [CrossRef]
- Kassavou, A.; Wang, M.; Mirzaei, V.; Shpendi, S.; Hasan, R. The Association Between Smartphone App-Based Self-monitoring of Hypertension-Related Behaviors and Reductions in High Blood Pressure: Systematic Review and Meta-analysis. JMIR Mhealth Uhealth. 2022, 10, e34767. [Google Scholar] [CrossRef]
- Ruilope, L.M.; Rodríguez-Sánchez, E.; Navarro-García, J.A.; Segura, J.; Órtiz, A.; Lucia, A.; Ruiz-Hurtado, G. Resistant hypertension: New insights and therapeutic perspectives. Eur. Heart J. Cardiovasc. Pharmacother. 2020, 6, 188–193. [Google Scholar] [CrossRef]
- Weldon, S.M.; Brown, N.F. Inhibitors of Aldosterone Synthase. Vitam. Horm. 2019, 109, 211–239. [Google Scholar] [CrossRef] [PubMed]
- Goyal, A.; Cusick, A.S.; Thielemier, B. ACE Inhibitors. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Burnier, M.; Bakris, G.; Williams, B. Redefining diuretics use in hypertension: Why select a thiazide-like diuretic? J. Hypertens. 2019, 37, 1574–1586. [Google Scholar] [CrossRef] [PubMed]
- Elliott, W.J.; Ram, C.V. Calcium channel blockers. J. Clin. Hypertens. 2011, 13, 687–689. [Google Scholar] [CrossRef]
- Agarwal, R.; Sinha, A.D.; Cramer, A.E.; Balmes-Fenwick, M.; Dickinson, J.H.; Ouyang, F.; Tu, W. Chlorthalidone for Hypertension in Advanced Chronic Kidney Disease. N. Engl. J. Med. 2021, 385, 2507–2519. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.M.; Seemer, J.; Knudsen, A.W.; Munk, T. Narrative Review of Low-Intake Dehydration in Older Adults. Nutrients 2021, 13, 3142. [Google Scholar] [CrossRef]
- Dani, M.; Dirksen, A.; Taraborrelli, P.; Panagopolous, D.; Torocastro, M.; Sutton, R.; Lim, P.B. Orthostatic hypotension in older people: Considerations, diagnosis and management. Clin. Med. 2021, 21, e275–e282. [Google Scholar] [CrossRef]
- Schlaich, M.P.; Sobotka, P.A.; Krum, H.; Lambert, E.; Esler, M.D. Renal sympathetic-nerve ablation for uncontrolled hypertension. N. Engl. J. Med. 2009, 361, 932–934. [Google Scholar] [CrossRef]
- Esler, M.D.; Krum, H.; Schlaich, M.; Schmieder, R.E.; Böhm, M.; Sobotka, P.A.; Symplicity HTN-2 Investigators. Renal sympathetic denervation for treatment of drug-resistant hypertension: One-year results from the Symplicity HTN-2 randomized, controlled trial. Circulation 2012, 126, 2976–2982. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Kandzari, D.E.; O’Neill, W.W.; D’Agostino, R.; Flack, J.M.; Katzen, B.T.; Leon, M.B.; Liu, M.; Mauri, L.; Negoita, M.; et al. A controlled trial of renal denervation for resistant hypertension. N. Engl. J. Med. 2014, 370, 1393–1401. [Google Scholar] [CrossRef]
- Townsend, R.R.; Mahfoud, F.; Kandzari, D.E.; Kario, K.; Pocock, S.; Weber, M.A.; Ewen, S.; Tsioufis, K.; Tousoulis, D.; Sharp, A.S.P.; et al. Catheter-based renal denervation in patients with uncontrolled hypertension in the absence of antihypertensive medications (SPYRAL HTN-OFF MED): A randomised, sham-controlled, proof-of-concept trial. Lancet 2017, 390, 2160–2170. [Google Scholar] [CrossRef]
- Azizi, M.; Schmieder, R.E.; Mahfoud, F.; Weber, M.A.; Daemen, J.; Davies, J.; Basile, J.; Kirtane, A.J.; Wang, Y.; Lobo, M.D.; et al. Endovascular ultrasound renal denervation to treat hypertension (RADIANCE-HTN SOLO): A multicentre, international, single-blind, randomised, sham-controlled trial. Lancet 2018, 391, 2335–2345, Erratum in: Lancet 2018, 392, 820. [Google Scholar] [CrossRef]
- Kandzari, D.E.; Böhm, M.; Mahfoud, F.; Townsend, R.R.; Weber, M.A.; Pocock, S.; Tsioufis, K.; Tousoulis, D.; Choi, J.W.; East, C.; et al. Effect of renal denervation on blood pressure in the presence of antihypertensive drugs: 6-month efficacy and safety results from the SPYRAL HTN-ON MED proof-of-concept randomised trial. Lancet 2018, 391, 2346–2355. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, U.C.; Brandt, M.C.; Wachter, R.; Beige, J.; Rump, L.C.; Kroon, A.A.; Cates, A.W.; Lovett, E.G.; Haller, H. Minimally invasive system for baroreflex activation therapy chronically lowers blood pressure with pacemaker-like safety profile: Results from the Barostim neo trial. J. Am. Soc. Hypertens. 2012, 6, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Scheffers, I.J.; Kroon, A.A.; Schmidli, J.; Jordan, J.; Tordoir, J.J.; Mohaupt, M.G.; Luft, F.C.; Haller, H.; Menne, J.; Engeli, S.; et al. Novel baroreflex activation therapy in resistant hypertension: Results of a European multi-center feasibility study. J. Am. Coll. Cardiol. 2010, 56, 1254–1258. [Google Scholar] [CrossRef]
- Bisognano, J.D.; Bakris, G.; Nadim, M.K.; Sanchez, L.; Kroon, A.A.; Schafer, J.; de Leeuw, P.W.; Sica, D.A. Baroreflex activation therapy lowers blood pressure in patients with resistant hypertension: Results from the double-blind, randomized, placebo-controlled rheos pivotal trial. J. Am. Coll. Cardiol. 2011, 58, 765–773. [Google Scholar] [CrossRef]
- Clinical Trials [Internet]. Controlling and Lowering Blood Pressure with the MOBIUSHD™ (CALM-FIM_US); National Institutes of Health: Bethesda, MD, USA, 2015. Available online: https://clinicaltrials.gov/ct2/show/NCT01831895 (accessed on 28 August 2015).
- Wei, F.F.; Zhang, Z.Y.; Huang, Q.F.; Yang, W.Y.; Staessen, J.A. Resistant hypertension. Kardiol. Pol. 2018, 76, 1031–1042. [Google Scholar] [CrossRef]
- Scholz, S.S.; Vukadinović, D.; Lauder, L.; Ewen, S.; Ukena, C.; Townsend, R.R.; Wagenpfeil, S.; Böhm, M.; Mahfoud, F. Effects of Arteriovenous Fistula on Blood Pressure in Patients With End-Stage Renal Disease: A Systematic Meta-Analysis. J. Am. Heart Assoc. 2019, 8, e011183. [Google Scholar] [CrossRef]
- Lobo, M.D.; Ott, C.; Sobotka, P.A.; Saxena, M.; Stanton, A.; Cockcroft, J.R.; Sulke, N.; Dolan, E.; van der Giet, M.; Hoyer, J.; et al. Central Iliac Arteriovenous Anastomosis for Uncontrolled Hypertension: One-Year Results From the ROX CONTROL HTN Trial. Hypertension 2017, 70, 1099–1105. [Google Scholar] [CrossRef]
- Mathew, R.O.; Fleg, J.; Rangaswami, J.; Cai, B.; Asif, A.; Sidhu, M.S.; Bangalore, S. Effect of Arteriovenous Fistula Creation on Systolic and Diastolic Blood Pressure in Patients With Pre-dialysis Advanced Chronic Kidney Disease. Am. J. Hypertens. 2019, 32, 858–867. [Google Scholar] [CrossRef]
- Faul, J.; Schoors, D.; Brouwers, S.; Scott, B.; Jerrentrup, A.; Galvin, J.; Luitjens, S.; Dolan, E. Creation of an iliac arteriovenous shunt lowers blood pressure in chronic obstructive pulmonary disease patients with hypertension. J. Vasc. Surg. 2014, 59, 1078–1083. [Google Scholar] [CrossRef]
- Lobo, M.D.; Sobotka, P.A.; Stanton, A.; Cockcroft, J.R.; Sulke, N.; Dolan, E.; van der Giet, M.; Hoyer, J.; Furniss, S.S.; Foran, J.P.; et al. Central arteriovenous anastomosis for the treatment of patients with uncontrolled hypertension (the ROX CONTROL HTN study): A randomised controlled trial. Lancet 2015, 385, 1634–1641, Erratum in: Lancet 2016, 387, 648. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Kario et al. [38] | Bourque et al. [39] | Lee et al. [40] | Feng et al. [41] |
|---|---|---|---|---|
| Year | 2023 | 2023 | 2022 | 2021 |
| All patients | 58 | 71,353 | 27,785,595 | 2,769,700 |
| Study design | Post hoc analysis | Meta-analysis | Meta-analysis | Meta-analysis |
| Patient characteristics | RH patients aged 20–75 years old. | RH patients aged ≥18 years old; uncontrolled with ≥3 drugs or controlled with ≥4 drugs. | AH patients with a mean age of 57; 42.9% men. | AH patients ≥18 years old at baseline, without a history of CVD events. |
| Aim of the study | Drug adherence at baseline and after 3 months postprocedure (uRDN). | Determine the overall prevalence of nonadherence and evaluate the effect of the method of assessment on this estimate. | Explore global epidemiology, regional differences, and trends in AHM nonadherence. | Determine the association between AHM adherence and risk of CVD events in patients with AH. |
| Methods | Urine sample testing for AHM or their metabolites to assess drug adherence. | MEDLINE, EMBASE, Cochrane, CINAHL, and Web of Science (databases from inception to November 2020) were searched. | Multiple medical databases and clinicaltrials.gov were searched for articles (data from 2010 to 2020). | Two databases (PubMed and Embase) from 1974 to 15 December 2019 were searched. |
| Drug adherence evaluation | 45% of RH patients had poor medication adherence. | The overall incidence of nonadherence was 37% (20% for indirect methods and 46% for direct methods). | AHM nonadherence did not improve between 2010 and 2020 and remained at 27–40%. | Each 20% increase in AHM adherence was associated with a 13% reduced risk of CVD events. |
| Trail | Year | Study Patients’ Office SBP | Study Patients’ Office DBP | Study Patients’ Ambulatory BP | Results | Reference |
|---|---|---|---|---|---|---|
| SYMPLICITY HTN-2 | 2012 | ≥160 mm Hg (≥150 mm Hg if they had T2DM) | - | - | lasting BP reduction to 1 year | [53] |
| SYMPLICITY HTN-3 | 2014 | ≥160 mm Hg | - | - | no significant BP reduction | [54] |
| SPYRAL HTN-OFF MED | 2017 | 150–180 mm Hg | ≥90 mm Hg | SBP 140–170 mm Hg | significant BP reduction | [55] |
| RADIANCE-HTN SOLO | 2018 | - | - | SBP 135–170 mm Hg DBP 85–105 mm Hg | significant BP reduction | [56] |
| SPYRAL HTN-ON MED | 2018 | 150–180 mm Hg | ≥90 mm Hg | SBP 140–170 mm Hg | lasting BP reduction to 6 months | [57] |
| Authors | Scholz et al. [63] | Lobo et al. [64] | Mathew et al. [65] | Faul et al. [66] |
|---|---|---|---|---|
| Study design | Meta-analysis | Randomized controlled trial | Comparative study | Clinical trial |
| All patients | 412 | 83 | 5095 | 24 |
| Patient category | Patients with ESRD, on dialysis or before dialysis, as well as post-transplant patients who were scheduled to receive an AVF or were already on an AVF implantation procedure. | Patients aged 18–80 years who maintained high BP values despite pharmacotherapy with three or more drugs. | Patients with ESRD before starting hemodialysis. | Patients with COPD and high BP values despite pharmacological treatment. |
| Effect on BP | AVF creation led to a significant reduction in SBP, DBP, and MAP, while AVF closure led to an increase in BP. | AFV caused a reduction in SBP and DBP. | A small reduction in BP over 12 months of follow-up in the intervention group was reported, with a greater reduction in DBP. | AFV caused a decrease in SBP and DBP. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dybiec, J.; Krzemińska, J.; Radzioch, E.; Szlagor, M.; Wronka, M.; Młynarska, E.; Rysz, J.; Franczyk, B. Advances in the Pathogenesis and Treatment of Resistant Hypertension. Int. J. Mol. Sci. 2023, 24, 12911. https://doi.org/10.3390/ijms241612911
Dybiec J, Krzemińska J, Radzioch E, Szlagor M, Wronka M, Młynarska E, Rysz J, Franczyk B. Advances in the Pathogenesis and Treatment of Resistant Hypertension. International Journal of Molecular Sciences. 2023; 24(16):12911. https://doi.org/10.3390/ijms241612911
Chicago/Turabian StyleDybiec, Jill, Julia Krzemińska, Ewa Radzioch, Magdalena Szlagor, Magdalena Wronka, Ewelina Młynarska, Jacek Rysz, and Beata Franczyk. 2023. "Advances in the Pathogenesis and Treatment of Resistant Hypertension" International Journal of Molecular Sciences 24, no. 16: 12911. https://doi.org/10.3390/ijms241612911