
β-Adrenoreceptors as Therapeutic Targets for Ocular Tumors and Other Eye Diseases—Historical Aspects and Nowadays Understanding


Abstract
:1. Introduction
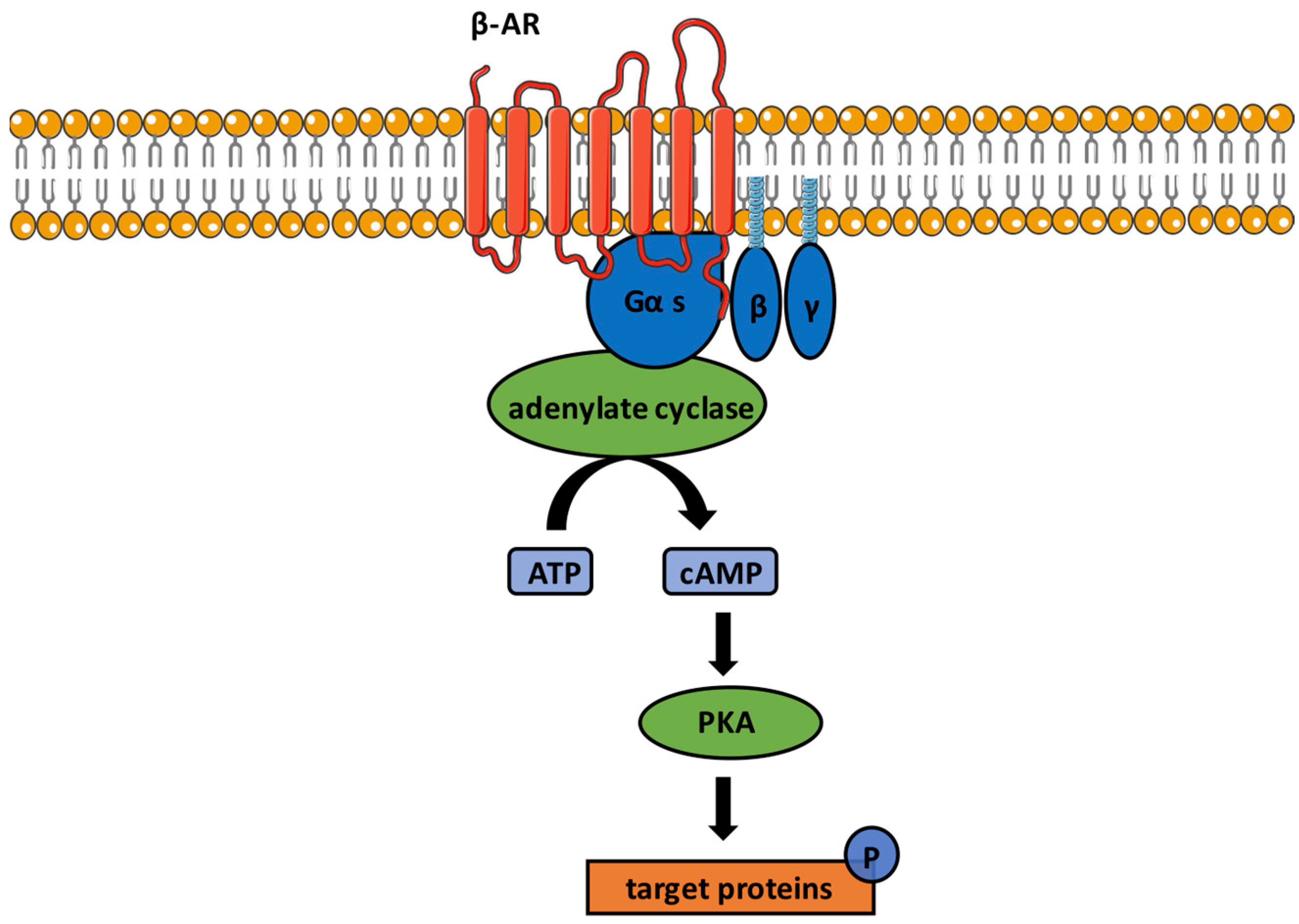
2. Historical Aspects, Classification and Function of β-Adrenoceptors
3. β-Adrenoceptors in Ocular Structures
3.1. Cornea
3.2. Conjunctiva
3.3. Lacrimal Gland
3.4. Trabecular Meshwork
3.5. Uvea
3.6. Retina
3.6.1. Potential Sources of Catecholamines in the Retina
3.6.2. Expression of β-Adrenoreceptors in the Retina
3.6.3. Role of β-Adrenoreceptors in the Retina
4. β-Adrenoreceptors in Ocular Tumors
4.1. Periocular Infantile Hemangioma
4.2. Choroidal Hemangioma
4.3. Retinal Hemangioblastoma
4.4. Conjunctival Hemangioma
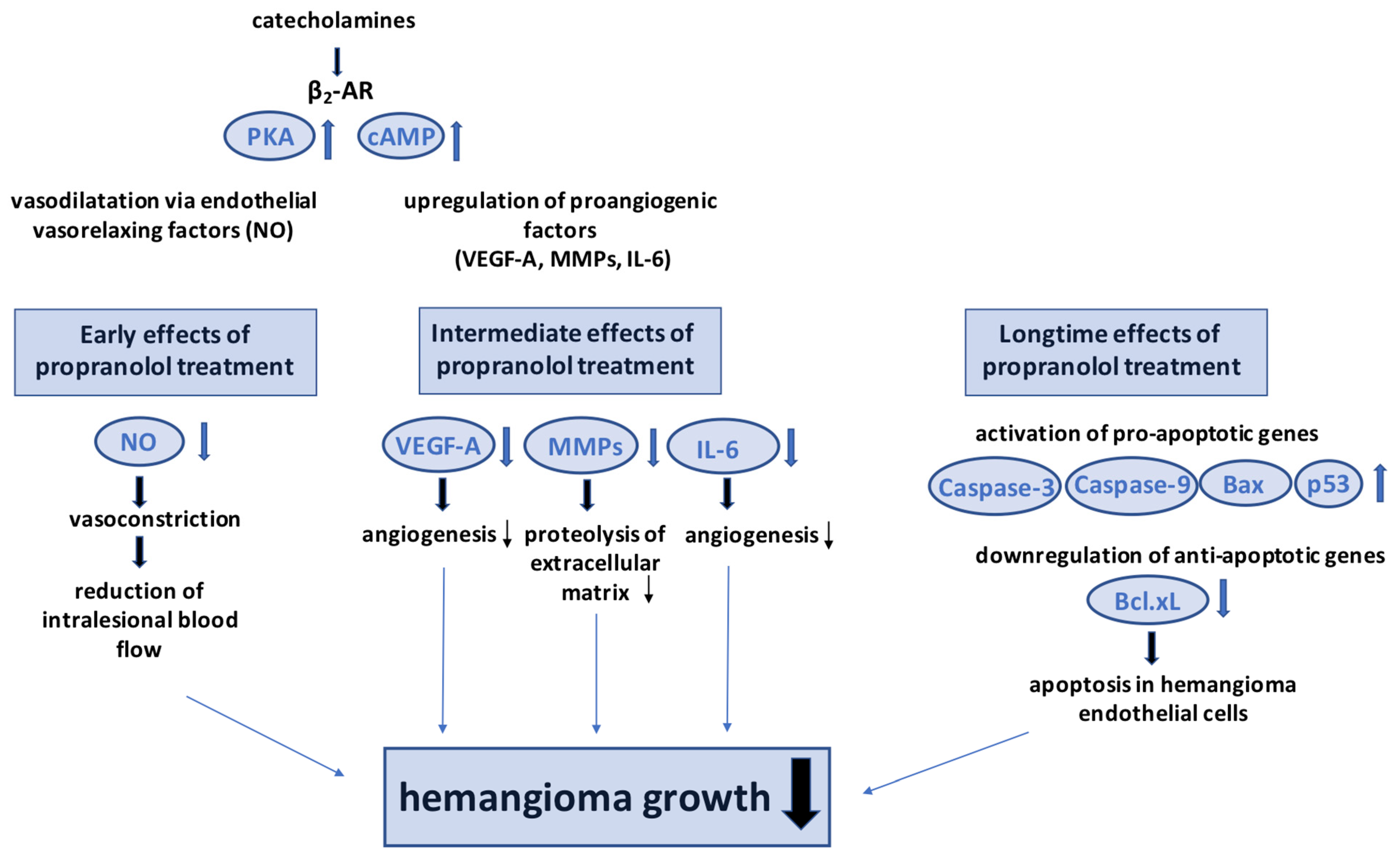
4.5. Potential Mechanisms of Ocular Hemangioma Treatment with Non-Subtype-Selective β-Blockers
4.6. Uveal Melanoma
4.7. β-ARs as Therapeutic Targets in Uveal Melanoma
5. Future Directions in Research
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ahlquist, R.P. A study of the adrenotropic receptors. Am. J. Physiol. 1948, 153, 586–600. [Google Scholar] [CrossRef]
- Wikberg-Matsson, A. α1- and α2-Adrenoceptors in the Eye: Pharmacological and Functional Characterization. Ph.D. Thesis, Acta Universitatis Upsaliensis, Uppsala, Sweden, 2001. [Google Scholar]
- Ruan, Y.; Böhmer, T.; Jiang, S.; Gericke, A. The Role of Adrenoceptors in the Retina. Cells 2020, 9, 2594. [Google Scholar] [CrossRef]
- Wachter, S.B.; Gilbert, E.M. Beta-adrenergic receptors, from their discovery and characterization through their manipulation to beneficial clinical application. Cardiology 2012, 122, 104–112. [Google Scholar] [CrossRef]
- Velmurugan, B.K.; Baskaran, R.; Huang, C.Y. Detailed insight on β-adrenoceptors as therapeutic targets. Biomed. Pharmacother. Biomed. Pharmacother. 2019, 117, 109039. [Google Scholar] [CrossRef]
- Benovic, J.L. Novel beta2-adrenergic receptor signaling pathways. J. Allergy Clin. Immunol. 2002, 110, S229–S235. [Google Scholar] [CrossRef] [PubMed]
- Grogan, A.; Lucero, E.Y.; Jiang, H.; Rockman, H.A. Pathophysiology and pharmacology of G protein-coupled receptors in the heart. Cardiovasc. Res. 2022, cvac171. [Google Scholar] [CrossRef]
- Bylund, D.B.; Eikenberg, D.C.; Hieble, J.P.; Langer, S.; Lefkowitz, R.; Minneman, K.P.; Molinoff, P.; Ruffolo, R.; Trendelenburg, U. International Union of Pharmacology nomenclature of adrenoceptors. Pharmacol. Rev. 1994, 46, 121–136. [Google Scholar]
- Kaumann, A.J.; Engelhardt, S.; Hein, L.; Molenaar, P.; Lohse, M. Abolition of (-)-CGP 12177-evoked cardiostimulation in double beta1/beta2-adrenoceptor knockout mice. Obligatory role of beta1-adrenoceptors for putative beta4-adrenoceptor pharmacology. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2001, 363, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Molinoff, P.B. Alpha- and beta-adrenergic receptor subtypes properties, distribution and regulation. Drugs 1984, 28 (Suppl. S2), 1–15. [Google Scholar] [CrossRef] [PubMed]
- Motiejunaite, J.; Amar, L.; Vidal-Petiot, E. Adrenergic receptors and cardiovascular effects of catecholamines. Ann. D’endocrinologie 2021, 82, 193–197. [Google Scholar] [CrossRef]
- Steinle, J.J.; Zamora, D.O.; Rosenbaum, J.T.; Granger, H.J. Beta 3-adrenergic receptors mediate choroidal endothelial cell invasion, proliferation, and cell elongation. Exp. Eye Res. 2005, 80, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Djurup, R. Adrenoceptors: Molecular Nature and Role in Atopic Diseases. Allergy 1981, 36, 289–307. [Google Scholar] [CrossRef] [PubMed]
- Toivanen, M.; Tervo, T.; Partanen, M.; Vannas, A.; Hervonen, A.J.I.o.; Science, v. Histochemical demonstration of adrenergic nerves in the stroma of human cornea. Vis. Sci. 1987, 28, 398–400. [Google Scholar]
- Müller, L.J.; Marfurt, C.F.; Kruse, F.; Tervo, T.M.T. Corneal nerves: Structure, contents and function. Exp. Eye Res. 2003, 76, 521–542. [Google Scholar] [CrossRef]
- Musayeva, A.; Manicam, C.; Steege, A.; Brochhausen, C.; Straub, B.K.; Bell, K.; Pfeiffer, N.; Gericke, A. Role of α(1)-adrenoceptor subtypes on corneal epithelial thickness and cell proliferation in mice. Am. J. Physiol. Cell Physiol. 2018, 315, C757–C765. [Google Scholar] [CrossRef] [Green Version]
- Candia, O.A.; Neufeld, A.H. Topical epinephrine causes a decrease in density of β-adrenergic receptors and catecholamine-stimulated chloride transport in the rabbit cornea. Biochim. Et Biophys. Acta (BBA) Gen. Subj. 1978, 543, 403–408. [Google Scholar] [CrossRef]
- Grayson, T.H.; Ellis, J.M.; Chen, S.; Graham, R.; Dale Brown, R.; Hill, C.J.C. Immunohistochemical localisation of α1B-adrenergic receptors in the rat iris. Cell Tissue Res. 1998, 293, 435–444. [Google Scholar] [CrossRef]
- Colley, A.; Cavanagh, H.D. Binding of [3H] dihydroalprenolol and [3H] quinuclidinyl benzilate to intact cells of cultured corneal epithelium. Metab. Pediatr. Syst. Ophthalmol. 1982, 6, 75–86. [Google Scholar]
- Walkenbach, R.J.; Gibbs, S.R.; Bylund, D.B.; Chao, W.-T. Characteristics of β-adrenergic receptors in bovine corneal epithelium: Comparison of fresh tissue and cultured cells. Biochem. Biophys. Res. Commun. 1984, 121, 664–672. [Google Scholar] [CrossRef]
- Elena, P.-P.; Denis, P.; Kosina-Boix, M.; Saraux, H.; Lapalus, P. Beta Adrenergic Binding Sites in the Human Eye: An Autoradiographic Study. J. Ocul. Pharmacol. Ther. 1990, 6, 143–149. [Google Scholar] [CrossRef]
- Pullar, C.E.; Zhao, M.; Song, B.; Pu, J.; Reid, B.; Ghoghawala, S.; McCaig, C.; Isseroff, R.R. Beta-adrenergic receptor agonists delay while antagonists accelerate epithelial wound healing: Evidence of an endogenous adrenergic network within the corneal epithelium. J. Cell. Physiol. 2007, 211, 261–272. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.S.; Trope, G.E.; Basu, P.K. Beta Adrenoceptors and Regenerating Corneal Epithelium. J. Ocul. Pharmacol. Ther. 1990, 6, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Nork, T.M.; Holly, F.J.; Hayes, J.; Wentlandt, T.; Lamberts, D.W. Timolol Inhibits Corneal Epithelial Wound Healing in Rabbits and Monkeys. Arch. Ophthalmol. 1984, 102, 1224–1228. [Google Scholar] [CrossRef] [PubMed]
- Reidy, J.J.; Zarzour, J.; Thompson, H.W.; Beuerman, R.W. Effect of topical beta blockers on corneal epithelial wound healing in the rabbit. Br. J. Ophthalmol. 1994, 78, 377. [Google Scholar] [CrossRef] [Green Version]
- Ghoghawala, S.Y.; Mannis, M.J.; Pullar, C.E.; Rosenblatt, M.I.; Isseroff, R.R. Beta2-adrenergic receptor signaling mediates corneal epithelial wound repair. Investig. Ophthalmol. Vis. Sci. 2008, 49, 1857–1863. [Google Scholar] [CrossRef]
- Yuan, X.; Ma, X.; Yang, L.; Zhou, Q.; Li, Y. β-blocker eye drops affect ocular surface through β2 adrenoceptor of corneal limbal stem cells. BMC Ophthalmol. 2021, 21, 419. [Google Scholar] [CrossRef]
- Diebold, Y.; Ríos, J.D.; Hodges, R.R.; Rawe, I.; Dartt, D.A. Presence of nerves and their receptors in mouse and human conjunctival goblet cells. Investig. Ophthalmol. Vis. Sci. 2001, 42, 2270–2282. [Google Scholar]
- Gautheron, P.; Sugrue, M.F. The ability of salbutamol and theophylline to suppress immediate allergic conjunctivitis in the guinea pig. Graefe’s Arch. Clin. Exp. Ophthalmol. Albrecht Von Graefes Arch. Fur Klin. Und Exp. Ophthalmol. 1987, 225, 331–334. [Google Scholar] [CrossRef]
- Dartt, D.A.; McCarthy, D.M.; Mercer, H.J.; Kessler, T.L.; Chung, E.H.; Zieske, J.D. Localization of nerves adjacent to goblet cells in rat conjunctiva. Curr. Eye Res. 1995, 14, 993–1000. [Google Scholar] [CrossRef]
- Gabanyi, I.; Muller, P.A.; Feighery, L.; Oliveira, T.Y.; Costa-Pinto, F.A.; Mucida, D.J.C. Neuro-immune interactions drive tissue programming in intestinal macrophages. Cell 2016, 164, 378–391. [Google Scholar] [CrossRef] [Green Version]
- Sharif, N.A.; Crider, J.Y.; Griffin, B.W.; Davis, T.L.; Howe, W.E. Pharmacological analysis of mast cell mediator and neurotransmitter receptors coupled to adenylate cyclase and phospholipase C on immunocytochemically-defined human conjunctival epithelial cells. J. Ocul. Pharmacol. Ther. Off. J. Assoc. Ocul. Pharmacol. Ther. 1997, 13, 321–336. [Google Scholar] [CrossRef]
- Ríos, J.D.; Forde, K.; Diebold, Y.; Lightman, J.; Zieske, J.D.; Dartt, D.A. Development of conjunctival goblet cells and their neuroreceptor subtype expression. Investig. Ophthalmol. Vis. Sci. 2000, 41, 2127–2137. [Google Scholar]
- Enríquez de Salamanca, A.; Siemasko, K.F.; Diebold, Y.; Calonge, M.; Gao, J.; Juárez-Campo, M.; Stern, M.E. Expression of muscarinic and adrenergic receptors in normal human conjunctival epithelium. Investig. Ophthalmol. Vis. Sci. 2005, 46, 504–513. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Huang, S.; Li, F.; Wu, M.; He, J.; Xue, Y.; Fu, T.; Yu, R.; Chen, X.; Wang, Y.; et al. Sympathetic Nerves Positively Regulate Eosinophil-Driven Allergic Conjunctivitis via α1-Adrenergic Receptor Signaling. Am. J. Pathol. 2020, 190, 1298–1308. [Google Scholar] [CrossRef]
- Woodward, D.F.; Nieves, A.L. Topical anti-inflammatory activity of beta 2-adrenoceptor agonists in the conjunctiva. J. Ocul. Pharmacol. 1985, 1, 391–396. [Google Scholar] [CrossRef] [PubMed]
- García-Posadas, L.; Hodges, R.R.; Utheim, T.P.; Olstad, O.K.; Delcroix, V.; Makarenkova, H.P.; Dartt, D.A. Lacrimal Gland Myoepithelial Cells Are Altered in a Mouse Model of Dry Eye Disease. Am. J. Pathol. 2020, 190, 2067–2079. [Google Scholar] [CrossRef]
- Botelho, S.Y.; Goldstein, A.M.; Martinez, E.V. Norepinephrine-responsive beta-adrenergic receptors in rabbit lacrimal gland. Am. J. Physiol. 1973, 224, 1119–1122. [Google Scholar] [CrossRef] [Green Version]
- Ikeda-Kurosawa, C.; Higashio, H.; Nakano, M.; Okubo, M.; Satoh, Y.; Kurosaka, D.; Saino, T. α1-Adrenoceptors relate Ca(2+) modulation and protein secretions in rat lacrimal gland. Biomed. Res. (Tokyo Jpn.) 2015, 36, 357–369. [Google Scholar] [CrossRef] [Green Version]
- Mauduit, P.; Herman, G.; Rossignol, B. Protein secretion in lacrimal gland: Alpha 1-beta-adrenergic synergism. Am. J. Physiol. 1986, 250, C704–C712. [Google Scholar] [CrossRef]
- Hodges, R.R.; Dicker, D.M.; Rose, P.E.; Dartt, D.A. Alpha 1-adrenergic and cholinergic agonists use separate signal transduction pathways in lacrimal gland. Am. J. Physiol. 1992, 262, G1087–G1096. [Google Scholar] [CrossRef]
- Aberg, G.; Adler, G.; Wikberg, J. Inhibition and facilitation of lacrimal flow by beta-adrenergic drugs. Acta Ophthalmol. (Copenh) 1979, 57, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Ding, C.; Walcott, B.; Keyser, K.T. The alpha1- and beta1-adrenergic modulation of lacrimal gland function in the mouse. Investig. Ophthalmol. Vis. Sci. 2007, 48, 1504–1510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petounis, A.D.; Akritopoulos, P. Influence of topical and systemic beta-blockers on tear production. Int. Ophthalmol. 1989, 13, 75–80. [Google Scholar] [CrossRef]
- Esmaeli-Gutstein, B.; Hewlett, B.R.; Harvey, J.T. Characterization of adrenergic receptors in the accessory lacrimal glands of the upper eyelid. Ophthalmic Plast. Reconstr. Surg. 1999, 15, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Jun, I.; Choi, Y.J.; Kim, B.R.; Seo, K.Y.; Kim, T.I. Activation of ADRB2/PKA Signaling Pathway Facilitates Lipid Synthesis in Meibocytes, and Beta-Blocker Glaucoma Drug Impedes PKA-Induced Lipid Synthesis by Inhibiting ADRB2. Int. J. Mol. Sci. 2022, 23, 9478. [Google Scholar] [CrossRef]
- Jampel, H.D.; Lynch, M.G.; Brown, R.H.; Kuhar, M.J.; De Souza, E.B. Beta-adrenergic receptors in human trabecular meshwork. Identification and autoradiographic localization. Investig. Ophthalmol. Vis. Sci. 1987, 28, 772–779. [Google Scholar]
- Wax, M.B.; Molinoff, P.B.; Alvarado, J.; Polansky, J. Characterization of beta-adrenergic receptors in cultured human trabecular cells and in human trabecular meshwork. Investig. Ophthalmol. Vis. Sci. 1989, 30, 51–57. [Google Scholar]
- Crider, J.Y.; Sharif, N.A. Adenylyl cyclase activity mediated by beta-adrenoceptors in immortalized human trabecular meshwork and non-pigmented ciliary epithelial cells. J. Ocul. Pharmacol. Ther. Off. J. Assoc. Ocul. Pharmacol. Ther. 2002, 18, 221–230. [Google Scholar] [CrossRef]
- Hudson, B.D.; Kelly, M.E. Identification of novel competing β2AR phospho-extracellular signal regulated kinase 1/2 signaling pathways in human trabecular meshwork cells. J. Ocul. Pharmacol. Ther. Off. J. Assoc. Ocul. Pharmacol. Ther. 2012, 28, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.C.; Kaufman, P.L. Effects and interactions of epinephrine, norepinephrine, timolol, and betaxolol on outflow facility in the cynomolgus monkey. Am. J. Ophthalmol. 1990, 109, 189–194. [Google Scholar] [CrossRef]
- Wiederholt, M.; Schäfer, R.; Wagner, U.; Lepple-Wienhues, A. Contractile response of the isolated trabecular meshwork and ciliary muscle to cholinergic and adrenergic agents. Ger. J. Ophthalmol. 1996, 5, 146–153. [Google Scholar] [PubMed]
- Nakamura, S.; Taniguchi, T.; Suzuki, F.; Akagi, Y.; Muramatsu, I. Evaluation of alpha1-adrenoceptors in the rabbit iris: Pharmacological characterization and expression of mRNA. Br. J. Pharmacol. 1999, 127, 1367–1374. [Google Scholar] [CrossRef] [Green Version]
- Wikberg-Matsson, A.; Wikberg, J.E.; Uhlén, S. Characterization of alpha 2-adrenoceptor subtypes in the porcine eye: Identification of alpha 2A-adrenoceptors in the choroid, ciliary body and iris, and alpha 2A- and alpha 2C-adrenoceptors in the retina. Exp. Eye Res. 1996, 63, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Wax, M.B.; Molinoff, P.B. Distribution and properties of beta-adrenergic receptors in human iris-ciliary body. Investig. Ophthalmol. Vis. Sci. 1987, 28, 420–430. [Google Scholar]
- Suzuki, F.; Taniguchi, T.; Nakamura, S.; Akagi, Y.; Kubota, C.; Satoh, M.; Muramatsu, I. Distribution of alpha-1 adrenoceptor subtypes in RNA and protein in rabbit eyes. Br. J. Pharmacol. 2002, 135, 600–608. [Google Scholar] [CrossRef]
- Yu, Y.; Koss, M.C. Functional characterization of alpha-adrenoceptors mediating pupillary dilation in rats. Eur. J. Pharmacol. 2003, 471, 135–140. [Google Scholar] [CrossRef]
- Elena, P.P.; Kosina-Boix, M.; Moulin, G.; Lapalus, P. Autoradiographic localization of beta-adrenergic receptors in rabbit eye. Investig. Ophthalmol. Vis. Sci. 1987, 28, 1436–1441. [Google Scholar]
- Bromberg, B.B.; Gregory, D.S.; Sears, M.L. Beta-adrenergic receptors in ciliary processes of the rabbit. Investig. Ophthalmol. Vis. Sci. 1980, 19, 203–207. [Google Scholar]
- Oelke, M.; Gericke, A.; Michel, M.C. Cardiovascular and ocular safety of α1-adrenoceptor antagonists in the treatment of male lower urinary tract symptoms. Expert Opin. Drug Saf. 2014, 13, 1187–1197. [Google Scholar] [CrossRef]
- Nathanson, J.A. Human ciliary process adrenergic receptor: Pharmacological characterization. Investig. Ophthalmol. Vis. Sci. 1981, 21, 798–804. [Google Scholar]
- Elena, P.P.; Fredj-Reygrobellet, D.; Moulin, G.; Lapalus, P. Pharmacological characteristics of beta-adrenergic-sensitive adenylate cyclase in non pigmented and in pigmented cells of bovine ciliary process. Curr. Eye Res. 1984, 3, 1383–1389. [Google Scholar] [CrossRef]
- Mittag, T.; Tormay, A. Desensitization of the beta-adrenergic receptor-adenylate cyclase complex in rabbit iris-ciliary body induced by topical epinephrine. Exp. Eye Res. 1981, 33, 497–503. [Google Scholar] [CrossRef]
- Potter, D.E. Adrenergic pharmacology of aqueous humor dynamics. Pharmacol. Rev. 1981, 33, 133–153. [Google Scholar]
- Trope, G.E.; Clark, B. Binding potencies of 3 new beta 2 specific blockers to beta receptors in the ciliary processes and the possible relevance of these drugs to intraocular pressure control. Br. J. Ophthalmol. 1984, 68, 245–247. [Google Scholar] [CrossRef]
- Neufeld, A.H. Experimental studies on the mechanism of action of timolol. Surv. Ophthalmol. 1979, 23, 363–370. [Google Scholar] [CrossRef]
- Nathanson, J.A. Effects of a potent and specific beta 2-adrenoceptor antagonist on intraocular pressure. Br. J. Pharmacol. 1981, 73, 97–100. [Google Scholar] [CrossRef]
- Nathanson, J.A. ICI 118,551: An effective ocular hypotensive agent with selectivity for the ciliary process beta 2-adrenoceptor and with minimal cardiac side effects. Br. J. Pharmacol. 1984, 83, 821–829. [Google Scholar] [CrossRef]
- Grajewski, A.L.; Ferrari-Dileo, G.; Feuer, W.J.; Anderson, D.R. Beta-adrenergic responsiveness of choroidal vasculature. Ophthalmology 1991, 98, 989–995. [Google Scholar] [CrossRef]
- Steinle, J.J.; Smith, P.G. Role of adrenergic receptors in vascular remodelling of the rat choroid. Br. J. Pharmacol. 2002, 136, 730–734. [Google Scholar] [CrossRef]
- Lavine, J.A.; Sang, Y.; Wang, S.; Ip, M.S.; Sheibani, N. Attenuation of choroidal neovascularization by β(2)-adrenoreceptor antagonism. JAMA Ophthalmol. 2013, 131, 376–382. [Google Scholar] [CrossRef] [Green Version]
- Lavine, J.A.; Farnoodian, M.; Wang, S.; Darjatmoko, S.R.; Wright, L.S.; Gamm, D.M.; Ip, M.S.; Sorenson, C.M.; Sheibani, N. β2-Adrenergic Receptor Antagonism Attenuates CNV Through Inhibition of VEGF and IL-6 Expression. Investig. Ophthalmol. Vis. Sci. 2017, 58, 299–308. [Google Scholar] [CrossRef] [Green Version]
- Amini, R.; Rocha-Martins, M.; Norden, C. Neuronal Migration and Lamination in the Vertebrate Retina. Front. Neurosci. 2018, 11, 742. [Google Scholar] [CrossRef]
- Masland, R.H. The Neuronal Organization of the Retina. Neuron 2012, 76, 266–280. [Google Scholar] [CrossRef] [Green Version]
- Haider, N.B.; Cruz, N.M.; Allocca, M.; Yuan, J. Pathobiology of the Outer Retina: Genetic and Nongenetic Causes of Disease. In Pathobiology of Human Disease; McManus, L.M., Mitchell, R.N., Eds.; Academic Press: San Diego, CA, USA, 2014. [Google Scholar]
- Herzlich, A.A.; Patel, M.; Charles Sauer, T.; Chan, C.-C. CHAPTER 2-Retinal anatomy and pathology. In Retinal Pharmacotherapy; Nguyen, Q.D., Rodrigues, E.B., Farah, M.E., Mieler, W.F., Eds.; W.B. Saunders: Edinburgh, UK, 2010. [Google Scholar]
- Kur, J.; Newman, E.A.; Chan-Ling, T. Cellular and physiological mechanisms underlying blood flow regulation in the retina and choroid in health and disease. Prog. Retin. Eye Res. 2012, 31, 377–406. [Google Scholar] [CrossRef] [Green Version]
- Hogan, M.J.; Feeney, L. The ultrastructure of the retinal blood vessels: I. The large vessels. J. Ultrastruct. Res. 1963, 9, 10–28. [Google Scholar] [CrossRef]
- Ferrari-Dileo, G.; Davis, E.B.; Anderson, D.R. Biochemical evidence for cholinergic activity in retinal blood vessels. Investig. Ophthalmol. Vis. Sci. 1989, 30, 473–477. [Google Scholar]
- Gericke, A.; Goloborodko, E.; Sniatecki, J.J.; Steege, A.; Wojnowski, L.; Pfeiffer, N. Contribution of nitric oxide synthase isoforms to cholinergic vasodilation in murine retinal arterioles. Exp. Eye Res. 2013, 109, 60–66. [Google Scholar] [CrossRef]
- Liu, H.; Mercieca, K.; Anders, F.; Prokosch, V. Hydrogen Sulfide and β-Synuclein Are Involved and Interlinked in the Aging Glaucomatous Retina. J. Ophthalmol. 2020, 2020, 8642135. [Google Scholar] [CrossRef] [Green Version]
- Hadjiconstantinou, M.; Cohen, J.; Neff, N.H. Epinephrine: A Potential Neurotransmitter in Retina. J. Neurochem. 1983, 41, 1440–1444. [Google Scholar] [CrossRef]
- Nguyen-Legros, J. Chapter 5 morphology and distribution of catecholamine-neurons in mammalian retina. Prog. Retin. Res. 1988, 7, 113–147. [Google Scholar] [CrossRef]
- Casini, G.; Dal Monte, M.; Fornaciari, I.; Filippi, L.; Bagnoli, P. The β-adrenergic system as a possible new target for pharmacologic treatment of neovascular retinal diseases. Prog. Retin. Eye Res. 2014, 42, 103–129. [Google Scholar] [CrossRef]
- Hirasawa, H.; Contini, M.; Raviola, E. Extrasynaptic release of GABA and dopamine by retinal dopaminergic neurons. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2015, 370, 20140186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haeggendal, J.; Malmfors, T. Identification and Cellular Localization of the Catecholamines in the Retina and the Choroid of The Rabbit. Acta Physiol. Scand. 1965, 64, 58–66. [Google Scholar] [CrossRef]
- Osborne, N.N. Noradrenaline, a Transmitter Candidate in the Retina. J. Neurochem. 1981, 36, 17–27. [Google Scholar] [CrossRef]
- Lei, S. Cross interaction of dopaminergic and adrenergic systems in neural modulation. Int. J. Physiol.Pathophysiol.Pharm. 2014, 6, 137–142. [Google Scholar]
- Mori, A.; Hanada, M.; Sakamoto, K.; Nakahara, T.; Ishii, K. Noradrenaline contracts rat retinal arterioles via stimulation of alpha(1A)- and alpha(1D)-adrenoceptors. Eur. J. Pharmacol. 2011, 673, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Wikberg-Matsson, A.; Uhlén, S.; Wikberg, J.E. Characterization of alpha(1)-adrenoceptor subtypes in the eye. Exp. Eye Res. 2000, 70, 51–60. [Google Scholar] [CrossRef]
- Forster, B.A.; Ferrari-Dileo, G.; Anderson, D.R. Adrenergic alpha 1 and alpha 2 binding sites are present in bovine retinal blood vessels. Investig. Ophthalmol. Vis. Sci. 1987, 28, 1741–1746. [Google Scholar]
- Gericke, A.; Böhmer, T.; Michel, M.C. β3-Adrenoceptors: A drug target in ophthalmology? Naunyn-Schmiedeberg’s Arch. Pharmacol. 2013, 386, 265–267. [Google Scholar] [CrossRef] [Green Version]
- Steinle, J.J.; Booz, G.W.; Meininger, C.J.; Day, J.N.; Granger, H.J. β3-adrenergic receptors regulate retinal endothelial cell migration and proliferation. J. Biol. Chem. 2003, 278, 20681–20686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Böhmer, T.; Manicam, C.; Steege, A.; Michel, M.C.; Pfeiffer, N.; Gericke, A. The α1B -adrenoceptor subtype mediates adrenergic vasoconstriction in mouse retinal arterioles with damaged endothelium. Br. J. Pharmacol. 2014, 171, 3858–3867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinle, J.J. Sympathetic neurotransmission modulates expression of inflammatory markers in the rat retina. Exp. Eye Res. 2007, 84, 118–125. [Google Scholar] [CrossRef]
- Wiley, L.A.; Berkowitz, B.A.; Steinle, J.J. Superior cervical ganglionectomy induces changes in growth factor expression in the rat retina. Investig. Ophthalmol. Vis. Sci. 2006, 47, 439–443. [Google Scholar] [CrossRef] [Green Version]
- Wiley, L.A.; Rupp, G.R.; Steinle, J.J. Sympathetic Innervation Regulates Basement Membrane Thickening and Pericyte Number in Rat Retina. Investig. Ophthalmol. Vis. Sci. 2005, 46, 744–748. [Google Scholar] [CrossRef] [Green Version]
- Zarbin, M.A.; Wamsley, J.K.; Palacios, J.M.; Kuhar, M.J. Autoradiographic localization of high affinity GABA, benzodiazepine, dopaminergic, adrenergic and muscarinic cholinergic receptors in the rat, monkey and human retina. Brain Res. 1986, 374, 75–92. [Google Scholar] [CrossRef]
- Ferrari-Dileo, G. Beta 1 and beta 2 adrenergic binding sites in bovine retina and retinal blood vessels. Investig. Ophthalmol. Vis. Sci. 1988, 29, 695–699. [Google Scholar]
- Mori, A.; Miwa, T.; Sakamoto, K.; Nakahara, T.; Ishii, K. Pharmacological evidence for the presence of functional β3-adrenoceptors in rat retinal blood vessels. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2010, 382, 119–126. [Google Scholar] [CrossRef]
- Ristori, C.; Filippi, L.; Dal Monte, M.; Martini, D.; Cammalleri, M.; Fortunato, P.; la Marca, G.; Fiorini, P.; Bagnoli, P. Role of the adrenergic system in a mouse model of oxygen-induced retinopathy: Antiangiogenic effects of beta-adrenoreceptor blockade. Investig. Ophthalmol. Vis. Sci. 2011, 52, 155–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dal Monte, M.; Martini, D.; Latina, V.; Pavan, B.; Filippi, L.; Bagnoli, P. Beta-Adrenoreceptor Agonism Influences Retinal Responses to Hypoxia in a Model of Retinopathy of Prematurity. Investig. Ophthalmol. Vis. Sci. 2012, 53, 2181–2192. [Google Scholar] [CrossRef] [Green Version]
- Safi, S.Z.; Qvist, R.; Yan, G.O.; Ismail, I.S. Differential expression and role of hyperglycemia induced oxidative stress in epigenetic regulation of β1, β2 and β3-adrenergic receptors in retinal endothelial cells. BMC Med. Genom. 2014, 7, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindgren, I.; Altimiras, J. Chronic prenatal hypoxia sensitizes beta-adrenoceptors in the embryonic heart but causes postnatal desensitization. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2009, 297, R258–R264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aiello, L.P.; Avery, R.L.; Arrigg, P.G.; Keyt, B.A.; Jampel, H.D.; Shah, S.T.; Pasquale, L.R.; Thieme, H.; Iwamoto, M.A.; Park, J.E.; et al. Vascular endothelial growth factor in ocular fluid of patients with diabetic retinopathy and other retinal disorders. N. Engl. J. Med. 1994, 331, 1480–1487. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Smith, L.E.H. Retinopathy of prematurity. Angiogenesis 2007, 10, 133–140. [Google Scholar] [CrossRef] [Green Version]
- Dal Monte, M.; Cammalleri, M.; Mattei, E.; Filippi, L.; Bagnoli, P. Protective Effects of β1/2 Adrenergic Receptor Deletion in a Model of Oxygen-Induced Retinopathy. Investig. Ophthalmol. Vis. Sci. 2015, 56, 59–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martini, D.; Monte, M.D.; Ristori, C.; Cupisti, E.; Mei, S.; Fiorini, P.; Filippi, L.; Bagnoli, P. Antiangiogenic effects of β2-adrenergic receptor blockade in a mouse model of oxygen-induced retinopathy. J. Neurochem. 2011, 119, 1317–1329. [Google Scholar] [CrossRef]
- Jiang, Y.; Zhang, Q.; Steinle, J. Beta-adrenergic receptor agonist decreases VEGF levels through altered eNOS and PKC signaling in diabetic retina. Growth Factors (Chur Switz.) 2015, 33, 192–199. [Google Scholar] [CrossRef] [Green Version]
- Amato, R.; Pisani, F.; Laudadio, E.; Cammalleri, M.; Lucchesi, M.; Marracci, S.; Filippi, L.; Galeazzi, R.; Svelto, M.; Dal Monte, M.; et al. HIF-1-Dependent Induction of β3 Adrenoceptor: Evidence from the Mouse Retina. Cells 2022, 11, 1271. [Google Scholar] [CrossRef]
- Hirota, K. HIF-α Prolyl Hydroxylase Inhibitors and Their Implications for Biomedicine: A Comprehensive Review. Biomedicines 2021, 9, 468. [Google Scholar] [CrossRef]
- Filippi, L.; Cammalleri, M.; Amato, R.; Ciantelli, M.; Pini, A.; Bagnoli, P.; Dal Monte, M. Decoupling Oxygen Tension from Retinal Vascularization as a New Perspective for Management of Retinopathy of Prematurity. New Opportunities from β-adrenoceptors. Front. Pharmacol. 2022, 13, 835771. [Google Scholar] [CrossRef]
- Dal Monte, M.; Filippi, L.; Bagnoli, P. Beta3-adrenergic receptors modulate vascular endothelial growth factor release in response to hypoxia through the nitric oxide pathway in mouse retinal explants. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2013, 386, 269–278. [Google Scholar] [CrossRef]
- Oikawa, F.; Nakahara, T.; Akanuma, K.; Ueda, K.; Mori, A.; Sakamoto, K.; Ishii, K. Protective effects of the β3-adrenoceptor agonist CL316243 against N-methyl-D-aspartate-induced retinal neurotoxicity. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2012, 385, 1077–1081. [Google Scholar] [CrossRef] [PubMed]
- Jean-Luc, B. Beta3-Adrenoreceptors in Cardiovasular Diseases: New Roles for an “Old” Receptor. Curr. Drug Deliv. 2013, 10, 64–66. [Google Scholar] [CrossRef]
- Wallukat, G. The beta-adrenergic receptors. Herz 2002, 27, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Yun, J.-H.; Jeong, H.-S.; Kim, K.-J.; Han, M.H.; Lee, E.H.; Lee, K.; Cho, C.-H. β-Adrenergic receptor agonists attenuate pericyte loss in diabetic retinas through Akt activation. FASEB J. 2018, 32, 2324–2338. [Google Scholar] [CrossRef] [Green Version]
- Steinle, J.J.; Chin, V.C.; Williams, K.P.; Panjala, S.R. Beta-adrenergic receptor stimulation modulates iNOS protein levels through p38 and ERK1/2 signaling in human retinal endothelial cells. Exp. Eye Res. 2008, 87, 30–34. [Google Scholar] [CrossRef]
- Dickison, P.; Christou, E.; Wargon, O. A prospective study of infantile hemangiomas with a focus on incidence and risk factors. Pediatr. Dermatol. 2011, 28, 663–669. [Google Scholar] [CrossRef]
- Tavakoli, M.; Yadegari, S.; Mosallaei, M.; Aletaha, M.; Salour, H.; Lee, W.W. Infantile Periocular Hemangioma. J. Ophthalmic Vis. Res. 2017, 12, 205–211. [Google Scholar] [CrossRef]
- Chang, L.C.; Haggstrom, A.N.; Drolet, B.A.; Baselga, E.; Chamlin, S.L.; Garzon, M.C.; Horii, K.A.; Lucky, A.W.; Mancini, A.J.; Metry, D.W.; et al. Growth characteristics of infantile hemangiomas: Implications for management. Pediatrics 2008, 122, 360–367. [Google Scholar] [CrossRef] [Green Version]
- Alniemi, S.T.; Griepentrog, G.J.; Diehl, N.; Mohney, B.G. Incidence and clinical characteristics of periocular infantile hemangiomas. Arch. Ophthalmol. 2012, 130, 889–893. [Google Scholar] [CrossRef]
- Frieden, I.J.; Reese, V.; Cohen, D. PHACE syndrome. The association of posterior fossa brain malformations, hemangiomas, arterial anomalies, coarctation of the aorta and cardiac defects, and eye abnormalities. Arch. Dermatol. 1996, 132, 307–311. [Google Scholar] [CrossRef]
- Kronenberg, A.; Blei, F.; Ceisler, E.; Steele, M.; Furlan, L.; Kodsi, S. Ocular and systemic manifestations of PHACES (Posterior fossa malformations, Hemangiomas, Arterial anomalies, Cardiac defects and coarctation of the Aorta, Eye abnormalities, and Sternal abnormalities or ventral developmental defects) syndrome. J. AAPOS Off. Publ. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2005, 9, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Haik, B.G.; Jakobiec, F.A.; Ellsworth, R.M.; Jones, I.S. Capillary hemangioma of the lids and orbit: An analysis of the clinical features and therapeutic results in 101 cases. Ophthalmology 1979, 86, 760–792. [Google Scholar] [CrossRef] [PubMed]
- Spierer, O.; Neudorfer, M.; Leibovitch, I.; Stolovitch, C.; Kessler, A. Colour Doppler ultrasound imaging findings in paediatric periocular and orbital haemangiomas. Acta Ophthalmol. 2012, 90, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Navarro, O.M.; Laffan, E.E.; Ngan, B.Y. Pediatric soft-tissue tumors and pseudo-tumors: MR imaging features with pathologic correlation: Part 1. Imaging approach, pseudotumors, vascular lesions, and adipocytic tumors. Radiographics 2009, 29, 887–906. [Google Scholar] [CrossRef]
- Bilaniuk, L.T. Vascular lesions of the orbit in children. Neuroimaging Clin. North Am. 2005, 15, 107–120. [Google Scholar] [CrossRef] [PubMed]
- Satterfield, K.R.; Chambers, C.B. Current treatment and management of infantile hemangiomas. Surv. Ophthalmol. 2019, 64, 608–618. [Google Scholar] [CrossRef] [PubMed]
- Léauté-Labrèze, C.; Dumas de la Roque, E.; Hubiche, T.; Boralevi, F.; Thambo, J.B.; Taïeb, A. Propranolol for severe hemangiomas of infancy. N. Engl. J. Med. 2008, 358, 2649–2651. [Google Scholar] [CrossRef]
- Hermans, D.J.; Bauland, C.G.; Zweegers, J.; van Beynum, I.M.; van der Vleuten, C.J. Propranolol in a case series of 174 patients with complicated infantile haemangioma: Indications, safety and future directions. Br. J. Dermatol. 2013, 168, 837–843. [Google Scholar] [CrossRef]
- Zaher, H.; Rasheed, H.; Hegazy, R.A.; Hegazy, R.A.; Abdelhalim, D.M.; Gawdat, H.I. Oral propranolol: An effective, safe treatment for infantile hemangiomas. Eur. J. Dermatol. EJD 2011, 21, 558–563. [Google Scholar] [CrossRef] [Green Version]
- Schneider, M.; Cremer, H.J.; Ruef, P. A retrospective analysis of systemic propranolol for the treatment of complicated infantile haemangiomas. Acta Paediatr. 2014, 103, 977–983. [Google Scholar] [CrossRef]
- Bonifazi, E.; Acquafredda, A.; Milano, A.; Montagna, O.; Laforgia, N. Severe hypoglycemia during successful treatment of diffuse hemangiomatosis with propranolol. Pediatr. Dermatol. 2010, 27, 195–196. [Google Scholar] [CrossRef] [PubMed]
- Handgretinger, R. How an accidental discovery paved the way for the treatment of complicated infantile haemangiomas. Acta Paediatr. 2014, 103, 896–897. [Google Scholar] [CrossRef] [PubMed]
- De Graaf, M.; Breur, J.; Raphaël, M.F.; Vos, M.; Breugem, C.C.; Pasmans, S. Adverse effects of propranolol when used in the treatment of hemangiomas: A case series of 28 infants. J. Am. Acad. Dermatol. 2011, 65, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Price, C.J.; Lattouf, C.; Baum, B.; McLeod, M.; Schachner, L.A.; Duarte, A.M.; Connelly, E.A. Propranolol vs corticosteroids for infantile hemangiomas: A multicenter retrospective analysis. Arch. Dermatol. 2011, 147, 1371–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizvi, S.A.; Yusuf, F.; Sharma, R.; Rizvi, S.W. Managment of superficial infantile capillary hemangiomas with topical timolol maleate solution. Semin. Ophthalmol. 2015, 30, 62–64. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; Ni, N. Topical treatment for capillary hemangioma of the eyelid using beta-blocker solution. Arch. Ophthalmol. 2010, 128, 255–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvo, M.; Garcia-Millán, C.; Villegas, C.; Fueyo-Casado, A.; Burón, I. Topical timolol for infantile hemangioma of the eyelid. Int. J. Dermatol. 2013, 52, 603–604. [Google Scholar] [CrossRef] [PubMed]
- Painter, S.L.; Hildebrand, G.D. Review of topical beta blockers as treatment for infantile hemangiomas. Surv. Ophthalmol. 2016, 61, 51–58. [Google Scholar] [CrossRef]
- Junejo, M.S.; Rebecca; Memon, M.N.; Shaikh, S.P. Role of topical beta blockers in regression of infantile capillary hemangioma. Pak. J. Med. Sci. 2021, 37, 1935–1938. [Google Scholar] [CrossRef]
- Chambers, C.B.; Katowitz, W.R.; Katowitz, J.A.; Binenbaum, G. A controlled study of topical 0.25% timolol maleate gel for the treatment of cutaneous infantile capillary hemangiomas. Ophthalmic Plast. Reconstr. Surg. 2012, 28, 103–106. [Google Scholar] [CrossRef]
- Painter, S.L.; Hildebrand, G.D. Topical timolol maleate 0.5% solution for the management of deep periocular infantile hemangiomas. J. AAPOS Off. Publ. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2016, 20, 172–174.e171. [Google Scholar] [CrossRef] [PubMed]
- Xue, K.; Hildebrand, G.D. Deep periocular infantile capillary hemangiomas responding to topical application of timolol maleate, 0.5%, drops. JAMA Ophthalmol. 2013, 131, 1246–1248. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Garza, F.Z.; Ríos, M.; Roé-Crespo, E.; Bernabeu-Wittel, J.; Montserrat-García, M.T.; Puig, L.; Gich, I.; Baselga, E. Efficacy and Safety of Topical Timolol for the Treatment of Infantile Hemangioma in the Early Proliferative Stage: A Randomized Clinical Trial. JAMA Dermatol. 2021, 157, 583–587. [Google Scholar] [CrossRef] [PubMed]
- Marey, H.M.; Elmazar, H.F.; Mandour, S.S.; Khairy, H.A. Combined Oral and Topical Beta Blockers for the Treatment of Early Proliferative Superficial Periocular Infantile Capillary Hemangioma. J. Pediatr. Ophthalmol. Strabismus 2018, 55, 37–42. [Google Scholar] [CrossRef] [Green Version]
- Awadein, A.; Fakhry, M.A. Evaluation of intralesional propranolol for periocular capillary hemangioma. Clin. Ophthalmol. 2011, 5, 1135–1140. [Google Scholar] [CrossRef] [Green Version]
- Torres-Pradilla, M.; Baselga, E. Failure of intralesional propranolol in infantile hemangiomas. Pediatr. Dermatol. 2014, 31, 156–158. [Google Scholar] [CrossRef]
- Mehta, A.; Bajaj, M.S.; Pushker, N.; Chawla, B.; Pujari, A.; Grewal, S.S.; Grewal, S.P.S.; Singh, S.R.; Kishore, A.; Yadav, N.S. To compare intralesional and oral propranolol for treating periorbital and eyelid capillary hemangiomas. Indian J. Ophthalmol. 2019, 67, 1974–1980. [Google Scholar] [CrossRef]
- Sen, M.; Honavar, S.G. Circumscribed choroidal hemangioma: An overview of clinical manifestation, diagnosis and management. Indian J. Ophthalmol. 2019, 67, 1965–1973. [Google Scholar] [CrossRef]
- Singh, A.D.; Kaiser, P.K.; Sears, J.E. Choroidal hemangioma. Ophthalmol. Clin. North Am. 2005, 18, 151–161. [Google Scholar] [CrossRef]
- Shields, C.L.; Honavar, S.G.; Shields, J.A.; Cater, J.; Demirci, H. Circumscribed choroidal hemangioma: Clinical manifestations and factors predictive of visual outcome in 200 consecutive cases. Ophthalmology 2001, 108, 2237–2248. [Google Scholar] [CrossRef]
- Krohn, J.; Rishi, P.; Frøystein, T.; Singh, A.D. Circumscribed choroidal haemangioma: Clinical and topographical features. Br. J. Ophthalmol. 2019, 103, 1448–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schepens, C.L.; Schwartz, A. Intraocular tumors. I. Bilateral hemangioma of the choroid. AMA. Arch. Ophthalmol. 1958, 60, 72–83. [Google Scholar] [CrossRef] [PubMed]
- Perri, P.; Incorvaia, C.; Costagliola, C.; Parmeggiani, F.; Lamberti, G.; Paduano, B.; Sebastiani, A.; Ciro, C. Bilateral circumscribed haemangioma of the choroid not associated with systemic vascular syndrome. Br. J. Ophthalmol. 2001, 85, 1260–1261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, H.V.; Schalenbourg, A.; Zografos, L. Bilateral circumscribed choroidal hemangioma in an otherwise healthy individual. Retin. Cases Brief Rep. 2007, 1, 149–152. [Google Scholar] [CrossRef]
- Sanborn, G.E.; Augsburger, J.J.; Shields, J.A. Treatment of circumscribed choroidal hemangiomas. Ophthalmology 1982, 89, 1374–1380. [Google Scholar] [CrossRef]
- Boixadera, A.; García-Arumí, J.; Martínez-Castillo, V.; Encinas, J.L.; Elizalde, J.; Blanco-Mateos, G.; Caminal, J.; Capeans, C.; Armada, F.; Navea, A.; et al. Prospective clinical trial evaluating the efficacy of photodynamic therapy for symptomatic circumscribed choroidal hemangioma. Ophthalmology 2009, 116, 100–105.e101. [Google Scholar] [CrossRef]
- Shields, C.L.; Shields, J.A.; Perez, N.; Singh, A.D.; Cater, J. Primary transpupillary thermotherapy for small choroidal melanoma in 256 consecutive cases: Outcomes and limitations. Ophthalmology 2002, 109, 225–234. [Google Scholar] [CrossRef]
- Kivelä, T.; Tenhunen, M.; Joensuu, T.; Tommila, P.; Joensuu, H.; Kouri, M. Stereotactic radiotherapy of symptomatic circumscribed choroidal hemangiomas. Ophthalmology 2003, 110, 1977–1982. [Google Scholar] [CrossRef]
- Ritland, J.S.; Eide, N.; Tausjø, J. External beam irradiation therapy for choroidal haemangiomas. Visual and anatomical results after a dose of 20 to 25 Gy. Acta Ophthalmol. Scand. 2001, 79, 184–186. [Google Scholar] [CrossRef]
- Lasave, A.F.; Serrano, M.A.; Arevalo, J.F. Photodynamic Therapy with Verteporfin Plus Intravitreal Bevacizumab for Circumscribed Choroidal Hemangioma: 4 Years of Follow-Up. Retin. Cases Brief Rep. 2020, 14, 110–115. [Google Scholar] [CrossRef]
- Mandal, S.; Naithani, P.; Venkatesh, P.; Garg, S. Intravitreal bevacizumab (avastin) for circumscribed choroidal hemangioma. Indian J. Ophthalmol. 2011, 59, 248–251. [Google Scholar] [CrossRef] [PubMed]
- Witschel, H.; Font, R.L. Hemangioma of the choroid. A clinicopathologic study of 71 cases and a review of the literature. Surv. Ophthalmol. 1976, 20, 415–431. [Google Scholar] [CrossRef] [PubMed]
- Karimi, S.; Nourinia, R.; Mashayekhi, A. Circumscribed Choroidal Hemangioma. J. Ophthalmic Vis. Res. 2015, 10, 320–328. [Google Scholar] [CrossRef]
- Giatromanolaki, A.; Arvanitidou, V.; Hatzimichael, A.; Simopoulos, C.; Sivridis, E. The HIF-2alpha/VEGF pathway activation in cutaneous capillary haemangiomas. Pathology 2005, 37, 149–151. [Google Scholar] [CrossRef] [PubMed]
- Ji, Y.; Chen, S.; Li, K.; Xiao, X.; Zheng, S.; Xu, T. The role of β-adrenergic receptor signaling in the proliferation of hemangioma-derived endothelial cells. Cell Div. 2013, 8, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanz-Marco, E.; Gallego, R.; Diaz-Llopis, M. Oral propranolol for circumscribed choroidal hemangioma. Case Rep. Ophthalmol. 2011, 2, 84–90. [Google Scholar] [CrossRef] [PubMed]
- O’Bryhim, B.E.; Li, A.S.; Bayliss, S.J.; Tychsen, L.; Lueder, G.T.; Rajagopal, R. Successful treatment of an exudative choroidal hemangioma with oral propranolol in a 10-year-old boy. J. AAPOS Off. Publ. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2019, 23, 236–238. [Google Scholar] [CrossRef]
- Arevalo, J.F.; Arias, J.D.; Serrano, M.A. Oral propranolol for exudative retinal detachment in diffuse choroidal hemangioma. Arch. Ophthalmol. 2011, 129, 1373–1375. [Google Scholar] [CrossRef] [Green Version]
- Thapa, R.; Shields, C.L. Oral propranolol therapy for management of exudative retinal detachment from diffuse choroidal hemangioma in Sturge-Weber syndrome. Eur. J. Ophthalmol. 2013, 23, 922–924. [Google Scholar] [CrossRef]
- Dave, T.; Dave, V.P.; Shah, G.; Pappuru, R.R. Diffuse Choroidal Hemangioma Masquerading as Central Serous Chorioretinopathy Treated with Oral Propranolol. Retin. Cases Brief Rep. 2016, 10, 11–14. [Google Scholar] [CrossRef]
- Tanabe, H.; Sahashi, K.; Kitano, T.; Tomita, Y.; Saito, A.M.; Hirose, H. Effects of oral propranolol on a juxtapapillary capillary hemangioma: A single-subject pilot study. Ophthalmic Surg. Lasers Imaging Retin. 2015, 46, 380–383. [Google Scholar] [CrossRef] [PubMed]
- Sancho, K.; Zett, C.; Gonçalves Júnior, I.; Morales, M.C.; Maia, M.; Mattos Neto, R.B. Effects of oral propranolol for circumscribed choroidal hemangioma. Arq. Bras. De Oftalmol. 2018, 81, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Krema, H.; Yousef, Y.A.; Durairaj, P.; Santiago, R. Failure of systemic propranolol therapy for choroidal hemangioma of Sturge-Weber syndrome: A report of 2 cases. JAMA Ophthalmol. 2013, 131, 681–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helmi, H.A.; Alkatan, H.M.; Al-Essa, R.S.; Aljudi, T.W.; Maktabi, A.M.Y.; Eberhart, C.G. Choroidal hemangioma in Sturge Weber syndrome: Case series with confirmed tissue diagnosis. Int. J. Surg. Case Rep. 2021, 89, 106626. [Google Scholar] [CrossRef]
- Jorge, R.; Chaves, L.; Cunha, A.D.S.; Correa, Z.M. Alternative Management of Circumscribed Choroidal Hemangioma Using Intravitreal Metoprolol. Retin. Cases Brief Rep. 2022, 16, 106–110. [Google Scholar] [CrossRef]
- Chaves, L.; Messias, A.; Correa, Z.; Jorge, R. Intravitreal metoprolol for circumscribed choroidal hemangiomas: A phase I clinical trial. Graefe’s Arch. Clin. Exp. Ophthalmol. Albrecht Von Graefes Arch. Fur Klin. Und Exp. Ophthalmol. 2021, 259, 2837–2841. [Google Scholar] [CrossRef]
- Gonçalves, A.N.; Messias, A.; Chaves, L.; de Azeredo Bastos, T.M.; Jorge, R. Safety of intravitreal metoprolol in eyes with central serous chorioretinopathy. Doc. Ophthalmologica. Adv. Ophthalmol. 2022, 145, 211–219. [Google Scholar] [CrossRef]
- De Paiva, M.R.B.; Arribada, R.G.; da Silva, C.N.; Ribeiro, M.C.S.; Jorge, R.; Fialho, S.L.; Silva-Cunha, A. Assessment of the safety of intravitreal injection of metoprolol tartrate in rabbits. Doc. Ophthalmologica. Adv. Ophthalmol. 2021, 142, 75–85. [Google Scholar] [CrossRef]
- Binderup, M.L.M.; Stendell, A.S.; Galanakis, M.; Møller, H.U.; Kiilgaard, J.F.; Bisgaard, M.L. Retinal hemangioblastoma: Prevalence, incidence and frequency of underlying von Hippel-Lindau disease. Br. J. Ophthalmol. 2018, 102, 942–947. [Google Scholar] [CrossRef]
- Wiley, H.E.; Krivosic, V.; Gaudric, A.; Gorin, M.B.; Shields, C.; Shields, J.; Aronow, M.E.; Chew, E.Y. MANAGEMENT OF RETINAL HEMANGIOBLASTOMA IN VON HIPPEL-LINDAU DISEASE. Retina 2019, 39, 2254–2263. [Google Scholar] [CrossRef]
- Chittiboina, P.; Lonser, R.R. Von Hippel-Lindau disease. Handb. Clin. Neurol. 2015, 132, 139–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, W.T.; Agrón, E.; Coleman, H.R.; Tran, T.; Reed, G.F.; Csaky, K.; Chew, E.Y. Clinical characterization of retinal capillary hemangioblastomas in a large population of patients with von Hippel-Lindau disease. Ophthalmology 2008, 115, 181–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahr, S.S.; Cusick, M.; Rodriguez-Coleman, H.; Srivastava, S.K.; Thompson, D.J.; Linehan, W.M.; Ferris, F.L., III; Chew, E.Y. Intravitreal anti-vascular endothelial growth factor therapy with pegaptanib for advanced von Hippel-Lindau disease of the retina. Retin. (Phila. Pa.) 2007, 27, 150–158. [Google Scholar] [CrossRef]
- Chan, C.C.; Chew, E.Y.; Shen, D.; Hackett, J.; Zhuang, Z. Expression of stem cells markers in ocular hemangioblastoma associated with von Hippel-Lindau (VHL) disease. Mol. Vis. 2005, 11, 697–704. [Google Scholar]
- Chan, C.C.; Collins, A.B.; Chew, E.Y. Molecular pathology of eyes with von Hippel-Lindau (VHL) Disease: A review. Retin. (Phila. Pa.) 2007, 27, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albiñana, V.; Villar Gómez de Las Heras, K.; Serrano-Heras, G.; Segura, T.; Perona-Moratalla, A.B.; Mota-Pérez, M.; de Campos, J.M.; Botella, L.M. Propranolol reduces viability and induces apoptosis in hemangioblastoma cells from von Hippel-Lindau patients. Orphanet J. Rare Dis. 2015, 10, 118. [Google Scholar] [CrossRef] [Green Version]
- Cuesta, A.M.; Albiñana, V.; Gallardo-Vara, E.; Recio-Poveda, L.; de Rojas, P.I.; de Las Heras, K.V.G.; Aguirre, D.T.; Botella, L.M. The β2-adrenergic receptor antagonist ICI-118,551 blocks the constitutively activated HIF signalling in hemangioblastomas from von Hippel-Lindau disease. Sci. Rep. 2019, 9, 10062. [Google Scholar] [CrossRef] [Green Version]
- Albiñana, V.; Escribano, R.M.J.; Soler, I.; Padial, L.R.; Recio-Poveda, L.; Villar Gómez de Las Heras, K.; Botella, L.M. Repurposing propranolol as a drug for the treatment of retinal haemangioblastomas in von Hippel-Lindau disease. Orphanet J. Rare Dis. 2017, 12, 122. [Google Scholar] [CrossRef] [Green Version]
- González-Rodríguez, B.; Villar Gómez de Las Heras, K.; Aguirre, D.T.; Rodríguez-Padial, L.; Albiñana, V.; Recio-Poveda, L.; Cuesta, A.M.; Botella, L.M.; Jiménez-Escribano, R.M. Evaluation of the safety and effectiveness of oral propranolol in patients with von Hippel-Lindau disease and retinal hemangioblastomas: Phase III clinical trial. BMJ Open Ophthalmol. 2019, 4, e000203. [Google Scholar] [CrossRef] [Green Version]
- Das, D.; Raj, S.J.S.; Bajaj, M.S. Acquired sessile conjunctival capillary haemangioma in an adult managed with topical timolol. BMJ Case Rep. 2020, 13, e237547. [Google Scholar] [CrossRef]
- Muranaka, K.; Kunimatsu, S.; Kaji, Y.; Joko, S.; Kato, S.; Numaga, J. Conjunctival haemangioma in an elderly patient. Eye 1999, 13((Pt. 6)), 790. [Google Scholar] [CrossRef]
- Honavar, S.G.; Manjandavida, F.P. Tumors of the ocular surface: A review. Indian J. Ophthalmol. 2015, 63, 187–203. [Google Scholar] [CrossRef] [PubMed]
- Nattis, A.; Perry, H.D.; Rosenberg, E.D.; Cocker, R. Conjunctival Capillary Hemangioma. Cureus 2017, 9, e1892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lubahn, J.G.; Lee, R.K.; Karp, C.L. Resolution of conjunctival sessile hemangioma with topical timolol. Cornea 2014, 33, 99–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, T.C.; Estes, R. Beta blocker treatment of infantile conjunctival hemangiomas—Observations from 2 cases. J. AAPOS Off. Publ. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2014, 18, 80–82. [Google Scholar] [CrossRef]
- Theiler, M.; Baselga, E.; Gerth-Kahlert, C.; Mathes, E.F.; Schwieger-Briel, A.; Chaloupka, K.; Weibel, L.; Frieden, I.J. Infantile hemangiomas with conjunctival involvement: An underreported occurrence. Pediatr. Dermatol. 2017, 34, 681–685. [Google Scholar] [CrossRef]
- Chisholm, K.M.; Chang, K.W.; Truong, M.T.; Kwok, S.; West, R.B.; Heerema-McKenney, A.E. β-Adrenergic receptor expression in vascular tumors. Mod. Pathol. 2012, 25, 1446–1451. [Google Scholar] [CrossRef] [Green Version]
- Bassi, A.; Filippeschi, C.; Oranges, T.; Caporalini, C.; Pini, A.; Nardini, P.; Gentile, R.M.; Filippi, L. Infantile hemangiomas β(3)-adrenoceptor overexpression is associated with nonresponse to propranolol. Pediatr. Res. 2022, 91, 163–170. [Google Scholar] [CrossRef]
- Storch, C.H.; Hoeger, P.H. Propranolol for infantile haemangiomas: Insights into the molecular mechanisms of action. Br. J. Dermatol. 2010, 163, 269–274. [Google Scholar] [CrossRef]
- Vanhoutte, P.M. Endothelial adrenoceptors. J. Cardiovasc. Pharm. 2001, 38, 796–808. [Google Scholar] [CrossRef]
- McSorley, P.D.; Warren, D.J. Effects of propranolol and metoprolol on the peripheral circulation. Br. Med. J. 1978, 2, 1598–1600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenberger, S.; Bischoff, J. Infantile hemangioma-mechanism(s) of drug action on a vascular tumor. Cold Spring Harb. Perspect. Med. 2011, 1, a006460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fredriksson, J.M.; Lindquist, J.M.; Bronnikov, G.E.; Nedergaard, J. Norepinephrine induces vascular endothelial growth factor gene expression in brown adipocytes through a beta -adrenoreceptor/cAMP/protein kinase A pathway involving Src but independently of Erk1/2. J. Biol. Chem. 2000, 275, 13802–13811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thaker, P.H.; Han, L.Y.; Kamat, A.A.; Arevalo, J.M.; Takahashi, R.; Lu, C.; Jennings, N.B.; Armaiz-Pena, G.; Bankson, J.A.; Ravoori, M.; et al. Chronic stress promotes tumor growth and angiogenesis in a mouse model of ovarian carcinoma. Nat. Med. 2006, 12, 939–944. [Google Scholar] [CrossRef]
- Huang, C.; Huang, J.; Yu, G. Co-suppression of VEGF-A and VEGF-C inhibits development of experimental hemangioma. Am. J. Transl. Res. 2018, 10, 2911–2919. [Google Scholar]
- Annabi, B.; Lachambre, M.P.; Plouffe, K.; Moumdjian, R.; Béliveau, R. Propranolol adrenergic blockade inhibits human brain endothelial cells tubulogenesis and matrix metalloproteinase-9 secretion. Pharmacol. Res. Off. J. Ital. Pharmacol. Soc. 2009, 60, 438–445. [Google Scholar] [CrossRef]
- Bergers, G.; Brekken, R.; McMahon, G.; Vu, T.H.; Itoh, T.; Tamaki, K.; Tanzawa, K.; Thorpe, P.; Itohara, S.; Werb, Z.; et al. Matrix metalloproteinase-9 triggers the angiogenic switch during carcinogenesis. Nat. Cell Biol. 2000, 2, 737–744. [Google Scholar] [CrossRef]
- Taraboletti, G.; Garofalo, A.; Belotti, D.; Drudis, T.; Borsotti, P.; Scanziani, E.; Brown, P.D.; Giavazzi, R. Inhibition of angiogenesis and murine hemangioma growth by batimastat, a synthetic inhibitor of matrix metalloproteinases. J. Natl. Cancer Inst. 1995, 87, 293–298. [Google Scholar] [CrossRef]
- Guo, K.; Ma, Q.; Wang, L.; Hu, H.; Li, J.; Zhang, D.; Zhang, M. Norepinephrine-induced invasion by pancreatic cancer cells is inhibited by propranolol. Oncol. Rep. 2009, 22, 825–830. [Google Scholar] [CrossRef]
- Nilsson, M.B.; Armaiz-Pena, G.; Takahashi, R.; Lin, Y.G.; Trevino, J.; Li, Y.; Jennings, N.; Arevalo, J.; Lutgendorf, S.K.; Gallick, G.E.; et al. Stress hormones regulate interleukin-6 expression by human ovarian carcinoma cells through a Src-dependent mechanism. J. Biol. Chem. 2007, 282, 29919–29926. [Google Scholar] [CrossRef] [Green Version]
- Maimaiti, A.; Aierken, Y.; Zhou, L.; He, J.; Abudureyimu, A.; Li, S.X. Inhibiting Interleukin-6/Signal Transducers and Activators of Transduction-3/Hypoxia-Inducible Factor-1α Signaling Pathway Suppressed the Growth of Infantile Hemangioma. Eur. J. Pediatr. Surg. 2022. [Google Scholar] [CrossRef] [PubMed]
- Sommers Smith, S.K.; Smith, D.M. Beta blockade induces apoptosis in cultured capillary endothelial cells. Vitr. Cell. Dev. Biology. Anim. 2002, 38, 298–304. [Google Scholar] [CrossRef]
- Sun, B.; Dong, C.; Lei, H.; Gong, Y.; Li, M.; Zhang, Y.; Zhang, H.; Sun, L. Propranolol inhibits proliferation and induces apoptosis of hemangioma-derived endothelial cells via Akt pathway by down-regulating Ang-2 expression. Chem. Biol. Interact. 2020, 316, 108925. [Google Scholar] [CrossRef] [PubMed]
- Ji, Y.; Li, K.; Xiao, X.; Zheng, S.; Xu, T.; Chen, S. Effects of propranolol on the proliferation and apoptosis of hemangioma-derived endothelial cells. J. Pediatr. Surg. 2012, 47, 2216–2223. [Google Scholar] [CrossRef]
- Yao, T.H.; Pataer, P.; Regmi, K.P.; Gu, X.W.; Li, Q.Y.; Du, J.T.; Ge, S.M.; Tu, J.B. Propranolol induces hemangioma endothelial cell apoptosis via a p53-BAX mediated pathway. Mol. Med. Rep. 2018, 18, 684–694. [Google Scholar] [CrossRef] [Green Version]
- Virgili, G.; Gatta, G.; Ciccolallo, L.; Capocaccia, R.; Biggeri, A.; Crocetti, E.; Lutz, J.M.; Paci, E. Incidence of uveal melanoma in Europe. Ophthalmology 2007, 114, 2309–2315. [Google Scholar] [CrossRef]
- Kaliki, S.; Shields, C.L. Uveal melanoma: Relatively rare but deadly cancer. Eye (Lond. Engl.) 2017, 31, 241–257. [Google Scholar] [CrossRef] [Green Version]
- Andreoli, M.T.; Mieler, W.F.; Leiderman, Y.I. Epidemiological trends in uveal melanoma. Br. J. Ophthalmol. 2015, 99, 1550–1553. [Google Scholar] [CrossRef]
- Singh, A.D.; Turell, M.E.; Topham, A.K. Uveal melanoma: Trends in incidence, treatment, and survival. Ophthalmology 2011, 118, 1881–1885. [Google Scholar] [CrossRef]
- Shields, C.L.; Furuta, M.; Thangappan, A.; Nagori, S.; Mashayekhi, A.; Lally, D.R.; Kelly, C.C.; Rudich, D.S.; Nagori, A.V.; Wakade, O.A.; et al. Metastasis of uveal melanoma millimeter-by-millimeter in 8033 consecutive eyes. Arch. Ophthalmol. 2009, 127, 989–998. [Google Scholar] [CrossRef]
- Chattopadhyay, C.; Kim, D.W.; Gombos, D.S.; Oba, J.; Qin, Y.; Williams, M.D.; Esmaeli, B.; Grimm, E.A.; Wargo, J.A.; Woodman, S.E.; et al. Uveal melanoma: From diagnosis to treatment and the science in between. Cancer 2016, 122, 2299–2312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shields, C.L.; Kaliki, S.; Shah, S.U.; Luo, W.; Furuta, M.; Shields, J.A. Iris melanoma: Features and prognosis in 317 children and adults. J. AAPOS Off. Publ. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2012, 16, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Carvajal, R.D.; Schwartz, G.K.; Tezel, T.; Marr, B.; Francis, J.H.; Nathan, P.D. Metastatic disease from uveal melanoma: Treatment options and future prospects. Br. J. Ophthalmol. 2017, 101, 38–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eskelin, S.; Pyrhönen, S.; Summanen, P.; Hahka-Kemppinen, M.; Kivelä, T. Tumor doubling times in metastatic malignant melanoma of the uvea: Tumor progression before and after treatment. Ophthalmology 2000, 107, 1443–1449. [Google Scholar] [CrossRef]
- De Giorgi, V.; Grazzini, M.; Gandini, S.; Benemei, S.; Lotti, T.; Marchionni, N.; Geppetti, P. Treatment with β-blockers and reduced disease progression in patients with thick melanoma. Arch. Intern. Med. 2011, 171, 779–781. [Google Scholar] [CrossRef]
- Moretti, S.; Massi, D.; Farini, V.; Baroni, G.; Parri, M.; Innocenti, S.; Cecchi, R.; Chiarugi, P. β-adrenoceptors are upregulated in human melanoma and their activation releases pro-tumorigenic cytokines and metalloproteases in melanoma cell lines. Lab. Investig. A J. Tech. Methods Pathol. 2013, 93, 279–290. [Google Scholar] [CrossRef] [Green Version]
- Yang, E.V.; Kim, S.J.; Donovan, E.L.; Chen, M.; Gross, A.C.; Webster Marketon, J.I.; Barsky, S.H.; Glaser, R. Norepinephrine upregulates VEGF, IL-8, and IL-6 expression in human melanoma tumor cell lines: Implications for stress-related enhancement of tumor progression. Brain Behav. Immun. 2009, 23, 267–275. [Google Scholar] [CrossRef] [Green Version]
- De Giorgi, V.; Grazzini, M.; Benemei, S.; Marchionni, N.; Botteri, E.; Pennacchioli, E.; Geppetti, P.; Gandini, S. Propranolol for Off-label Treatment of Patients With Melanoma: Results From a Cohort Study. JAMA Oncol. 2018, 4, e172908. [Google Scholar] [CrossRef]
- Bustamante, P.; Miyamoto, D.; Goyeneche, A.; de Alba Graue, P.G.; Jin, E.; Tsering, T.; Dias, A.B.; Burnier, M.N.; Burnier, J.V. Beta-blockers exert potent anti-tumor effects in cutaneous and uveal melanoma. Cancer Med. 2019, 8, 7265–7277. [Google Scholar] [CrossRef] [Green Version]
- Kaliki, S.; Shields, C.L.; Shields, J.A. Uveal melanoma: Estimating prognosis. Indian J. Ophthalmol. 2015, 63, 93–102. [Google Scholar] [CrossRef]
- Koch, K.R.; Refaian, N.; Hos, D.; Schlereth, S.L.; Bosch, J.J.; Cursiefen, C.; Heindl, L.M. Autocrine impact of VEGF-A on uveal melanoma cells. Investig. Ophthalmol. Vis. Sci. 2014, 55, 2697–2704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Filali, M.; Van der Velden, P.A.; Luyten, G.P.M.; Jager, M.J. Anti-angiogenic therapy in uveal melanoma. Dev. Ophthalmol. 2012, 49, 117–136. [Google Scholar] [CrossRef] [PubMed]
- Dithmer, M.; Kirsch, A.M.; Gräfenstein, L.; Wang, F.; Schmidt, H.; Coupland, S.E.; Fuchs, S.; Roider, J.; Klettner, A.K. [Uveal Melanoma Cell Under Oxidative Stress-Influence of VEGF and VEGF-Inhibitors]. Klin. Mon. Fur Augenheilkd. 2019, 236, 295–307. [Google Scholar] [CrossRef]
- Yamazaki, T.; Komuro, I.; Zou, Y.; Kudoh, S.; Shiojima, I.; Hiroi, Y.; Mizuno, T.; Aikawa, R.; Takano, H.; Yazaki, Y. Norepinephrine induces the raf-1 kinase/mitogen-activated protein kinase cascade through both alpha 1- and beta-adrenoceptors. Circulation 1997, 95, 1260–1268. [Google Scholar] [CrossRef] [PubMed]
- Zuidervaart, W.; van Nieuwpoort, F.; Stark, M.; Dijkman, R.; Packer, L.; Borgstein, A.M.; Pavey, S.; van der Velden, P.; Out, C.; Jager, M.J.; et al. Activation of the MAPK pathway is a common event in uveal melanomas although it rarely occurs through mutation of BRAF or RAS. Br. J. Cancer 2005, 92, 2032–2038. [Google Scholar] [CrossRef] [Green Version]
- Gaudi, S.; Messina, J.L. Molecular bases of cutaneous and uveal melanomas. Pathol. Res. Int. 2011, 2011, 159421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janik, M.E.; Szlęzak, D.; Surman, M.; Gołas, A.; Lityńska, A.; Przybyło, M. Diversified β-2-adrenergic Receptor Expression and Action in Melanoma Cells. Anticancer Res. 2017, 37, 3025–3033. [Google Scholar] [CrossRef] [Green Version]
- El-Shabrawi, Y.; Ardjomand, N.; Radner, H.; Ardjomand, N. MMP-9 is predominantly expressed in epithelioid and not spindle cell uveal melanoma. J. Pathol. 2001, 194, 201–206. [Google Scholar] [CrossRef]
- Lai, K.; Conway, R.M.; Crouch, R.; Jager, M.J.; Madigan, M.C. Expression and distribution of MMPs and TIMPs in human uveal melanoma. Exp. Eye Res. 2008, 86, 936–941. [Google Scholar] [CrossRef]
- Roewe, J.; Higer, M.; Riehl, D.R.; Gericke, A.; Radsak, M.P.; Bosmann, M. Neuroendocrine Modulation of IL-27 in Macrophages. J. Immunol. 2017, 199, 2503–2514. [Google Scholar] [CrossRef] [Green Version]
- Nishioka, R.; Nishi, Y.; Choudhury, M.E.; Miyaike, R.; Shinnishi, A.; Umakoshi, K.; Takada, Y.; Sato, N.; Aibiki, M.; Yano, H.; et al. Surgical stress quickly affects the numbers of circulating B-cells and neutrophils in murine septic and aseptic models through a β(2) adrenergic receptor. J. Immunotoxicol. 2022, 19, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Omri, S.; Tahiri, H.; Pierre, W.C.; Desjarlais, M.; Lahaie, I.; Loiselle, S.E.; Rezende, F.; Lodygensky, G.; Hebert, T.E.; Ong, H.; et al. Propranolol Attenuates Proangiogenic Activity of Mononuclear Phagocytes: Implication in Choroidal Neovascularization. Investig. Ophthalmol. Vis. Sci. 2019, 60, 4632–4642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.Y.; Wang, S.Q.; Zhu, W.Z.; Chruscinski, A.; Kobilka, B.K.; Ziman, B.; Wang, S.; Lakatta, E.G.; Cheng, H.; Xiao, R.P. Culture and adenoviral infection of adult mouse cardiac myocytes: Methods for cellular genetic physiology. Am. J. Physiology. Heart Circ. Physiol. 2000, 279, H429–H436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, Y.; Zhang, Q.; Liu, L.; Tang, J.; Kern, T.S.; Steinle, J.J. β2-Adrenergic Receptor Knockout Mice Exhibit A Diabetic Retinopathy Phenotype. PLoS ONE 2013, 8, e70555. [Google Scholar] [CrossRef] [Green Version]
- Cernecka, H.; Pradidarcheep, W.; Lamers, W.H.; Schmidt, M.; Michel, M.C. Rat β3-adrenoceptor protein expression: Antibody validation and distribution in rat gastrointestinal and urogenital tissues. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2014, 387, 1117–1127. [Google Scholar] [CrossRef]
- Pradidarcheep, W.; Stallen, J.; Labruyère, W.T.; Dabhoiwala, N.F.; Michel, M.C.; Lamers, W.H. Lack of specificity of commercially available antisera against muscarinergic and adrenergic receptors. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2009, 379, 397–402. [Google Scholar] [CrossRef] [Green Version]
- Cernecka, H.; Ochodnicky, P.; Lamers, W.H.; Michel, M.C. Specificity evaluation of antibodies against human β3-adrenoceptors. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2012, 385, 875–882. [Google Scholar] [CrossRef]
- Böhmer, T.; Pfeiffer, N.; Gericke, A. Three commercial antibodies against α1-adrenergic receptor subtypes lack specificity in paraffin-embedded sections of murine tissues. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2014, 387, 703–706. [Google Scholar] [CrossRef]
- Vrydag, W.; Michel, M.C. Tools to study beta3-adrenoceptors. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2007, 374, 385–398. [Google Scholar] [CrossRef] [Green Version]
- Michel, M.C. α(1)-adrenoceptor activity of β-adrenoceptor ligands-An expected drug property with limited clinical relevance. Eur. J. Pharmacol. 2020, 889, 173632. [Google Scholar] [CrossRef]
- Billington, C.K.; Penn, R.B.; Hall, I.P. β(2) Agonists. Handb. Exp. Pharmacol. 2017, 237, 23–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Structure | β1-AR | β2-AR | β3-AR | Possible Functions | Relevance for Ocular Diseases | References |
|---|---|---|---|---|---|---|
| Cornea | x |
|
| [10,11,12,13,14,15,16,17,18,19,20,21,22,23] | ||
| Conjunctiva | x | x | x |
|
| [24,25,26,27,28,29,30,31,32] |
| Lacrimal gland | x | x | x |
|
| [33,34,35,36,37,38,39,40,41,42] |
| Trabecular meshwork | x |
| [43,44,45,46,47,48] | |||
| Ciliary body | x | x |
|
| [49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64] | |
| Choroid | x | x | x |
|
| [54,65,66,67,68] |
| Retina | x | x | x |
|
| [17,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114] |
| Title | Disease | β-AR Antagonist | Type of Clinical Trial | Trial Registration | Outcome |
|---|---|---|---|---|---|
| Propranolol in a case series of 174 patients with complicated infantile haemangioma: indications, safety and future directions [131] | Infantile hemangioma | Oral propranolol | Prospective case series (174 patients) | Not stated in pubication | Sucessful treatment in 99.4% |
| Oral propranolol: an effective, safe treatment for infantile hemangiomas [132] | Infantile hemangioma | Oral propranolol | Prospective clinical study (30 patients) | Not stated in publication | Complete lesion resolution in 60%, 50% reduction in size in 20%, less than 50% reduction in size in 16.6%, resistance to treatment in 3.3% |
| A retrospective analysis of systemic propranolol for the treatment of complicated infantile hemangiomas. [133] | Infantile hemangioma | Oral propranolol | Retrospective study (207 patients) | Not stated in publication | Successful treatment in 99.5% |
| Propranolol vs. corticosteroids for infantile hemangiomas: a multicenter retrospective analysis [137] | Infantile hemangioma | Oral propranolol vs. oral corticosteroids | Multicenter retrospective analysis (110 patients) | Not stated in publication | Clearance of 75% or more in 82% of patients treated with propranolol and in 29% of patients treated with corticosteroids |
| A controlled study of topical 0.25% timolol maleate gel for the treatment of cutaneous infantile capillary hemangiomas [143] | Infantile hemangioma | Topical 0.25% timolol maleate gel | Retrospective, consecutive, nonrandomized, comparative single-masked cohort study (23 patients) | Not stated in publication | Good response in 61.5%, moderate response in 30.8% and poor response in 7.7% in the treated group |
| Efficacy and Safety of Topical Timolol for the Treatment of Infantile Hemangioma in the Early Proliferative Stage: A Randomized Clinical Trial [146] | Infantile hemangioma | Topical 0.25% timolol maleate gel | Multicenter, randomized, double-blind, placebo-controlled, phase 2a pilot clinical trial (69 patients) | NCT02731287,EudraCT Number: 2013-005199-17 | No significant differences between timolol and placebo for complete or nearly complete IH resolution |
| Combined Oral and Topical Beta Blockers for the Treatment of Early Proliferative Superficial Periocular Infantile Capillary Hemangioma [147] | Infantile hemangioma | Oral propranolol and topical 0.25% timolol maleate gel or oral propranolol only | Randomized, controlled comparison trial (25 patients) | Not stated in publication | Hemangioma Activity Score was significantly improved in both groups, significantly better response in the systemic and topical treated group |
| To compare intralesional and oral propranolol for treating periorbital and eyelid capillary hemangiomas [150] | Infantile hemangioma | Oral propranolol or intralesional propranolol hydrochloride | Pilot randomized control trial (20 patients) | Clinical Trials Registry of India: CTRI/2017/08/009440 | No difference in area reduction, change in appearance, ptosis and side effects between the two groups |
| Effects of oral propranolol for circumscribed choroidal hemangioma [175] | Choroidal hemangioma | Oral propranolol | Prospective, longitudinal interventional study (5 patients) | Not stated in publication | No clinical or diagnostic changes in tumor size during treatment |
| Intravitreal metoprolol for circumscribed choroidal hemangiomas: a phase I clinical trial [179] | Choroidal hemangioma | Intravitreal metoprolol | Prospective interventional phase I clinical trial (5 patients) | Not stated in publication | No signs of acute ocular toxicity |
| Evaluation of the safety and effectiveness of oral propranolol in patients with von Hippel-Lindau disease and retinal hemangioblastomas: phase III clinical trial [192] | Retinal hemangioblastoma in von Hippel-Lindau disease | Oral propranolol | Prospective interventional phase III clinical trial (7 patients) | EudraCT Number: 2014-003671-30. | Number and size of retinal hemangioblastomas remained stable |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Böhm, E.W.; Stoffelns, B.; Gericke, A. β-Adrenoreceptors as Therapeutic Targets for Ocular Tumors and Other Eye Diseases—Historical Aspects and Nowadays Understanding. Int. J. Mol. Sci. 2023, 24, 4698. https://doi.org/10.3390/ijms24054698
Böhm EW, Stoffelns B, Gericke A. β-Adrenoreceptors as Therapeutic Targets for Ocular Tumors and Other Eye Diseases—Historical Aspects and Nowadays Understanding. International Journal of Molecular Sciences. 2023; 24(5):4698. https://doi.org/10.3390/ijms24054698
Chicago/Turabian StyleBöhm, Elsa Wilma, Bernhard Stoffelns, and Adrian Gericke. 2023. "β-Adrenoreceptors as Therapeutic Targets for Ocular Tumors and Other Eye Diseases—Historical Aspects and Nowadays Understanding" International Journal of Molecular Sciences 24, no. 5: 4698. https://doi.org/10.3390/ijms24054698